
Abstract
Background
Economic evaluation is an important tool in the evaluation of competing healthcare interventions. Little is known about the economic benefits of different cardiac rehabilitation program delivery models.
Design
The goal of this study was to review and evaluate the methodological quality of published economic evaluations of cardiac rehabilitation services.
Methods
Electronic databases were searched for English language evaluations (trials, modeling studies) of the economic impact of cardiac rehabilitation. A review of study characteristics and methodological quality was completed using standardized tools. All costs are adjusted to 2004 US dollars.
Results
Fifteen economic evaluations were identified which met eligibility criteria but which displayed wide variation in the use of comparators, evaluation type, perspective and design. Evidence to support the cost-effectiveness of supervised cardiac rehabilitation in myocardial infarction and heart failure patients was identified. The range of cost per life year gained was estimated as from $2193 to $28193 and from -$668 to $16118 per quality adjusted life year gained. The level of evidence supporting the economic value of home-based cardiac rehabilitation interventions is limited to partial economic analyses.
Conclusions
Evidence to support the cost-effectiveness of supervised cardiac rehabilitation compared with usual care in myocardial infarction and heart failure was identified. Further trials are required to support the cost-effectiveness of cardiac rehabilitation in cardiac patients who have under gone revascularization. The literature evaluating home-based and alternative delivery models of cardiac rehabilitation was insufficient to draw conclusions about their relative cost-effectiveness. The overall quality of published economic evaluations of cardiac rehabilitation is poor and further well-designed trials are required.
Keywords
Introduction
Economic evaluation is an important tool when comparing competing healthcare interventions and serves as a way to inform policy and more effectively allocate limited healthcare resources [1]. Cardiac rehabilitation services are considered to be an integral part of the contemporary care of patients with heart disease [2,3]. Although several systematic reviews have demonstrated the effectiveness of cardiac rehabilitation on clinical outcomes including morbidity, mortality, cardiac risk factors, and quality of life [4–7, only two systematic reviews have considered economic evaluations [8,9]. A systematic review by Oldridge [8] identified eight publications that reported original data or findings on the cost-effectiveness of cardiac rehabilitation interventions. A second review by the Canadian Coordinating Office of Health Technology Assessment (CCOHTA) [9] was limited to three full economic evaluations evaluating exercise-based interventions against usual care. Given the increasing importance of alternative cardiac rehabilitation program delivery models (e.g. case-managed, telephone-based, internet-based) there is a need to review and evaluate the evidence supporting the cost-effectiveness of these delivery models. The goals of the present systematic review are: (i) to summarize published economic evaluations of cardiac rehabilitation delivery models; (ii) to evaluate the methodological quality of the economic evaluations of cardiac rehabilitation; and (iii) to make recommendations regarding future directions for economic evaluation of cardiac rehabilitation.
Methods
Economic evaluation
Economic evaluations are influenced by a number of design factors including analysis type, perspective, and the comparators selected. Two main categories of economic evaluation exist. The first, partial economic analyses evaluate either the costs or consequences between two interventions or both the costs and consequences of a single intervention. The second, full economic analyses evaluate both the cost and consequences between two or more interventions and provide an incremental cost-to-effect ratio. Criteria for partial and full economic evaluations are provided in Table 1 [10]. The present review has included both partial and full economic evaluations of cardiac rehabilitation in effort to summarize the quality of best available economic evaluations.
Literature search strategy
Electronic databases (Medline and The Cochrane Library) were searched for English language publications reporting original data on the economic impact of cardiac rehabilitation published before January 2005. The following text word terms and MeSH headings were used: ‘economic evaluation’ or ‘costs’ or ‘cost’ or ‘cost effectiveness’ or ‘cost benefit’ or ‘cost utility’ and ‘cardiac rehabilitation'. To identify additional publications, hand searches of bibliographies were conducted. The titles and abstracts of all citations generated from the search were reviewed to identify eligible publications.
Description of economic analyses

Eligibility criteria
An economic evaluation was eligible for inclusion if it met each of the following criteria: a full economic analysis which evaluates both cost and effect of comparators, or a partial economic evaluation examining costs; prospective economic evaluations with 6 months or more follow-up or modeling studies; the study population includes adult patients with heart disease [myocardial infarction (MI), percutaneous transluminal angioplasty (PTCA), coronary artery bypass surgery (CABG), or heart failure]; at least one comparator includes a cardiac rehabilitation program (supervised, home-based).
Data abstraction
Eligible publications were audited by two independent reviewers. Standardized data abstraction forms were used to review all potentially relevant articles. If there was disagreement between reviewers, a third reviewer's opinion was obtained. The abstraction form was used as the basis for data synthesis and evaluation. The following descriptive data were collected for each economic evaluation: objective and perspective, analysis type and study design, sample size and population, comparator, intervention, results, and conclusions. All costs have been adjusted to reflect 2004 United States dollars using international exchange rates and the consumer price index for medical costs [11].
