
Abstract
Background
Coronary heart disease as well as major cardiovascular risk factors are associated with elevated levels of proinflammatory markers. There is, however, limited information about how changes in lifestyle improving the cardiovascular risk profile influence these levels. The aim of the study was to evaluate whether changes in lifestyle measures with special attention to physical activity, were associated with the levels of such markers.
Design
Coronary heart disease patients (n = 197) were randomized to either a comprehensive lifestyle intervention programme comprising regular physical activity, low fat diet and smoking cessation, or usual care with routine follow-up in the outpatient clinic for 6 months. An exercise test and fasting blood samples analysed for soluble cell adhesion molecules, C reactive protein and pro-inflammatory cytokines were evaluated before and at the end of the study.
Results
Improved diet, physical performance and reduction in smoking were obtained in the intervention programme when compared with usual care patients, but no significant group differences in levels of inflammatory markers were observed. In the total population, however, physical performance significantly and inversely predicted levels of soluble cell adhesion molecule 1, (P>0.001), C-reactive protein (P>0.001) and interleukin-6 (P=0.01) at 6 months. Smokers had elevated levels of soluble cell adhesion molecule 1 when compared with non-smokers (P=0.011).
Conclusions
We demonstrated that physical performance is inversely correlated with levels of pro-inflammatory markers in coronary heart disease patients, possibly retarding the process of atherosclerosis. No effect on inflammatory markers was obtained with a 6-month lifestyle intervention programme when compared with patients who received usual care follow-up. Eur J Cardiovasc Prev Rehabil 13:356-362 © 2006 The European Society of Cardiology
Keywords
Introduction
Vascular inflammation is a crucial process in atherosclerosis. The activated endothelium expresses adhesion molecules to which leukocytes adhere, resulting in infiltration and migration of monocytes and T-lymphocytes into the arterial intima. Vascular cell adhesion molecule-1 (VCAM-1), intercellular adhesion molecule-1 (ICAM-1), P and E-selectin are expressed on the endothelial surface, and increased levels of the soluble forms of these soluble cell adhesion molecules (sCAMs) have been demonstrated in patients with coronary heart disease (CHD) [1–4]. Proinflammatory cytokines are important regulators of the expression of cell adhesion molecules [5–7], and elevated circulating levels of tumor necrosis factor (TNF)α and interleukin (IL)-6, as well as C-reactive protein (CRP) have been demonstrated in CHD patients [8–12]. Soluble ICAM-1 has been reported to be elevated in unstable CHD when compared with stable CHD [13] and, together with CRP and IL-6, to predict future cardiac events in healthy individuals [14–16] and CHD patients [17–19].
In addition to the observed associations between established atherosclerotic disease and increased levels of markers of vascular inflammation, an association between major risk factors for cardiovascular disease and levels of endothelial markers have been demonstrated. Smoking [20, 21], hypercholesterolemia [2, 21], increased body mass index (BMI), diabetes mellitus and hypertension [1, 22, 23] have all been shown to predict elevated levels of sCAMs. There is, however, limited information about how changes in lifestyle and improvement of the cardiovascular risk profile influence these levels.
Secondary prevention programmes in patients with established CHD include a combination of optimal drug treatment and lifestyle measures. Successful prevention programmes have resulted in improved medical and lifestyle risk profiles [24–26]. In the present study we wanted to evaluate whether these changes in lifestyle measures influenced levels of soluble markers of vascular inflammation in CHD patients. Special attention was paid to the possible relationship between physical performance and these markers.
Methods
Study population, intervention and examination programme
The study population was recruited from the Vestfold Heartcare study [26]. It comprised 197 patients (162 men, 35 women), mean age was 55 years (minimum 27 years, maximum 68 years). All patients had documented CHD, included at a median 16 days after an acute myocardial infarction (AMI); hospitalization for unstable angina pectoris, stabilized on medical treatment and percutanous transluminal coronary angioplasty or coronary artery bypass grafting (CABG). Patients in a chronic stage of their CHD, with more than 3 months since their last acute event, were also included (Table 1). None of the patients had severe heart failure (New York Heart Association class 3 or 4), and 137 (70%) had suffered a previous myocardial infarction. The regional ethics committee approved the study, and all patients gave their informed written consent prior to inclusion.
After an interview, full clinical examination and collection of a fasting blood sample the patients performed an ergometer bicycle test, at a sub-maximal level (4 min on 50W, 4 min on 100 W). This test was performed to exclude patients with evidence of exercise-induced ischaemia, and all patients were stopped after 4 min on 100 W. Thus, no direct quantitative data on physical fitness were obtained at baseline. The heart rate response to 100 W was used, however, as an indirect measure of physical fitness at baseline.
