
Abstract
Background
Elevated levels of serum biomarkers such as C-reactive protein (CRP) and homocysteine have been independently associated with cardiovascular risk. However, the prevalence of concurrent elevations of these biomarkers in the general population is unknown, as is their association with cardiovascular disease (CVD).
Methods
Data from adults (n = 4900) in the National Health and Nutrition Examination Survey were used to investigate the relationship between combinations of serum biomarkers of inflammation (CRP), atherosclerosis (homocysteine), and insulin sensitivity [homeostatic model assessment (HOMA) fasting insulin] and CVD. Using SUDAAN, logistic regression models were constructed to examine the relationships between elevated serum biomarkers (CRP, homocysteine, HOMA, or insulin), singly or in combination, and having a history of heart failure, myocardial infarction (MI), stroke, or any CVD, while controlling for age, race, sex, obesity, smoking, cholesterol level, diabetes history, hypertension history, exercise level, and dietary fiber intake.
Results
After adjustment for covariates, there was a significant relationship between concomitant elevations of CRP plus homocysteine and a history of MI [odds ratio (OR) 2.21], heart failure (OR 2.14), and any CVD (OR 1.87) that was stronger than the relationship between individual biomarkers alone and a history of CVD. In addition, combinations of elevated CRP plus HOMA and CRP plus insulin, remained significantly related to having a history of any CVD.
Conclusion Recent scientific evidence and the present findings demonstrate the possibility for improving cardiovascular risk stratification through the concurrent evaluation of multiple biomarkers. In particular, these findings demonstrate the need to evaluate the combination of CRP and homocysteine prospectively as predictors of CVD.
Introduction
Although the mechanisms underlying the development of cardiovascular disease (CVD) are still not completely understood, an accumulating body of evidence suggests that inflammation may play an important role. Elevated levels of inflammatory markers such as C-reactive protein (CRP) independently predict increased rates of cardiovascular events, including myocardial infarction (MI), heart failure, and stroke [1–4], in both high-risk and low-risk populations. Elevated levels of CRP have also been linked to several atherogenic conditions, including hyperglycemia, insulin resistance, and overt diabetes [5–9].
Previous studies [9–11] have generally evaluated cardiovascular risk markers singly, adjusting for other known CVD risk factors. However, elevated CRP levels only explain a small portion of the total cardiovascular risk [12]. One strategy for improving the predictive capacity of serum markers is to combine markers and indicators associated with cardiovascular risk. Determining which combination of serum markers would be best is a clinical challenge.
Using data from adults in the National Health and Nutrition Examination Survey 1999–2000 (NHANES 99-00) we investigated combinations of serum biomarkers of inflammation, atherosclerosis, and insulin sensitivity to determine their associations with CVD, including MI, stroke, and heart failure. Using a large population representative of the United States offers the advantage of being able to control for other cardiovascular and demographic risk factors, and allows us to extrapolate the results to the general population.
Methods
Data collection
We derived our study sample from the participants in the NHANES 99-00. The NHANES 99-00 is the most recent release of this nationally representative, complex, multistage, probability-based survey of the civilian, non-institutionalized population of the United States. The 12-month survey was conducted beginning in April 1999 by the National Center for Health Statistics (NCHS), the Centers for Disease Control and Prevention. This survey has been designed to collect information about the health and diet of people in the United States. The NHANES 99-00 is valuable in that it combines a home interview with health tests that are performed in a mobile examination center. The health tests consist of both a physical examination and laboratory components. The laboratory data files include findings from analyses of blood, urine, hair, air, tuberculosis skin test, and household dust specimens. Specimens were collected at the mobile examination centers or in the home. The NHANES design includes an over-sampling of minority, low-income, and elderly individuals. Because of this complex sampling design appropriate weighting factors (based on statistical stratification and population estimates) must be taken into account when calculating population-based frequency estimates. In the NHANES 99-00, 5733 adults aged 17 years or older were interviewed and examined. By race/ethnicity, this population contains 2024 Hispanic individuals, 2414 non-Hispanic whites, 1129 non-Hispanic blacks, and 166 others. We limited our sample for this analysis to adults who had serum drawn for highly sensitive CRP (n = 4900). For analyses involving measurements of serum insulin or glucose we used the morning subsample of fasting individuals (n = 2109). Details about the specific methods used in the laboratory procedures of the NHANES 99-00 are available on the NHANES web site (www.cdc.gov/nchs/nhanes.htm) and elsewhere [13, 14].
