
Abstract
Background
The aim of this study was to determine the achievement of National Cholesterol Education Program Adult Treatment Panel III goals in patients with primary hypercholesterolemia starting statin therapy in clinical practice.
Methods and results
Data were collected by 4401 physicians in private practice on 52 848 patients aged 35–65 years (46.3% women, 53.7% men). 56.1% of patients had no manifested atherosclerosis (primary prevention) among whom 34.9% of men and 0.5% of women had a 10-year coronary heart disease risk over 20% (high-risk) as calculated using the Prospective Cardiovascular Münster study (PROCAM) algorithm. After 6 weeks of statins, only 6.9% of these high-risk men and 4.6% of these high-risk women reached their low-density lipoprotein (LDL) cholesterol target of 2.6 mmol/l or below (100 mg/dl). Even after 9 months, only 8.0% of these men and 6.2% of these women achieved their LDL target. No fewer than 57.3% of treated women had a coronary risk below 10%, and 18.8% of women were already at target before statins were prescribed. Of patients 43.9% had manifest atherosclerosis (secondary prevention). After 6 weeks of therapy, only 12.9% of the women and 16.3% of the men in this secondary prevention group reached LDL target levels of 2.6 mmol/l or below. Even after 9 months, only 21.3% of men and 17.3% of women with manifest atherosclerosis reached target LDL.
Conclusions
Most high-risk patients do not achieve LDL targets. Overtreatment of low-risk groups is also very common.
Introduction
Coronary heart disease (CHD) is the most common cause of death in the United States of America and in most European countries. A major risk factor for CHD is hypercholesterolemia. Large clinical studies have shown that it is possible to reduce the coronary event rate in patients at risk by specifically modifying cardiovascular risk factors. In the Prospective Cardiovascular Münster (PROCAM) study, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol level were found to be among the most important predictors for the development of CHD [1].
HMG-CoA-reductase-inhibitors or statins are very effective lipid-lowering agents. They reduce LDL cholesterol by competitively inhibiting the key enzyme of hepatic cholesterol biosynthesis, hydroxymethylglutaryl coenzyme A (HMG-CoA) reductase. Starved of endogenous cholesterol, the cells of the liver respond by over-expressing surface LDL receptors, thus increasing uptake of circulating LDL and lowering blood LDL cholesterol levels. In clinical studies such as the Scandinavian Simvastatin Survival Study [2] and the Heart Protection Study [3], effective LDL cholesterol reduction resulted in a statistically significant decrease in cardiovascular morbidity and mortality. Today, statins are the drugs of first choice for lowering LDL cholesterol.
LDL cholesterol goals depend on a person's absolute risk of coronary heart disease [4, 5]. The LDL cholesterol level is the most important target in the treatment of hypercholesterolemia. LDL cholesterol lowering is also the most important option for patients with risk factors that cannot be modified, such as cardiovascular family history or raised lipoprotein (a) levels. In addition control of blood pressure and blood glucose often cannot reduce the coronary risk sufficiently, so that patients with these risk factors also require effective lowering of LDL cholesterol.
International guidelines such as those of the National Cholesterol Education Program Adult Treatment Panel (NCEP-ATP)III [4] and the guidelines of the International Atherosclerosis Society (IAS) [6] recognize the multifactorial nature of CHD.
The European Action on Secondary Prevention through Intervention to Reduce Events (EUROASPIRE I) I [7, 8] and II [9, 10] studies show, however, that for patients with CHD these findings are not properly implemented in clinical practice. In Italy, for example, a cross-sectional cohort study of guideline adherence to NCEP ATP II with 1168 patients found that only 7.3% achieved their respective goals [11]. In the United States of America the situation is not much better. In one managed care organization of 6538 CHD patients, only 23% reached NCEP ATP II goals [12]. One reason for this could be that the risk of a patient experiencing a cardiovascular event is usually not determined at the start of or during therapy [10]. Quantitative assessment of absolute risk of CHD as a basis of rational risk factor management might therefore be expected to improve treatment of high-risk patients.
The PROCAM study of coronary heart disease risk factors has been running for over 25 years and now includes data on over 37 000 persons [1]. Data from the 10-year follow-up of middle-aged men in PROCAM has been used to construct a simple and effective coronary risk score. The aim of the 4E-Registry (Efficacy Calculation and Measurement of Cardiovascular and Cerebrovascular Events including Physicians' Experience and Evaluation) was to determine cardiovascular risk and the pattern of treatment in patients with primary hypercholesterolemia and statin therapy under practice conditions. The 4E-Registry differs from many previous studies of this nature in that it contains a substantial amount of data on women.
Specifically, the 4E-Registry sought, firstly, to determine the risk factor profile and cardiovascular risk, calculated using the PROCAM multiple logistic regression model, in men and women with primary hypercholesterolemia undergoing statin therapy; secondly, to determine the short- and medium-term change in the risk factor profile in these patients under statin therapy taking into account the treating physicians knowledge of the patient's risk profile; thirdly, to determine the treatment pattern in different risk groups and in men and women; and finally to determine achievement of the NCEP ATP III goals in men and women.
Study population and methods
The 4E-registry was generated by 4401 physicians (cardiologists, internists) in private practice. Beginning in March 2001, each participating physician registered consecutive patients aged 35–65 years that were prescribed statins and met the following criteria: primary hypercholesterolemia unresponsive to diet and lifestyle changes; absence of contra-indications for statin use according to the most recent version of the Physician's Desk Reference; no lipid-lowering medication during previous 4 weeks; total cholesterol ≥ 4.7 mmol/l (180 mg/dl); triglycerides ≤ 4.5 mmol/l (400 mg/dl); blood glucose 2.8–13.9 mmol/l (50–250 mg/dl).
During the first examination the patient's initials, sex, age, size, body weight, history, and blood pressure were documented. The following parameters were measured in a blood sample taken after an overnight fast of at least 12 h: total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides, blood glucose and uric acid. Patients were asked to avoid alcohol for at least 12 h before taking the blood sample. The lipid values were compared with the NCEP ATP III guidelines.
