
Abstract
Background
There is a positive association between chronic inflammation and the risk of cardiovascular disease, but whether there is an association between C-reactive protein (CRP) and carotid atherosclerosis is controversial. We investigated the relationship between high-sensitivity CRP (hsCRP) levels and carotid intima-media thickness (IMT) in healthy Koreans.
Design
We measured hsCRP levels, the carotid IMT, and conventional cardiovascular risk factors including obesity parameters, blood pressure, lipid profiles, insulin resistance, and smoking habits in 820 volunteers (35–79 years old) in a cross-sectional study.
Results
Higher hsCRP quartile groups had higher mean IMTs, as compared with the lowest quartile (P < 0.001 for the trend across quartiles). However, after adjustment for age, the relationship between hsCRP level and IMT was substantially weaker (P = 0.018). After additional adjustments for conventional cardiovascular risk factors, no significant association was observed (P = 0.548). The unadjusted risk for a high carotid IMT value (≥ 1.0 mm) was also positively related to hsCRP quartile, but this relationship was not significant after adjustment for age and other cardiovascular risk factors.
Conclusions
Both hsCRP levels and the carotid IMT were strongly correlated with conventional cardiovascular risk factors, but there was no independent association between hsCRP levels and carotid IMT in healthy Korean adults.
Introduction
Chronic inflammation is important for the development and progression of atherosclerosis [1]. C-reactive protein (CRP) is a marker of chronic inflammation and epidemiologic studies have revealed positive associations between CRP levels and the risk of developing atherosclerotic cardiovascular disease [2–8. Carotid intima–media thickness (IMT) measured by high-resolution-ultrasonography is a marker of atherosclerosis that is associated with future cardiovascular events [9–11. However, the relationship between CRP levels and carotid atherosclerosis is not understood. Some studies reported a positive association between CRP levels and carotid atherosclerosis [8,12–17], whereas other studies failed to detect an independent association between inflammatory markers and carotid atherosclerosis [18–22. The association between high-sensitivity CRP (hsCRP) levels and major cardiovascular risk factors has been studied in Korean populations [23], but the association between hsCRP levels and the carotid IMT in Koreans has not been assessed. Therefore, in the present study, we investigated the association between hsCRP levels and carotid IMT in healthy Korean adults.
Methods
Subjects
This study was performed as a part of the Korean Metabolic Syndrome Study that commenced in 2001, to evaluate the role of metabolic syndrome as a risk for cardiovascular disease in Korean adults [24]. The study protocol was approved by the ethics committee of the Severance Hospital at Yonsei University, and informed consent was obtained from each participant.
We measured the carotid IMT of 1230 men and women who were 35–79 years old. These measurements were made over a 3-month period (April-June, 2001) at a health screening centre in Seoul, Korea. All participants were healthy, independently functioning individuals who were at the health centre to undergo screening tests. Of the 1230 initial volunteers, hsCRP levels were available for 948 individuals. During the initial time of inclusion, we measured only traditional CRP level rather than hsCRP, therefore we excluded these data for this analysis. However, there was no significant differences between those who had data for hsCRP level and those who did not, except for age and body mass index in women (data not shown). We excluded 99 people who had a previous history of myocardial infarction, stroke, or peripheral arterial disease and also excluded 29 people with hsCRP levels of > 10 mg/1 for considering acute inflammation [25]. Finally, we enrolled 820 individuals (431 men and 389 women) in the study.
Clinical characteristics and biochemical analysis
Trained nurses interviewed all participants and obtained their medical history using a standardized questionnaire. Participants rested for 5 min prior to their blood pressure being checked twice at an interval of at least 1 min. The mean value of these two measurements was used for the analyses. The weight and height of each participant was measured while the subject was clothed only in a light gown, and body mass index was calculated as body weight (kg) divided by the square of height (m2). Waist circumference was measured by the same examiner between the lowest rib and the iliac crest in a standing position.
