
Abstract
Background
Depressive symptoms have been suggested to increase the risk of cardiovascular diseases, but this may reflect reversed causality. We investigated to what extent depressive symptoms are a true risk factor for cardiovascular mortality in elderly men.
Design
The Finland, Italy and Netherlands Elderly (FINE) study is a prospective cohort study conducted in Finland, Italy and The Netherlands.
Methods
Depressive symptoms were measured with the Zung self-rating Depression Scale in 799 elderly men, aged 70–90 years, free from cardiovascular diseases. Using Cox models, hazard ratios (HRs) were calculated for specific cardiovascular mortality endpoints. The analyses were adjusted for potential confounders, stratified on country and repeated after exclusion of men who died from cardiovascular diseases up to 5 years after baseline.
Results
During 10-years of follow-up 224 (28%) men died from cardiovascular diseases. The adjusted hazard for a five-point increase in depressive symptoms was 1.15 [95% confidence interval (CI) 1.08–1.23] for cardiovascular mortality. This risk was stronger for mortality from stroke (HR 1.35; 95% CI 1.19–1.53) and heart failure (HR 1.16; 95% CI 1.00–1.35) in comparison with mortality from coronary heart disease (HR 1.08; 95% CI 0.97–1.20) and other degenerative heart diseases (HR 1.06; 95% CI 0.91–1.23). Exclusion of men who died from cardiovascular diseases within 5 years after baseline did not change the strength of the associations. There were no significant differences in HRs between northern and southern Europe.
Conclusions
This study provides further and more convincing prospective evidence for depressive symptoms as a risk factor for cardiovascular mortality in elderly men.
Introduction
Cardiovascular diseases (CVDs), including coronary heart disease (CHD) and stroke, are still the major causes of death in most European countries and account for 32% of all deaths [1]. There is increasing evidence that besides classical risk factors, such as hypertension, hypercholesterolemia, diabetes and smoking, psychosocial factors and depression also play a role in the occurrence of cardiovascular diseases [2].
In patients with CVD depression is common. For instance, one in five patients with newly diagnosed coronary disease is depressed [3]. Depression is not only common in patients with cardiovascular disease, it may also worsen the prognosis and may lead to a higher mortality from CVD [4, 5]. Several explanations have been put forward for a worse prognosis associated with depression, such as higher disease severity, unhealthy behavior, non-adherence to cardiac treatment, antide-pressant cardiotoxicity, more cardiovascular risk factors, inflammation, autonomic dysfunction and increased platelet activation [6].
More recently, it has been hypothesized that depression not only leads to poor prognosis in patients with established CVD, but also increases the risk of CVD in initially healthy persons. Recent reviews show evidence for the hypothesis that depression is a risk factor for CVD [2, 7]. Due to heterogeneity between studies, however, results of these studies are difficult to compare. For instance, most of the studies reviewed used different cardiovascular endpoints. In addition, most of the studies were performed in middle-aged persons. In elderly men the results are less conclusive. For instance, mild and major depression have been associated with increased total mortality [8] and CVD mortality [9–11] but the results are not conclusive for CHD [9, 12], stroke [13] and heart failure incidence [14, 15]. Also, depression may still be a consequence of subclinical disease, thus indicating reversed causality [16–19].
We investigated the relation between depressive symptoms and risk of cardiovascular mortality in a population-based sample of older men in three European countries. We investigated specific cardiovascular mortality endpoints, and excluded men who died from CVD in the first 5 years after baseline to minimize the possibility of reversed causality.
Methods
The Finland, Italy and Netherlands Elderly study
The Finland, Italy and Netherlands Elderly (FINE) study is a prospective population-based cohort study on risk factors and health in elderly men. The study design and measurements have been described in detail elsewhere [20]. In brief, the FINE study started in 1984 as a continuation of the Seven Countries Study (SCS), which was originally initiated in 1958 by Keys [21] as a cardiovascular risk factor survey among 12 763 middle-aged men, born between 1900 and 1920. In The Netherlands, the surviving cohort was enlarged in 1985 to an elderly cohort of 939 men, by inviting a random sample of men born between 1900 and 1920 who had not participated in the study before. In total, 2285 men from Finland (n = 716), Italy (n = 682) and The Netherlands (n = 887) participated in the baseline examination of the study in 1985. Informed consent was obtained from all study participants. Data collection followed the international protocol used in previous surveys of the SCS [21]. In 1989–1991 the second round of the FINE study took place. In this round, measures on depression, functional status, cognitive function and self-reported health were added. Around 1995 and 2000 the third and fourth round of examinations were carried out. Mortality data were collected until the year 2000.