A clinical nutritionist assessed the dietary habits by using a comprehensive food frequency questionnaire carried out as structured dietary interviews, also including self-reported smoking and exercise habits [26–28]. Following these baseline examinations, patients were randomized either to the lifestyle intervention programme or usual care. Those randomized to usual care received standardised nurse-based information on CHD in general and lifestyle measures, and their medication was prescribed according to existing guidelines. They were informed about the usefulness of regular exercise. Beyond the testing procedures, they had no contact with the team delivering the intervention programme. Their follow-up was in routine outpatient clinics and subsequently by their general practitioners.
Patients in the intervention programme group were subjected to a 6-week period of ‘heart school’ in the Cardiac Rehabilitation Center in our hospital. They were followed systematically on compliance with scheduled meetings and training sessions throughout the 6-month follow-up period. During the first 6 weeks they had physical exercise supervised by a specially educated physical therapist in addition to regular group meetings twice a week. These meetings were conducted by the study nurse in co-operation with the study physician, physical therapist and a clinical nutritionist and comprised dietary advice, smoking cessation, physical activity counselling, psychosocial management and health education related to cardiovascular disease. The detailed multidisciplinary cardiac rehabilitation programme has been described earlier [26].
Baseline characteristics in the randomized groups
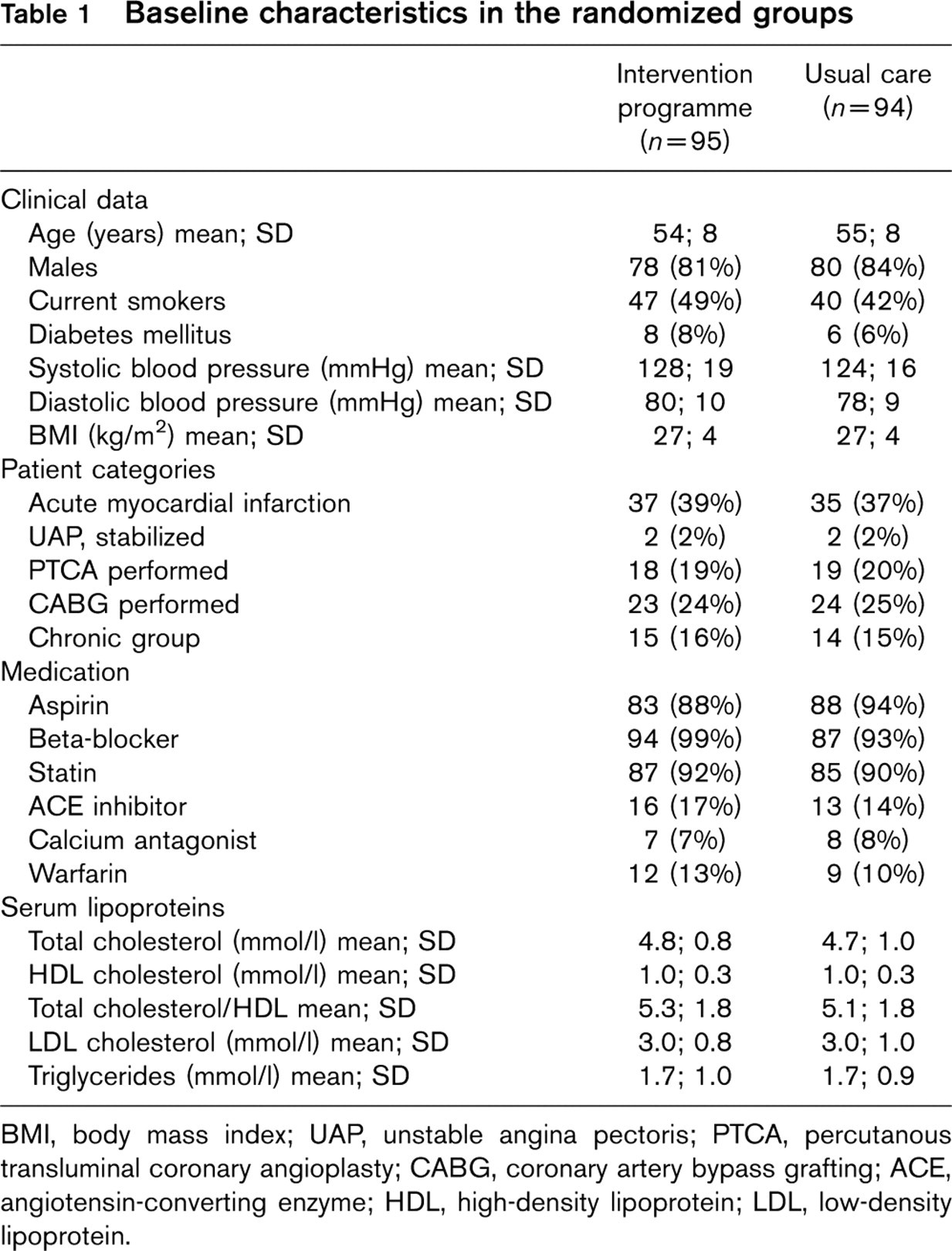
BMI, body mass index; UAP, unstable angina pectoris; PTCA, percutanous transluminal coronary angioplasty; CABG, coronary artery bypass grafting; ACE, angiotensin-converting enzyme; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Each training session started with 15 min of warm-up followed by 20 min of dynamic endurance training, 10 min of active cool-down activities and, finally, 10 min with stretching and relaxation. At the initiation of the exercise training, the patients had been instructed on how to use the Borg scale [29], and the intensity level of the endurance training corresponded to brisk walking or a subjective impression of an exertion rate of 11-13 on the Borg scale. Patients were encouraged to exercise on their own, preferably every day, and to keep an exercise diary in which they recorded all physical activities vigorous enough to make them sweat.