Elevated CRP was defined using cutoff points based on previous studies of CVD. Our purpose was to use threshold levels that have clinical meaning as predictors of CVD and cardiovascular events. Recently published American Heart Association guidelines [1] have designated CRP levels greater than 3.0 mg/l as high and associated with increased cardiovascular risk. Therefore, in the current study, we considered values above 3.0 mg/l as being elevated.
Homocysteine levels greater than 10 μg/l [15] and fasting insulin levels greater than 12.2 μU/ml [16] were considered elevated. The homeostatic model assessment (HOMA) of insulin sensitivity was calculated from values of fasting glucose (mg/dl) and insulin (μU/ml): HOMA = (insulin ∗ glucose)/405.
HOMA values greater than 4.0 indicated insulin insensitivity [17].
A series of questions in the NHANES were used to determine whether a participant had a history of medical conditions. These questions were: ‘Has a doctor ever told you that you had (diabetes, hypertension, congestive heart failure, coronary heart disease, angina/angina pectoris, heart attack, or stroke?)'. Individual answers were used to determine a history of diabetes, hypertension, heart failure, heart attack (MI), or stroke. A positive response to any of these conditions (except diabetes and hypertension) was used to determine a history of general CVD (any CVD).
Obesity was defined as a body mass index (BMI) greater than 30 kg/m2. Elevated cholesterol was defined as a level greater than 200 mg/dl. Exercise levels were determined from questions asking whether an individual had participated in moderate or vigorous exercise during the previous 30 days. Dietary fiber intake was calculated from a 24-h dietary recall.
Data analysis
Because NHANES 99-00 was a complex, stratified cluster sample, standard statistical techniques could not be used. Therefore, we used SUDAAN (Research Triangle Institute, Research Triangle, North Carolina, USA), a specialized statistical program that accounts for the complex weighting of the NHANES 99-00 sample. Using SUDAAN allowed us to correct for unequal probabilities of selection and different response rates, ensuring that the results can be generalized to the non-institutionalized civilian population of the United States. The percentages and odds ratios in this study thus represent weighted values. SUDAAN also adjusts the standard errors to account for the weighting, stratification, and clustering of the complex sampling design, to ensure that expressed P values are valid. A separate set of weighting values were used in analyses employing the morning subsample population from which fasting glucose and insulin were measured.
Descriptive characteristics of the US population were calculated with regards to elevated CRP, homocysteine, HOMA, or insulin. For the total US population and for the sub-populations who had elevated serum markers, the population distributions based on age group, race, sex, BMI, current smoker, total cholesterol level, diabetes history, hypertension history, exercise, or dietary fiber intake were calculated. In addition, for each of these demographic factors, the percentage that had elevated serum markers was calculated. The X2 statistics were calculated for each of these percentage distributions to determine the significance of the distribution when compared with the total US population.
Logistic regression models were used to examine the univariate relationships between elevated serum biomarkers (CRP, homocysteine, HOMA, or insulin), singly or in combination with CRP, and having a history of heart failure, MI, stroke, or any CVD. The relative likelihood (odds ratio) of having each medical history was calculated for each serum biomarker. To explore further the relationships between serum biomarkers and medical histories, multivariate analyses were performed with the inclusion of control variables: age group, race, sex, obesity, smoking, cholesterol level, diabetes history, hypertension history, exercise level, and dietary fiber intake.