Depressive symptoms
Depressive symptoms were measured using the self-rating depression scale (SDS), developed by Zung [22]. This scale was used to assess depression among patients admitted to a psychiatric hospital, but also for non-institutionalized elderly [23] and was highly comparable among different countries [24]. The reproducibility of the SDS is good in elderly men (Cronbach α 0.75) [25] and has been validated repeatedly with other questionnaires on depressive symptoms, such as the Center for Epidemiological Studies Depression Scale (r = 0.69) [26], the Geriatric Depression Scale (r = 0.59) [27] and the Hamilton Depression scale (r = 0.80) [28]. The questionnaire contained 20 either positively or negatively formulated items, based on clinical diagnostic criteria commonly used to diagnose depressive disorders. The answers on those items were coded on a four-point Likert-type scale varying from ‘none or sometimes’ to ‘most or always'. Negative items were converted into positive ones with total scores ranging from 20 to 80. Men with more than two missing items were excluded for the analysis. If one or two items were missing, the mean score of the valid items of the subject was calculated and the missing items were replaced by this mean score. An index for the SDS was derived by dividing the sum of the answers by 80 times 100 (range 25–100), with a higher score indicating more depressive symptoms. The original clinical cut-off values are: no depression (< 50); mild depression (50–59); and moderate-severe depression (≤60) [23]. To increase power a continous measure of the SDS was used (five-point increase) and the SDS was categorized into country-specific tertiles.
Cardiovascular endpoints
Mortality data were collected during 10 years of follow-up and obtained through official death certificates. One person was lost to follow-up. He was included in the analyses, but censored at the date of the examination round that he was lost to follow-up (after 3.6 years). Men who died from other causes were censored at date of death; for men who were still alive in 2000 the censor date was set at the examination date of the last round. In Finland, information on the causes of death was obtained from Finnish death registers; in Italy and The Netherlands the information was obtained from hospital registries or general practitioners. Original coding was done locally and checked by one clinical epidemiologist, who was blinded to the risk factor status of the subject.
All diagnoses were coded according to the International Classification of Diseases (ICD), ninth revision. The following ICD codes were used: CVD (390–459), coronary heart disease (CHD) (410–414), stroke (430–438), heart failure (428) and other degenerative heart disease (oDHD) (401–405, 426-427 and 429). For the analyses, both primary and secondary causes of death were considered.
Cardiovascular risk factors
The self-administered questionnaire contained questions on demographic characteristics, educational level, lifestyle habits, past and current morbidity. Participants were classified as current, past or never smokers according to their smoking habits. Alcohol intake was derived from the cross-check dietary history in The Netherlands, and in Finland and Italy assessed with self-administered questionnaires [29]. A proportion of the Finnish men (n = 62) had no information on alcohol intake, because in 1990 a reduced questionnaire was used. For these men the alcohol intake from 1985 was used. Alcohol intake was expressed as grams of alcohol per day, and classified into three categories (0, 1–29 and ≤30 g/day) [29]. Body mass index (BMI) (kg/m2) was calculated from weight and height, which were measured while the participant was standing in light clothing without shoes. Physical activity was assessed with a self-administered validated questionnaire designed for retired men [30] and expressed as minutes of total physical activity per week (min/week). Self-reported disability was measured using a standardized questionnaire about routine daily activities and classified as moderate/severe disabilities, compared to no/mild disabilities, following a hierarchical disability coding scheme [31].
Arterial blood pressure was measured twice on the right arm after 5 min of rest, with the man in a supine position. In Finland and Italy standard mercury sphygmomanometers were used, while in The Netherlands a random zero sphygmomanometer was used. The average of two readings of both systolic and diastolic blood pressure (fifth Korotkoff phase) was calculated. Venous blood samples (fasting in Finland and non-fasting in Italy and The Netherlands) were taken and total and high-density lipoprotein (HDL) cholesterol (mmol/l) were determined using standardized procedures according to the criteria of the World Health Organization's Lipid Reference Laboratories in Prague, Czech Republic, or Atlanta, Georgia [29]. History of myocardial infarction was obtained using the London School of Hygiene and Tropical Medicine questionnaire [32], verified by information from general practitioners or hospital registries. The clinical history of stroke, heart failure and diabetes was based on the doctor's conclusion using questionnaire information and the results of the physical examination.