The first 6-week period of heart school in the hospital was followed by 9 weeks of organized physical exercise twice weekly at a gymnasium outside the hospital under the supervision of a physical therapist. The intensity level was now increased to achieve an exertion rate equal to jogging, or corresponding to 13-15 on the Borg scale. For the rest of the study period, participants were encouraged to perform daily exercise on their own or participate in organized training groups. All intervention programme patients were invited to group meetings every third month following the initial 6 weeks throughout the 6-month follow-up period.
During the follow-up period patients in both groups were re-examined with a maximal bicycle test at 6 weeks and 6 months, along with fasting blood sampling at 6 months. The maximal bicycle test was limited by exhaustion, typical chest pain, significant arrhythmias or ST changes of 3 mm or more in the electrocardiogram. Physical performance was measured in all patients regardless of the reason for stopping exercise. Cumulative work performed during the test was measured as follows: cumulative work = kilojoules/minute × minutes of exercise where the products of each working load were added. To transform power meausurements in watts into work measurements in kilojoules, the number of watts is divided by a factor of 16.7.
One individual in the intervention programme group died before the 6 weeks control and seven individuals, two in the intervention programme and five in the usual care group were excluded from further analysis because of non-compliance. The results given are based upon 189 individuals, 95 in the intervention programme and 94 in the usual care group.
Laboratory methods
Blood samples were drawn at inclusion between 8 and 10 a.m. after an overnight fasting. Citrated blood (vacutainer tubes containing 0.129 mol/l trisodium citrate in dilution 1: 10) was collected and platelet poor plasma was obtained within 1 h by centrifugation at 2500g for 20 min for determination of sP-selectin. Serum was prepared within 1 h for measurements of soluble VCAM-1, soluble ICAM-1, sE-selectin, TNFα, IL-6, CRP and lipoproteins. All samples were kept frozen at – 70°C until analysis and analysed with the following methods (inter-assay coefficient of variation (CV) for each analysis in our laboratory is given in parentheses): human soluble VCAM-1 parameter (CV 5.2%); human soluble ICAM-1 parameter (CV 4.8%); human soluble E-selectin parameter (CV 5.3%); human soluble P-selectin parameter (CV 7.2%); human TNFα Quantikine high sensitivity (CV 8.5%) and human IL-6 Quantikine high sensitivity (CV 10.5%), all from R & D Systems Europe, Abingdon, Oxfordshire, UK. CRP was analysed with the immunoturbidimetric method (Cobas Integra; F. Hoffmann-La Roche, Basel, Switzerland) (detection limit 0.25 mg/l; CV >5% at the level of 1 mg/l). Serum lipids and lipoproteins were measured by conventional methods.
Statistical analyses
Results were analysed statistically using SPSS for Windows, version 11.0 (SPSS, Chicago, Illinois, USA). The intervention programme and usual care group were compared at baseline, 6 weeks and 6 months (categorical variables by cross tabs with Pearson χ2 test). Continuous variables were tested for normality by the Kolmogorov-Smirnov test. When comparing normally distributed variables, the independent t-test was used. For comparison of skew-distributed variables, median values were calculated and Mann–Whitney U and Kruskall-Wallis tests were used. Wilcoxon signed rank test for two related samples was used when comparing inclusion and 6 months samples within the same individuals.
Spearman rank correlation analysis was used to evaluate the relationship between physical performance and levels of inflammatory markers and all patients were included.
