
Abstract
Background
The kinetics of parasympathetic reactivation after dynamic endurance exercise have been well elucidated. However, autonomic recovery of cardiac function after resistance exercise is not known.
Purpose
The purpose of this study was to assess cardiac autonomic modulations during recovery from acute resistance exercise versus acute endurance exercise.
Methods
Electrocardiogram readings were collected before and 30 min after a single bout of endurance or resistance exercise in 14 male participants (aged 25.3±2.5 years). Heart rate (HR) variability was spectrally decomposed using an autoregressive approach. High frequency (HF) power was considered representative of vagal modulation. All values were expressed in both absolute and normalized units (normalized for change in total power).
Results
A mode-by-time interaction (P≤0.05) was detected for HR, which remained elevated to a greater extent after resistance exercise. Total power was significantly reduced after resistance exercise (P≤0.05) but not endurance exercise. An interaction (P≤0.05) was also detected for both a change in absolute natural log function HF power and natural log function low frequency (LF) power (P≤0.05), as both variables decreased more after resistance exercise. When normalized for changes in total power, interactions in LF and HF power were lost. The LF/HF ratio was significantly increased after both resistance and endurance exercise (P≤0.05).
Conclusion
Greater elevations in HR after acute resistance exercise versus acute endurance exercise may be related to greater reductions in cardiac parasympathetic tone.
Keywords
Introduction
Cardiac autonomic recovery after exercise has important physiological and clinical significance. An assessment of autonomic function after exercise provides a deeper insight into neural cardiovascular regulation with physiological stress. From a clinical standpoint, the risk of sudden cardiac death is increased 17-fold during and up to 30 min after an episode of vigorous exertion such as exercise [1]. It is currently believed that acute alterations in autonomic tone after exercise contribute to the heightened risk [2–4]. Sympathetic hyperactivity and reduced cardiac vagal tone after exercise may underlie this elevated risk [5,6], whereas increased parasympathetic activity during this critical time period may be protective [7].
Heart rate variability (HRV) has been used as a non-invasive means of assessing neuroautonomic modulation on the sinoatrial node [6]. High frequency (HF) oscillations of HRV (0.15–0.40 Hz), as determined by spectral decomposition, are thought to be mediated almost entirely by the vagus nerve and thus represents parasympathetic nervous activity [6]. Oscillations occurring within the low frequency (LF) region of the power spectra (0.04–0.15 Hz) have been attributed to both the vagus and cardiac sympathetic nerves [8], and thus represent parasympathetic and sympathetic nervous activity. Although still a matter of debate [9], the ratio of LF power to HF power (LF/HF) has been employed to assess the overall sympathovagal balance [8]. The kinetics of parasympathetic reactivation affecting heart rate (HR) recovery after dynamic endurance-type exercise have previously been explored using HRV. It appears that within 10–15 min of moderate intensity exercise, vagal modulation is not fully regained, as evidenced by significantly reduced HF power [10,11]. At one hour post-exercise, parasympathetic modulation returns to baseline and may even rebound above resting values [11,12]. The LF/HF ratio has been shown to be increased 20–30 min after exercise [10,13] and may remain elevated for up to 60 min post-exercise [13,14], suggesting a state of greater sympathetic predominance.
Resistance exercise confers many positive health benefits, and is recommended by professional medical organizations for healthy and clinical populations alike [15,16]. The cardiovascular response to resistance exercise is significantly different to that of endurance exercise. Whereas endurance exercise imposes a volume load on the cardiovascular system, resistance exercise exerts intermittent marked pressor responses on the cardiovascular system and is thus characterized primarily as a pressure load. Moreover, autonomic modulation during static compared with dynamic exercise at the same relative workload or at the same mean blood pressure appears to be divergent [17]. Using HRV, Gonzalez-Camarena et al. [17] demonstrated that unlike the parasympathetic withdrawal seen during dynamic exercise, there may actually be an increase in vagal modulation during static exercise, with no change in the LF/HF ratio. It is thus possible that neural modulation on the sinoatrial node after an acute bout of resistance versus endurance exercise may also be disparate. Recovery of the autonomic control of HR after resistance exercise currently remains unknown. Therefore, the purpose of this study was to use spectral decomposition of HRV to assess cardiac autonomic modulations at rest and during recovery from acute resistance versus endurance exercise.
