
Abstract
Background
Exercise-induced ST changes, suggestive of cardiac ischaemia, are found in asymptomatic patients. Methods Gas exchange kinetics were studied during exercise to help to separate patients affected by epicardial coronary disease from those without. Forty-eight patients, without angina symptoms and showing significant changes of ST during exercise, underwent a coronarography and maximal cardiopulmonary exercise test. Thirty-five healthy individuals of matched age and sex underwent a cardiopulmonary exercise test as controls.
Results
Patients were grouped according to the presence (group 1, n = 35) or the absence (group 2, n = 13) of significant coronary lesions at angiography. When corrected for predicted oxygen consumption (VO 2) at peak exercise and at anaerobic threshold, results showed a low VO 2 at peak exercise and anaerobic threshold in group 1 (68 ± 19 and 84 ± 17% of predicted, respectively) compared with normal subjects (91 ± 19 and 96 ± 24% of predicted VO 2) and group 2 patients (86 ± 17 and 96 ± 18%). Also the ischaemic threshold, when normalized for predicted workload at peak exercise, occurred earlier in group 1 (67 ± 22%) than in group 2 (87 ± 19%). The time-related (δ)VO 2/δwork relationship showed a significant flattening above the anaerobic threshold in group 1 (7.4 ± 2.2 versus 9.4 ± 1.4 ml/watt per minute, P<0.01), but not in controls or in group 2. Also the δVO 2/δwork relationship, above the ischaemic threshold, flattened in group 1, but not in group 2.
Conclusion
The suggestion of major coronary disease in patients with exercise-induced ST changes is given by: (i) a flattening of the δVO 2/δwork relationship, above both the ischaemic and anaerobic thresholds; and (ii) low VO 2 values at anaerobic and ischaemic thresholds.
Introduction
Exercise-induced ST changes are sometimes observed in the absence of chest pain or other symptoms related to cardiac ischaemia. This finding may be caused by silent ischaemia, or a so-called ‘false positive test’ [1–3]. The evidence of effort-induced ST changes makes it necessary to perform several diagnostic procedures, including eco-stress, myocardial scintigraphy, positron emission tomography, and almost inevitably in clinical practice, coronary angiography. The presence of relevant exercise-induced cardiac ischaemia is associated with an inadequate cardiac output increase during exercise. In terms of gas exchange analysis, exercise-induced cardiac ischaemia [4] implies that the anaerobic threshold should occur early, and the time-related (δ) oxygen consumption (VO 2)/δwork relationship should flatten above the ischaemic threshold. An early anaerobic threshold means that oxygen delivery is not enough to cope with the muscles’ aerobic metabolic needs [5], and that a flattening of the δVO 2/δwork relationship, which is a straight line in normal individuals, indicates inappropriate oxygen delivery and a relevant anaerobic energy production [6–8]. Therefore, with the hope of selectively discerning a gas exchange pattern suggestive of cardiac ischaemia in patients with ST-segment abnormalities and coronary artery disease, we performed a cardiopulmonary exercise test in all patients who had exercise-induced ST depression and were free of angina symptoms.
Methods
Population
We evaluated all patients who performed a cycloergometer exercise test, which showed ST changes suggestive of effort-induced myocardial ischaemia in the absence of angina. This exercise test was performed to rule out the diagnosis of cardiac ischaemia. The test was performed using a cycloergometer protocol, with 25-watt increments every 2 min. A test was defined as positive in the presence of one of the following: (i) the development of flat or down-sloping ST segment depression of 0.10 mV or greater at 60–80 ms after the J point in three consecutive beats; (ii) the development of up-sloping ST segment depression of 0.15 mV or greater at 60–80 ms after the J point in three consecutive beats; or (iii) the development of ST segment elevation of 0.10mV or greater at 60 ms after the J point in three consecutive beats [9]. The ischaemic threshold was identified when one of the above events occurred. In the absence of angina, severe arrhythmias, dyspnoea or severe hypertension, the test was interrupted by at least two workload increments after the observation of ST changes. Further study exclusion criteria were: (i) left ventricle ejection fraction less than 50% at echocardiography; (ii) lung disease; (iii) ST segment alteration at rest as a result of ischaemia, left ventricle hypertrophy, digitalis or anti-arrhythmic drugs; (iv) pacemakers; (v) effort-induced arrhythmia; (vi) hypertension; (vii) atrial fibrillation; (viii) bundle branch block, either right or left; (ix) anaemia (haemoglobin < 12 g/dl); or (x) patients who, for any reason, did not perform a coronary angiography in the 3 months after the test. Because the test was part of a clinical programme, subjects regularly carried out any therapy that the prescribing physician recommended them to continue. Thirty-five healthy individuals of matched age and sex participated in the study as controls.