Age, sex, smoking, diabetes, BMI and cumulative work (log transformed value because of skew distribution) were then introduced into a multiple linear regression model with log-transformed values of sCAMs, inflammatory cytokines and CRP as dependent variables. The influence of lipids and hypertension was not evaluated because of statin and β-blocker treatment. We also used the regression model to evaluate whether changes in smoking habits and physical performance predicted changes in the levels of inflammatory markers.
Results
There were no differences between the two groups in baseline characteristics as given in Table 1. As previously described, there were no significant differences in diet or exercise data between the groups at baseline. The heart rate response to 100W was 106.1 (SD 18.4) in the intervention programme group versus 108.8 (SD 14.5) in the usual care group (P=0.29). There were still no significant intergroup differences in medication after 6 months. Both groups reduced their intake of saturated fat from baseline to 6 months, with a 10% reduction in the usual care group versus 49% in the intervention programme group. The intervention programme patients had a significantly lower intake of saturated and monounsaturated fat, sugar and cholesterol combined with a higher intake of fibre when compared with the usual care group at 6 months (P >0.001 for all). Smoking cessation was obtained in 55% of initial smokers in the intervention programme group versus 33% in the usual care group (P >0.05), and 93% of the intervention programme patients versus 72% in the usual care group exercised for more than 1 h per week (P >0.001) [26].
The results from exercise testing at baseline were limited by the submaximal protocol used. At 6 weeks and 6 months, the intervention programme group performed better than the usual care group, as shown in Table 2. Neither the improvement in physical performance from 6 weeks to 6 months nor the heart rate response to 100W at 6 weeks or 6 months, however, differed between the groups.
From baseline to 6 months there was a significant fall in the levels of soluble VCAM-1 (P >0.001), soluble ICAM-1 (P = 0.043), TNFα (P >0.001), IL-6 (P >0.001) and CRP (P >0.001) in the total population. No significant differences between the study groups were observed, however, either in the levels of endothelial markers at 6 months (Table 3) or in changes from baseline. In the total population, smokers had significantly higher levels of soluble ICAM-1 when compared with non-smokers at baseline (P = 0.027) and after 6 months (P = 0.011) and of IL-6 at 6 months (P = 0.049). Both persistent smokers and those who had stopped smoking, however, had similar reductions in soluble ICAM-1 and IL-6 during the 6 months observation.
Cumulative work in kilojoules (minutes × watts) at 6 weeks and 6 months in the two groups
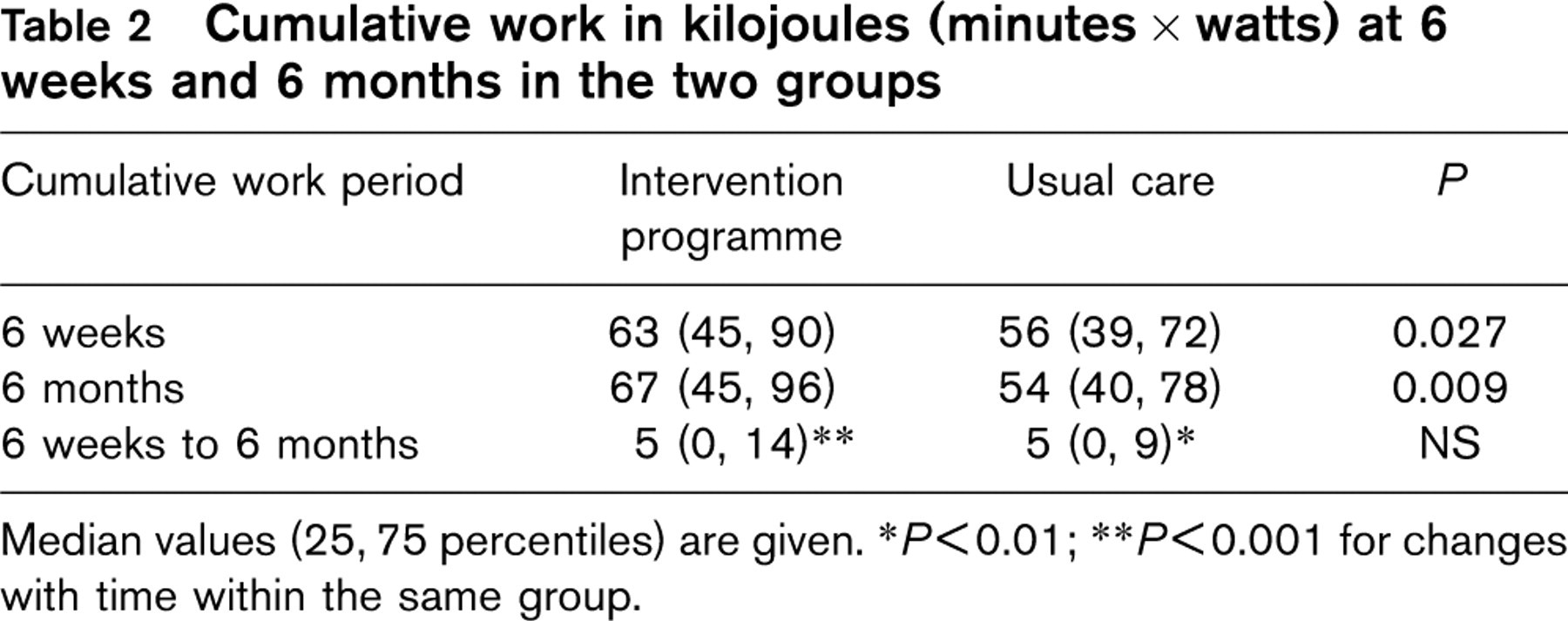
Median values (25, 75 percentiles) are given. ∗P >0.01; ∗∗P >0.001 for changes with time within the same group.