Methods
Subjects
Fourteen moderately active male volunteers aged 21–29 years participated in this study. The activity level was assessed using the Lipid Research Clinics Questionnaire [18]. Subjects had no history of hypertension, renal disease, metabolic disease, or any other diseases that could alter autonomic function. Subjects were excluded if they presented with orthopedic injuries preventing full compliance with the study protocol. Furthermore, they did not smoke or use medications of any kind (including aspirin and anti-inflammatory drugs). Before participation in this project, all subjects gave written informed consent and completed a physical activity readiness questionnaire. This research was approved by the University Institutional Review Board.
Study design
During the first laboratory visit, subjects underwent anthropometric assessment followed by an assessment of aerobic capacity. A series of 10-repetition maximum tests were then conducted for the following exercises: bench press, bent-over row, leg extension, leg curl, military (shoulder) press, biceps curl, close-grip bench press (triceps), and abdominal crunch. Maximal values attained from the aerobic capacity testing and 10-repetition maximum testing were used for the subsequent designation of training loads for acute endurance and resistance exercise bouts.
All testing sessions were conducted at the same time of day (late afternoon) to reduce possible diurnal variations in physiological signals. Subjects were tested in the postprandial state (~3 h) and were asked to refrain from caffeine and alcohol ingestion on testing days. This resulted in a minimum of 16 h since their last caffeine/alcohol ingestion. During the second and third visits, subjects rested quietly in the supine position in a dimly lit room for a period of 15 min. Electrocardiogram readings were then collected for a period of 10 min. Breathing frequency was maintained at 12 breaths per min with the aid of a metronome. After data acquisition, subjects underwent a supervised endurance or resistance exercise bout in accordance with published guidelines [15]. Exercise sessions were assigned in a randomized fashion, and were completed at least 72 h apart. Subjects were advised not to engage in any strenuous physical activity at least 48 h before the study days. The resistance exercise bout consisted of three sets of 10 repetitions of the aforementioned exercises with 90s of rest between sets. Endurance exercise consisted of 30 min of continuous upright stationary cycling at 65% of peak oxygen uptake. Immediately after completion of the exercise protocol, subjects resumed the supine position, at which time all instrumentation was again applied. Paced breathing was resumed and the electrocardiogram signal was then collected for a 10-min epoch, starting 25 min post-exercise (minutes 25–35).
Anthropometric measurement
Body composition was determined using whole-body air displacement plethysmography (Bod Pod; Life Measurement Inc., Concord, California, USA). Height and weight were measured using a stadiometer (to the nearest 0.5 cm) and a beam balance platform scale, respectively. Body mass index was calculated as weight (kg) divided by height (m) squared.
Maximal aerobic capacity
Peak oxygen consumption was assessed using a standardized graded exercise test on a cycle ergometer (Lode Excalibur; Medgraphics, St Paul, Minnesota, USA). Briefly, subjects began cycling at an intensity of 50 watts for a period of 2 min. Intensity was increased in a stepwise fashion by 50 watts every 2 min thereafter until volitional exhaustion was reached. HR was recorded once per minute during the protocol using a Polar Heart Rate Monitor (Polar Electro Inc., Woodbury, New York, USA). Expired gases were analysed using a CosMed Quark b2 breath-by-breath metabolic system, and data were expressed in 20-s averages (CosMed, Rome, Italy). In our laboratory, maximal effort was considered attained when subjects met two of the following four criteria: (1) no change in HR with an increase in exercise workload/intensity; (2) a final rating of perceived exertion score of 17 or greater on the Borg scale (scale 6–20); (3) a respiratory exchange ratio greater than 1.15; and (4) a ‘plateau’ (increase of no more than 150 ml) in oxygen uptake with an increase in workload [19].
Signal acquisition and analysis
Beat-to-beat HR was recorded using a modified CM5 configuration (Biopac Systems, Santa Barbara, California, USA). The electrocardiogram reading was collected online at a sampling rate of 1000 Hz, in real time, and stored on a computer. All data were stored off-line and used for analysis at a later time. Off-line signal processing was performed at 10-min epochs. Data were visually inspected for ectopic beats and noise and linearly interpolated to provide a continuous data stream. HR peaks were automatically detected via an established QRS detection algorithm and used to generate an R–R interval time event series (WinCPRS, Turku, Finland). The continuous data stream was re-sampled at 5 Hz and passed through a low-pass impulse response filter with a cutoff frequency of 0.5Hz [20].