A fasting blood sample was withdrawn from each subject. Serum total cholesterol, high-density lipoprotein (HDL) cholesterol, and triglyceride levels were measured by auto-analyzer (Au5200; Olympus, Tokyo, Japan) using enzymatic colorimetry, and the low-density lipoprotein (LDL) cholesterol level was calculated using Friedewald's equation [26]. The blood glucose level was measured using the glucose oxidase method (747 Automatic Analyzer; Hitachi, Tokyo, Japan). The serum insulin level was measured using a radioimmunoassay that had an interassay coefficient of variation (CV) of 4% (Linco Research, Missouri, USA). Insulin resistance was calculated using the homeostasis model assessment of insulin resistance (HOMA-IR) [27].
HOMA-IR = fasting insulin (μU/ml) × fasting plasma glucose (mmol/l)/22.5
We defined hypertension as systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg, and/or use of antihypertensive medication. Diabetes mellitus was defined as a serum glucose level
≥ 7.0 mmol/l (126 mg/dl) or use of glucose-lowering medication.
Measurement of carotid intima-media thickness
The carotid arteries were evaluated using high-resolution B-mode ultrasonography using a 7.5 MHz probe (SSA-270A; Toshiba, Tokyo, Japan). Both common carotid arteries were thoroughly scanned from proximal to distal to the bifurcation. Frozen photocopy of end-diastolic images in the longitudinal view showing the bifurcation were captured. All images were taken when the inner echoes of both near and far wall were clearly visible. The IMT was measured at the far wall of the both common carotid artery about 1 cm proximal to the carotid bulb. Measurements of IMT, the distance between the leading edge of first and second echogenic line were performed using a caliper (Digimatic; Mitutoyo, Japan). The IMT of the common carotid artery (CCA) was defined as the mean of the maximal IMTof each common carotid artery. All measurements were made by one examiner. The intra-observer coefficient of variation (CV) in our laboratory was 2.1% [28].
Measurement of high-sensitivity C-reactive protein levels
All blood samples were assayed using serum that had been stored at −70°C. Serum hsCRP levels were measured using a high-sensitivity automated immuno-turbidimetric method (Denka Seiken CRP II Latex X2; Tokyo, Japan). The range of sensitivity was 0.01–320.00 mg/1, the coefficient of variation was 2.9–7.6%, and the correlation coefficient (r2) for the immunoturbidimetric measurements versus those of a nephelometer was 0.97.
Statistical analysis
We compared conventional cardiovascular risk factors, hsCRP levels, and the carotid IMT for data categorized according to sex. Mean levels or frequencies of conventional cardiovascular risk factors and the carotid IMT were calculated according to sex-specific quartiles of hsCRP levels. The linear trends of conventional risk factors across hsCRP quartiles were tested for significance.
To examine the independent association between hsCRP levels and the carotid IMT, we applied the following serial models: unadjusted; age-adjusted; age- and hypertension-adjusted; and multivariate-adjusted. In the multivariate-adjusted models, age, hypertension, body mass index, total cholesterol, HDL-cholesterol, diabetes mellitus, and current smoking habits were included as variables. Crude and adjusted means of the carotid IMT across the hsCRP quartiles were estimated, and the significance of differences among quartiles was tested using multiple linear regression analysis. Crude and adjusted odds ratios for a high IMT (≥ 1.0 mm) across the hsCRP quartiles were estimated using multiple logistic regression. In these analyses, each quartile was compared to the lowest quartile, and a linear trend was calculated. Analyses were carried out on pooled data and data categorized according to sex.
The SAS System version 8.01 (SAS Institute, Cary, North Carolina, USA) was used to perform all statistical analyses. All statistical tests were two-sided, and P < 0.05 was considered to be statistically significant.