Quality assessment strategy
The methodological quality of economic evaluations was assessed using the 10-item Drummond [10] criteria for economic evaluations. Each of the criterion items assesses an important issue in the design of economic evaluations. Evaluators applying the criteria rank the publication as meeting appraisal criteria (Y), not meeting appraisal criteria (N), or not able to tell (C). The Drummond criteria [10] have been previously used in the evaluation of healthcare interventions [12] and are consistent with best practice guidelines [13,14] for economic evaluation.
Results
Synthesis
Of the 379 publications originally identified using keyword search combinations, 50 qualified for detailed review, following which 35 were excluded. Reasons for exclusion were a lack or inadequate assessment of costs and limited follow-up. A total of 15 economic evaluations [15–29 were identified as eligible for the present review.
Characteristics of the economic evaluations
An overview of the study and methodological characteristics, study populations, interventions and outcomes of the 15 economic evaluations included in the review are provided in Table 2.
Date of publication
The first economic evaluation was published in 1985 [15], five (33.3%) were published between 1990 and 1999 [16–20, and nine (60.0%) between 2000 and 2004 [21–29.
Location
Seven (46.6%) publications were conducted in the United States [15,17,20,21,23,26,27], two (13.3%) in Canada [18,22], four (26.6%) in Europe [16, 19,25,28], one (6.6%) in Australia [24], and one (6.6%) in Hong Kong [29].
Perspective
The majority of the publications (53.3%) evaluated costs from the perspective of the healthcare payee (all costs that would be incurred by the party responsible for medical expenses) [17,19,20,25–29] with 26.7% using the societal perspective [16, 18,22,23] and 20% using the perspective of the rehabilitation program [15, 21,24].
Design
A randomized, controlled trial (RCT) design was used in 60.0% of the publications [15,18,21,23,25–29], 20% used non-randomized designs [16, 17,19] and 20% were modeling studies [20, 22,24].
Type
Cost and cost-utilization analyses were used in nine (56.2%) of the economic evaluations [15–17,19,21, 24–27], cost-effectiveness in five (31.3%) [18,20,22, 23,28] and cost-utility in two (12.5%) [18,29].
Population
Excluding modeling studies based on previously published sources [20, 22,24], a total of 2779 patients (66.6% male, 33.4% female) were included in the 12 economic evaluations. The sample includes several cardiac patient populations including post-MI (68.1%), CABG (22.2%), PTCA (5.5%), angina patients (7.5%), heart failure (7.5%), and unspecified cardiovascular disease (6.9%). The majority of economic evaluations were completed in populations limited to male MI patients.
Comparative evaluations
Four types of comparisons were found with several of the publications reporting multiple comparisons. These included supervised cardiac rehabilitation versus standard care (n = 8) [16–18,20,22,23,25,29]; supervised cardiac rehabilitation versus revascularization (n = 1) [28]; home-based cardiac rehabilitation versus standard care (n = 5) [19,22,25–27]; supervised cardiac rehabilitation versus home-based cardiac rehabilitation (n = 4) [15, 21,24,25]. Table 2 provides a summary of the characteristics and main findings for each of these comparison groupings.
Supervised cardiac rehabilitation versus standard care
The findings for each of the comparisons against standard care have reported positive outcomes including lower rehospitalization rates [16, 17,25], greater cost-effectiveness [20, 22,23] and greater cost-utility ratios [18,29] favoring the cardiac rehabilitation intervention groups in all eight of the published studies. Prospective RCT evidence of the cost-effectiveness of supervised cardiac rehabilitation is limited to MI and heart failure patient populations [18,23]. The range of costs per life year gained resulting from cardiac rehabilitation as compared to standard care was $2193-$28193 [18, 20,22]. Amongst the eight published studies only two provide gold-standard full economic evaluations using RCT designs and cost-utility analyses. One of these trials reported that supervised cardiac rehabilitation cost $16118/Quality Adjusted Life Year (QALY) over 1 year or $11913/QALY over 3 years [18] and the other reported $668 saved/QALY over 2 years when compared with standard care [29].
Supervised cardiac rehabilitation versus revascularization
A single prospective RCT [28] reported direct head-to-head comparison of cardiac rehabilitation against revascularization procedure and found exercise-based cardiac rehabilitation to be more cost-effective than stent angioplasty in patients with one native coronary artery stenosis of 75% or greater.