Study sample
Depressive symptoms were measured for the first time during the second round of the FINE study, between October 1989 and November 1991, when in total 1416 men (82%) participated of the 1734 men still alive. At that time, 909 (64%) were free of CVD and diabetes. We excluded 85 men with more than two missing items in the SDS as well as 25 men with missing values in covariates. Thus, a study sample of 799 men remained for analysis, 229 men from Finland, 332 men from The Netherlands and 238 men from Italy.
Statistical analysis
Means and standard deviations (SDs) were computed for continuous baseline variables, and medians and 10–90 percentiles for continous variables with a skewed distribution. Frequency distributions were given for categorical variables according to country-specific tertiles of the SDS index score. Differences between SDS tertiles were tested for each country, with ANOVA, Kruskal-Wallis (in case of skewed distribution) or X2-test.
To investigate the association between depressive symptoms and CVD mortality, Cox proportional hazard analyses were performed. By censoring other types of events we could analyze different CVD mortality endpoints separately. Age was used as the time scale in the proportional hazards models to optimally adjust for age [33]. Age at entry was assigned as the age at the date of examination in 1990. Censoring age was defined as age at death or end of study. A hazard curve of the follow-up years versus the percentage of subjects who died of CVD was made, according to tertiles of depressive symptoms. With a log versus log minus log plot the assumptions of proportional hazards were checked. The assumptions of proportionality were not violated. Analyses were done for five-point increase and tertiles of baseline depressive symptoms. In the first model we adjusted for age (in the time-axis). In the second model analyses we also adjusted for possible confounders: country (Finland, The Netherlands, Italy), years of education, body mass index (kg/m2), smoking (never, past, current), alcohol intake (0, 1–29/ ≤30 g/day), SBP (mmHg), total and HDL cholesterol levels (mmol/l) and physical activity (min/week). Analyses were additionally adjusted for disabilities and repeated with clinical categories of depressive symptoms (no, < 50; mild, 50–59; moderate-severe, ≤60). To evaluate whether country modified the association between depressive symptoms and cardiovascular mortality, analyses were also done after stratification by country and interaction terms of country and the SDS index score were included. Analyses were repeated after exclusion of men who died from CVD in the subsequent 5 years after baseline.
All analysis were performed with SPSS version 12.0.1 (SPSS Inc, Chicago, Illinois, USA) and the SAS statistical software package, version 8.2 (SAS Institute, Cary, North Carolina, USA) [34]. Point estimates are given with corresponding 95% confidence intervals (CIs).
Results
After 10 years of follow-up 396 (50%) men had died and 403 men were still alive. Two-hundred and twenty-four (28%) men died from CVD, 93 from CHD, 66 from stroke, 45 from heart failure and 46 from oDHD. The total number of person-years was 5893 and the mean follow-up time was 7.4 years (SD = 3.0). The average SDS score was 49.2 (SD = 11) in Italy, 45.4 (SD = 10) in Finland and 42.6 (SD = 10) in The Netherlands. Table 1 presents the baseline characteristics of the men (n = 799) for each country and for the whole study population, according to country-specific tertiles of the SDS score. Men with more depressive symptoms had received shorter education, were more disabled and less physically active. Although not significant, men from Finland and Italy with more depressive symptoms seemed to have lower total and HDL cholesterol levels. One-hundred and ten men (8%) who were excluded from the analyses due to missing values in the SDS or other covariates were older, less educated and less physically active, more disabled and had a higher mortality rate in comparison with men who were not excluded (results not shown).
