
Abstract
Background
It has been shown that acute intake of red wine improves endothelial-dependent vasodilatation. It is not clear, however, which constituents of red wine are responsible for this effect. We examined whether acute intake of a red grape polyphenol extract has a positive effect on brachial artery flow-mediated dilatation.
Methods
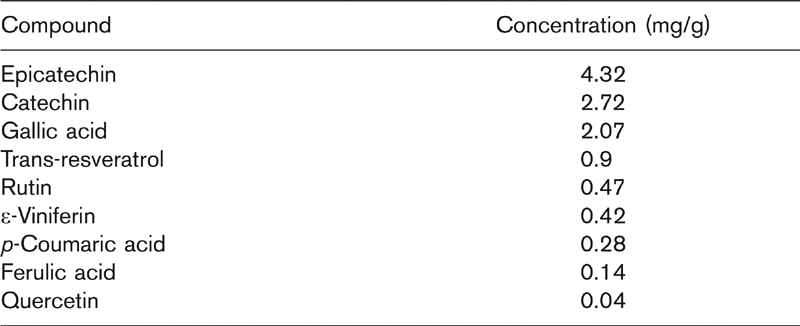
We recruited 30 male patients with coronary heart disease. They were randomly assigned either to a red grape polyphenol extract (600 mg) dissolved in 20 ml of water (n = 15) or 20 ml of water (placebo) (n = 15). The extract of grapes contained 4.32 mg epicatechin, 2.72 mg catechin, 2.07 mg gallic acid, 0.9 mg trans-resveratrol, 0.47 mg rutin, 0.42 mg ε-viniferin, 0.28 mg, p-coumaric acid, 0.14 mg ferulic acid and 0.04 mg quercetin per gram. Flow-mediated dilatation of the brachial artery was evaluated after reactive hyperemia induced by cuff obstruction of the forearm, using high-resolution ultasonography. Particularly, flow-mediated dilatation was measured after fasting and 30, 60 and 120 min after the intake of the grape extract or placebo.
Results
Intake of the red grape polyphenol extract caused an increase in flow-mediated dilatation, peaking at 60 min, which was significantly higher than the baseline values (4.52 ± 1.34 versus 2.6 ± 1.5%; P < 0.001) and the corresponding values at 60 min after the intake of placebo (4.52 ± 1.34 versus 2.64 ± 1.8%, P < 0.001). There was no change in FMD values after the intake of placebo throughout the whole duration of the study.
Conclusion
Polyphenolic compounds from red grapes acutely improve endothelial function in patients with coronary heart disease. These results could probably, at least partly, explain the favorable effects of red wine on the cardiovascular system.
Introduction
Several studies have suggested an inverse relationship between moderate alcohol consumption and coronary heart disease (CHD) [1]. The type of alcohol consumed has been proposed as a determinant of this relationship [2]. The ‘French paradox’ which refers to the lower CHD mortality in France than in other industrialized countries with a similar coronary risk factor profile, has been attributed to the higher consumption of red wine by the French [3,4]. There is no clear-cut evidence, however, showing whether red wine is more beneficial than other alcoholic beverages [1].
Red wine differs from other forms of alcohol by its higher content in polyphenols, which are important components of grape skins [5]. The concentration of polyphenols in red wine shows a great variation depending on the grape variety, the geographic origin and the wine-making process [6,7]. It has been proposed that polyphenols may contribute to the cardioprotective effect of red wine by preventing low-density lipoprotein oxidation [8], decreasing platelet aggregation [9,10] and improving endothelial function [10,11]. In addition, in-vitro studies [12,13] have suggested a potential anti-atherogenic effect of polyphenols by inhibiting the proliferation and migration of vascular smooth muscle cells while animal studies [14,15] have demonstrated inhibition of the atherosclerotic process.
It has been shown that acute intake of red wine improves endothelial-dependent vasodilatation in healthy subjects [16]. It is not clear, however, which exact constituents of red wine are responsible for this effect. In our study we tested the hypothesis that acute intake of a red grape polyphenol extract (RGPE) has a favorable effect on brachial artery flow-mediated dilatation (FMD) in patients with CHD.
Materials and methods
Subjects and study design
Thirty male patients with angiographically documented CHD were recruited. Exclusion criteria were age over 70 years, recent (<2 months) acute coronary syndrome or coronary artery bypass graft, and atrial fibrillation. They were randomly assigned either to a RGPE (600 mg) dissolved in 20 ml of water (n = 15) or 20 ml of water (placebo) (n = 15). Table 1 presents the main polyphenolic compounds of the extract. All patients gave their informed consent before entering the study.