Median levels (25, 75 percentiles) of inflammation markers in the two groups at baseline and 6 months
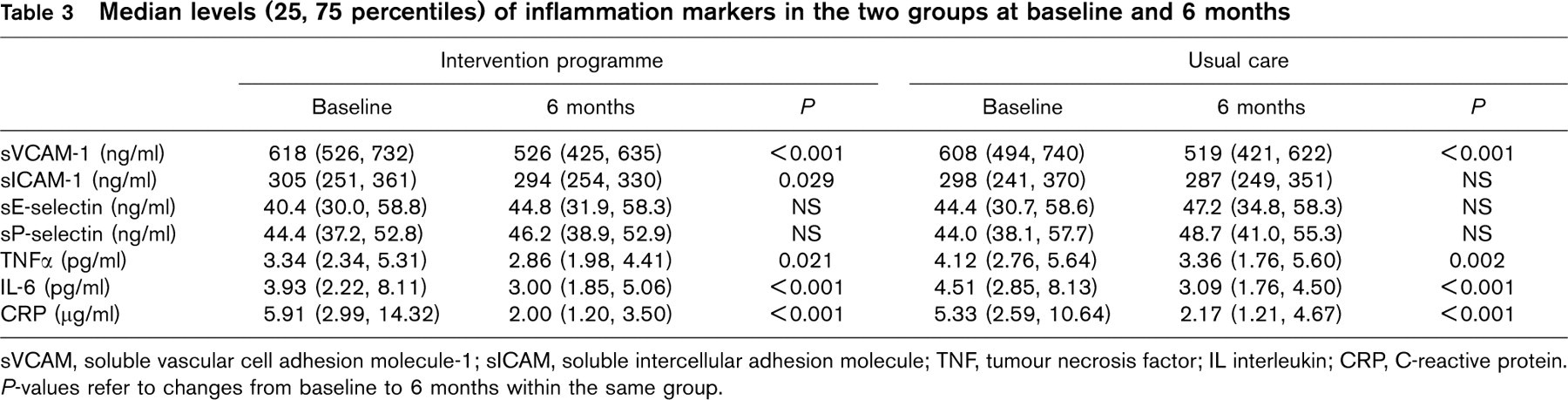
sVCAM, soluble vascular cell adhesion molecule-1; sICAM, soluble intercellular adhesion molecule; TNF, tumour necrosis factor; IL interleukin; CRP, C-reactive protein. P-values refer to changes from baseline to 6 months within the same group.
Association between physical performance and inflammatory markers
Cumulative work correlated significantly with soluble VCAM-1, soluble ICAM-1, IL-6 and CRP at 6 months in all patients (Table 4). In the multiple regression model, cumulative work independently and inversely predicted levels of soluble ICAM-1 (P >0.001), CRP (P >0.001) and IL-6 (P = 0.01). Figure 1 shows median levels of the inflammatory markers in relation to tertiles of cumulative work at 6 months in the total population. The same pattern was observed for all the variables, with lower levels of inflammatory markers associated with higher physical performance, statistically significant for soluble ICAM-1 and CRP (P = 0.005 and P >0.001, respectively).
Discussion
A significant decrease in levels of adhesion molecules, proinflammatory cytokines and CRP was observed 6 months after inclusion, but there were no differences between the intervention programme group with a comprehensive lifestyle intervention programme and the usual care group. This overall reduction was probably mostly due to acute phase influence at baseline combined with the influence of medication during follow-up in both groups. Changes in lifestyle measures might also have contributed to the improvement in all patients.