The first re-assessment was performed after 6 weeks, the second after 9 months. Participating physicians also noted compliance with regard to lipid-lowering medication and any changes in the preparation or dosage used.
All patient data were documented in case report forms. The documentation period started in March 2001 and ended on 31 August 2002.
During the documentation period, the treating physicians were supplied with information on the cardiovascular risk of their patients as calculated using PROCAM score.
High risk was defined as the presence of manifest atherosclerosis or of a 10-year calculated risk of a coronary event exceeding 20%, intermediate risk was defined as a 10-year coronary event risk of between 10 and 20%, while low to moderate risk was defined as a 10-year coronary event risk of less than 10%. Thus, by definition, all secondary prevention patients in the registry were regarded as high-risk patients.
The 4E-Registry was intended to represent real-life routine therapy and its results. Therefore, no restrictions were placed on therapy, diagnostic tests or time points for examinations.
Definitions of primary and secondary prevention
Primary prevention was defined as prevention in patients in whom the doctor did not record myocardial infarction, cerebral ischemia, peripheral artery disease or angina pectoris. More than half of the patients (56.1%, n = 29 646) were primary prevention patients, of whom 52.2% were women (n = 15479) and 47.8% were men (n = 14167).
Secondary prevention was defined as prevention in patients who had already suffered myocardial infarction, cerebral ischemia, peripheral artery disease or angina pectoris. Of the 43.9% of patients on secondary prevention (n = 23 202), 61.4% (n = 14 236) were men and 38.6% (n = 8966) were women.
Quality assurance
To ensure proper data recording, an audit was performed in several randomly selected practices by Medicore International AG.
Statistical analysis
Means, standard deviations and proportions were calculated for the group of primary and secondary prevention, for the different risk categories, and for men and women. Scientific evaluation of the data collected was carried out by the Institute of Arteriosclerosis Research at the University of Muenster using SPSS for Windows, version 11.0.1 (SPSS Inc, Chicago, Illinois, USA).
Results
Data were collected on 52 848 consecutive patients (46.3% male, n = 28 403; 53.7% female, n = 24 445) aged 35–65 years. Men and women were similar with regard to age and body mass index (Table 1). Coronary heart disease, peripheral vascular disease and smoking were more common in men than women (Table 2). At the start of the study, mean cholesterol was 7.2 ± 1.4 mmol/l (280 ± 55 mg/dl), LDL cholesterol was 4.8 ± 1.0 mmol/l (186 ± 39 mg/dl), HDL-cholesterol was 1.3 ± 0.4 mmol/l (50 ± 16 mg/dl), and triglycerides were 2.3 ± 0.9 mmol/l (205 ± 80 mg/dl). No major differences existed between the sexes (Table 3). Before the start of treatment, 9.9% of patients were already at their respective target value for LDL cholesterol.
Baseline demographics and lipid values of the study population (mean ± standard deviation)
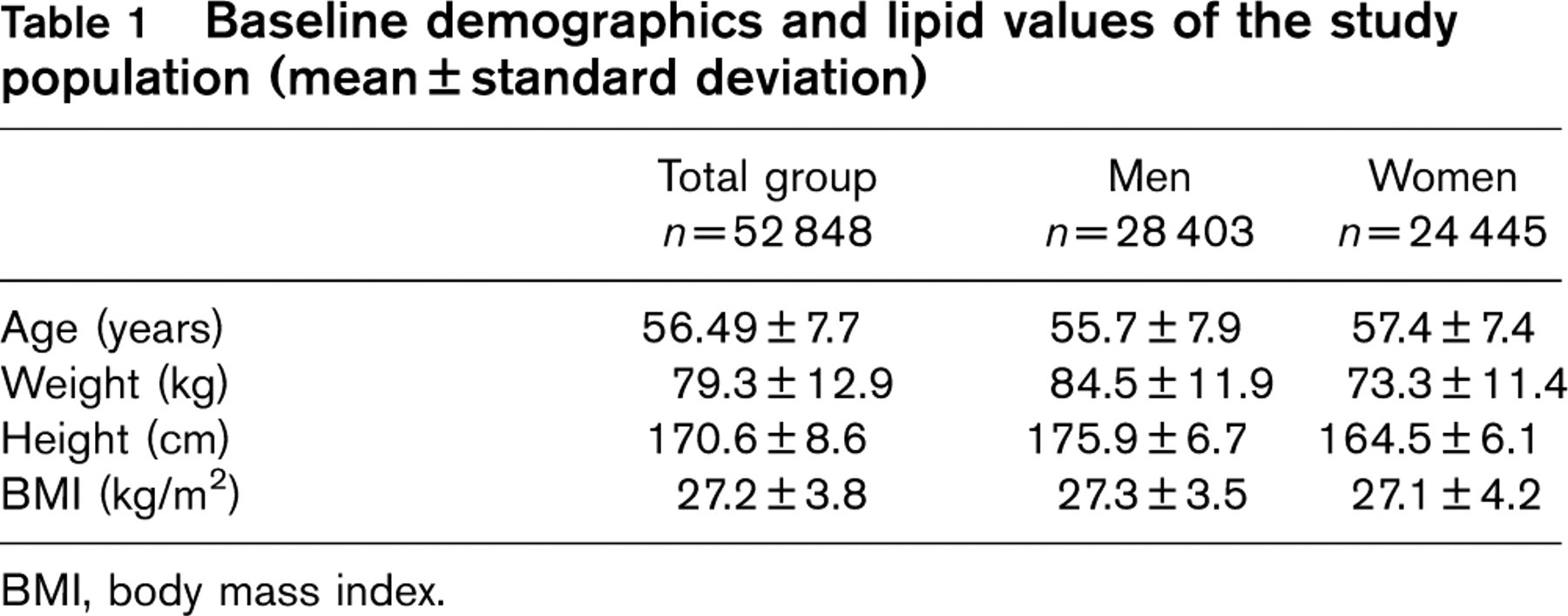
BMI, body mass index.