Results
The overall and sex-specific characteristics of the participants are presented in Table 1. There was no significant age difference between men and women. The body mass index was higher but the waist circumference and waist–hip ratio were lower in women than in men. Total and LDL-cholesterol levels were higher in women, whereas triglyceride and HDL-cholesterol levels were higher in men. Prevalence of diabetes and current smoking were higher in men than in women. The distribution of hsCRP levels was skewed to the right, and the mean and median value was 1.35 and 0.70 mg/1, respectively (range: 0.10–9.60 mg/1). Despite differences between sexes for the various cardiovascular risk factors, the carotid IMT levels were similar in men and women.
Quartiles of hsCRP levels were calculated separately for men and women, and the association between the hsCRP quartiles and conventional cardiovascular risk factors were evaluated (Table 2). Age, body mass index, waist circumference, and blood pressure were positively associated with hsCRP levels, both in men and women. Associations between lipid profiles and hsCRP levels differed between the sexes. Total cholesterol, triglycerides and the total/HDL-cholesterol ratio were positively associated with hsCRP levels in both sexes. However, LDL-cholesterol was positively associated with hsCRP levels only in women, while HDL-cholesterol was not associated with hsCRP levels in either sex. Fasting glucose levels were not associated with hsCRP levels in either sex. The HOMA-IR was positively associated with hsCRP levels only in men.
The carotid IMT was positively associated with hsCRP levels in both sexes in the univariate analysis (Table 3). However, this association was substantially weaker after adjustment for age. In the age- and hypertension-adjusted model and the fully adjusted model, the association between the carotid IMT and the hsCRP levels was no longer statistically significant. The same outcome was obtained from the analysis of the pooled and sex-categorized data.
Clinical characteristics of study subjects
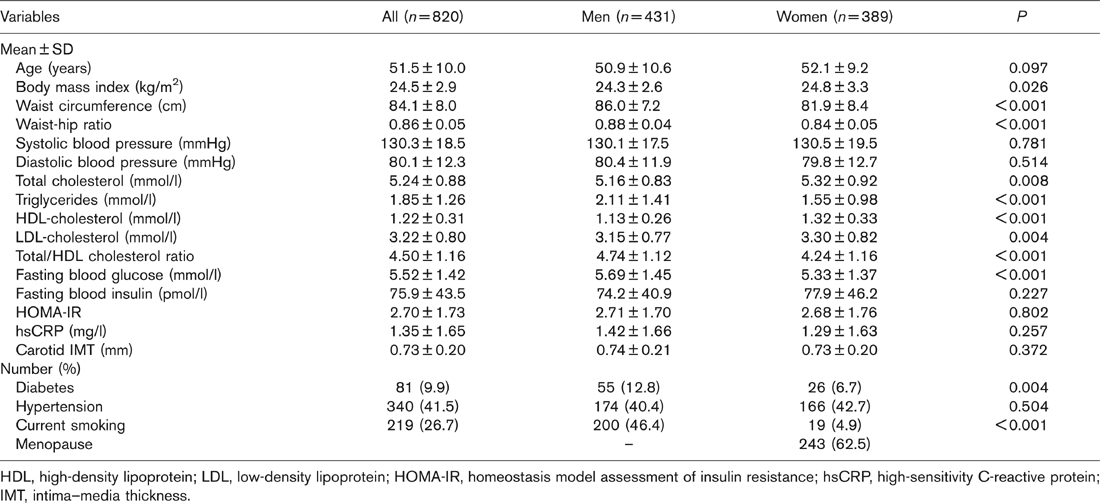
HDL, high-density lipoprotein; LDL, low-density lipoprotein; HOMA-IR, homeostasis model assessment of insulin resistance; hsCRP, high-sensitivity C-reactive protein; IMT, intima-media thickness.