Cardiopulmonary exercise test
All individuals who met the study inclusion/exclusion criteria performed a cycloergometer cardiopulmonary exercise test with breath-by-breath analysis of ventilation and exhaled gas (V-Max; Sensor Medics, Yorba Linda, California, USA). The exercise was performed with a ramp protocol, with workload adjusted to achieve the same effort-induced workload as the first test in approximately 10 min. Data are reported as mean over 20 s. The anaerobic threshold was calculated using the V-slope analysis of carbon dioxide production (VCO2)/VO2 [10]. The δVO2/δwork relationship was calculated using linear regression analysis from the end of the second minute of active exercise to peak exercise. The δVO2/δwork relationship was also analysed below and above the anaerobic threshold using data from the second minute of active exercise to the anaerobic threshold, and from the anaerobic threshold to peak exercise, respectively. In patients, the δVO2/δwork relationship was further analysed below and above the ischaemic threshold.
Coronary angiography
Coronary angiography was performed as part of the patients’ routine evaluation. Coronary angiography was carried out using a standard Seldinger technique with multiple projections of coronary arteries. Results were analysed by independent experts, with lesions rated as significant in the case of lesions that generated a lumen reduction greater than 70% or greater than 50% for the left main coronary artery. Patients were grouped according to the presence or absence of vessels with significant lesions.
The study was part of our clinical evaluation for ischaemic heart diseases. It was approved by the ethical committee, and each patient provided written informed consent to participate in the study.
Statistical analysis
Data are reported as mean ± standard deviation. Comparisons were made by paired or unpaired t-tests as appropriate, applying the Bonferroni correction when multiple comparisons were made. Sex differences among the groups were evaluated by X 2 analysis.
Results
Forty-eight patients had significant ST changes without angina during the exercise and met the study inclusion/exclusion criteria. All patients agreed to participate in the study. Patients were grouped according to the presence or the absence of significant coronary lesions at coronary angiography. Group 1 included 35 patients with relevant coronary lesions (single vessel 10 patients, two vessels nine patients, three vessels 16 patients); of these 35 patients, four had left main coronary artery lesions. Group 2 included 13 patients without significant coronary lesions. All the tests were performed without unwanted effects. The mean age and sex distributions are reported in Table 1. The number of women was greater in group 2, explaining the difference in predicted VO2max (Table 1), and confirming the higher incidence of non-ischaemic ST changes in a female population [11]. To avoid interference in the results caused by sex, age, height, etc., we report our data as the percentage of predicted VO2 [12] (Table 1). The anaerobic threshold occurred at a lower workload in patients (76 ± 27 and 63 ± 21 watts in groups 1 and 2, respectively) when compared with normal subjects (92 ± 31 watts; P < 0.05). In contrast, the VO2 anaerobic threshold/predicted VO2 anaerobic threshold (%) occurred at a lower value in group 1 patients when compared with group 2 and normal subjects (Fig. 1). The ischaemic threshold occurred above the anaerobic threshold and showed no differences in group 1 patients when compared with group 2; 101 ± 35 and 86 ± 13 watts, respectively. However, if normalized for predicted workload at peak exercise, the ischaemic threshold occurred earlier in group 1 than in group 2 (67 ± 22 versus 87 ± 19%; P<0.01).
