
Abstract
Background
The aim of this study was to explore the relationship between soy products and the risk of subarachnoid hemorrhage in a case-control study.
Design
A case-control study was conducted.
Methods
Incident subarachnoid hemorrhage cases (n = 201) were identified and individually matched on age (± 2 years) and sex to community (n = 201) controls from April 1992 to March 1997. A factor analysis was conducted to identify dietary patterns in relation to subarachnoid hemorrhage risk.
Results
Soy-rich products were significantly associated with a decreased risk of subarachnoid hemorrhage (lowest versus highest quartile, adjusted odds ratio 0.46; 95% confidence interval 0.18–0.88).
Conclusion
The findings suggest that a diet high in soy products may be protective against the development of subarachnoid hemorrhage.
Introduction
Subarachnoid hemorrhage (SAH) is caused by the rupture of a cerebral aneurysm resulting from focal weakness of the cerebral artery walls [1]. Several epidemiological studies have examined the risk factors of SAH; most have focused on hypertension [2–6], smoking [1–4, 6, 7], alcohol use [2–6], and oral contraceptives [2, 3, 8, 9]. Very little is known, however, about the relationship of dietary factors with the risk of SAH.
Recently, several studies demonstrated in vivo that soy and its products (such as tofu and soy drink) include many isoflavones with estrogen-like activity [9], and were inversely associated with the risk of cardiovascular diseases [10, 11]. Phytoestrogens contained in soy products also have preventive effects for oxidative DNA damage in vascular smooth cells [12]. Taking into account the origination of SAH, these findings suggest that soy products might play a protective role against the occurrence of the condition. To the best of our knowledge, no epidemiological studies have examined the relationship between the intake of soy products and the risk of SAH.
We therefore conducted a case-control study to explore the relationship between the intake frequency of soy products and the risk of SAH using a relatively large number of newly diagnosed patients in Japan.
Methods
The methods have been previously described in detail [13, 14]. Briefly, we recruited all consecutive and incident SAH patients admitted to two large medical hospitals located in Nagoya, Aichi Prefecture, Japan from April 1992 to March 1997. SAH was diagnosed by the presence of one or more aneurysm by surgical inspection based on the findings from computed tomography or angiography.
Cases
The patients were all aged 30–79 years and had experienced the first spontaneous onset of SAH with ruptured cerebral aneurysms. Patients with traumatic SAH were excluded.
Controls
We set up community control subjects with no past history of SAH matching to each patient for age (± 2 years) and sex. Controls were randomly selected from among the general population in the same district as our patients, based on the basic register of residents. If a potential control did not respond after one request, another eligible candidate was selected. The controls were interviewed at home within 2 weeks of completing the interview of patients by the same investigators.
Data collection
All patients were personally interviewed within a month after their admission by two investigators (K.O. and R.H.). We asked the patients to describe their lifestyles during 5 years before the onset of SAH, and the community controls to describe their lifestyles before the interview. When patients were unable to provide any information on their lifestyle and exposures because of early death or severely impaired conditions, proxies (mainly spouses) were interviewed. To minimize information bias, when a patient proxy to a case was interviewed, the proxy to the control was also interviewed even if the control was competent to be interviewed.
Institutional ethics committees in each of the two study hospitals approved the protocol before commencement. All participants provided informed consent, including next of kin for patients who were severely ill, unconscious, or dead, and including proxy respondents for control subjects, after verbal explanation of the study protocol was provided.
Dietary information
Participants were asked about the frequencies of their intake of preserved foods and soy foods with five response options as follows: ‘never/seldom', ‘less than once a week', ‘one to two times per week', ‘three to four times per week', and ‘almost everyday'.
Other data
Information on demographic characteristic (age at diagnosis, sex) and risk factors was collected with the use of a structured questionnaire specifically designed for this case-control study. Hypertension was defined as a history of treated hypertension. Smoking status was classified into current smokers and non-smokers (including ex-smokers and never smokers). Drinking status was classified into current drinkers and non-drinkers (including ex-drinkers and those who never drank alcohol). A positive family history of SAH was defined as when anyone of the participants’ first-degree relatives had experienced SAH in the past. Educational level was classified into three categories (less than high school, high school, college or above).
Statistical analysis
Eating patterns were developed using factor analysis. We focused on factors whose eigenvalues were greater than 1.30. Food items with a loading of 0.40 or greater were considered to contribute to the factor. Factor scores were categorized into quartiles based on the distribution of the control population.
The odds ratio (OR) and its 95% confidence interval (CI) were estimated using multiple conditional logistic regression models in which matched variables (sex and age at diagnosis) and potential confounders (past episode of hypertension, smoking, family history of SAH and educational level) were controlled [15].
Tests for trend in logistic regression analysis were performed by the exposure variable and treating the scored variables as continuous. Since the food frequency questionnaire (FFQ) was completed by 190 (95.4%) of patients and 185 (92.0%) of controls, missing values in the food items and the covariates were replaced by median values.
Results
A total of 204 consecutive patients with spontaneous SAH were identified from the two study hospitals. Three of these patients were excluded because they had other SAH origins (arteriovenous malformation and traumatic SAH), leaving 201 SAH patients eligible for the present analysis. The mean ages were around 59.0 years, accounting for about 60% of the women among SAH patients and community controls. The average interview time was not significantly different between SAH patients and controls. The proportion of proxy interviews was similar between SAH patients and controls. SAH patients included significantly more hypertensive subjects (P = 0.0000), current smokers (P = 0.003), and current drinkers (P < 0.00001), positive family histories of SAH (P=0.0000) and were more educated (P=0.0005).