Associations between high-sensitivity C-reactive protein (hsCRP) level and conventional cardiovascular risk factors
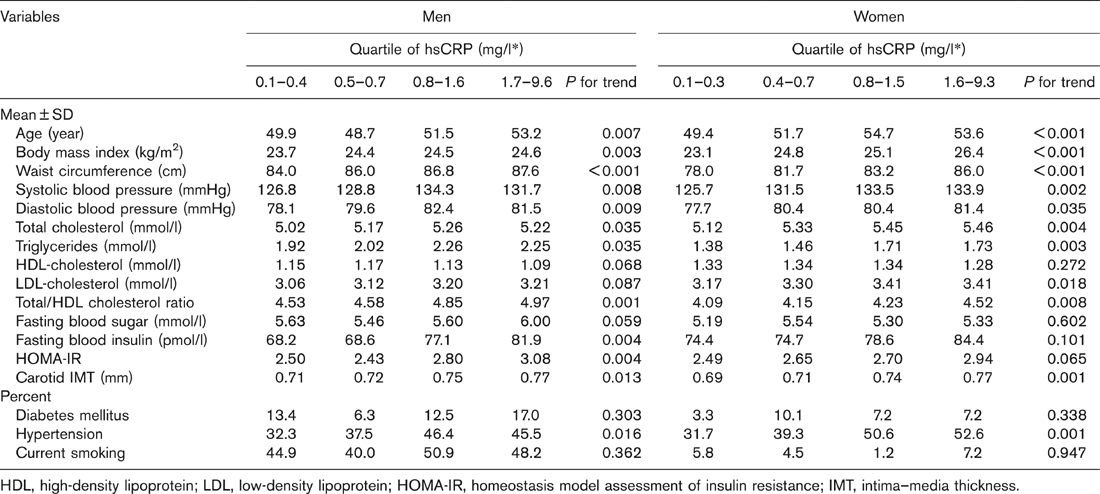
HDL, high-density lipoprotein; LDL, low-density lipoprotein; HOMA-IR, homeostasis model assessment of insulin resistance; IMT, intima–media thickness.
Relationship between high-sensitivity C-reactive protein (hsCRP) levels and carotid intima-media thickness (IMT)
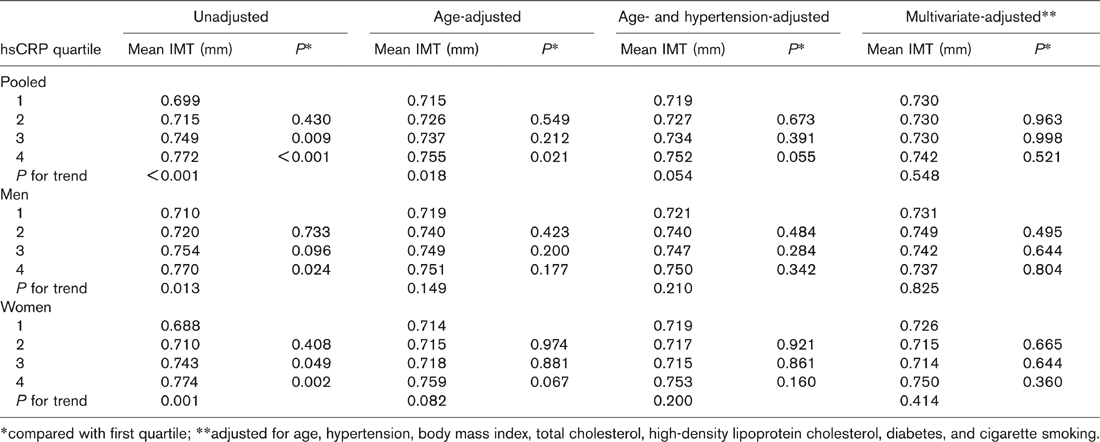
*compared with first quartile; ∗∗adjusted for age, hypertension, body mass index, total cholesterol, high-density lipoprotein cholesterol, diabetes, and cigarette smoking.