Frequency domain analysis
HR recovery after exercise proceeds in an inherently non-stationary manner. Numerous measures were thus taken to safeguard signal integrity. Briefly, analyses were carried out 25 min after exercise, ensuring that spectral decomposition was performed on the asymptotic portion of the HR recovery curve [11]. Consecutive 60-s datasets, sliding in steps of 10 s, were detrended by removing the polynomial baseline of the time series [11]. Power spectral analysis was performed using a maximum entropy method in order to improve temporal resolution [21]. The optimum order of the autoregressive model was determined by Akaike's information criterion. If this method yielded a model order of less than 16, we used 16 to avoid possible shifting of the spectral peaks [22]. The power was calculated by measuring the area under the peak of the power spectra density curve. Three peaks were revealed and their corresponding bandwidths defined as follows: a HF region (0.15–0.40 Hz) caused by arrhythmic respiratory oscillations that is indicative of parasympathetic modulation of the heart; a LF region (0.04–0.15 Hz) related to baroreflex activity and thermo-regulatory components that is mediated by both the sympathetic and parasympathetic arms of the autonomic nervous system; and a very LF component (< 0.04 Hz) resulting from non-harmonic fractal oscillations of unknown origin. The power spectra were calculated in both absolute and normalized units in order to represent the relative value of each power component as a proportion of the total power. Total power was taken as an index of overall variability [6] and was used as a global marker of vagal modulation [23]. The ratio of normalized LF to HF power (LF/HF ratio) was used as an indicator of sympathovagal balance [8]. A sample power spectrum is provided in three dimensions (Fig. 1; x axis = frequency in Hz; y axis = density beats/min per Hz; and z axis = time in min). All data acquisition and post-acquisition analyses were carried out in accordance with standards put forth by the Task Force of the European Society of Cardiology and North American Society of Pacing and Electrophysiology [6].
Statistical analysis
The Shapiro Wilke's test revealed that the total power and absolute powers of LF and HF were not normally distributed. Therefore, outcome measures were logarithmically transformed (natural log function). This resulted in data meeting assumptions for parametric statistical analysis. A 2 × 2 analysis of variance with repeated measures [mode (endurance versus resistance) by time (rest versus recovery)] was conducted on all dependent variables to compare the effects of an endurance exercise with a resistance exercise bout. If significant interactions were detected, t-tests were further conducted to determine where the interactions occurred. All data are reported as means ± SEM. A priori significance was set at an alpha < 0.05.
Results
Subject characteristics are presented in Table 1. Resting and recovery HR and frequency domain analysis are presented in Table 2. HR was significantly higher during recovery compared with rest after both bouts of exercise (P≤0.05). A mode-by-time interaction was detected (P < 0.05) indicating that the change in HR from rest to recovery was significantly different between bouts (23.5% higher after resistance exercise versus 11.8% higher after endurance exercise).
A mode-by-time interaction was detected for natural log function total power (P≤0.05), indicating greater reductions after resistance versus endurance exercise (18.2 versus 3.4%, respectively). Similarly, a mode-by-time interaction (P< 0.05) was detected for natural log function LF power (P < 0.05), as natural log function LF power was reduced 18.9% after resistance exercise (P < 0.05) but did not change after endurance exercise. When normalized for changes in total power, LF power was higher than at rest after both bouts of exercise (P≤0.05), increasing 25.0% after acute endurance exercise and 23.9% after acute resistance exercise (P≤0.05). There was no difference in the change in normalized LF power from rest to recovery between the endurance and resistance exercise bouts. A mode-by-time interaction (P < 0.05) was detected for natural log function HF power. Decreases in natural log function HF power were greater after acute resistance exercise (26.7%) compared with acute endurance exercise (6.3%). Again, when normalized for changes in total power, no differences in HF power between the groups was detected. Normalized HF power decreased similarly and significantly after both endurance (20.8% reduction) and resistance (25.2% reduction) exercise (P < 0.05). A time effect was detected for the LF/HF ratio, increasing after both resistance (81.5% increase) and endurance (63.9% increase) exercise (P< 0.05), but there were no statistical differences in these increases between the bouts of exercise.