Home-based cardiac rehabilitation versus standard care
A cost savings of $966-$1954 per person has been reported for home-based delivery over standard care [25–27. One modeling study [22] provided support for the cost-effectiveness of home-based cardiac rehabilitation over standard care. There has been no prospective full evaluation comparing home-based cardiac rehabilitation delivery with standard care.
Supervised cardiac rehabilitation versus home-based cardiac rehabilitation
Each of the four cost analyses comparing supervised cardiac rehabilitation against home-based cardiac rehabilitation programs report a greater cost saving ($363 to $9575/person) as compared to supervised program delivery [15, 21,24,25]. There has been no full prospective evaluations comparing the cost-effectiveness of supervised to home-based cardiac rehabilitation programs.
Overview of the 15 economic evaluations reviewed by study characteristics and outcomes with all costs in 2004 US dollars

Costs have been reported in 2004 US dollars using consumer price index for medical care [11]. CR, cardiac rehabilitation; RCT, randomized controlled trial; Ml, myocardial infarction; PTCA, percutaneous transluminal coronary angioplasty; QALY, quality adjusted life year; NYHA, New York Heart Association; LYS, life year saved; N/A, not applicable; CABG, coronary artery bypass graft; CCS, Canadian Cardiovascular Society Angina Pectoris Classification System; CHD, coronary heart disease; CVD, cardiovascular disease; I, intervention group; UC, usual care; ECG, electrocardiogram.
Summary of Drummond evaluation of methodological quality
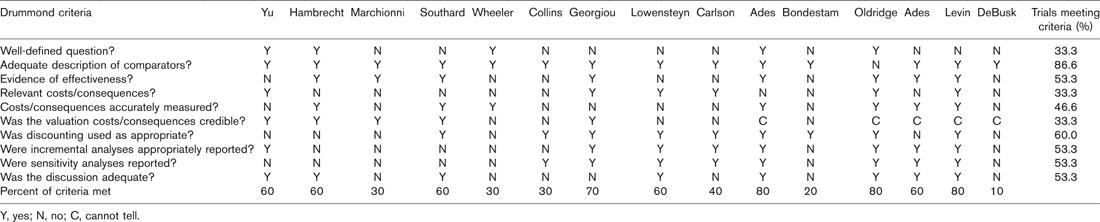
Y, yes; N, no; C, cannot tell.
Quality assessment
Table 3 provides a summary of the Drummond review criteria for all 15 economic evaluations included in this evaluation with none meeting all of the criteria. Of the 15 economic evaluations reviewed, 33.3% [18,20,27–29] provide a well-defined question in an answerable form, 53.3% [16–18,20,23,25,26,28] provide evidence of effectiveness, and 53.3% [16,17,20–24] conducted sensitivity analyses. The majority of publications provided only partial economic evaluations and are therefore limited in scope. Only two (13.3%) of the 15 economic evaluations reviewed conducted cost-utility analysis [18,29], which is considered to be the gold standard for economic evaluation of healthcare interventions [13].
Discussion
Economic analyses can assist with rational decisionmaking about the allocation of limited health resources by providing information about the value of alternative health interventions. Following an extensive review, 15 publications were identified that contained economic evaluations of cardiac rehabilitation services and all cost figures provided in this review have been adjusted to 2004 US dollars. The published economic evaluations displayed wide variation in the use of comparators, evaluation type, perspective and design making data pooling inappropriate.
Evidence to support the cost-effectiveness of supervised cardiac rehabilitation compared to usual care in MI and heart failure was identified within this review. The range of costs was estimated as $2193–28 193 per life year gained [20, 22,23]. Until recently there had been only one published cost-utility analysis of cardiac rehabilitation services in which Oldridge and colleagues [18] reported incremental cost-utility ratios of $16 118 and $11 913/QALY gained over 1 and 3 years, respectively. A second RCT with a cost-utility analysis [29] was published in 2004 in which a savings of $668 per QALY gained at the end of 2 years cardiac rehabilitation was reported in a sample of MI and PTCA patients in Hong Kong. The methodology in these two RCTs, including study population, intervention, length of follow-up, and cost determination, varied widely. The cost/QALY, however, in both of these economic evaluations falls well under the accepted range of $20 000/QALY to be considered highly cost-effective [13].
Other than one RCT in patients with heart failure in which the intervention was highly cost-effective [23], there is little high quality prospective trial data to support the cost-effectiveness of cardiac rehabilitation in non-MI patient groups. Differences observed in cost-effectiveness in the present review suggest that different patient diagnosis groups may benefit differentially from cardiac rehabilitation interventions and requires further evaluation. In addition, although there is evidence from modeling studies to suggest that sex differences may exist in the cost-effectiveness of cardiac rehabilitation [22], sex differences require further exploration before any conclusions can be drawn. Women have not been adequately represented in cardiac rehabilitation settings [30] and are also under-represented in the economic evaluations conducted to date (e.g. the study by Oldridge [18] in which only 12% were female).