Results
Compared with the general US population, individuals with elevated CRP, homocysteine, HOMA, or fasting insulin levels were significantly more likely to be older, have elevated cholesterol, have a history of diabetes or hypertension, and to exercise less (Table 1). In addition, individuals with elevated CRP were more likely to be female, obese, and eat less fiber than the general US population. Individuals with elevated homocysteine were more likely to be male. In contrast, for individuals with elevated HOMA or insulin, gender was not a significant factor, but race and BMI were. Individuals with elevated HOMA or insulin were more likely to be black or Hispanic and obese.
A greater percentage of older participants had elevated serum biomarkers than younger participants (Table 2). Although there was no significant difference in the rates of elevated CRP or homocysteine by race, blacks and Hispanics had significantly greater rates of elevated HOMA and insulin. Obese individuals (BMI >30) were more likely to have elevated levels of CRP, fasting insulin, or HOMA than non-obese individuals (BMI >30). Current smoking was not related to an elevation of any of these serum markers. Individuals with elevated cholesterol, a history of diabetes, a history of hypertension, or who exercise less were more likely to have elevated serum biomarkers. The percentage of individuals with elevated CRP decreased significantly with each quartile increase in fiber consumption, but this trend did not hold for homocysteine, HOMA, or fasting insulin.
Population distribution (%) of demographic characteristics within each elevated serum marker group
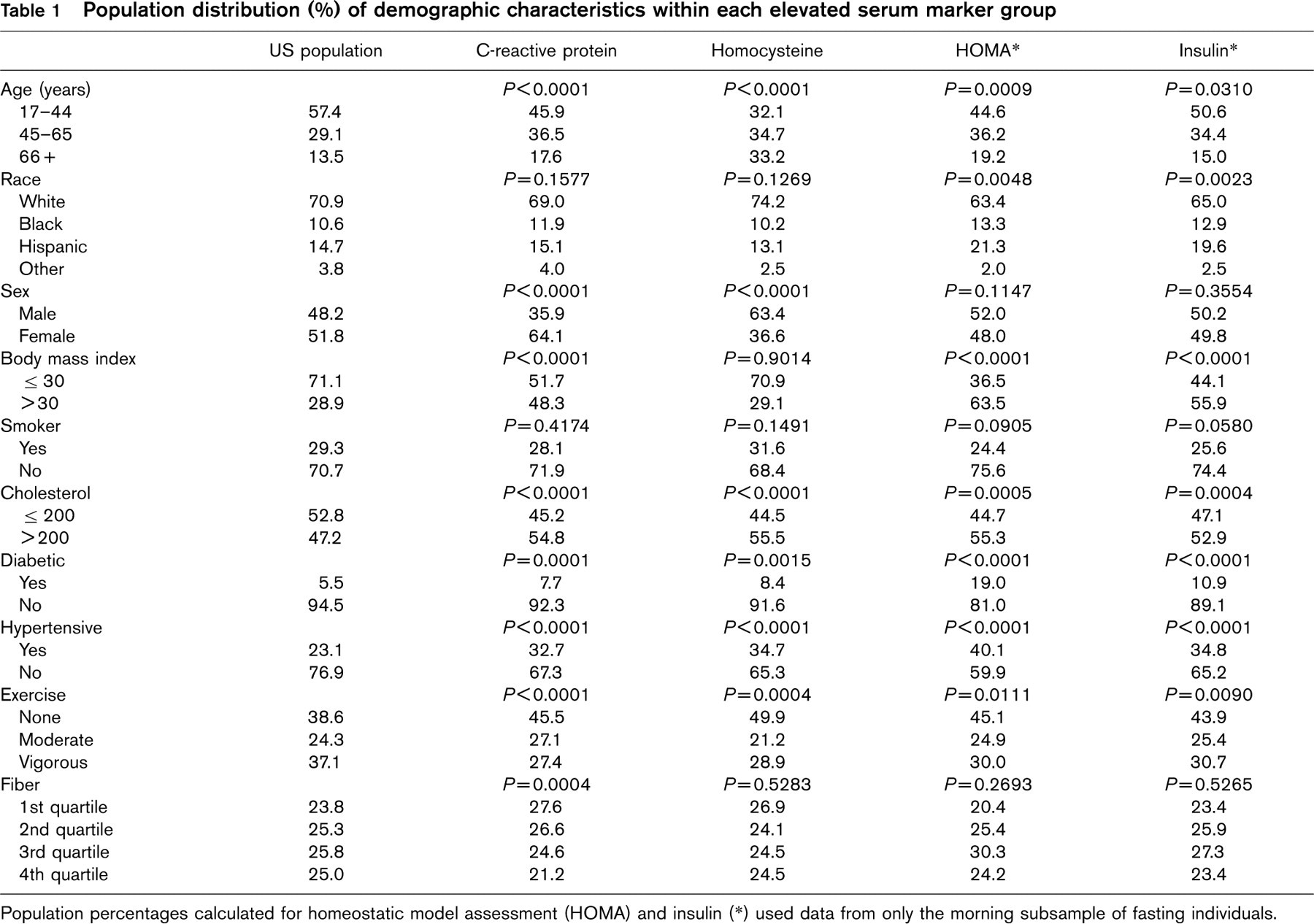
Population percentages calculated for homeostatic model assessment (HOMA) and insulin (∗) used data from only the morning subsample of fasting individuals.
Percentage of each population group with elevated serum markers
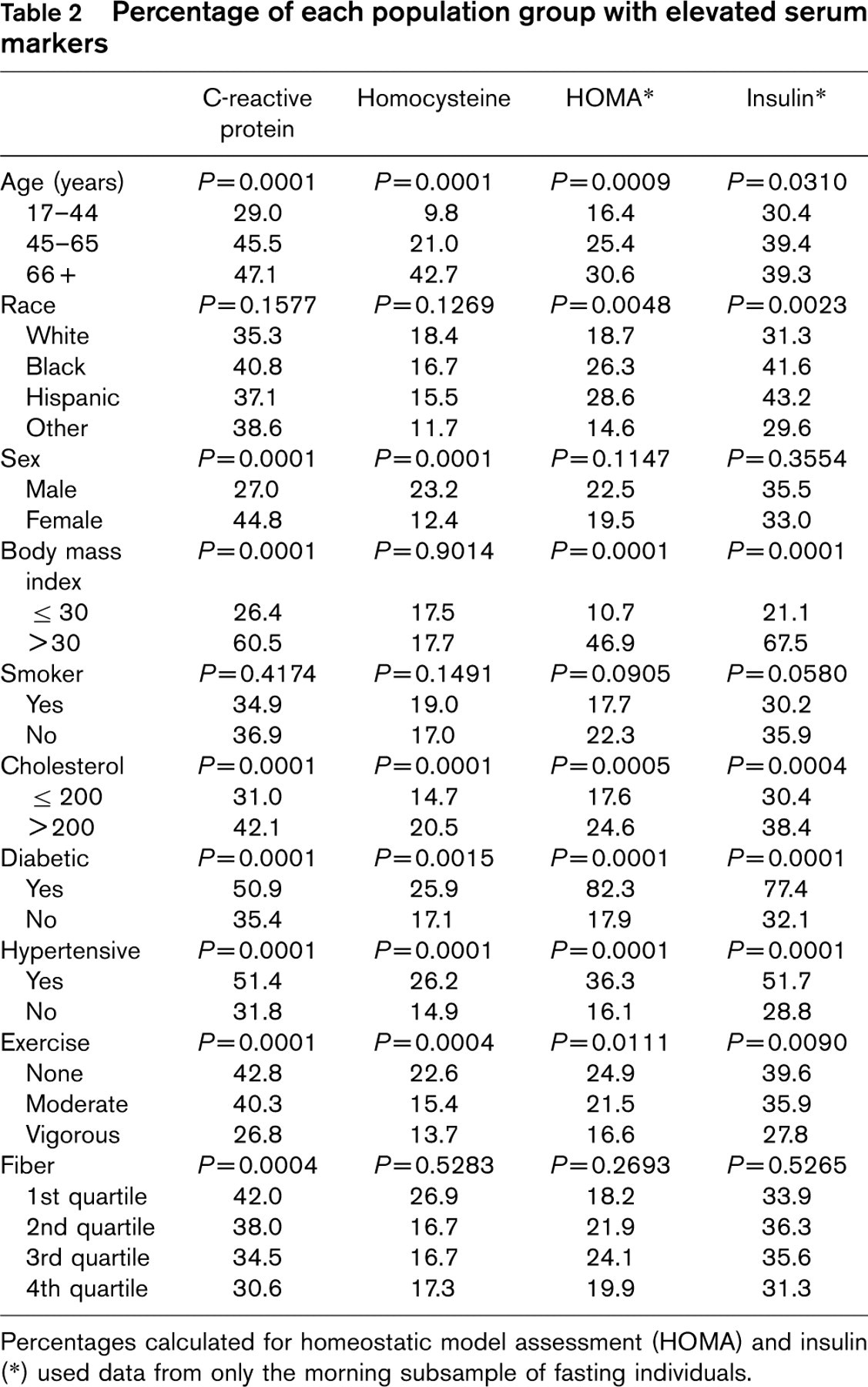
Percentages calculated for homeostatic model assessment (HOMA) and insulin (∗) used data from only the morning subsample of fasting individuals.
In unadjusted (univariate) analyses, individuals with an elevated serum biomarker, singly or in combination with CRP, were significantly (P<0.05) more likely to have a history