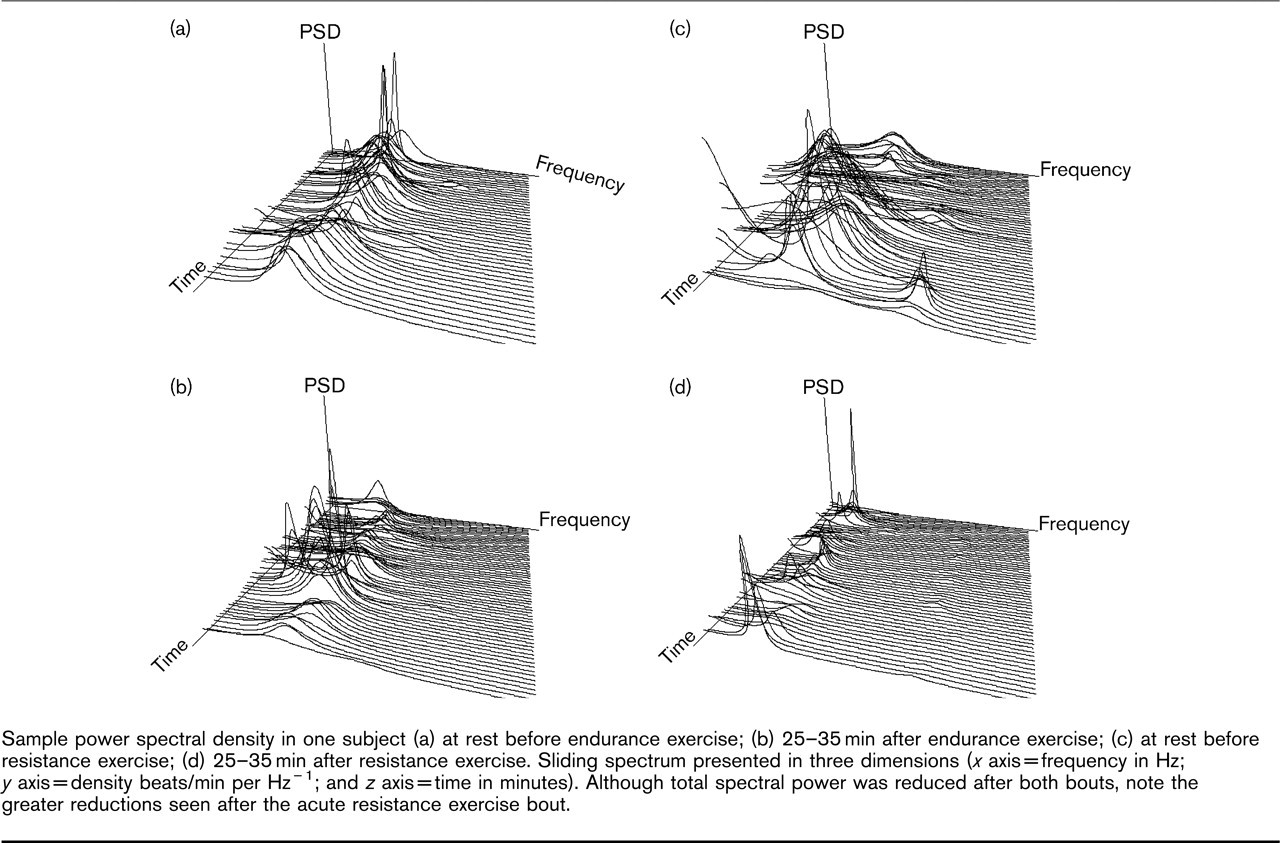
Sample power spectral density in one subject (a) at rest before endurance exercise; (b) 25–35 min after endurance exercise; (c) at rest before resistance exercise; (d) 25–35 min after resistance exercise. Sliding spectrum presented in three dimensions (x axis =frequency in Hz; y axis = density beats/min per Hz−1; and z axis =time in minutes). Although total spectral power was reduced after both bouts, note the greater reductions seen after the acute resistance exercise bout.