Spearman's correlation coefficients (r) and level of significance (P) in bivariate correlation between cumulative work and levels of inflammatory markers at 6 months in all patients
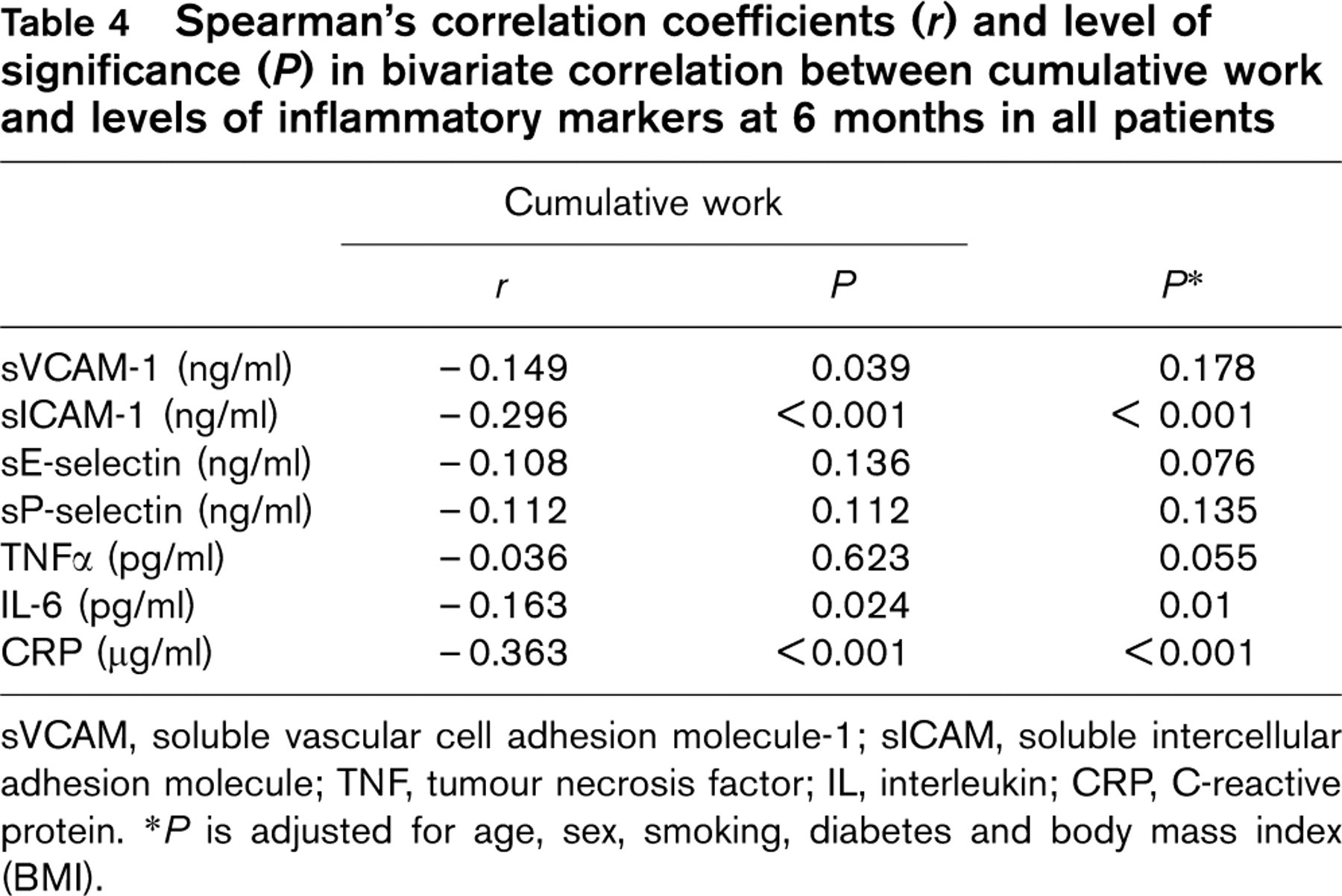
sVCAM, soluble vascular cell adhesion molecule-1; sICAM, soluble intercellular adhesion molecule; TNF, tumour necrosis factor; IL, interleukin; CRP, C-reactive protein. ∗P is adjusted for age, sex, smoking, diabetes and body mass index (BMI).