Baseline percentage risk factors of the study population
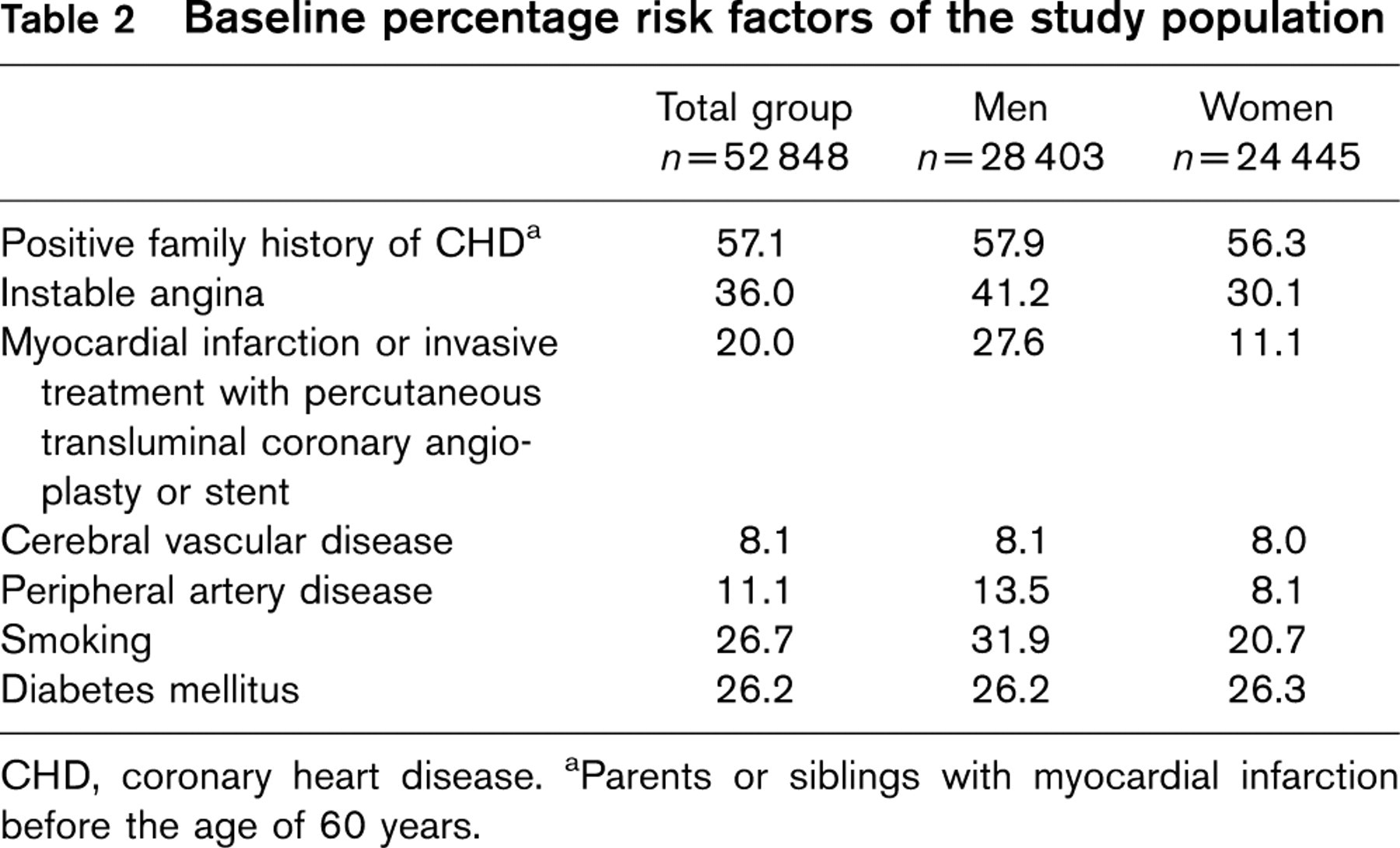
CHD, coronary heart disease.
aParents or siblings with myocardial infarction before the age of 60 years.
Initiation of statin therapy
Most patients (92.1%) received either simvastatin (84.0%) or atorvastatin (8.1%). The remaining 7.9% received cerivastatin (2.8%), pravastatin (2.6%) fluvastatin (1.7%) or lovastatin (0.7%). The most commonly used daily dosages of atorvastatin were 10 mg (51.9% of atorvastatin patients) and 20 mg (45.2% of atorvastatin patients); only 1.1% of patients on atorvastatin received 40 mg of the drug per day. The most common dose of simvastatin was 20 mg/day (49.2% of simvastatin patients) followed by 40 mg (30.3% of simvastatin patients) and 10 mg (18.2% of simvastatin patients).
Six weeks after initiation of statin therapy, mean LDL cholesterol was lowered by 23.7% (Table 3). There was no difference between men and women. After 9 months, lipid values differed little from the results after 6 weeks of therapy. In 17.6% of patients the statin was switched (mostly from cerivastatin, which was withdrawn from the market during the course of this study). In 6186 patients the statin dose was increased and in 6451 patients the dose of statin was reduced.
Primary prevention
Of the patients in the registry, 43.9% (n = 23 202) were in the category of primary prevention and 56.1% (n = 29 646) were in the category of secondary prevention. In primary prevention, patients were assigned to risk categories based on the PROCAM score. Of the 49.9% of the men (n = 14 167) and 63.3% of the women (n = 15 479) who were in the category of primary prevention, 34.9% of men (n = 4938) and 0.5% of women (n = 73) were at high risk, 25.2% of men (n = 3576) and 8.4% of women (n = 1297) were at intermediate risk and 39.9% of men (n = 5653) and 91.5% of women (n = 14 109) were at low to moderate risk (Fig. 1). Before treatment, 16.6% of the patients (n = 8773) (14.2% of men, n = 4030; 18.8% of women n = 4600) in the category of primary prevention already had LDL cholesterol levels below their NCEP ATP III target value.