Participant characteristics
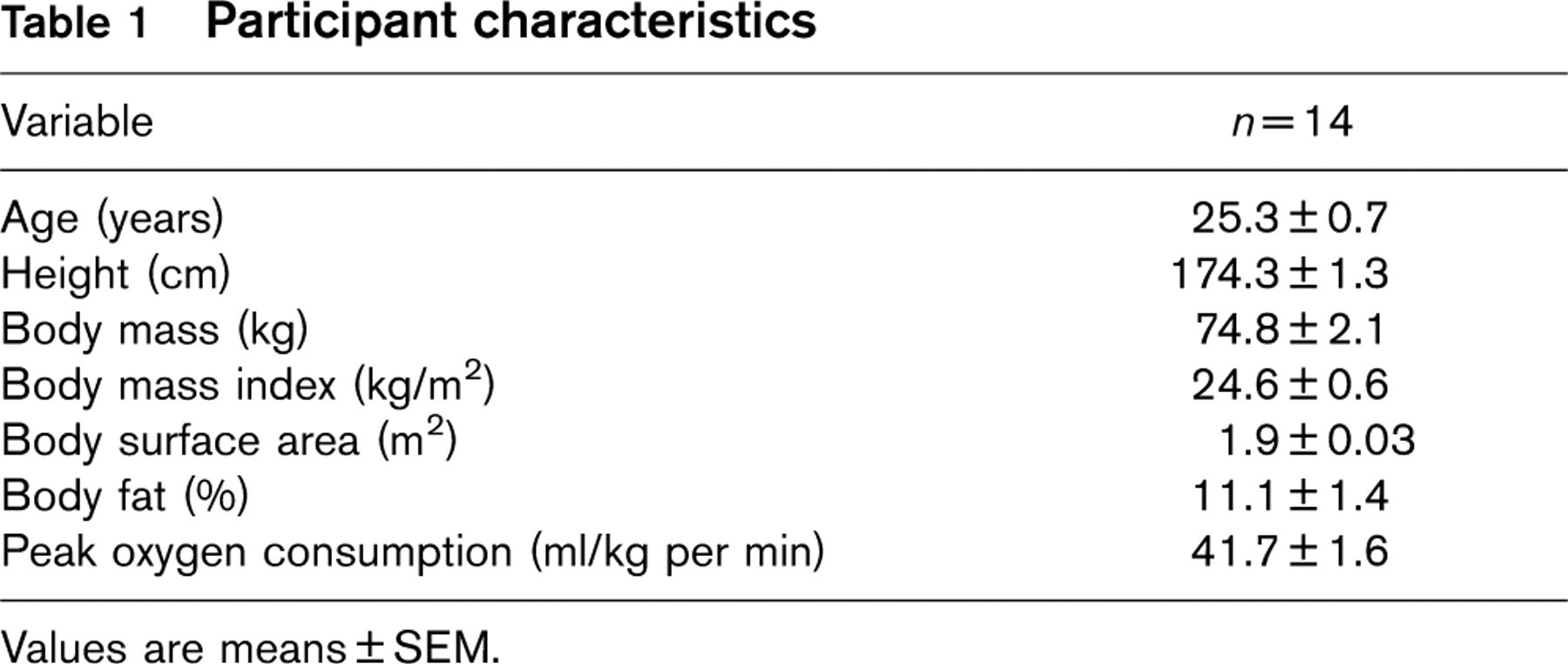
Values are means ± SEM.
Discussion
Several noteworthy findings were observed in the present study. Autonomic cardiovascular control of the heart is not fully regained within 30 min of either acute endurance or resistance exercise. A slight tachycardia was detected after both modes of exercise, but the magnitude of the elevated HR was greater after resistance compared with endurance exercise. There were similar reductions in normalized HF power and similar increases in normalized LF power after both bouts of exercise. The LF/HF ratio increased similarly after both bouts, suggesting a comparable shift towards a state of sympathetic predominance. However, greater reductions in total power were seen after acute resistance exercise, suggesting greater reductions in parasympathetic modulation. The slower HR recovery after acute resistance versus endurance exercise may thus be caused by slower vagal reactivation.