Table 2 presents hazard ratios for a five-point increase and tertiles of depressive symptoms and different CVD mortality endpoints. The age-adjusted hazard ratio for the continuous SDS score and CVD mortality was 1.14 (95% CI 1.08–1.22), indicating that for each increase of five points on the SDS (range 25–100) the risk of mortality from CVD increased with 14%. This hazard ratio did not change after additional adjustments for demographical and other cardiovascular risk factors (model 2). In addition, the association was slightly attenuated after adjustment for disabilities (HR 1.12; 95% CI 1.05–1.20). The associations were stronger for mortality due to stroke (HR 1.35; 95% CI 1.19–1.53) and heart failure (HR 1.16; 95% CI 1.00–1.35) in comparison with mortality due to CHD (HR 1.08; 95% CI 0.97–1.20) and oDHD (HR 1.06; 95% CI 0.91–1.23). Figure 1 illustrates a fully adjusted cumulative hazard curve for CVD mortality according to country-specific tertiles of depressive symptoms. The death rate increased with the number of depressive symptoms. In addition, when using the clinical cutoff scores, the adjusted hazard ratios for CVD mortality were 1.72 (95% CI 1.25–2.37) for men with mild depression (50–59) and 1.87 (95% CI 1.25–2.80) for moderate-severe depression (≤60), compared to men with no depression (< 50). Analyses with the primary death causes showed the same estimates with wider CIs (results not shown).
Exclusion of early CVD deaths did not materially change the results (Table 3). After exclusion of 144 men who died within 5 years after baseline, the hazard ratio for a five-point increase was 1.16 (95% CI 1.03–1.30).
After stratification for country the adjusted hazard ratios for CVD mortality did not differ between countries and none of the interaction terms were statistically significant (results not shown).
Discussion
The results of this prospective study among elderly men without CVD at baseline show that depressive symptoms are associated with an increased risk of future cardiovascular mortality. The risk is highest for mortality due to stroke and heart failure. There are no risk differences observed between northern and southern Europe.
A major strength of this study is its prospective longitudinal design, which made it possible to determine depressive symptoms before onset of CVD. Furthermore, the long follow-up period and large sample size enabled us to examine specific causes of death and to exclude subjects who died from CVD in the first 5 years after baseline, making the possibility of reversed causality even more unlikely. In addition, the estimated effects were not disturbed by a selective loss to follow-up, because the mortality follow-up was complete. Finally, to investigate the independent effect of depressive symptoms, we were able to adjust for many potential confounding variables, in particular, lifestyle and CVD risk factors.