Clinical data of patients (group 1, patients with significant coronary lesions at angiography; group 2, patients without significant coronary lesions) and controls
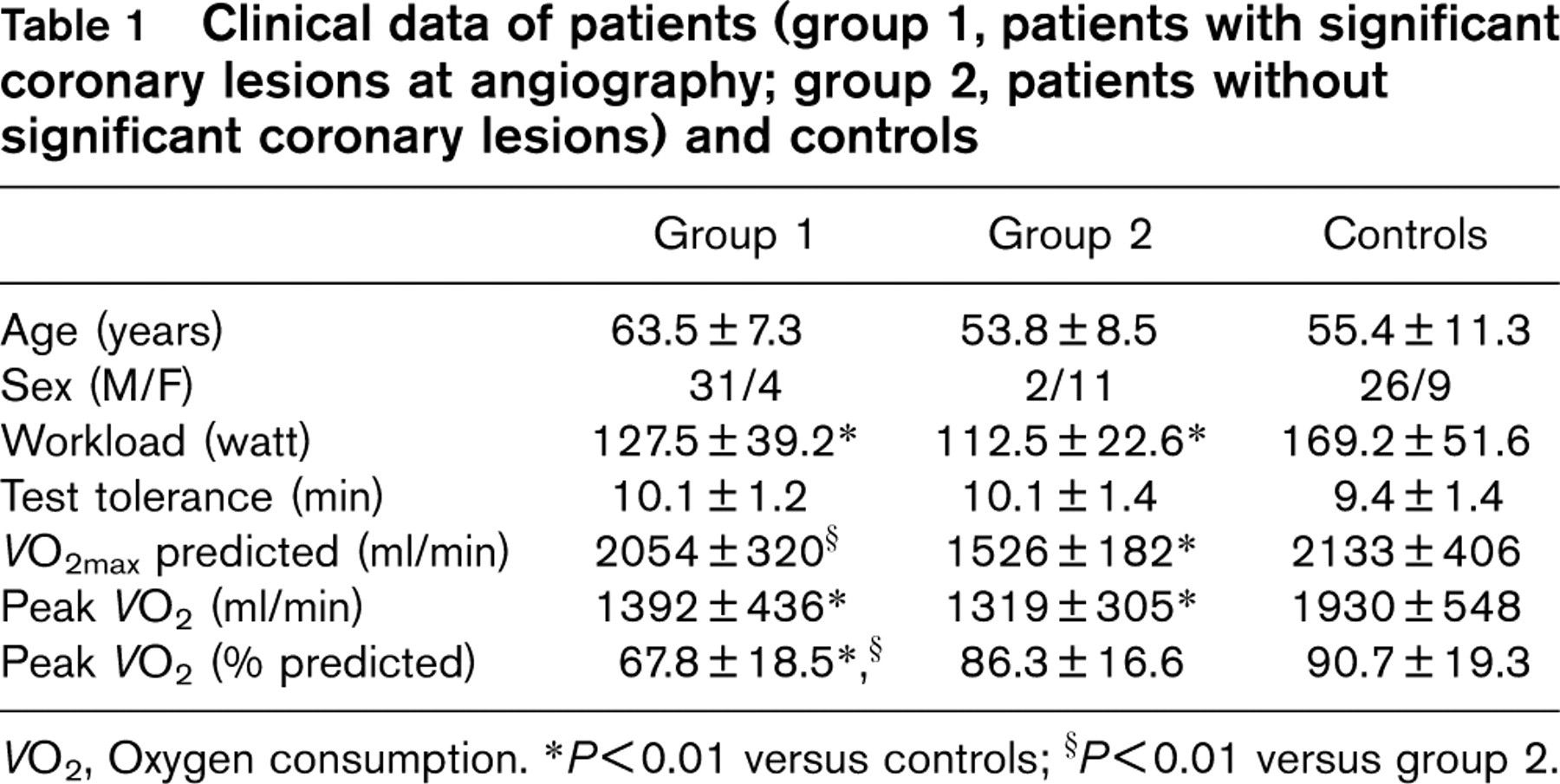
VO2, Oxygen consumption. ∗P<0.01 versus controls; §P<0.01 versus group 2.