Associations between hsCRP levels and the risk of a high carotid IMT value (≥ 1.0 mm) were assessed using multiple logistic regression analysis (Table 4). Compared to the lowest quartile, the remaining (higher) quartiles had increased odds ratios for a high IMT, but a statistically significant difference was observed only for the highest quartile in women and in the pooled data. When we adjusted for age and other cardiovascular risk factors, no significant associations between hsCRP levels and the risk of high IMT were observed. Similarly, no significant trends were observed.
Discussion
Despite a high correlation between conventional cardiovascular risk factors and the carotid IMT, elevated hsCRP levels were not an independent predictor of carotid atherosclerosis in a healthy population of Koreans, after adjusting for age and other risk factors.
High-sensitivity C-reactive protein and carotid intima-media thickness in previous studies
The association between CRP levels and carotid atherosclerosis is controversial. Several factors may explain apparent discrepancies in the findings of previous studies. First, differences among study populations, such as age, may have produced variable results. The Rotterdam Study revealed a positive association between hsCRP levels and the carotid IMT in a relatively old population (mean age: 71.2 years) [14], and the Framingham Heart Study (mean age of participants: 55 years) revealed a positive association only in women [15]. Other studies of younger subjects (including our study) have failed to reveal a significant association between hsCRP levels and the carotid IMT [19–22. A positive correlation between hsCRP levels and carotid atherosclerosis is more likely to be observed in people at high risk of cardiovascular disease, such as smokers [12], patients with neurological disorders [16], and men with dyslipidaemia [19]. Therefore, CRP might modify the effect of other risk factors rather than being an independent risk factor for the development of atherosclerosis. Further studies are needed to clarify the relationship and interaction between inflammatory markers and conventional cardiovascular risk factors in the development of atherosclerotic cardiovascular diseases.
Relationship between high-sensitivity C-reactive protein (hsCRP) levels and the risk of high carotid intima–media thickness (IMT) values (IMT ≥ 1.0mm)
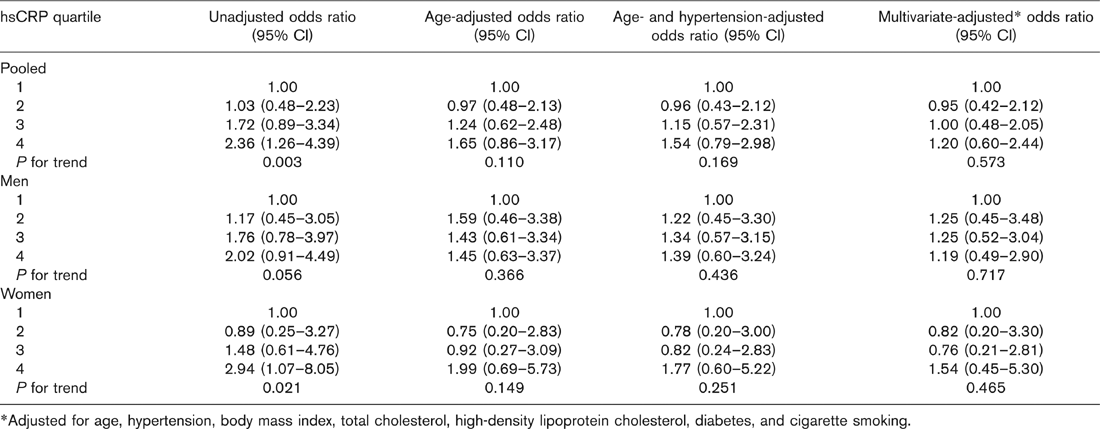
*Adjusted for age, hypertension, body mass index, total cholesterol, high-density lipoprotein cholesterol, diabetes, and cigarette smoking.
The second factor that may explain discrepancies in the findings of previous studies is that different methods were used to measure the carotid artery in different studies. The Framingham Heart Study showed that elevated CRP levels were associated with carotid stenosis and the internal carotid IMT, but not with the common carotid IMT [15]. Blackburn and colleagues [19] reported that hsCRP levels in men with dyslipidaemia were associated with advanced carotid plaques, but not with the common carotid IMT. Several studies in which the common carotid IMT was measured did not report a positive correlation between CRP levels and the IMT [18–22. These results suggested that the common carotid IMT might not be a sensitive marker of atherosclerosis.