Although no full prospective economic evaluation has evaluated two competing cardiac rehabilitation program formats (e.g. supervised cardiac rehabilitation versus home-based cardiac rehabilitation), studies evaluating cardiac rehabilitation delivery model characteristics indicate that mode of delivery may play an important role in how resources are utilized to achieve a desired outcome. Several alternative forms of home-based programs were evaluated within the literature reviewed including telephone-based [15], internet-based [26], case-managed programs [15,24]. For home-based cardiac rehabilitation against standard care, economic evaluations indicate a net cost saving [25–27 and improved cost-effectiveness [22]. When compared to supervised cardiac rehabilitation, cost analyses have also found home-based cardiac rehabilitation programs can be delivered at a reduced cost [15, 21,24,25]. Specifically, savings in accommodation, overhead, equipment, and staff time have been documented with home-based delivery. As we learn more about the characteristics and components that improve clinical outcomes produced by cardiac rehabilitation it will be important to also evaluate the immediate and downstream economic impact of these programs.
The body of literature supporting the cost-effectiveness of cardiac rehabilitation services is characterized by poor methodological quality. Previously published systematic reviews of the cost-effectiveness of cardiac rehabilitation have documented the lack of evidence to support the cost-effectiveness of cardiac rehabilitation, particularly the lack of RCTs, and the poor quality of existing trials [8]. The methodological quality of economic evaluation comparing alternative cardiac rehabilitation models is limited to cost analyses and questions remain concerning the relative cost-effectiveness of different program designs [21,25]. Several recent publications [22, 24,26,27] do not demonstrate improved methodological quality. The limited number of cost-utility analyses of cardiac rehabilitation [18,29] is troubling for two reasons. Firstly, improved health-related quality of life is considered an important benefit of cardiac rehabilitation interventions [2,3] and cost-utility analyses are the only economic evaluation type that can effectively capture these changes [31,32]. Secondly, the US Public Health Services Panel on Cost-Effectiveness in Health and Medicine has recommended using QALYs as the denominator in the cost-effectiveness ratio in an attempt to improve the quality and comparability of economic analyses [13]. This further reinforces the importance of cost-utility analyses in future studies of cardiac rehabilitation.
Limitations of this systematic review include the possibility that studies may have been missed in the identification process and the fact that non-English and unpublished studies are not included in the review. Although, this systematic review was limited to literature published in the English language, which may introduce some bias to the reviews findings [33], we have included English language publications conducted in a variety of international healthcare settings. All studies under review except one (Hong Kong) were conducted in western, industrialized countries. The validity of making comparisons between economic analyses conducted in different healthcare systems is unknown and may not be appropriate [34]. In addition, a portion of studies included in the review would have been conducted prior to the maturity of modern medical therapies (e.g. thrombolysis, statins, PTCA, stent), which have resulted in improved patient morbidity and mortality and therefore may overestimate the cost-effectiveness of cardiac rehabilitation today.
As a result of this systematic review, and in conjunction with the recommendations of the US Public Health Services Panel on Cost-Effectiveness in Health and Medicine [13], the following recommendations are directed towards advancing policy and research surrounding the economic viability of cardiac rehabilitation:
Greater dissemination of best practices in the design of economic evaluations is required within the field of cardiac rehabilitation.
Well-designed RCTs should be conducted evaluating the cost-effectiveness and cost-utility of alternative cardiac rehabilitation delivery models including home-based rehabilitation programs, telephonic interventions, dose-response models, and program characteristics.
Research is required to assist with identifying and understanding which patient segments will produce greater cost-effectiveness and cost-utility from comprehensive cardiac rehabilitation and other alternative delivery models. This includes high-risk and low-risk patients, sex, age, and cardiac patient groups.
Conclusion
Following an extensive review, 15 economic evaluations of cardiac rehabilitation services were identified. Evidence to support the cost-effectiveness of supervised cardiac rehabilitation compared with usual care in patients with MI or heart failure was identified within this review. The published economic evaluations, however, displayed wide variation in the use of comparators, evaluation type, perspective and design. To date only two RCTs have provided gold standard evidence of the cost-utility of supervised cardiac rehabilitation services. The literature evaluating home-based and alternative delivery models of cardiac rehabilitation was insufficient to draw conclusions about their relative cost-effectiveness. There is a need for further well designed RCTs preferably with cost-utility analyses to support the generalizability of these findings. In particular studies evaluating the cost-utility of cardiac rehabilitation services in patients who have undergone revascularization and studies comparing alternative cardiac rehabilitation delivery models.