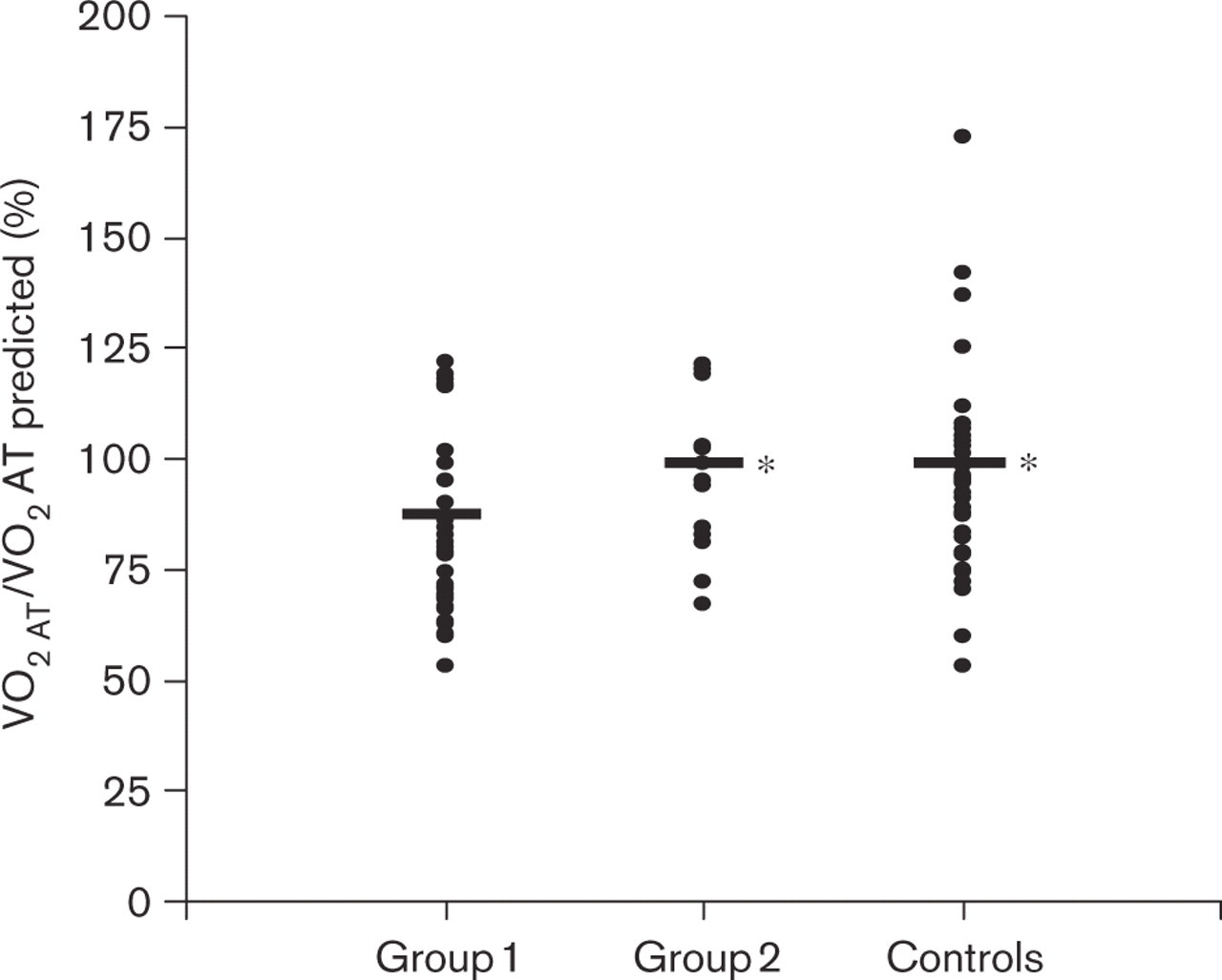
Differences in the oxygen consumption at anaerobic threshold (VO2AT) corrected for the predicted VO2AT in patients in group 1 (with coronary lesions) and group 2 (without coronary lesions) and in controls. ∗P <0.05 versus group 1.