We observed a dose-response relationship between depressive symptoms at baseline and CVD mortality providing further evidence of a causal relationship. Also, we extensively adjusted for possible confounding variables, in particular, lifestyle and CVD risk factors. These factors explained only a small part of the association between depressive symptoms and CVD mortality. Additional adjustments for disabilities attenuated the strength of the association a little further, but there was still an independent effect of depressive symptoms.
Our results provide further and more convincing evidence of depression as a true risk factor for CVD [2, 7]. The strength of the association for CHD mortality that we observed is highly similar to the risk ratio of 1.64 that was found in two systematic reviews [17, 35]. In the present study we found stronger associations for depressive symptoms and mortality from stroke and heart failure, in comparison with mortality from CHD and oDHD. To date, in the elderly, results on specific cardiovasular endpoints such as CHD [9, 12] and stroke [13] have been inconclusive. In addition, increased risks on heart failure incidence were observed in elderly women and hypertensive patients [14, 15]. Our study is the first to observe an increased risk for heart failure mortality in elderly men without CVD at baseline.
Baseline characteristics per country and tertiles of the Zung self-rating depression scale index score (n = 799)
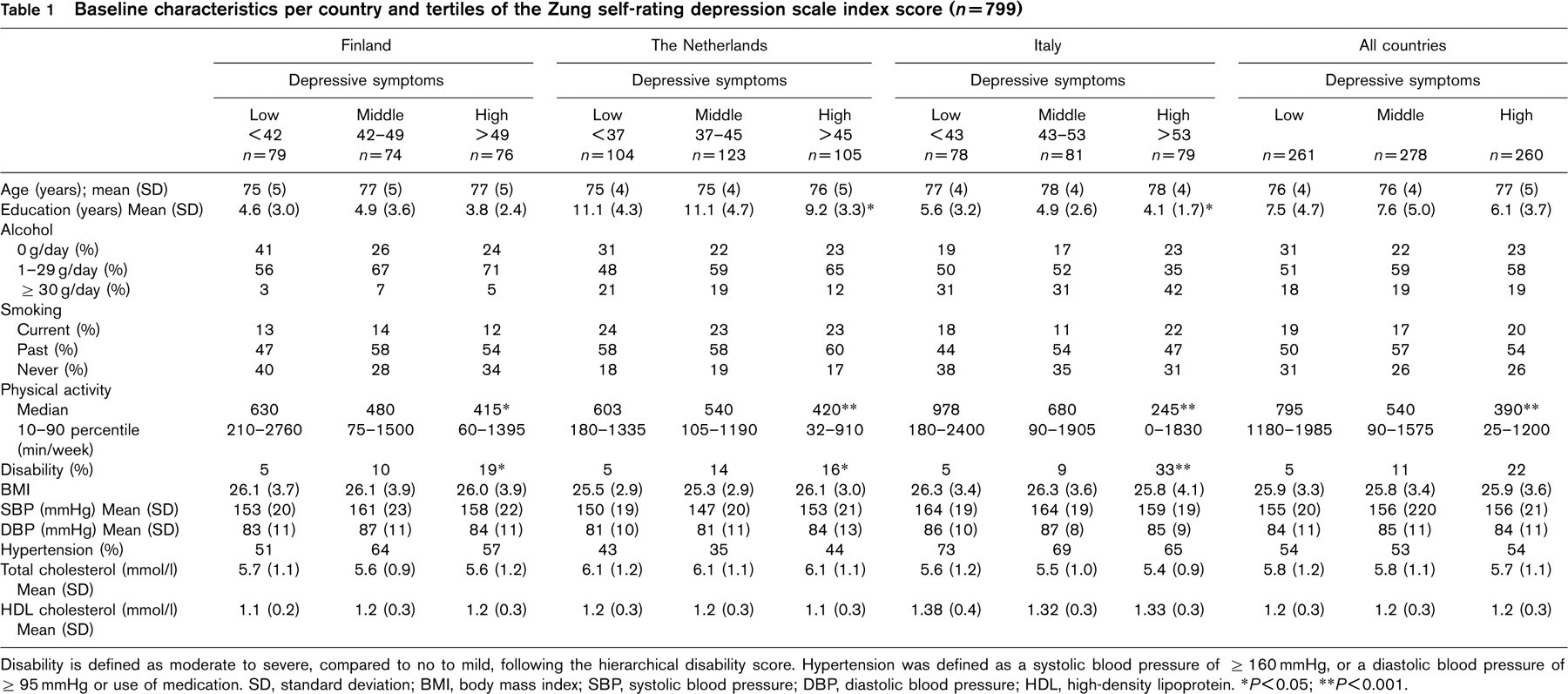
Disability is defined as moderate to severe, compared to no to mild, following the hierarchical disability score. Hypertension was defined as a systolic blood pressure of ≤160 mmHg, or a diastolic blood pressure of ≤95 mmHg or use of medication. SD, standard deviation; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HDL, high-density lipoprotein. ∗P<0.05; ∗∗P<0.001.
Hazard ratios with 95% confidence interval (CI), according to a five-point increase and country specific tertiles of depressive symptoms and mortality from specific cardiovascular diseases
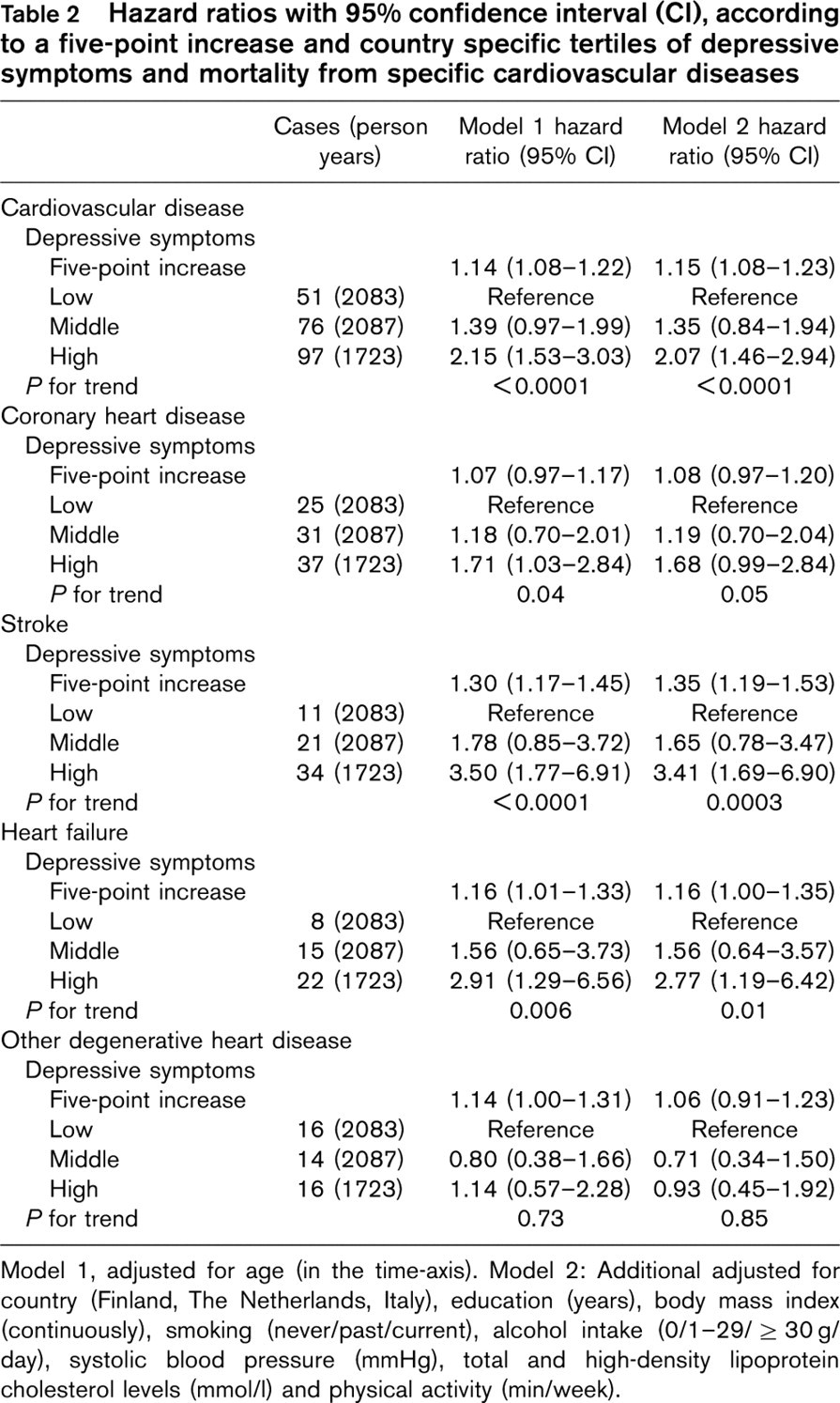