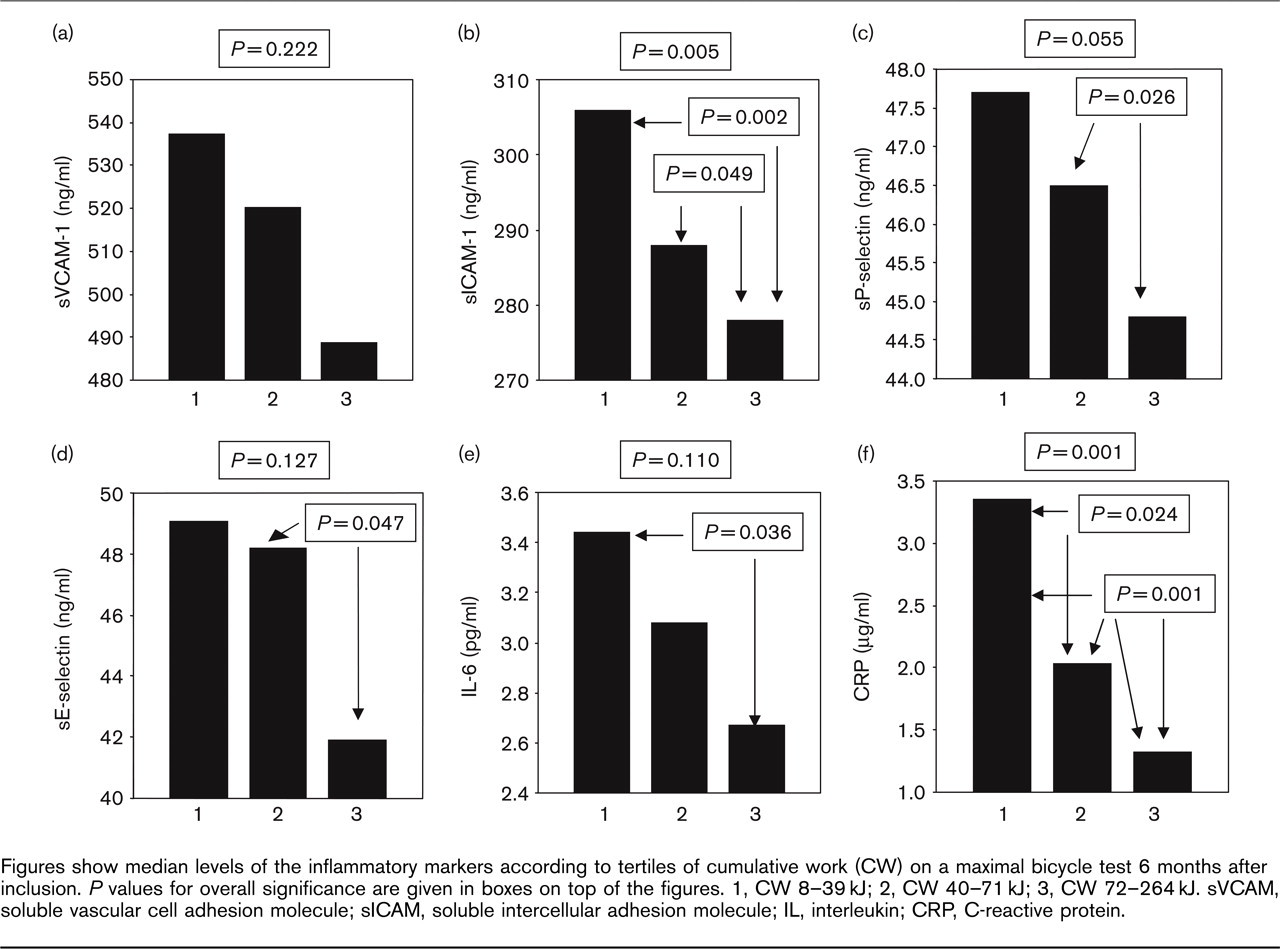
Figures show median levels of the inflammatory markers according to tertiles of cumulative work (CW) on a maximal bicycle test 6 months after inclusion. P values for overall significance are given in boxes on top of the figures. 1, CW 8-39 kJ; 2, CW 40-71 kJ; 3, CW 72-264 kJ. sVCAM, soluble vascular cell adhesion molecule; sICAM, soluble intercellular adhesion molecule; IL, interleukin; CRP, C-reactive protein.
Better diet, reduction in smoking and improved physical performance in the intervention programme patients were obviously not accompanied by a significant reduction in the levels of inflammatory markers when compared with the usual care group. We found higher levels of soluble ICAM-1 in smokers than in non-smokers. This is in accordance with earlier observations in patients with atherosclerotic disease [1, 12] as well as in healthy individuals [12, 20]. Furthermore, Schaberg et al. [30] demonstrated a significantly increased expression of ICAM-1 in lung vessel biopsies of smokers and a positive correlation between the duration of smoking and ICAM-1 expression. A significant correlation between cigarette years (one cigarette year = 20 cigarettes/day for 1 year) and levels of soluble ICAM-1 has also been demonstrated in healthy individuals [12].