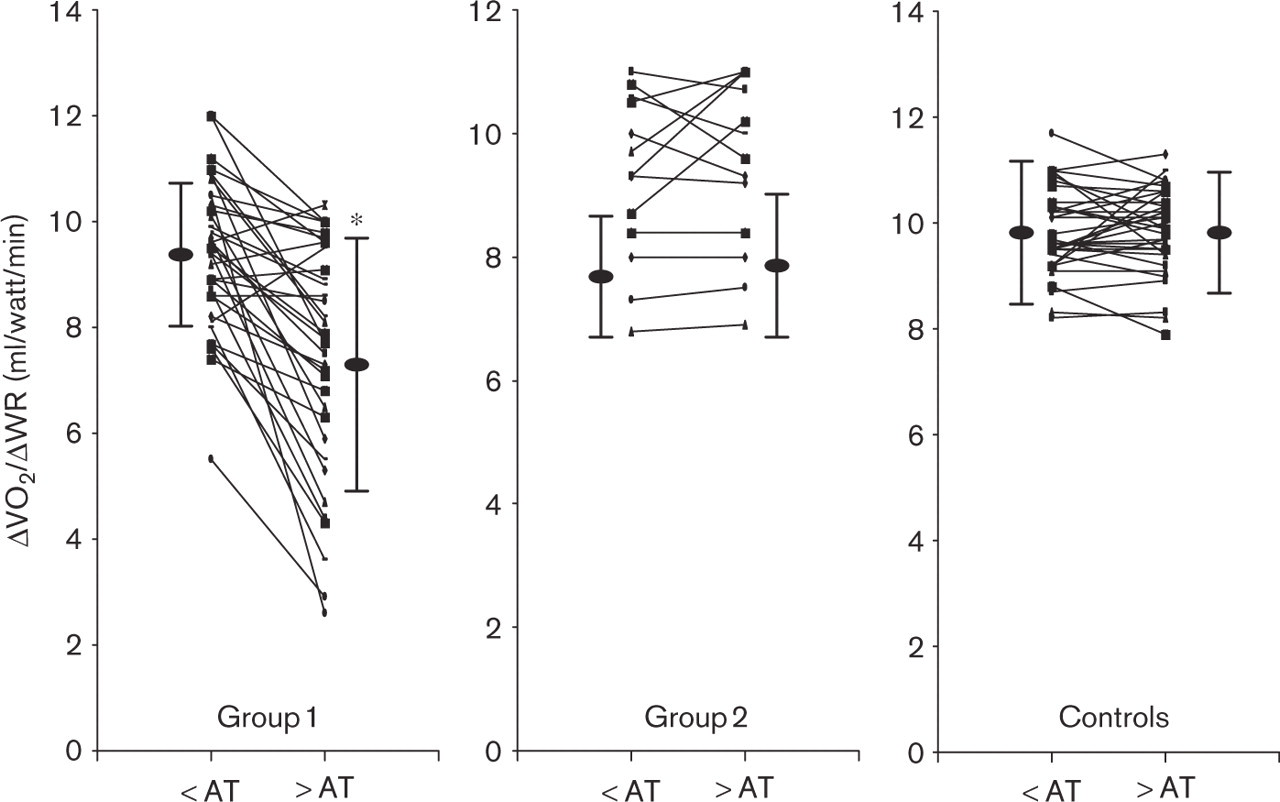
Behaviour of the time-related (δ) oxygen consumption (VO2)/δwork relationship below (>) and above (>) the anaerobic threshold (AT) in patients in group 1 (with coronary lesions, left), group 2 (without coronary lesions, middle) and in controls (right). Mean, standard deviation and single cases are reported. ∗P<0.01 versus < AT.
