
Abstract
Background
Survival of a myocardial infarction and subsequent prognosis are highly dependent on the time between onset of symptoms and medical intervention.
Design
This cross-sectional study examines whether patients who used the psychological defence mechanism of denial when faced with symptoms of a first-time myocardial infarction tended to also show a prolonged delay in going to the hospital and to be less willing to participate in a cardiac rehabilitation programme.
Methods
One hundred and seven patients, 78 men and 29 women, were enrolled in this study. The sample was divided into two groups depending on whether the patients sought medical help within 4h after they began experiencing myocardial infarction symptoms (non-delayers) or whether they waited longer (delayers). Denial was measured with the Hackett and Cassem semi-structured interview 3–5 days after the patients entered the hospital. Data on participation (attenders) or not (non-attenders) in the rehabilitation programme was also obtained.
Results
Forty-nine patients exhibited a prolonged delay and 76 patients did not attend the rehabilitation programme. Both prolonged delay and a lesser readiness to attend the rehabilitation programme that was offered were related to a greater use of denial. In addition, the great majority of the patients categorized as being high deniers were found to also be both delayers and non-attenders.
Conclusions
The results suggest denial to increase the health risks of persons potentially prone to myocardial infarction. If our knowledge about this psychological defence mechanism is increased, we might be able to reach more patients in alternative and individually based cardiac rehabilitation programmes.
Introduction
A prolonged delay time, in most studies defined as more than 4 h from onset of symptoms of myocardial infarction (MI) to seeking medical assistance, can have life-threatening consequences and is a major determinant of the prognosis in acute MI [1–6. A number of factors have been found to be associated with prolonged delay. These include female sex, advanced age, a history of diabetes, and living alone [2,5–7]. Research also suggests that prolonged delay is related to the patient's beliefs that the symptoms are neither serious nor cardiac-related, such as ‘it was nothing serious', ‘the symptoms will go away', or ‘symptoms are not clear enough to justify calling for an ambulance’ [4,8–11]. Failure to recognize or to correctly appraise the significance of MI symptoms thus appears to be a major cause of delay. It has become increasingly evident that psychological factors can contribute to a delay of this sort. Denial, perhaps the most commonly used psychological mechanism for coping with serious threats and with strong emotional stress, is one such factor.
The present study examines the extent to which individuals, who when faced with an acute first-time MI, exhibit denial – such as projecting their fears onto others (e.g. ‘I'm not worried but my wife is'), minimizing the seriousness of their health condition, or displaying omnipotence regarding their mastery of the situation – tended to also show a delay in taking the steps needed to be sent to the hospital. Since inadequate coping of this type could also be thought to have a negative impact on the patient's readiness to adhere to principles conducive to maintaining health, the study also investigates whether patients who show denial tend to be less willing than those who do not employ coping of this sort, to participate in a cardiac rehabilitation programme that was offered to all MI patients.