The third factor that may explain discrepancies in the findings of previous studies is study design. Hashimoto and colleagues [13,17] reported that hsCRP levels were not related to the baseline plaque number or plaque score, but were related to annual changes in these parameters. A positive association between hsCRP levels and the progression of carotid atherosclerosis was also observed in the Rotterdam Study [29]. Therefore, hsCRP levels may be related more closely to atherosclerotic progression than to the extent of atherosclerosis.
Explanations of findings of the present study
There are several explanations for the lack of an association between hsCRP levels and the carotid IMT that we observed in the present study. First, the characteristics of the study population should be considered. Our population had a relatively lower body mass index, lower total and LDL-cholesterol levels, and a lower risk of coronary heart disease and ischaemic stroke, as compared to most Western populations. Our population also had a low prevalence of carotid atherosclerosis (9.1% had IMT ≥ 1.0 mm; 2.0% had IMT ≥ 1.3 mm) relative to previous studies. Therefore, chronic inflammation may not be as important a risk factor for atherosclerosis in our low-risk population. A recent study of Koreans reported that the hsCRP level was not associated with the carotid IMT, even in patients with hypertension [30].
A second explanation for our failure to observe an association between hsCRP levels and carotid IMT may be over-adjustment for other cardiovascular risk factors. If chronic inflammation contributed to the development of atherosclerosis through other risk factors such as hypertension, dyslipidaemia, and insulin resistance, adjustment for these factors may have obscured an association between hsCRP levels and the carotid IMT. If this were the case, such an association could not be investigated properly in a cross-sectional study such as ours.
Third, inadequate statistical power due to a small sample size is a common source of false negatives in epidemiological studies. We calculated statistical power in the present study (for a two-sided significance level of 0.05) and found that the statistical power to detect the difference between the lowest and highest quartiles of hsCRP levels was 95.8, 73.7, and 78.1% for the pooled data, for men, and for women, respectively. In addition, there was a decrease in the strength of the association between hsCRP levels and the carotid IMT with serial adjustments for possible confounding variables. Our findings were consistent irrespective of whether the data were pooled, categorized according to sex, or divided according to the carotid IMT value (continuous versus dichotomous). Therefore, it is unlikely that our conclusion is the result of a small sample size.
Strengths and limitations of the present study
Our study had several advantages over other studies. Measurement of the carotid IMT is particularly vulnerable to inter-observer variation. In our study, all IMT measurements were performed by the same examiner, in the same (regulated) setting, over a relatively short period (3 months). Therefore, measurement error and misclassification bias were minimized. In addition, the characteristics of the study population conferred an advantage on our study: either patients or high-risk individuals were used in most previous studies, whereas all the participants in our study were healthy, independently functioning individuals who had no medical history of major illness.
We should point out some of the limitations of our study. First, we could not assess the temporal relationship between hsCRP levels and the carotid IMT, because our study was cross-sectional. Second, we could not account for variations in CRP levels over time, because we obtained only one measurement of the hsCRP level in each participant. It is unlikely that CRP levels were affected markedly by acute inflammation, because we excluded subjects with hsCRP level > 10 mg/l. Finally, the study participants were healthy, but recruited from within a health screening centre; therefore, our population is not representative of the general population of Korea.
Conclusion
Both hsCRP levels and the carotid IMT were correlated with conventional cardiovascular risk factors in healthy Korean adults, but there was no independent association between hsCRP levels and the carotid IMT.
Footnotes
Acknowledgements
This study was supported in part by grants from Lilly Korea Ltd. We are deeply grateful for the co-operation of subjects participating in this study. We thank the Korea Association of Health for their help and support in collecting the data for this manuscript.