Model 1, adjusted for age (in the time-axis). Model 2: Additional adjusted for country (Finland, The Netherlands, Italy), education (years), body mass index (continuously), smoking (never/past/current), alcohol intake (0/1–29/ ≤30 g/day), systolic blood pressure (mmHg), total and high-density lipoprotein cholesterol levels (mmol/l) and physical activity (min/week).
In the present study we did not have clinical diagnoses of depression. As a result, this study cannot draw conclusions on the relation between clinical diagnoses of depression and CVDs mortality. The analyses with depressive symptoms classified according to the original clinical cut-off values, however, showed similar results as the analyses with tertiles of depressive symptom scores. Moreover, the linear and dose-response relationship we observed suggests that there is no clinical threshold to increase the risk of CVD mortality.
Several mechanisms have been hypothesized to explain the relationship between depression and CVD [6]. First, dietary habits or nutrients might play a role. Depressed persons might have a higher saturated-fat intake or a lower Ω-3 fatty acid intake compared with controls [36]. Second, neuro-endocrine changes during depression may accelerate the development of CVD. For instance, dysregulation of the hypothalamic-pituitary-adrenocortical axis, with its elevated cortisol levels is often present in depression and may lead to atherosclerosis-inducing actions such as injury of vascular endothelial cells, hypertension, hypercholesterolemia and inflammation [37]. Depression is also associated with excessive sympathetic and diminished parasympathetic nervous system activity, which may influence the progression of heart failure by impaired left ventricular function and renal sodium retention [38, 39]. Autonomic dysfunction may also lead to decreased heart rate variability [40], which in turn is associated to arrhythmia and sudden cardiac death [41]. Some mechanisms or factors such as dietary Ω-3 fatty acid intake [36] or inflammation [42] are also associated with an increased risk of depression, indicating that they might be common causes for depression as well as CVD. In the present study, we were not able to discern these potential mechanisms. Our rigorous exclusion of men with prevalent CVD and diabetes at baseline and our extensive adjustment for classical cardiovascular and lifestyle risk factors indicate, however, that the relation between depression and CVD mortality cannot be explained by unhealthy behavior or severity of disease. The relatively high risk we observed for mortality from stroke associated with depressive symptoms may be supportive for the hypothesis that vascular pathology of the brain precedes depression [43].