LDL cholesterol target levels
Of the primary prevention patients at high coronary risk (4938 men, 73 women), only 0.2% of the men (n = 10) and none of the women had a pre-treatment LDL cholesterol level at or below the target of 2.6 mmol/l (100 mg/dl). After 6 weeks of statin therapy, only 6.9% of the men (n = 341) and 4.6% of the women (n = 3) in the high-risk primary prevention cohort achieved target LDL. Even after 9 months of therapy, goal achievement improved only slightly in men to 8% (n = 395) and in women to 6.2% (n = 5; Fig. 3). Thus, in the high-risk group, the discrepancy between treatment goals and reality was dramatic.
Lipid values during surveillance (mean ± standard deviation)
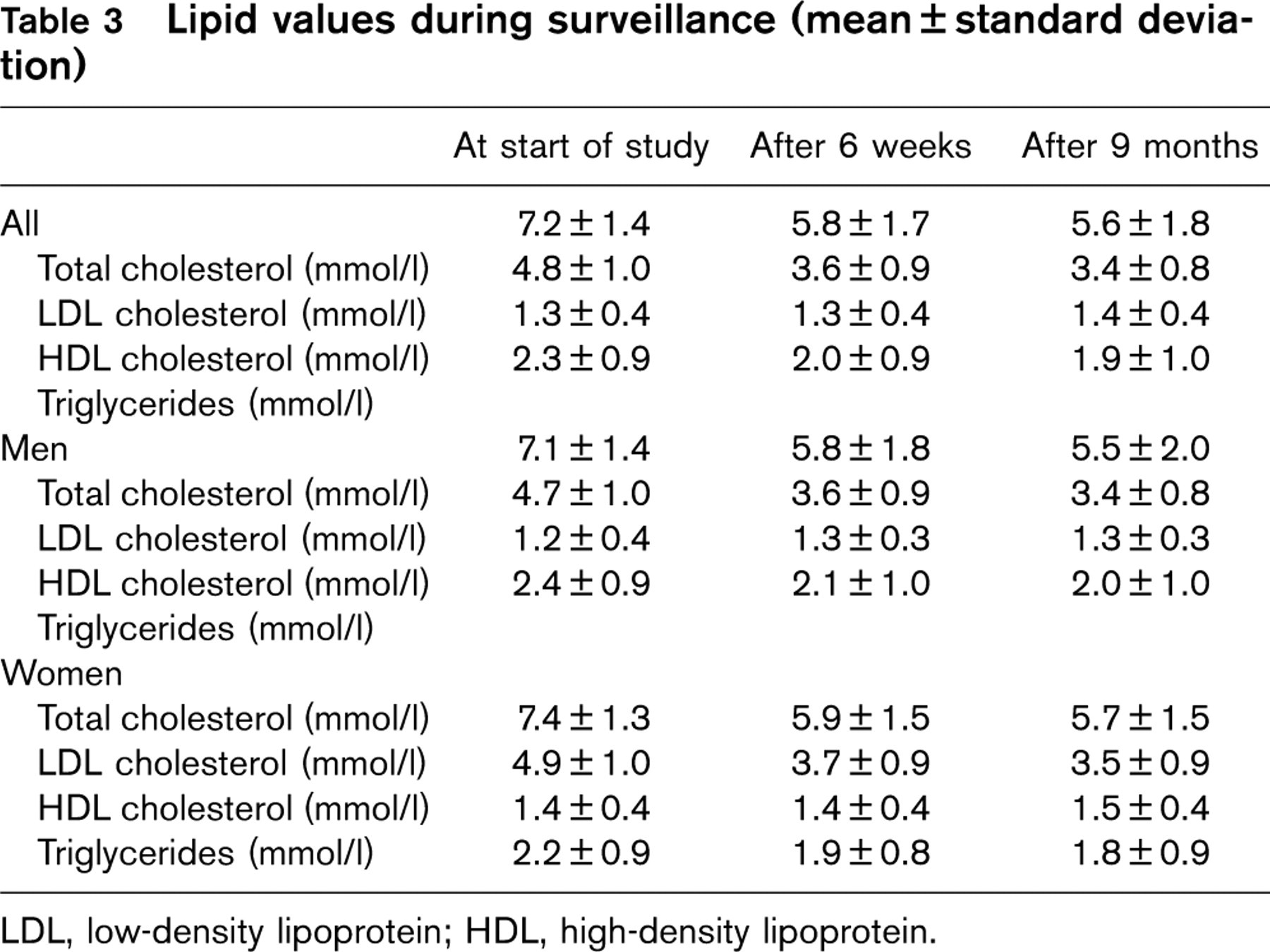
LDL, low-density lipoprotein; HDL, high-density lipoprotein.