Spectral analysis of heart rate variability at rest and recovery
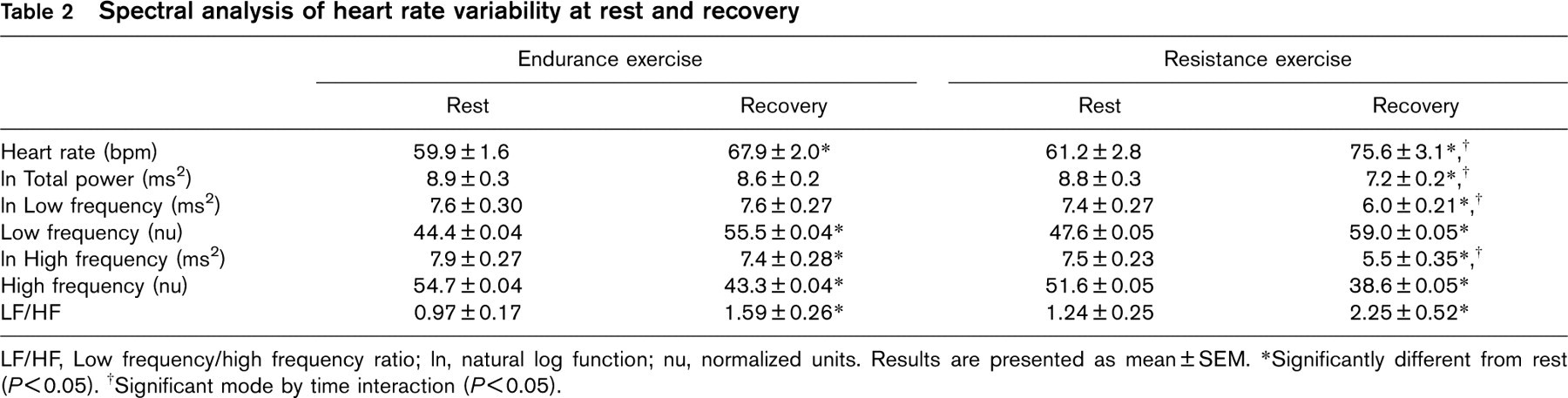
LF/HF, Low frequency/high frequency ratio; In, natural log function; nu, normalized units. Results are presented as mean ± SEM. ∗Significantly different from rest (P < 0.05). †Significant mode by time interaction (P < 0.05).
Our results are in agreement with and contribute further to previous studies examining autonomic regulation after endurance exercise. It has been shown that HR remains elevated 30 min after a single bout of endurance exercise [11,23], and may take upwards of 3 h to recover fully [11]. Alterations in HR towards baseline during late recovery from aerobic/endurance exercise are primarily mediated via a resumption of parasympathetic activity in the sinoatrial node [24]. Although it has been suggested that the prompt decline in HR after exercise may be caused by a progressive retreat of sympathetic activity [25], this has not been supported [26]. It has been demonstrated that beta blockade has no effect on HR recovery kinetics [27], and sympathetic blockade may actually speed recovery [24]. Consistent with the findings of Parekh et al. [23], the total power of HRV in the present study did not change 25–35 min after the bout of endurance exercise. This is not a universal finding, as Mourot et al. [13] noted a significant decrease in total power 20 min after an acute bout of continuous endurance-type exercise. Discrepancies may reside in the study design. Mourot et al. [13] employed a slightly longer and higher intensity endurance exercise stimulus than that used in the present study. Comparable with results attained by Javorka et al. [28], we noted that vagal modulation had not recovered 30 min after a bout of moderate intensity endurance exercise, as evidenced by reduced HF power. Similar findings at 10 and 20 min post-exercise have been reported by others [11,13,23,29]. Furthermore, elevations in the LF/HF ratio above resting values, as seen in the present study, have also been reported previously [26,29]. It appears that full autonomic recovery after endurance exercise of moderate intensity may take more than 1 h [11,13].
Similar to acute endurance exercise, the LF/HF ratio is increased and vagal tonus decreased after an acute bout of resistance exercise, indicating a possible shift towards a state of heightened sympathetic activity. However, parasympathetic activity may be more greatly reduced after resistance exercise, as evidenced by larger reductions in the total spectral power of HRV, and this may explain the greater tachycardia. It should be noted that differences detected for absolute natural log function HF power and absolute natural log function LF power after the different bouts were mediated by these differences in total power. Once the change in total power was accounted for, differences between bouts no longer existed. To our knowledge, this is the first study to assess the recovery of cardiac autonomic control after an acute bout of resistance exercise. Although potential mechanisms governing the disruption in autonomic balance after resistance exercise remain to be expounded, physiological contributors to reduced vagal tone during recovery from exercise that have been alluded to include: (1) shifts in plasma volume [30]; (2) resetting or alterations in the sensitivity of the baroreflex [31]; (3) alterations in the metaboreflex modulation of vagal tone [32]; and (4) a variation in tidal volume affecting respiratory fluctuation in venous return and thus sinus node stretch [33]. If the intensity of the resistance exercise bout were greater than the aerobic exercise bout, the magnitude of these mechanisms would be theorized to be greater, potentiating greater autonomic disruption [23].