As shown in Table 1, the ‘soy-rich products’ pattern score characterized by a higher intake of food made from soybeans showed the highest eigenvalue by factor analysis, and was significantly associated with a decreased risk of SAH, even after adjusting for confounding factors (lowest versus highest quartile, adjusted OR 0.46, 95% CI 0.21–0.96).
Discussion
We found a significant inverse relationship between the soy-rich products pattern score and the risk of SAH, even after adjusting confounding factors. This is the first epidemiological finding showing that a diet rich in soy products may have a protective role for the onset of SAH.
Odds ratio for the risk of subarachnoid hemorrhage according to quartile of soy product pattern, Nagoya, Japan, 1992–1997
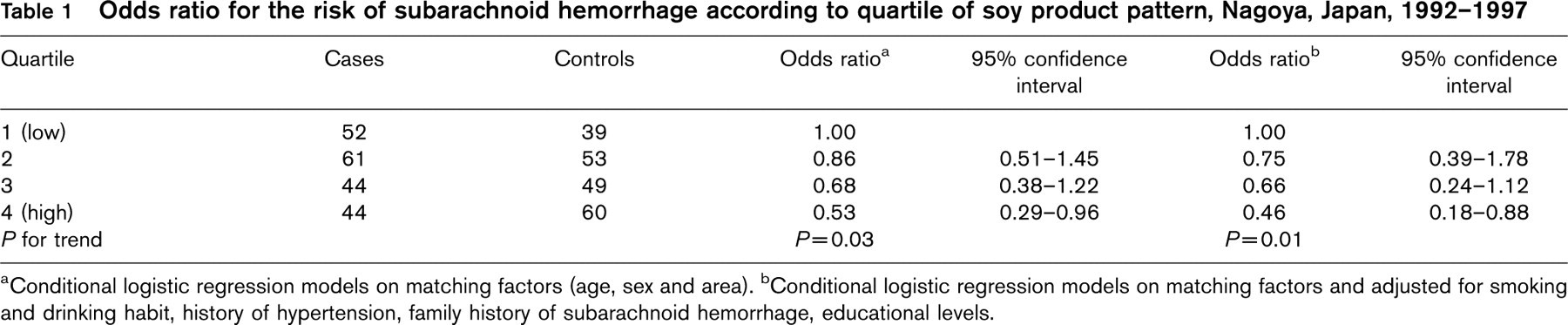
aConditional logistic regression models on matching factors (age, sex and area). bConditional logistic regression models on matching factors and adjusted for smoking and drinking habit, history of hypertension, family history of subarachnoid hemorrhage, educational levels.
A methodological issue is that an FFQ used in this study was not designed to examine the intake amount of selected foods, and so we could not estimate the intake amount of selected foods. Drewnowski and Hann [16] reported that the mean frequencies of food consumption were a significant predictor of dietary outcomes. These findings strongly suggest that any misclassification may not be serious. Moreover, we did not test for the reproducibility of each frequency of consumption of selected foods for these study participants, but the reproducibility appeared to be moderate, with a k-statistic ranging from 0.45 to 0.63 in other study subjects (unpublished data).
In this study, we found a significant inverse relationship between the soy-rich products pattern score and the risk of SAH. Soy isoflavones have also been reported to have vasodilatory effects [17–19], to improve arterial compliance and to serve as an index of elasticity of arteries [20]. We have already demonstrated that earlier age at menarche and nulligravidity related to lower levels of estrogens with bioavailability were associated with an increased risk of SAH. There is evidence that isoflavonic phytoestrogens contained in soy foods may stimulate plasma sex hormone-binding globulin (SHBG) and reduce the percentage of free, biologically active estradiol in the plasma [21–23]. These findings suggest that a higher frequency of the soy food intake might be indirectly associated with a decreased risk of SAH, through the increased level of SHBG.
There are some possible limitations to this study. First, we used SAH patients admitted to hospitals as the case subjects. Since the two hospitals used in this study are central hospitals in the eastern or southern area of the city, almost all patients with severe or acute medical conditions such as SAH patients are usually admitted to these hospitals. In addition, community controls were randomly selected from inhabitants residing in the same areas as SAH patients to ensure identical socio-economic backgrounds among cases and controls. Accordingly, the effects of selection bias, if any, seem to be small. These study designs suggest that our study might be close to a population-based, case–control study. Second, in this study information was provided by proxy respondents in approximately one-third of the cases [for subjects who had died (73%) or were too seriously impaired (27%)]. As previously reported, however, proxy respondents provided acceptable information for smoking [24], episodes of hypertension [24], and dietary information [25]. Moreover, the associations were unaltered after the data were reanalyzed with the exclusion of data obtained from proxy respondents (data not shown). Thirdly, SAH patients had significantly higher proportions of a history of hypertension than controls. It is possible that SAH patients may have changed dietary habits due to a history of hypertension. To assess the possible impact of this potential problem, we repeated the analyses with the exclusion of subjects with history of hypertension, but the results were unaltered.
Finally, the FFQ used in this study was not designed to examine only intake frequency of selected foods, so the relationship between the amount of soy intake and the risk of SAH should be clarified by further studies.
Two strengths of the present investigation warrant mention. First, all SAH patients in this study were newly-diagnosed, and both alive and deceased subjects were included to avoid the effect of survival bias. Second, bias due to disease misclassification is also unlikely because all patients recruited had aneurysmal SAH diagnosed by surgical inspection, whereas control subjects with possible SAH events were not included.
In conclusion, the present studies suggest that a higher frequency of soy food intake may be associated with a decreased risk of SAH.
Footnotes
Acknowledgements
We are very grateful to the staffs of the Department of Cranial Nerve Surgery and Alimentary Disease, Nagoya Daini Red Cross Hospital and of the Department of Cranial Nerve Surgery, Nagaya City Higashi Municipal Hospital for successful co-ordination in data collection.