Polyphenol extraction process
The polyphenol extract was prepared from the red grape Vitis vinifera variety mandilaria, collected in Santorini island, Greece in August 2003. After the removal of the juice during the wine-making process, the pomace was obtained and submitted to extraction. The pomace (4 kg) was air-dried and pulverized. The powder was extracted three times with ethanol (141 each time) for 48 h. The solvent was evaporated under reduced pressure at 45°C to give a semi-solid residue (130 g). A part of the residue (45 g) was dissolved in water, filtered and submitted to medium pressure liquid chromatography (RP-18 Si gel 60; Merck, Darmstad, Germany; 20–40 μmol/l), with water and ethanol as eluents. The water fraction (151) contained the majority of sugars and was rejected. The ethanol fraction (101) that contained the majority of the polyphenols was collected and evaporated. The dry purified extract (15 g) was mixed with maltodextrine (ratio 1:3) that was used as an inert carrier. The mixture was dissolved in water and freeze-dried. The final red powder was divided into 25 doses each containing 600 mg of extract and 1.8 g of maltodextrine. The consumption of one dose corresponded to the consumption of 1 kg of grapes based on the concentration of trans-resveratrol.
Main polyphenolic compounds of the extract of red grapes
Measurement of brachial artery endothelial function
FMD and nitroglycerin-induced dilatation of the brachial artery were evaluated by a single examiner blinded to the type of ingestion according to the method described previously [17,18]. All studies were performed in the morning after overnight fasting and discontinuation of nitrates 24 h before the test. After resting in a supine position for 10 min the diameter of the right brachial artery and baseline forearm blood flow were measured with an ultrasound machine (ATL HDI 3500, Bothell, Washington, USA) using a 7.5 MHz linear array transducer. Increased forearm blood flow was induced by inflating a pneumatic blood pressure tourniquet placed around the wrist to a systolic blood pressure of 250 mmHg for 5 min. Repeat blood flow scans were obtained immediately after cuff deflation and the brachial artery was scanned continuously for 120 s thereafter and its maximum diameter was defined. The same procedure was repeated 30, 60, and 120 min after drinking the beverage. Ten minutes were allowed for vessel recovery and analogous measurements were obtained before and 3 min after the administration of sublingual nitroglycerin (400 μg). The patients remained in the supine position throughout the whole test. FMD was defined as the percentage change of the artery's diameter (endothelial-dependent vasodilation) and hyperemia as the percentage increase of flow (at each time point of the study). Similar measurements were also performed before and after the administration of nitroglycerin. The interobserver and intraobserver variability for brachial diameter measurements in our laboratory is 0.1 ± 0.12 mm and 0.08 ± 0.19 mm, respectively.
Statistical analysis
Data are expressed as mean ± SD. Variables between the two studied groups were compared using t test. For repeated measurements analysis of variance was applied followed by post-hoc Bonferroni's correction in order to evaluate differences of repeated measurements within each group. Homogeneity of variances was tested using Levene's test. A P value under 0.05 was considered statistically significant.
Results
The two studied groups (RGPE versus placebo group) were comparable regarding age (59.7 ± 9.3 versus 62.2 ± 8.6 years; P, NS), number of diseased vessels (2.1 ± 0.95 versus 2.3 ± 0.95; P, NS), ejection fraction (53.3 ± 17 versus 52.4 ± 14.7%; P, NS), lipids and cardiovascular risk factors (Table 2) and type of medication (Table 3). Baseline artery diameter, baseline FMD, and flow at rest and hyperemic response did not differ significantly between the two groups (Table 4). After the ingestion of the RGPE there was an increase in FMD throughout the study which peaked at 60 min and was significantly higher at that stage from the baseline level (P < 0.001) (Table 4). In addition, the 60min value of FMD after the ingestion of the RGPE was higher than the corresponding value at 60 min after the intake of water (P < 0.001) (Fig. 1). There was no change in brachial diameter before cuff inflation throughout the study. After the ingestion of water there were no significant changes in FMD or hyperemic response at 30, 60 or 120 min. Finally, nitroglycerin-mediated dilatation was similar in both groups (8.4 ± 3.6 versus 8.5 ± 3.2%; P NS).