Therefore, our findings may ultimately stem from differences in HR during the exercise bouts. Convalescence of the autonomic control of HR is dependent on the HR during the exercise [11] and this may be intensity dependent [23]. Unfortunately, we did not assess HR during or upon immediate completion of the exercise bouts. Previous findings have demonstrated that the HR response per unit of oxygen consumption is significantly exaggerated during resistance-type exercise compared with endurance-type exercise [34]. Unlike endurance exercise, stroke volume does not change [35], or may even slightly decrease [36] during resistance exercise. This is caused by fluctuations in intrathoracic pressures and impeded venous return stemming from physical compression of the vasculature generated by the muscular contraction [34,35]. The maintenance of cardiac output is thus mediated strictly by increases in HR [34]. On the basis of these findings, a higher absolute HR during the bout of resistance exercise compared with the bout of endurance exercise may have instigated longer recovery kinetics.
Sympathetic hyperactivity or reduced cardiac vagal tone after exercise may underlie ischemic heart disease and the pathogenesis of malignant ventricular arrhythmias and sudden cardiac death [4,6]. It has recently been shown that post-myocardial infarction, animals capable of prompt reactivation of parasympathetic nervous activity after exercise are less susceptible to ventricular fibrillation [7]. Similarly, reflex vagal activation during acute myocardial ischemia has been shown to have an antifibrillatory effect in animals susceptible to sudden cardiac death [37,38]. The fast recovery of parasympathetic modulation after exercise thus appears to exert a powerful cardioprotective effect. Whether cardiovascular risk is elevated after acute resistance exercise, as is seen after acute endurance exercise, is unknown. As the overall HRV (i.e. total power) and thus parasympathetic activity may be more greatly suppressed after resistance exercise, it is reasonable to speculate that the risk of untoward cardiovascular events is greater after acute resistance compared with endurance exercise. However, future research will be needed to examine this possibility in target patient populations.
Great care should be taken with the interpretation of our spectral HRV data. The LF/HF ratio may not truly reflect sympathovagal balance [39], and is not universally accepted as such a marker. Parenthetically, it has been suggested that the sympathetic (LF power) and para-sympathetic (HF power) nervous systems do not respond to stimuli in a reciprocal fashion, and the concept of a sympathetic/parasympathetic balance may not be physiologically and mathematically supported [9]. Conversely, others have argued that as one branch is excited the other is inhibited, and there are data supporting the LF/HF ratio as an indicator of this dynamic interaction [40]. According to the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology, vagal afferent activation inhibits sympathetic efferent outflow and sympathetic afferent stimulation reflexively inhibits vagal efferent outflow [6]. Normalized LF and HF power thus ‘emphasizes the controlled and balanced behavior of the two branches of the autonomic nervous system’ [6].
A limitation to the present study may be that findings were influenced by differences in exercise intensity between bouts. However, it is difficult to equate intensity between endurance and resistance exercise, therefore we selected exercise intensity based on standard recommendations [15,16] providing a practical/clinical viewpoint.
In conclusion, HR recovery is not complete 30 min after acute endurance or resistance exercise. Endurance and resistance exercise each have distinctive and slightly variable effects on the autonomic nervous system. It appears that there is an increase in normalized LF power and the LF/HF ratio and a decrease in normalized HF power after both bouts of exercise, suggesting a similar state of sympathetic predominance. However, there are greater reductions in overall HRV (i.e. total power) after acute resistance exercise, suggesting greater vagal suppression. The greater tachycardia after acute resistance versus endurance exercise may thus be related to greater decrements in parasympathetic tone. Future research will be needed to determine the mechanisms of reduced vagal activity as well as the risk of possible cardiovascular events after resistance exercise related to these autonomic modulations.
Footnotes
Acknowledgements
The authors wish to thank all participants for graciously giving of their time. Much gratitude is also extended to Ken Wilund, PhD, for insightful comments pertaining to the preparation of this manuscript. This study was supported by grants from the Gatorade Sports Science Institute and Life Fitness.