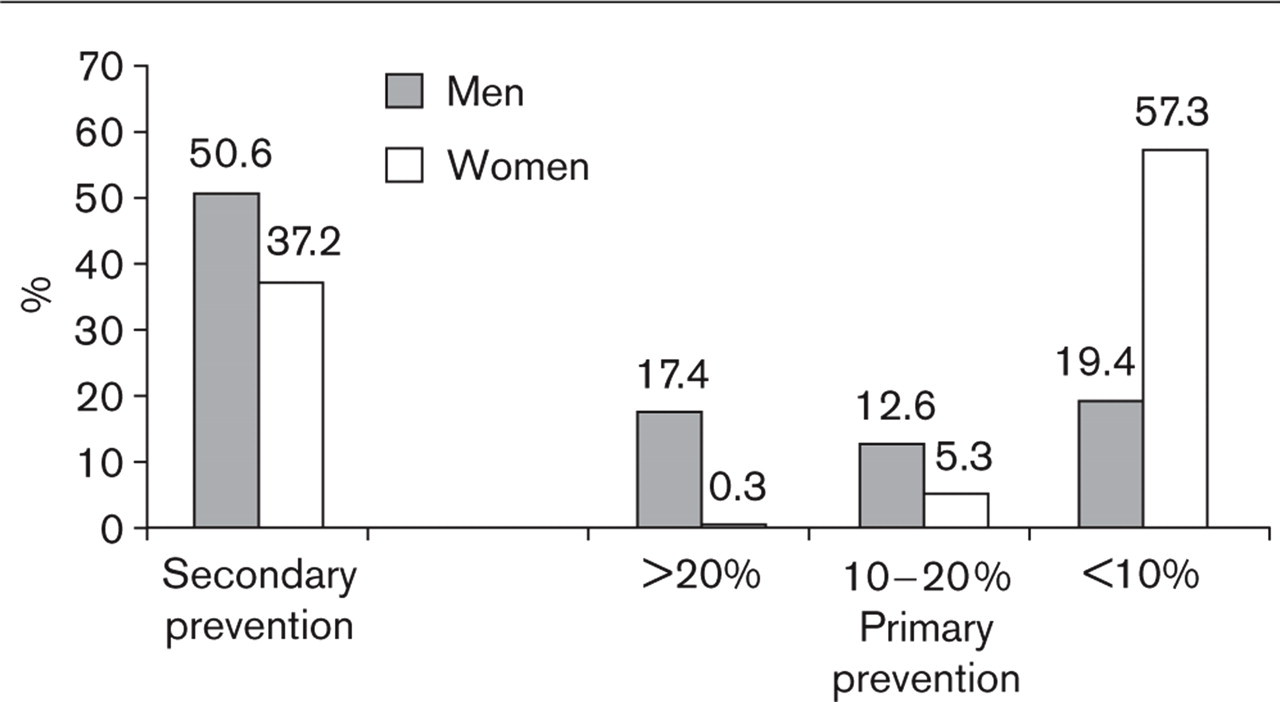
Prevalence of different risk categories: secondary prevention, primary prevention with subgroups of risk estimation > 20% for cardiovascular events within the next 10 years, 10–20% and below 10% in men and women starting statin therapy. High risk (risk of myocardial infarction or sudden coronary death > 20% in 10 years), intermediate risk (10–20% in 10 years), or low to moderate risk (< 10% in 10 years).
Of primary prevention patients at intermediate risk (3576 men, 1297 women), 4.2% of the men (n = 150) and 0.2% of the women (n = 3) had pretreatment LDL cholesterol levels at or below the target of 3.4 mmol/l (130 mg/dl). Of primary prevention patients at low to moderate risk (5653 men, 14 109 women), 33.9% of men (n = 1916) and 21.0% of women (n = 2963) had pre-treatment LDL cholesterol levels at or below the target value of 4.2 mmol/l (160 mg/dl).
Not surprisingly, a higher proportion of the patients in the intermediate and low/moderate risk groups achieved their treatment goals (Fig. 3). Taking into account only those persons at intermediate risk whose pretreatment LDL cholesterol levels exceeded target (3426 men, 1294 women), 31.4% of the men (n = 1076) and 20.0% of the women (n = 260) achieved LDL cholesterol levels at or below the target of 3.4 mmol/l (130 mg/dl) after 6 weeks of statin therapy. Of those at low/moderate risk who were above target before treatment, 65.2% of the men (n = 2435) and 62% of the women (n = 602) achieved LDL cholesterol values at or below the target level of 4.2 mmol/l (160 mg/dl) after 6 weeks of statin administration.
After 9 months of statin therapy of patients in the category of primary prevention, 35.9% of all men (n = 1284) and 26.5% of all women (n = 344) at intermediate risk and 59.6% of all men (n = 3369) and 59.1% of all women (n = 8338) at low/moderate risk achieved their respective LDL targets (Fig. 3).
Secondary prevention
As noted above, all patients in the secondary prevention group as defined in the present study were automatically regarded as being at high risk. Before treatment, 1.5% of the men on secondary prevention (n = 214) had LDL cholesterol levels of 2.6 mmol/l or below (100 mg/dl), 7.8% (n = 1110) had LDL cholesterol levels between 2.6 and 3.4 mmol/l (100 and 130 mg/dl), and 26.1% (n = 3716) had LDL cholesterol levels between 3.4 and 4.2 mmol/l (130 and 160 mg/dl). Thus 64.6% of the men in the category of secondary prevention (n = 9196) had a baseline LDL cholesterol above 4.2 mmol/l (160 mg/dl). Of the 8966 women in the category of secondary prevention, 1.3% (n = 12) had an LDL cholesterol of 2.6 mmol/l or below (100 mg/dl), 5.4% (n = 484) an LDL cholesterol between 2.6 and 3.4 mmol/l (100 and 130 mg/dl), and 21.2% (n = 1901) an LDL cholesterol between 3.4 and 4.2 mmol/l (130 and 160 mg/dl). Thus 72.1% of the women (n = 6569) in the secondary prevention group had LDL cholesterol levels above 4.2 mmol/l (160 mg/dl).
Taking into account those patients in the secondary prevention category who were above target (2.6 mmol/l, 100 mg/dl) before treatment, only 16.3% of the men (n = 2286) and 12.9% of the women (n = 1142) achieved target LDL cholesterol after 6 weeks of statin therapy (Fig. 2). Even after 9 months of statins, only 21.3% of the men (n = 2987) and 17.3% of the women (n = 1531) in the secondary prevention category reached LDL cholesterol levels of 2.6 mmol/l or below (100 mg/dl; Fig. 2).
Development of calculated coronary heart disease risk under treatment
We determined how risk as estimated by the PROCAM score altered during follow-up within the 4E-Registry. The mean improvement in risk in the whole population from baseline to 6 weeks was 40.8%. When risk estimation was compared between baseline and 6 weeks, 9.9% of patients moved from high to intermediate, and 13% from intermediate to low/moderate risk. Too few women were at high risk to allow calculation, but 15.2% of women moved from the intermediate to the low/moderate risk categories (Fig. 3).