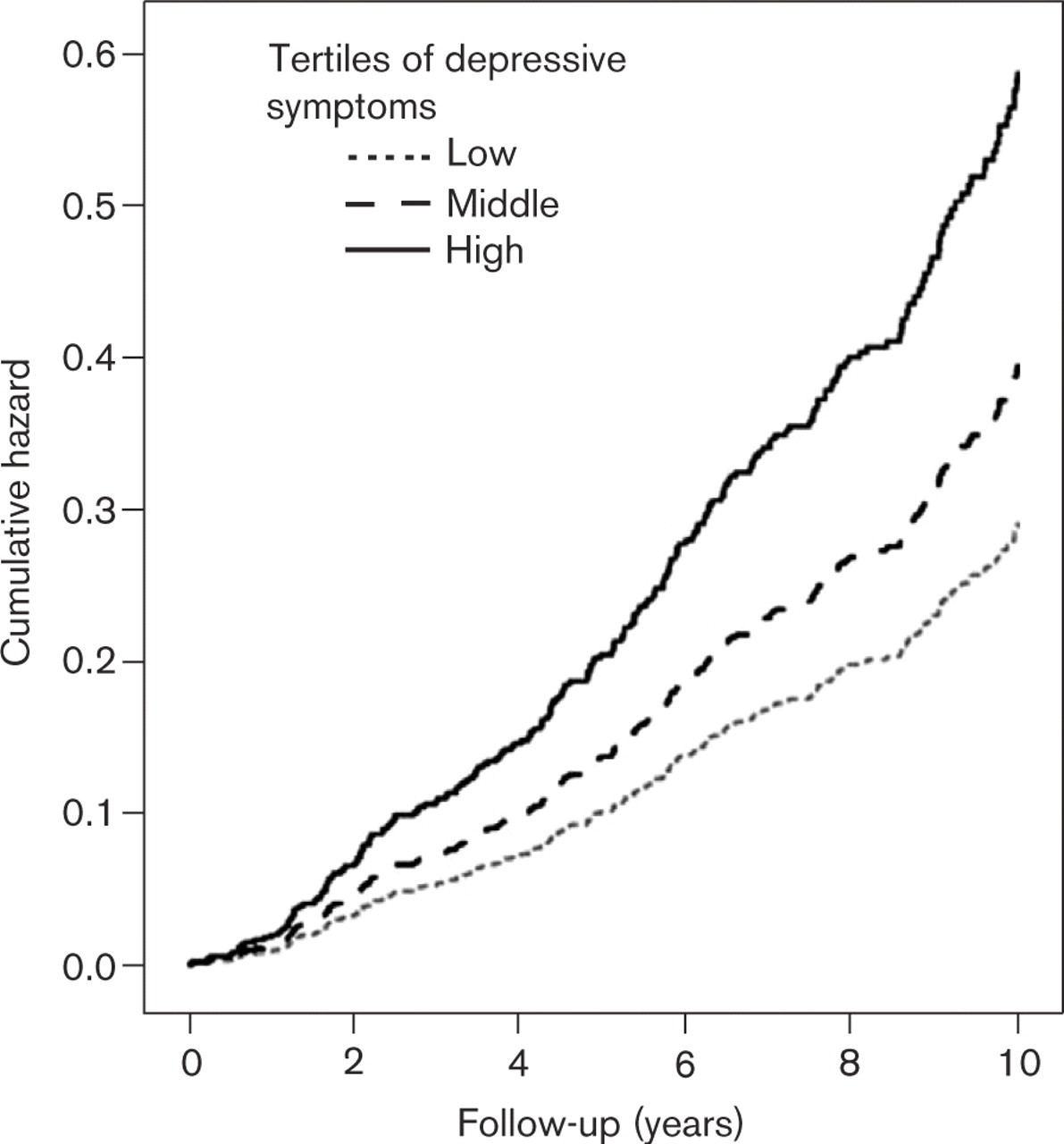
Hazard curves for cardiovascular mortality according to country-specific tertiles of depressive symptoms, adjusted for age, country (Finland, The Netherlands, Italy), education (years), body mass index (continuously), smoking (never/past/current), alcohol intake (0/1–29/ ≤30 g/day), systolic blood pressure (mmHg), total and high-density lipoprotein cholesterol levels (mmol/l) and physical activity (min/week).