The acute phase influence and change in soluble ICAM-1 levels due to clinical stabilization and medication probably explain that no additive effect of smoking cessation was observed in the present study. In addition, the observation period was relatively short and when dividing the study groups further into subgroups based upon smoking status, lack of significance due to small numbers might also be operative. It is, however, still possible that smoking cessation or reduction contribute to the decrease in soluble ICAM-1 levels observed in the whole study population during the observation period.
The improvement in physical performance between 6 weeks and 6 months was equal in the two study groups, but the working capacity at 6 weeks and 6 months was significantly better in the intervention programme when compared with the usual care group. As commented on earlier, due to the submaximal exercise test performed at baseline, we obtained no direct quantitative data on physical fitness at inclusion. No significant difference in heart rate response at 100 W was observed, however, indicating a similar capacity between the two groups. Presuming that physical fitness was similar in the two study groups at baseline, the main improvement was obtained in the intervention programme group during the first 6 weeks of heart school and maintained during the time period up to 6 months. Since the patients were randomly distributed to intervention programme or usual care follow-up, and no other relevant differences were observed at baseline, this seems most probable, but we lack data to confirm this. In the total study population, however, physical performance correlated significantly and inversely with the levels of soluble VCAM-1, soluble ICAM-1, IL-6 and CRP, possibly indicating that physical exercise convey anti-inflammatory effects and may contribute to improvement of endothelial function.
In accordance with this observation, earlier cross-sectional studies have demonstrated enhanced endothelial function in well trained compared with sedentary healthy individuals [31, 32]. Results from longitudinal studies are more conflicting; some showing increased flow-mediated endothelial-dependent dilatation [33, 34], while others find no change with regular physical training in healthy individuals [35, 36]. An improvement in endothelial-dependent vasodilatation with exercise training has also been demonstrated in patients with heart failure [37, 38] and CHD [39–41]. The knowledge about physical activity versus endothelial function on the molecular level is sparse. Sullivan reported similar rest levels of von Willebrand factor and thrombomodulin in plasma of physically fit when compared with sedentary healthy individuals [42]. In a rabbit aorta model, 8 weeks of exercise (5 days a week) has been shown to reduce the expression of VCAM-1, P-selectin and monocyte chemoattractant protein-1 [43]. Furthermore, Arosio et al. demonstrated a reduction in platelet adherence, but could not find any changes in the levels of soluble VCAM-1 or sP-selectin in patients with peripheral artery disease after 2 weeks supervised physical training [44]. We are not aware of any previous study dealing with a possible relationship between long-term physical training and the levels of vascular inflammatory or endothelial markers in patients with CHD.
Whether the improvement in physical performance of our total study population has contributed to the decrease in inflammatory markers in the study period is not possible to deduce from our data. The relatively modest improvement in work capacity from 6 weeks to 6 months in both study groups showed no correlation to changes in inflammatory markers from baseline to 6 months, and 6 weeks’ blood samples were not included in the study protocol.
In conclusion, we found a significant reduction in cell adhesion molecules, proinflammatory cytokines and CRP in CHD patients 6 months after inclusion. No detectable differences in levels of inflammatory markers were recorded in the patients allocated to a comprehensive life style intervention programme when compared with patients who got usual care, in spite of more extensive lifestyle changes in the intervention group. We could, however, demonstrate a significant association between physical performance and markers of vascular inflammation regardless of group belonging, possibly indicating that physical training has an anti-inflammatory effect and may contribute to retard the process of atherosclerosis.
Footnotes
Acknowledgements
We thank members of the Vestfold heart care study group: Torill Holthe, study nurse; Toril Liodden, study nurse, Line Kristin Johnson, study clinical nutritionist, Hospital of Vestfold, Tønsberg, Norway; Ian Ford, PhD, Robertson centre for Biostatistics, University of Glasgow, Scotland; Ingar Holme, PhD, Institute for Biomedical Statistics, Oslo, Norway; Simon Thom, MD, MRCP, Imperial College, St Mary's Hospital, London, UK. We also thank Rolf Schøyen and Anne Britt Lerkerød, Department of Microbiology; Sverre Marstein and Erna Engelstad, Clinical Chemical Laboratory, Hospital of Vestfold, Tønsberg; Lars Eikvar, Department of Clinical Chemistry, Ullevål University Hospital, Oslo, Norway, for their contribution.