Between 6 weeks and 9 months, a further 4.8% of patients moved from high to intermediate risk, 1.4% from high to low/moderate risk, and 6.6% from intermediate to low/moderate risk. In addition, however, 2.8% changed from low/moderate to intermediate risk, 0.5% from low/moderate to high, and 1.8% from intermediate to high risk during this period.
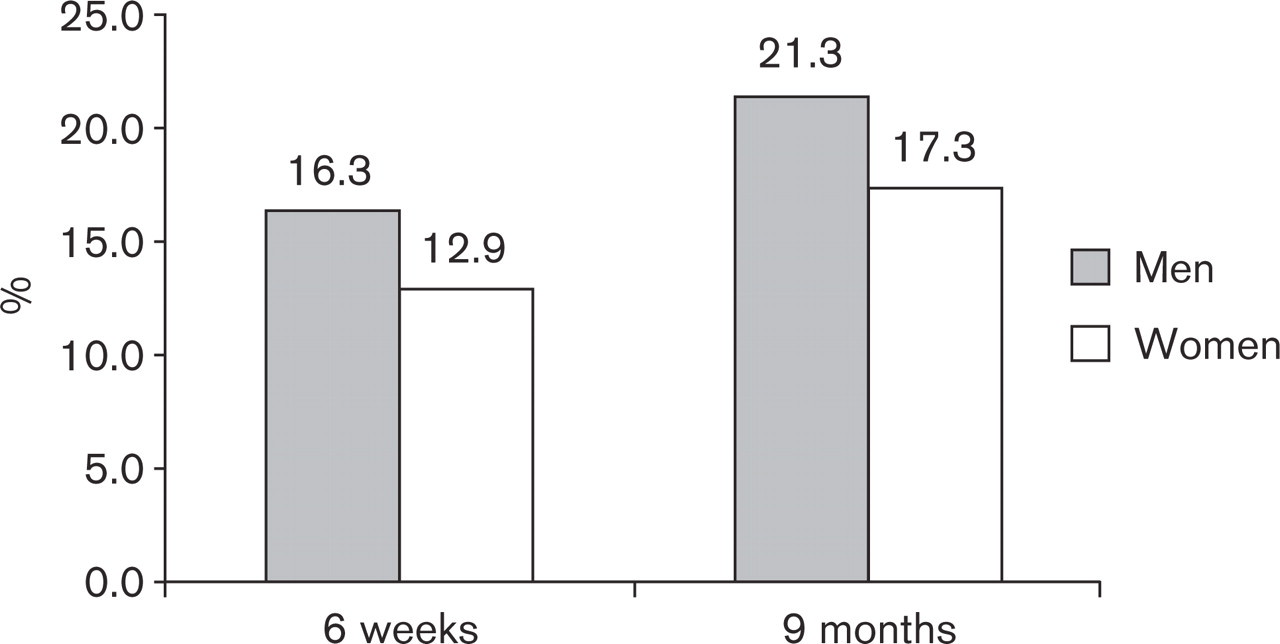
Goal attainment after initiation of statin therapy in men and women in secondary prevention after 6 weeks and 9 months of treatment.
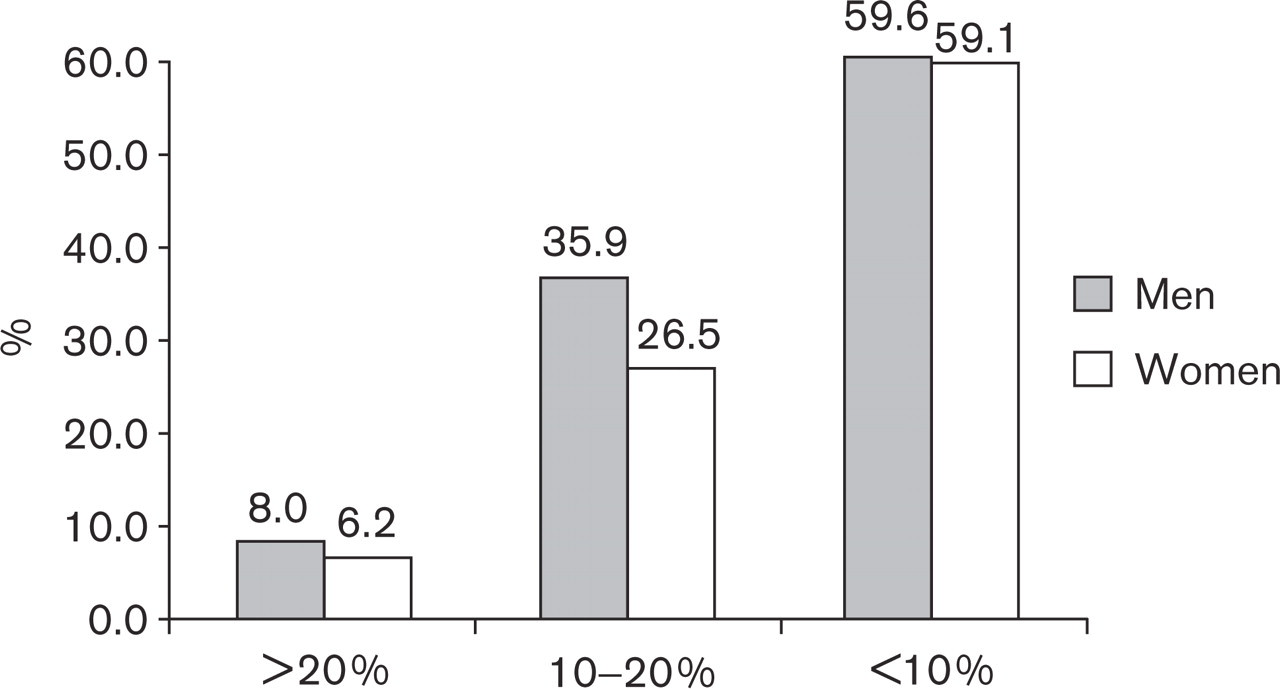
Goal attainment after initiation of statin therapy in men and women in primary prevention after 9 months of treatment according to their risk category using the National Cholesterol Education Program Adult Treatment Panel III guidelines [4].