The δVO2/δwork relationship was not as steep in group 1 patients (8.7 ± 1.2 ml/min per watt) as in group 2 patients (9.3 ± 1.4) and normal subjects (9.8 ± 0.7). As shown in Figure 2, this was caused by a greater flattening of the relationship above the anaerobic threshold in group 1. Also, the δVO2/δwork relationship above the ischaemic threshold flattens to a greater extent in group 1 than in group 2. The ratios between the δVO2/δwork slope, above and below the anaerobic threshold, and above and below the ischaemic threshold are reported in Table 2. Using data from subjects with effort-induced ST depression (groups 1 and 2), we also calculated the specificity and sensitivity to the ratio between the δVO2/δwork slope, above and below the anaerobic threshold and above and below the ischaemic threshold. In both cases, we arbitrarily used a cut-off of 0.9. For the anaerobic threshold, the specificity and sensitivity were 92 and 68%, respectively; for the ischaemic threshold the specificity and sensitivity were 85 and 86%.
Time-related oxygen consumption/work relationship slope behaviour below and above the anaerobic and ischaemic thresholds in patients (group 1, patients with significant coronary lesions at angiography; group 2, patients without significant coronary lesions) and controls
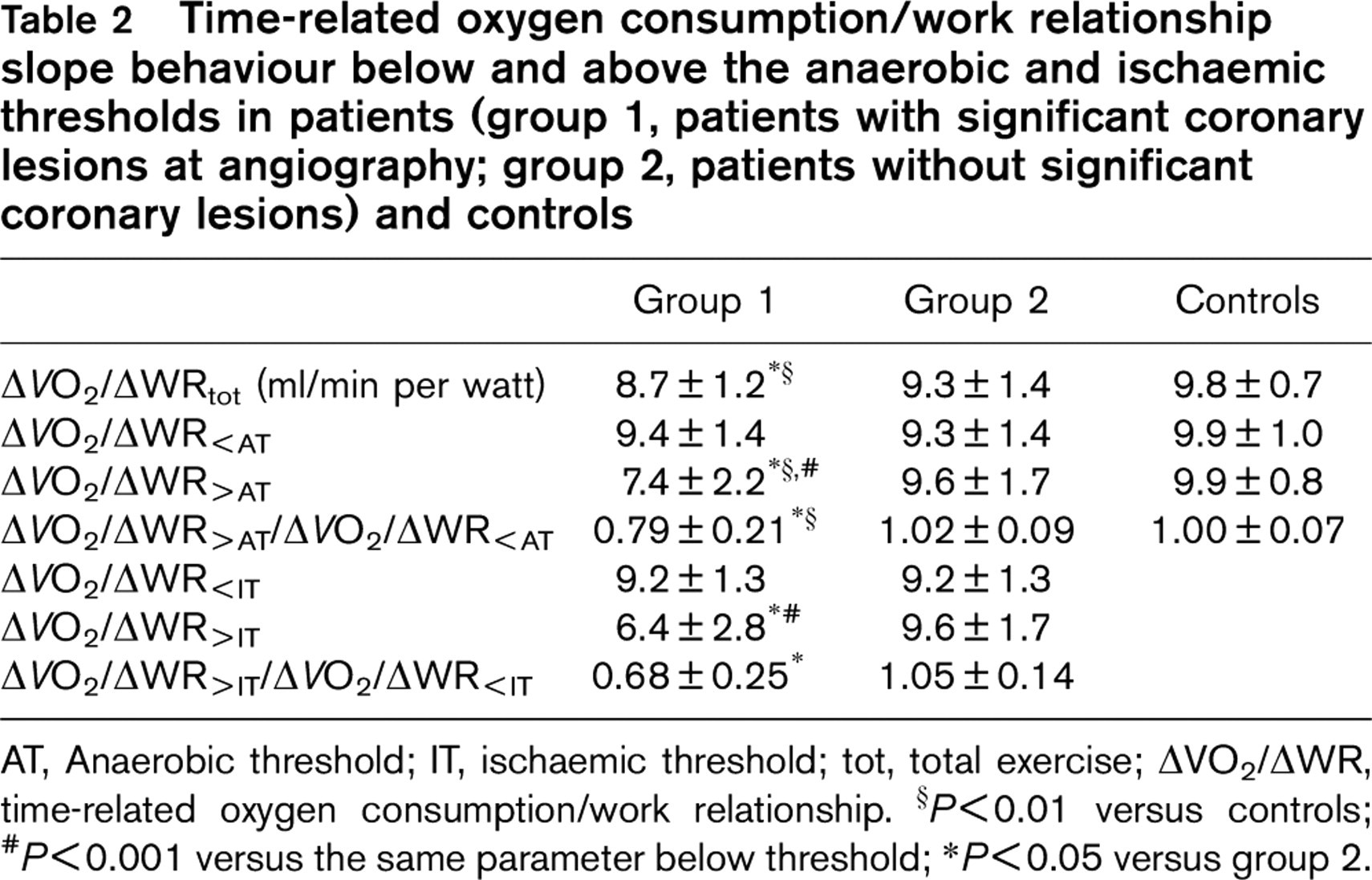
AT, Anaerobic threshold; IT, ischaemic threshold; tot, total exercise; δVO2/δWR, time-related oxygen consumption/work relationship. ∗P < 0.01 versus controls; #P<0.001 versus the same parameter below threshold; ∗P< 0.05 versus group 2.