Methods
A total of 107 consecutively admitted patients stricken with MI were enrolled in this study at two participating hospitals in southern Sweden. The research protocol was approved by the local ethics committee and written informed consent was obtained from all the patients. Patients were eligible for inclusion if they had been hospitalized for an acute MI in the preceding 3 days. The occurrence of MI was considered confirmed if symptoms met the criteria of the World Health Organization and if the event was associated with increased levels of troponin T and diagnostic electrocardiographic criteria. They were ineligible for the study if they were more than 70 years of age, had a history of previous MI, of percutaneous coronary intervention or coronary artery bypass surgery, of a coexisting condition that shortened expected survival to a period of less than 12 months, of drug or alcohol abuse or of poor mental function. A measure of delay in going to the hospital was obtained by asking patients how long a time had elapsed after they had begun experiencing the symptoms connected with their MI until they had sought medical help. In line with Ruston et al. [12], the sample was divided into two groups, depending on whether the patients sought medical help within 4h after they began experiencing MI symptoms (non-delayers) or whether they waited longer (delayers). To rule out the possibility of social desirability – a tendency to answer in such a way as to give a good impression, having biased self-reported delay-time – this variable was assessed by use of the Crowne Marlowe scale [13]. Denial was measured using the Hackett and Cassem [14] semi-structured interview given 3–5 days after admission to hospital. This semistructured interview assesses denial with questions about the typical way the patient copes with life's difficulties and about how the patient perceives and reacts to the current illness situation. It includes such variables as acknowledging fear and worry, inclination to take risks and accept challenges, having a superficially jovial attitude toward life, minimizing the reporting of symptoms, and the absence of fear of death, of re-infarction or invalidism. Higher scores indicate stronger denial. In order to examine the internal consistency of the Hackett and Cassem interview instrument, a Cronbach's α coefficient was calculated for the total study group. This analysis showed a satisfactory internal consistency, with a Cronbach's α coefficient of 0.74. At a 2-week follow-up visit, the patients were invited to participate in a cardiac rehabilitation programme started approximately 1–2 months after they had left the hospital. One part of the programme consisted of education (group and individually based) focusing on risk factor modification, such as smoking cessation, stress management training, cholesterol lowering and weight reduction. Another part of the cardiac rehabilitation programme, conducted once a week by a physiotherapist, involved aerobic cardiovascular training. Data on the patients’ participation in this cardiac rehabilitation programme was obtained. At that time, two patients had died.
Statistics
Means, medians, standard deviations, ranges, Student's two-tailed t-tests, and χ2 tests were calculated. One-way analysis of variance, η2 squared, and the Tukey HSD test for pairwise comparisons of means were also carried out. Data analyses were run on SPSS 11.5 (SPSS, Chicago, Illinois, USA).
Results
The 107 patients ranged in age from 38 to 70 years (mean age 59.1 years, SD 7.1). Seventy-eight were men (mean age 58.7 years, SD 7.1) and 29 were women (mean age 60.1 years, SD 7.1).
Fifty-eight patients contacted medical services within 4h, thus being classified as non-delayers, whereas 49 patients waited for more than 4h (delayers). No significant difference was obtained between the non-delayers and the delayers in terms of their scores on the Crowne-Marlowe social desirability scale [means 19.3 ± 5.4 (SD) versus 18.1 ± 4.6 (SD); t (104) = 1.19; P > 0.05].
There were 29 patients who participated in the cardiac rehabilitation programme (attenders) and 76 who did not (non-attenders). Scores on denial, as measured by the Hackett and Cassem denial interview, ranged from five to 34 (mean 15.0, median 14.0, SD 5.8). The delayers displayed higher denial scores than the non-delayers [means 17.5 ± 5.9 (SD) versus 12.9 ± 4.7 (SD); t (105) =4.44; P < 0.001] and the non-attenders showed higher denial scores than the attenders [means 16.0 ± 5.8 (SD) versus 12.8 ± 5.0 (SD); t (103) = 2.7; P < 0.01].
Denial scores
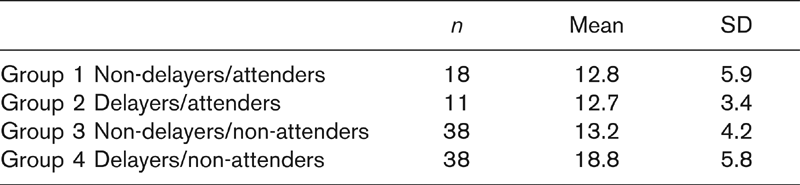
In order to examine certain correlates of the denial scores, four groups were created: (1) attenders/non-delayers, (2) non-attenders/non-delayers, (3) attenders/delayers, (4) non-attenders/delayers. A one-way between-groups analysis of variance showed statistically significant differences between the four groups in their denial scores [F (3, 101) = 10.8; P < 0.001]. The effect size in terms of η2 was 0.24. Post-hoc comparisons, using the Tukey HSD test, showed the scores for group four to be significantly higher than those of the three other groups (Table 1).