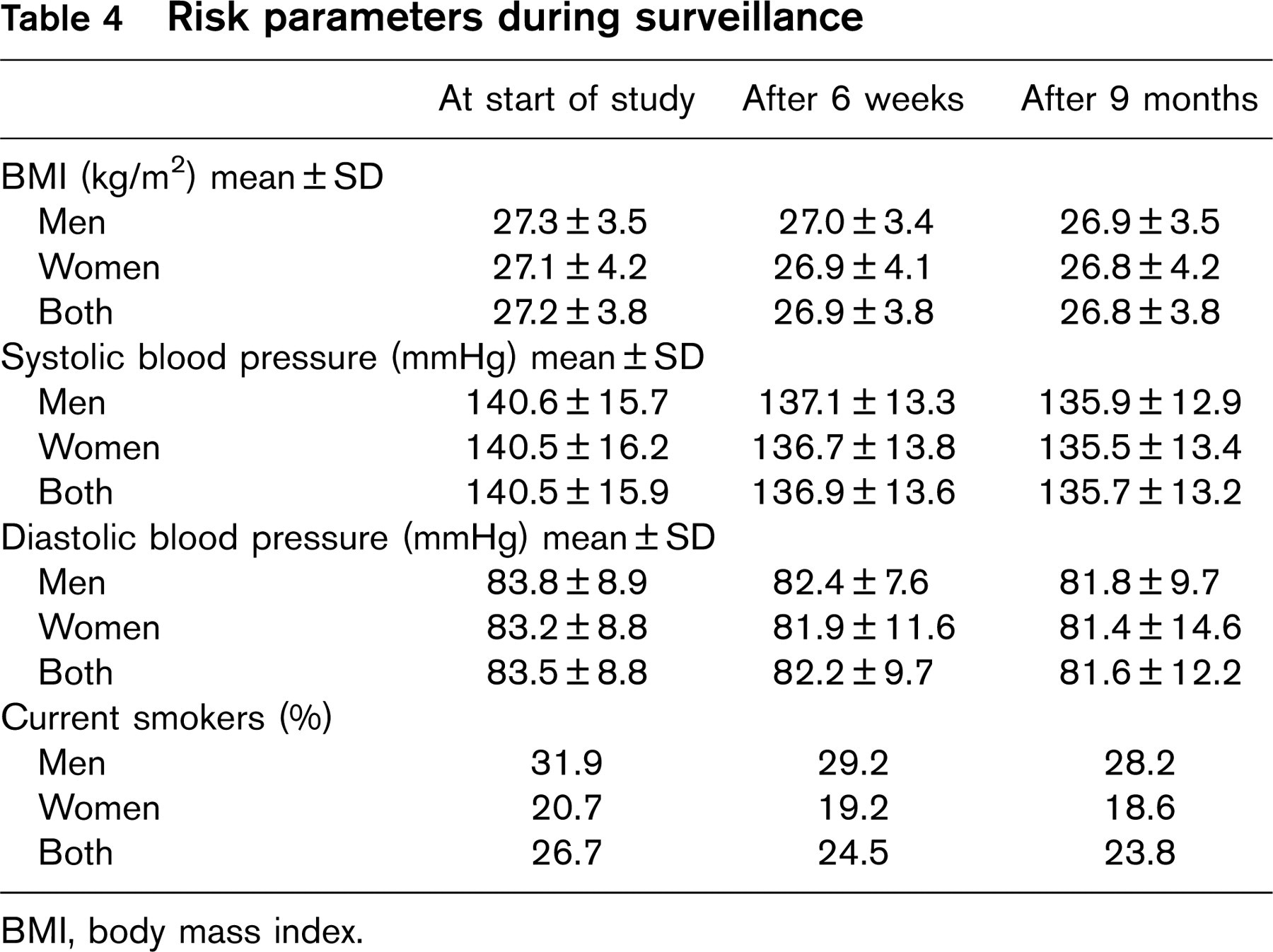
Risk parameters during surveillance
BMI, body mass index.
These changes in risk categories are not solely explained by changes in lipid parameters, because changes in BMI, blood pressure, and smoking status also occurred. Although, these changes were relatively small, they are likely to be of clinical relevance (Table 4).
Discussion
Hypercholesterolemia is one of the best-studied cardiovascular risk factors. Statins are the treatment of choice for treating hypercholesterolemia in patients at increased cardiovascular risk. The treatment pattern is influenced by the patient profile, by the physician's knowledge of treatment guidelines, and by socio-economic factors.
This registry described the treatment pattern of primary hypercholesterolemia in a large cohort of physicians and patients in private practice in Germany. Every participating physician was asked to include consecutively every patient on whom he or she was about to initiate statin therapy. Therefore the data represents current treatment practice in Germany.
More than half of men and more than one-third of the women receiving statin therapy had already had a cardiovascular event. Of these, only 21.3% of men and 17.3% of women reached target values for LDL cholesterol of less than 2.6 mmol/l (100 mg/dl).
Overtreatment was very also common. Thus 19.4% of men and as many as 57.3% of women prescribed statins had a calculated 10-year risk for cardiovascular events of less than 10% (data not shown). Moreover, 18.8% of women and 14.2% of men in the category of primary prevention were already at or below their target LDL cholesterol levels when statins were prescribed.
In patients with established CHD, pharmacotherapy should be prescribed if the LDL cholesterol level exceeds 2.6 mmol/l (100 mg/dl) despite lifestyle modification. In practice, the vast majority of such persons will require statins. CHD patients on statins who achieve their LDL cholesterol goal suffer fewer recurrent cardiovascular events than patients on statins who fail to do so [13]. There is also considerable evidence that goal attainment for this group of patients is cost effective [14].