of heart failure, MI, stroke, and any CVD than individuals without the elevated biomarker(s) (Table 3). The combination of having both CRP and homocysteine elevated consistently showed the strongest association with CVD histories.
After adjustment for age, race, sex, obesity, smoking, cholesterol, diabetes history, hypertension history, exercise, and dietary fiber consumption, the combined elevated CRP plus homocysteine odds ratios remained significant for heart failure, MI, and any CVD. In addition, elevated insulin and the combinations of elevated CRP plus HOMA and CRP plus insulin remained significantly related to having a history of any CVD. Elevated CRP plus insulin was also significantly related to a history of stroke.
Results of the univariate and multivariate logistic regression analyses
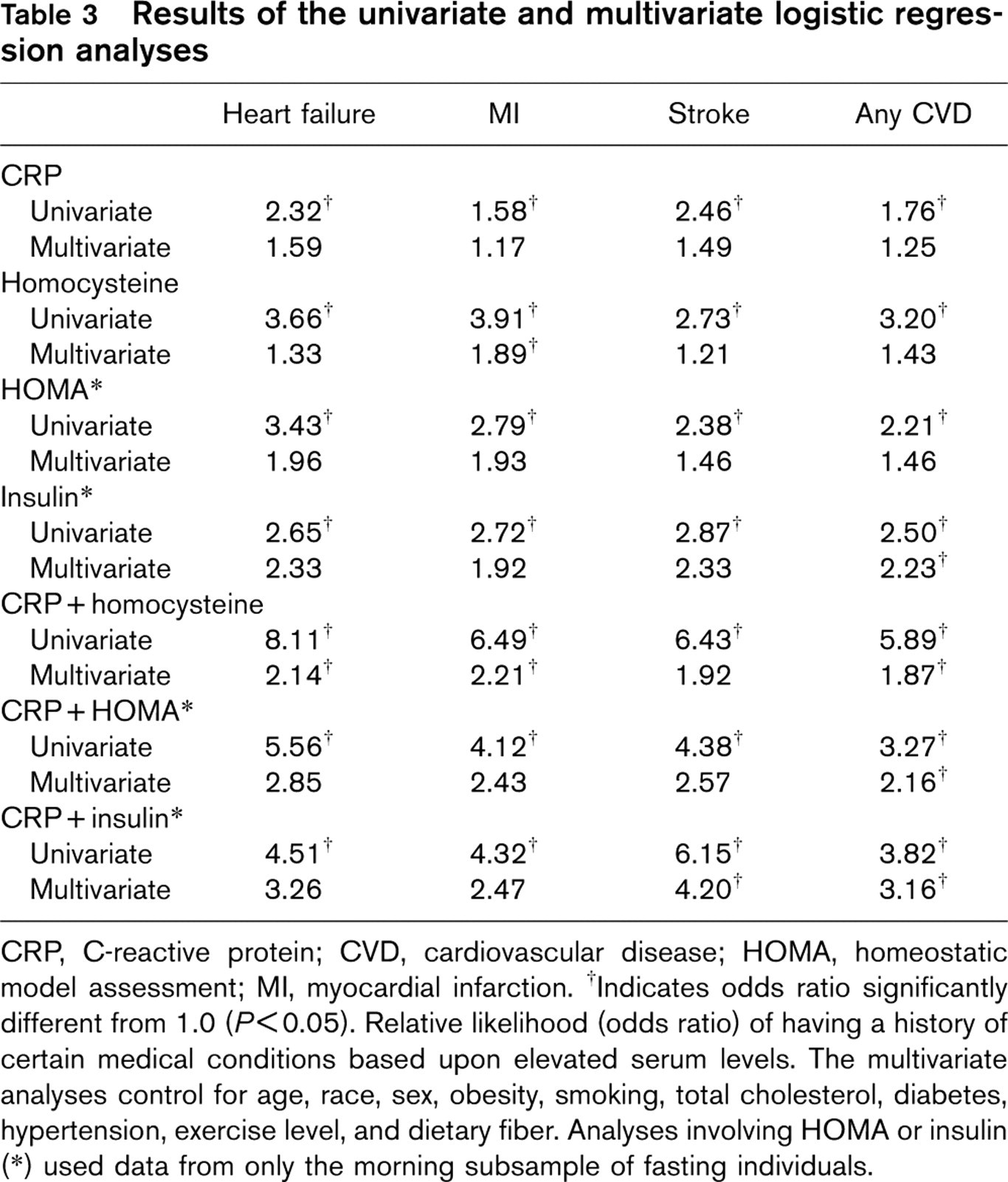
CRP, C-reactive protein; CVD, cardiovascular disease; HOMA, homeostatic model assessment; MI, myocardial infarction. †Indicates odds ratio significantly different from 1.0 (P<0.05). Relative likelihood (odds ratio) of having a history of certain medical conditions based upon elevated serum levels. The multivariate analyses control for age, race, sex, obesity, smoking, total cholesterol, diabetes, hypertension, exercise level, and dietary fiber. Analyses involving HOMA or insulin (∗) used data from only the morning subsample of fasting individuals.
Discussion
In this study, combined serum biomarkers, especially CRP with homocysteine, were more strongly associated with CVD outcomes than individual biomarkers. Elevated CRP combined with elevated homocysteine remained significantly associated with a history of MI, heart failure, and any CVD, even after adjustment for demographic and cardiovascular risk factors.
The implications of this study are that combining CRP and homocysteine may provide important new information for the assessment of cardiovascular risk. The strong association of the combined elevation of CRP and other serum biomarkers with current CVD, even after controlling for other CVD risk factors, demonstrates the potential utility of this relationship. The CRP plus homocysteine combination was the strongest of the combined factors, and would be the most promising to evaluate in prospective studies.