Lipids and cardiovascular risk factors in the studied subgroups
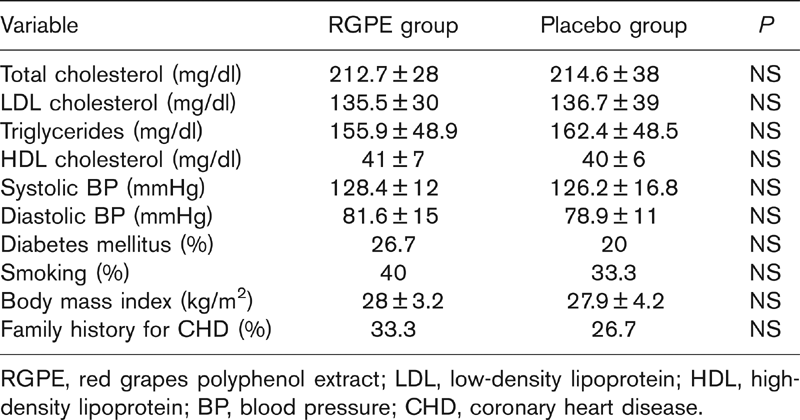
RGPE, red grapes polyphenol extract; LDL, low-density lipoprotein; HDL, high-density lipoprotein; BP, blood pressure; CHD, coronary heart disease.
Medication in the studied subgroups
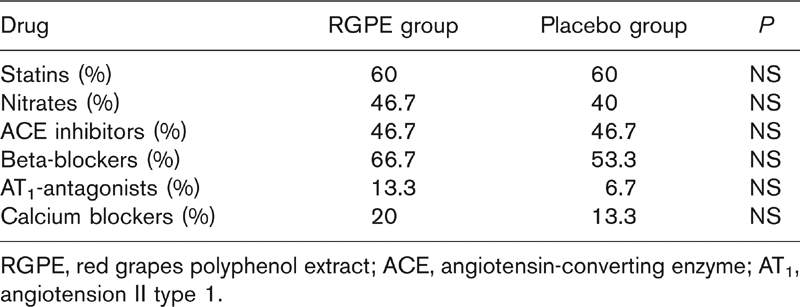
RGPE, red grapes polyphenol extract; ACE, angiotensin-converting enzyme; AT1, angiotension II type 1.
Vessel diameter at rest, flow at rest, hyperemia and flow mediated dilatation at baseline and after the ingestion of the extract of red grapes or placebo
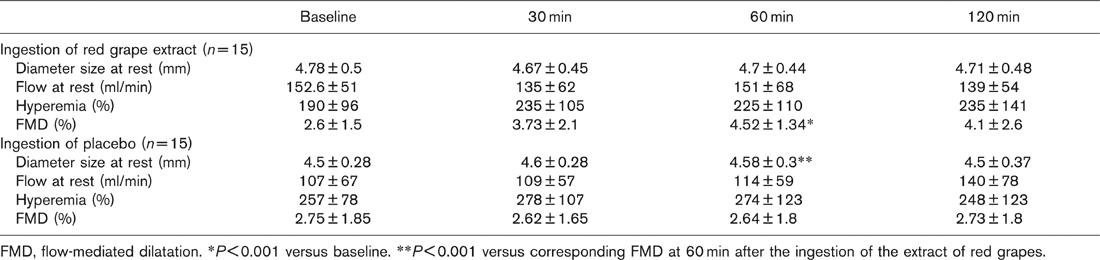
FMD, flow-mediated dilatation. ∗P < 0.001 versus baseline. ∗∗P < 0.001 versus corresponding FMD at 60 min after the ingestion of the extract of red grapes.
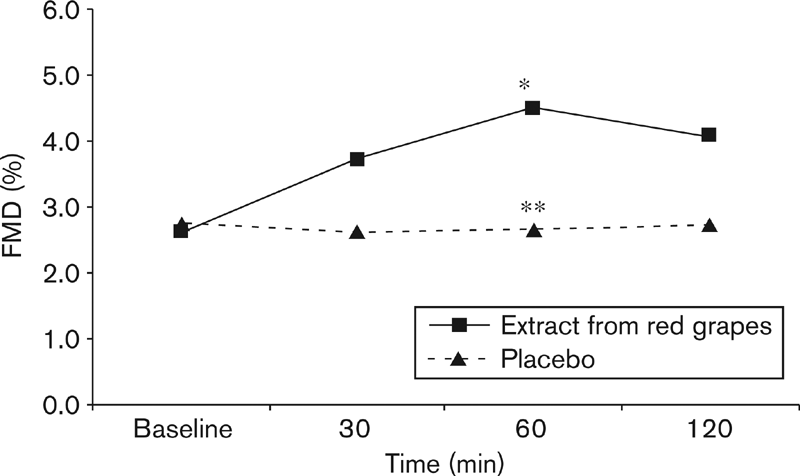
Flow-mediated dilatation (FMD) at baseline, 30, 60, and 120 min after the ingestion of the extract of red grapes or placebo. ∗P<0.001 versus baseline; ∗∗P<0.001 versus corresponding FMD at 60 min after the ingestion of the extract of red grapes.