Adjusted hazard ratios for five-point increase and country-specific tertiles of depressive symptoms and cardiovascular mortality, after exclusion of men who died from cardiovascular disease in the 5 years following baseline
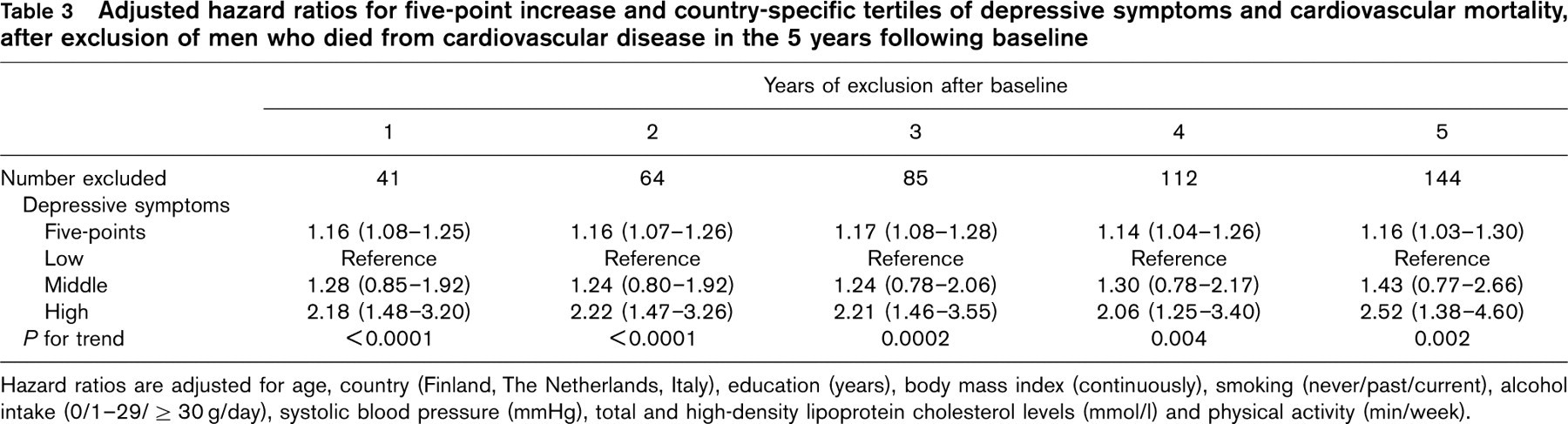
Hazard ratios are adjusted for age, country (Finland, The Netherlands, Italy), education (years), body mass index (continuously), smoking (never/past/current), alcohol intake (0/1–29/ ≤30 g/day), systolic blood pressure (mmHg), total and high-density lipoprotein cholesterol levels (mmol/l) and physical activity (min/week).
Finally, some methodological issues of the current study must be considered. First, selective participation of healthier respondents and exclusion of men with missing values who had a worse health profile may have led to a dilution of the observed hazard ratios. Second, the use of death certificates may have resulted in misclassification of some of the mortality endpoints. To minimize misclassification, however, in The Netherlands and Italy the death certificates were verified with clinical records and in Finland they were linked with the death registers. Furthermore, because the classification of mortality outcome was blinded for baseline status, possible misclassification of the outcome was not related with depression, and will therefore only have resulted in dilution of the associations. Finally, in an observational study the possibility of residual confounding cannot be excluded. We adjusted for many known classical cardiovascular risk factors, however, to minimize this possibility.
In conclusion, the results of the present longitudinal study among elderly men provide strong support for the hypothesis that depressive symptoms are a true risk factor for the occurrence of cardiovascular disease. Future studies should investigate what the underlying mechanisms are and which factors may be intermediates or common causes. They may suggest what preventive or therapeutic strategies may be effective to reduce depression in the elderly, who are often undertreated, and consequently the risk of cardiovascular disease.
Footnotes
Acknowledgements
The authors would like to thank Ingeborg Van der Tweel for her statistical advice, Carolien van den Brink and Boukje van Gelder for their database management.