It is therefore remarkable that goal attainment in this registry was so low, with fewer than 17% of men and 14% of women with established atherosclerosis achieving LDL cholesterol levels of less than 2.6 mmol/l (100 mg/dl).
Moreover, the effectiveness of lipid therapy has been slow to improve. Guidelines with goal values for lipid therapy have been available since 1993, and major updates appeared in 1998 (NCEP ATP III) and 2003 (IAS). In 1999, the German Society of Cardiology published guidelines recommending LDL cholesterol of lower than 2.6 mmol/l (100 mg/dl) in CHD patients [15]. The Joint European Task Force also recently modified their guidelines, accepting an LDL cholesterol goal in CHD patients of less than 2.6 mmol/l (100 mg/dl) [16].
There is some evidence that in this group of patients an even lower LDL cholesterol goal might be useful. In the Heart Protection Study, patients with baseline LDL cholesterol levels below 2.6 mmol/l (100 mg/dl) showed benefit from further lowering of LDL, while in the Pravastatin or Atorvastatin Evaluation and Infection Therapy (PROVE-IT) trial, patients with LDL cholesterol levels of 1.6 mmol/l (62 mg/dl) had a better outcome than patients with an LDL cholesterol of 2.5 mmol/l (96 mg/dl) [17]. The more recently published Treating to New Targets (TNT) study [18] also showed some, albeit slight, additional reduction of cardiovascular events in patients in whom LDL cholesterol was lowered to 2.0 mmol/l (77 mg/dl) by 80 mg atorvastatin compared with patients receiving 10 mg atorvastatin who had a mean LDL cholesterol of 2.1 mmol/l (101 mg/dl).
Other studies have also shown low rates of achievement of LDL targets during treatment in the general population. In a cross-sectional cohort study in Italy from 1994 to 1995, only 1.3% of 1168 treated CHD patients had LDL cholesterol levels below 2.6 mmol/l (100 mg/dl) [11]. The Lipid Treatment Assessment Project in the US from 1996 to 1997 reported that of the CHD patients receiving lipid treatment, only 18% reached target values [19]. In a retrospective study of members of a managed care organization in Minnesota, only 23.3% of patients with CHD reached the goal defined by ATP II [12]. Of the patients not at goal, only 46% were receiving drug therapy. In 1999 a screening of inhabitants in the Belgian town of Lede showed that only 13% of treated women and 24% of the treated men had achieved target LDL cholesterol values [20]. Also in Germany, low levels of achievement of LDL targets have been reported previously. Ruof et al. investigated a German outpatient population with known coronary heart disease who were taking part in a trial comparing atorvastatin and simvastatin [21, 22]. In this population, only 3% of these high-risk patients met target LDL cholesterol levels of below 100 mg/dl, and the overall reduction in LDL-cholesterol level was only 7%, due in part to the fact that only 35% of patients were prescribed lipid-lowering medication. The population described here differs however from that of Ruof and colleagues in that it is non-selected and therefore included many more primary prevention patients without coronary heart disease.
One reason for the difference between goal attainment in clinical studies and the lack in everyday usage might be the statin doses used. Of the patients receiving atorvastatin, half received 10 mg/day, and the other half 20 mg/day. Higher dose of atorvastatin were given in fewer than 3% of patients. For simvastatin the same was true, although slightly more patients received 40 mg daily.
Moreover, in the 4E-Registry, treatment, once started, was rarely modified. The statin dose was increased in only 10% of patients. This might mean that the German doctors are not aware of how to reach target values. The overall percentage decrease in LDL cholesterol on statin therapy in the registry was only 26%, less than expected. This observation is in accordance with the findings of Frolkis [23] who measured LDL reductions in 367 patients in a preventive cardiology practice. These patients were not taking any statins at entry and were placed on standard doses of several statins according to the package insert information. Frolkis observed LDL cholesterol reductions of 26 ± 20% compared with expected reductions of 34 ± 7% according to data from clinical studies. The average LDL cholesterol measured at the start of the survey was about 4.7 mmol/l (180 mg/dl), falling to 3.5 mmol/l (135 mg/dl) on treatment. Assuming that doubling of the statin dose would result in a further 6% reduction in LDL cholesterol [24], even a doubling of the dose would not allow all patients to achieve an LDL cholesterol of less than 2.6 mmol/l (100 mg/dl). Thus in order to reach their LDL cholesterol goal, many high-risk patients will require either the maximum dose of a low potency statin or a statin of higher potency.
Titration of statin dose increases the chances of therapeutic success [25] and reduces the incidence of stroke, myocardial infarction and revascularization. Titration is also cost effective [26].
In the primary prevention patients with an annual CHD risk above 2% (high risk), goal attainment was even worse than in the patients with known atherosclerosis. This is important because this is the group in whom treatment is most cost-effective. Moreover, this group comprises only about 15% of middle-aged men and 3% of middle-aged women and therefore does not place such a drain on resources. Therefore our first goal should be to improve lipid treatment in this group.
A further disturbing point in the present study was that almost as many women as men were being treated with statins. In the 50–60-year age group, men suffer at least three times more CHD than women [11]. Most of the women receiving statins had no CHD and a 10-year risk for coronary events of less than 10%. This finding strongly suggests that the bulk of German doctors in private practice do not base their treatment decisions on risk estimation. Remarkably, this did not change during the life of the registry even though participating physicians received risk evaluations on each of their patients. This indicates that risk estimation of itself may unfortunately not be enough to alter prescribing habits.
Conclusion
The 4E-Registry shows that there are large inconsistencies between guidelines and the treatment patterns of office-based physicians in Germany. Although treatment can be improved by risk prediction and by titration of dosage to reach LDL targets, this does not occur in the vast majority of cases. In addition, overtreatment is common in low-risk groups. Clearly, there is huge room for improvement in the treatment of patients at high risk of CHD.