Discussion
The presented data show that polyphenols obtained from red grapes improve FMD acutely in men with documented CHD. This is the first study to confirm this favorable effect by the consumption of a red grape extract with polyphenols being the only active components.
Previous studies indirectly proposed the same effect of polyphenols on endothelium. It was shown that acute ingestion of de-alcoholized red wine increases FMD in healthy subjects and it was hypothesized that the nonalcoholic components of red wine, most likely polyphenols, are responsible for this effect [16, 18,19]. In another study [20] short-term ingestion of purple grape juice, rich in flavonoids (polyphenol derivatives), improved FMD and reduced susceptibility of low-density lipoprotein to oxidation in CHD patients. In-vitro data suggest that the effect of purple grape juice on endothelial function may be mediated through the production of nitric oxide [11, 21,22]. It has been proposed that the critical step for the activation of nitric oxide synthase is the increase of intracellular free calcium [23]. Recently, incubation of porcine coronary artery with red wine polyphenols increased formation of nitric oxide by redox-sensitive PI3-kinase/Akt-dependent phosphorylation of the endothelial nitric oxide synthase [24].
The grape extract that we provided contained mainly epicatechin, catechin, gallic acid, trans-resveratrol, rutin, ε-viniferin, p-coumaric acid, ferulic acid and quercetin. From these compounds, catechin, trans-resveratrol, and quercetin have been studied more extensively due to their powerful antioxidant effect against low-density lipoprotein oxidation in vitro [25]. Leikert et al. [11] suggested that resveratrol was the only compound from an alcohol-free red wine polyphenol extract that could enhance endothelial nitric oxide synthase in vitro. In another study [26] administration of resveratrol to hypercholestelolemic rabbits for 12 weeks improved FMD, decreased endothelin and increased nitric oxide levels. In addition, resveratrol and quercetin could inhibit platelet aggregation and synthesis of procoagulant and proinflammatory eicosanoids in vitro [27]. Finally, the administration of catechin, quercetin and resveratrol to hypercholesterolemic hamsters efficiently protected against aortic fatty streak accumulation [28].
In our study the increase in FMD started 30 min and peaked 60 min after ingestion of the RGPE. This pattern of action could be nicely explained by the proposed absorption by Goldberg et al. [29] who tested the absorptive efficiency of catechin, trans-resveratrol, and quercetin. They found that the concentration of these compounds (free and conjugated) when given orally to healthy subjects peaked in serum around 30 min after consumption. The absorption of resveratrol was the most efficient with catechin being the poorest and quercetin intermediate. Furthermore, the duration of the observed favorable effect of RGPE on endothelium is in accordance with previous reports which showed that the maximum plasma antioxidant capacity is usually reached 1–4 h after the ingestion of the polyphenol source [30].
An issue raised by our study is whether the amount of polyphenols that we provided can be achieved by the usual dietary intake of grapes. The RGPE that was given in each subject was derived from 1 kg of red grapes, a quantity that is rather unusual to be consumed even from a person who follows a Mediterranean-type diet. Therefore, it will be interesting to consider in future the production of supplements containing polyphenols from red grapes, provided that their beneficial effect is confirmed by larger and long-term studies.
Moreover, it would be interesting to investigate the effect of the parallel consumption of RGPE with a high fat meal on FMD. It has been reported that a meal rich in fat acutely impairs endothelial function for up to 4 h [31] more severely in CHD patients [32]. This postprandial endothelial dysfunction has been attributed mainly to an augmentation of oxidative stress [33] and it has been shown that red wine consumption prevents this vascular oxidative stress [34,35]. Therefore, it will be challenging for future studies to explore whether the addition of RGEP to a high fat meal will attenuate or neutralize the postprandial endothelial dysfunction.
A limitation of our study is that we did not measure markers of oxidative stress, such as reactive oxygen species, or levels of serum antioxidants since a direct scavenging of free radicals by polyphenols has been proposed [30]. This could probably provide a more mechanistic insight into RGPE actions. Another potential limitation is related to the fact that the RGPE we used did not only contain the listed polyphenols in Table 1 but also few others, such as vanillic acid, syringic acid and protocatechuit acid which could have contributed to the observed effect on FMD. The very low concentration of these polyphenols, however, much lower than the listed polyphenols, minimizes this possibility. In addition, it should be noted that the RGPE also contained important quantities of sugars that had no effect on FMD.
In conclusion, polyphenolic compounds from red grapes acutely improve endothelial function in patients with CHD. This effect could probably explain, at least partly, the favorable effects of red wine on the cardiovascular system. The long-term effect of RGPE on endothelial function remains to be elucidated.