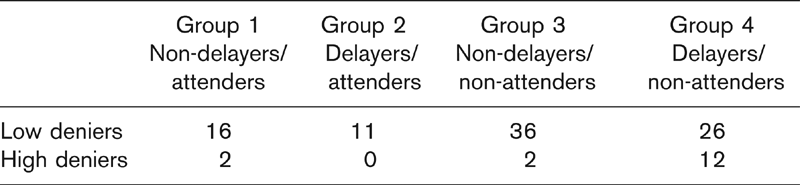
In accordance with a study of Levenson et al. [15], a denial score of 22 or more was used to categorize patients as high deniers, and a score of 21 or less categorized low deniers. It was found that 12 of the 16 patients, who belonged to the group of high deniers, and thus a clear majority of them, were both delayers and non-attenders (Table 2). Comparing in this respect group 4 with the other three groups (considered as a whole) showed high deniers to be significantly more frequent in group 4 than in the three other groups (χ2= 12.31; df 1; P < 0.001).
Since the results of others [2,5–7] have shown female sex, advanced age, a history of diabetes, and living alone to be related to prolonged delay, relations of these variables to the delay variable were examined; there were 21 patients who had diabetes mellitus and 15 patients who lived alone. The only significant relationship found was that the delayers were somewhat younger than the non-delayers [mean 57.6 ± 7.3 versus mean 60.4 ± 6.6, t(105) = 2.03; P < 0.05]. An analysis of variance between the four groups described in Table 1 and a t-test between group 4 and the other three groups (considered as a whole) presented in Table 2, however, did not reveal any significant age differences.
Discussion
In this exploratory study, we examined possible associations between delay presentation following a first-time MI, attendance at a cardiac rehabilitation programme, and the patients’ use of the psychological defence mechanism denial. In line with results of others [3–5, approximately 45% of our sample was found to delay 4h or more after the onset of MI symptoms before seeking medical assistance. Both prolonged delay and a lesser readiness to attend a later cardiac rehabilitation programme that was offered were related to a greater use of denial. In addition, the great majority of the patients categorized as being high deniers were found to also be both delayers and non-attenders.
Occurrence of low versus high deniers
Using denial as a defence mechanism has long been recognized as one of the primary ways in which individuals cope with threats and high levels of emotional stress [16,17]. Although benefits of this sort of coping have been noted [15], the costs are unambiguously harmful and even fatal when one is stricken with an acute MI, since denial increases the risk to overlook significant signs and thus to evade suitable actions, specifically seeking medical care, as O'Carroll [18] likewise found to be the case in a sample of MI patients. Moreover, since this defence mechanism is quite stable over time, the patient may lack insight into the situation, fail to adhere to medical recommendations, and may be unable to adequately handle later problems that arise in connection with the illness. For example, in a mixed group of patients hospitalized for either MI or coronary bypass surgery, high deniers were found to be more non-compliant with medical recommendations [19]. Also, in a group of male patients admitted after their first MI, denial – specifically denial of responsibility – was found to be negatively related to both short and long-term recovery measures [20].
In the view of results showing that one to two-thirds of MI cases that occur are fatal prior to hospitalization and also that most of the deaths take place within 4 h of the onset of acute symptoms [1,21], attempts to identify patients who tend to delay and modify beliefs that contribute to prolonged delay are highly important both for those at a high risk of being stricken by an acute first-time MI and for those at risk for a re-infarction, the latter in the light of results showing previous experience of MI not necessarily leading to a reduction in delay time [22]. It is highly important too that family members and significant others are being told to expect denial, are helped to understand that denial is a common reaction, and are made familiar with the diversity of symptoms, so as to be able to help the patient decide in time to seek emergency care.
In conclusion, high denial scores, found in a substantial number of patients with a first-time MI, were significantly associated with long delay before seeking medical assistance as well as unwillingness to attend the hospital-based rehabilitation programme. If our knowledge about this psychological defence mechanism is increased, we might be able to reach more patients in alternative and individually based cardiac rehabilitation strategies.