The utility of combining serum biomarkers in risk assessment is an important area for study, because the elevation of single markers such as CRP explain only a small portion of total cardiovascular risk [12]. There is an ongoing debate regarding whether CRP adds significantly to the predictive ability of risk factors that are routinely collected in clinical practice, such as BMI, cholesterol, and hypertension. A recent meta-analysis [12] compared individuals in the lowest tertile of highly sensitive CRP with those in the upper tertile for the prediction of major coronary events, and found a relative odds ratio of 1.9 (95% confidence interval, 1.7–2.2). After adjustment for other known risk factors, including age, cholesterol level, smoking, BMI, history of diabetes, hypertension, exercise level, and family history of coronary disease, the predictive capacity of highly sensitive CRP is attenuated, and in some cases lost [1, 12, 18].
A few previous studies have examined the ability of CRP and another marker in combination. For example, Ridker and colleagues [19] evaluated the predictive capacity of elevated highly sensitive CRP and the low-density lipoprotein (LDL)-cholesterol level and found that, although each marker is independently associated with increased CVD, when both are elevated, the combined risk is even greater than with either alone. However, recent guidelines by the American Heart Association [1] have not recommended screening people for CRP unless they are already known to be at intermediate cardiovascular risk as a result of the relatively lower predictive ability of elevated CRP alone. Other researchers [20] have evaluated CRP in combination with markers of insulin sensitivity, and have found that prediabetic individuals with more insulin resistance are more likely to have elevated levels of CRP. In our study, this combination was not as strongly associated with CVD as CRP plus homocysteine.
Determining which combinations of serum markers would be best is a challenging clinical question. The best markers would be highly associated with the clinical CVD outcomes of interest, be widely available, and be complimentary. For these reasons, we chose to evaluate markers of inflammation, atherosclerosis, and insulin sensitivity. The positive findings in our study, showing a strong association between such markers and CVD outcomes, and even stronger association when markers are combined, lend support to the concept that combining serum biomarkers may be a useful approach in CVD risk stratification.
The physiological explanation behind our findings is in the process of being elucidated. The vascular endothelium is an active, dynamic tissue that controls many important functions, including the regulation of vascular tone and the maintenance of blood circulation, fluidity, coagulation, and inflammatory responses [21]. Cardiovascular risk factors affect many of the normal functions of the endothelium. In particular, oxidized LDL-cholesterol initiates a series of events that begin with cell activation, endothelial dysfunction, local inflammation, and a procoagulant vascular surface. These conspire to result in plaque formation and ultimately plaque rupture and cardiovascular events. Endothelial dysfunction has been evaluated using a variety of techniques, such as coronary artery reactivity to acetylcholine, or arterial ultrasonography. The loss of endothelium-dependent vasodilation is a characteristic feature throughout the development of atherosclerosis, and it is independently related to future adverse cardiovascular risk. Therefore, the measurement of markers that reflect endothelial function would be the logical choice to be used to determine risk, to triage management, and to improve outcomes. At the same time, inflammation is a crucial factor in the atherosclerotic disease process. To identify and monitor the ongoing inflammatory process, CRP has been identified by the American Heart Association [1] as the best indicator.
Limitations of this study include the fact that the NHANES is a cross-sectional assessment and no long-term follow-up to observe actual cardiovascular outcomes is possible. Likewise, CVD are self-reported and do not represent actual clinical findings based on patient examination. Despite the methodological concerns, the large size and representative nature of this national sample make the NHANES dataset an invaluable tool for exploring new relationships that require subsequent clinical evaluation. In this regard, the present study raises an important issue about the potential benefit of combining serum biomarkers to improve cardiovascular risk stratification. Because sudden death remains the presenting symptom of CVD in a disturbingly high percentage of patients, innovative methods are needed to improve risk stratification. Our findings suggest that a combined assessment of CRP and homocysteine may provide an improved method of risk stratification. However, further research is needed to clarify the exact value of this strategy, relative to or in addition to the use of more traditional means of cardiovascular risk stratification using lipids, blood pressure, etc.
In conclusion, the combination of serum biomarkers, in particular the combination of CRP and homocysteine, has a stronger association with self-reported CVD than the individual markers alone. Recent scientific evidence and our current study findings support the next step, which is to explore the combination of CRP and homocysteine prospectively as predictors of CVD outcomes.