Discussion
The present study was performed in order to describe the physiological behaviour of gas exchange during exercise in patients with exercise-induced cardiac ischaemia, but free of angina symptoms.
The VO2 was lower, both at peak exercise and at the anaerobic threshold, in patients with symptom-free exercise-induced ST changes, if they were associated with major epicardial coronary lesions. Patients with effort-induced ST changes, but with normal coronary artery, behaved, from a cardiopulmonary exercise point of view, as normal subjects. The anaerobic threshold occurs when oxygen delivery to exercising muscles is not enough to cope with the muscles’ aerobic needs. During myocardial ischaemia, cardiac output decreases [4, 13, 14]. The anaerobic threshold slightly precedes the ischaemic threshold. It is possible that myocardial ischaemia is present before its electrocardiogram appearance [13], particularly when strict electrocardiogram criteria for ischaemia are applied.
The anaerobic metabolism is cardiac output independent. The flattening of the δVO2/δwork relationship suggests that the energy needed for the increased work is caused by anaerobic metabolism. Accordingly, the finding of a flattening of the δVO2/δwork relationship above the ischaemic threshold (or above the anaerobic threshold) in patients with major coronary lesions reinforces the concept that, above the ischaemic threshold, oxygen delivery is reduced in such patients [8, 15].
A significant overlap of data exists among groups, showing that information derived from the cardiopulmonary exercise test cannot be used as the sole criteria for myocardial ischaemia associated with major coronary lesions. Accordingly, the specificity and sensitivity to the ratio between the δVO2/δwork relationship slopes above and below the anaerobic and ischaemic thresholds are relatively modest. On the other hand, if flattening of the δVO2/δwork relationship or an anticipated anaerobic threshold occurs for unexplained reasons in symptom-free patients, exercise-induced cardiac ischaemia should be considered a possibility.
Several study limitations are relevant to the present study. First, the definition of myocardial ischaemia was based on ST changes, and was not confirmed by any other technique. We considered as being caused by ischaemia the ST changes associated with major coronary lesions even if no certain cause–effect relationship was defined. However, in clinical practice, the finding of exercise-induced ST changes and significant coronary lesions is considered reason enough to proceed with some sort of myocardial revascularization. Second, we were unable to devote our attention to the severity of ischaemia and the quantity of myocardium involved. This could have led us to underestimate the cardiopulmonary measurement changes in the presence of minor myocardial involvement, as might occur in patients with microvascular disease who usually have localized myocardial ischaemia. Furthermore, our population with epicardial lesions was too small to carry out a comparative ranking between the severity of coronary lesions and cardiopulmonary changes during exercise. Third, we were unable to evaluate the role of therapy on cardiopulmonary parameters during ischaemia.
In conclusion, the main message of the present work is that, if significant ST changes occur during effort in symptom-free patients, the anaerobic threshold and δVO2/δwork relationship could help to discriminate between ST change causes. If the anaerobic threshold occurs early, and the δVO2/δwork relationship flattens, major coronary artery disease should be considered a possibility.