
Abstract
Background
Heart rate recovery (HRR1) immediately after exercise reflects parasympathetic activity, which is markedly attenuated in chronic heart failure (CHF) patients. The aim of our study was to examine both continuous and interval exercise training effects on HRR1 in these patients.
Design
The population study consisted of 29 stable CHF patients that participated at a rehabilitation program of 36 sessions, three times per week. Of the 29 patients, 24 completed the program. Patients were randomly assigned to interval {n = 10 [100% peak work rate (WRp) for 30 s, alternating with rest for 30 s]} and to continuous training [n = 14 (50%WRp)].
Methods
All patients performed a symptom-limited cardiopulmonary exercise test on a cycle ergometer before and after the completion of the program. Measurements included peak oxygen uptake (VO2p), anaerobic threshold (AT), WRp, first degree slope of VO2 during the first minute of recovery (VO2/t-slope), chronotropic response [% chronotropic reserve (CR) = (peak HR - resting HR) × 100/(220 - age - resting HR)], HRR1 (HR difference from peak exercise to one minute after).
Results
After the completion of the rehabilitation program there was a significant increase of WRp, VO2p, AT and VO2/t-slope (by 30%, P=0.01; 6%, P=0.01; 10%, P=0.02; and 27%, P=0.03 respectively for continuous training and by 21%, P≤0.05; 8%, P=0.01; 6%, P=NS; and 48%, P=0.02 respectively for interval training). However, only patients exercised under the continuous training regime had a significant increase in HRR1 (15.0±9.0 to 24.0±12bpm; P=0.02) and CR (57±19 to 72±21%, P=0.02), in contrast with those assigned to interval training (HRR1: 21 ± 11 to 21 ± 8 bpm; P=NS and CR: 57 ± 18 to 59 ± 21%, P=NS).
Conclusions
Both continuous and interval exercise training program improves exercise capacity in CHF patients. However, continuous rather than interval exercise training improves early HRR1, a marker of parasympathetic activity, suggesting a greater contribution to the autonomic nervous system.
Keywords
Introduction
Patients with chronic heart failure (CHF) are characterized by an accentuated autonomic dysregulation [1–7] that has been demonstrated to represent one of the main pathophysiological mechanisms of their high mortality rate [8–13]. A recent exercise training meta-analysis of randomized trials has demonstrated an overall mortality reduction in CHF patients who underwent rehabilitation programs [14]. Reduction in the adrenergic and increase in the vagal tone has been recently proposed as the main mechanism underlying improvement by exercise training in functional capacity, quality of life and prognosis in these patients [15,16]. In normal subjects, chronotropic response to exercise (CR) seems to reflect a combination of parasympathetic withdrawal and sympathetic activation [17], while heart rate recovery immediately after exercise reflects mostly parasympathetic reactivation [17,18]. Patients with chronic heart failure present an impaired chronotropic response to exercise [19,20], that has been related to their poor prognosis [21] and a delayed heart rate recovery after exercise [22–24], that preliminary data from a recent report support its negative prognostic significance in these patients [25]. Exercise training resulted in a partial reversal of impaired chronotropic response to exercise in CHF patients in a recent study [26], but evaluation of the effect of rehabilitation program on heart rate recovery (HRR1) in CHF patients has not been determined yet.
Aim of our prospective study was to evaluate the effects of a 12-week supervised exercise rehabilitation program, by continuous or interval training, on early HRR1 after cardiopulmonary exercise testing in CHF patients.
Methods
Study population
The study population consisted of 29 consecutive patients with stable CHF, who were referred to our rehabilitation laboratory by their clinicians, in order to participate at the rehabilitation program. Five patients did not complete the program because of orthopaedic-related problems or inconvenient timetable of the program. The diagnosis of CHF was based on a thorough clinical evaluation and laboratory testing, utilizing non-invasive and invasive tests, including electrocardiogram (ECG), chest roentgenogram, echocardiogram, right-heart catheterization, radionuclide ventriculography, coronary angiography and myocardial biopsy, as clinically indicated. Patients were excluded from the study if there was any contraindication for a cardiopulmonary exercise testing (CPET) according to the American Thoracic Society/American College of Chest Physicians Statement on CPET [27]. The baseline characteristics of all patients that completed the program (n = 24) are listed in Table 1. The mean age was 60.5 ± 9.4 years, (range: 37–74 years) and they had a mean left ventricular ejection fraction of 32.1 ± 10.6%, (range: 15–51%). Patients were under treatment with angiotensin-converting enzyme (ACE)-inhibitors (n = 23; 97%), β-adrenergic blockers (n = 20; 83%), diuretics (n = 21; 85%), spironolactone (n = 15; 63%), digoxin (n = 10; 42%), nitrates (n = 9; 38%), and amiodarone (n = 8; 33%). One of the patients included at the study had a history of type II diabetes mellitus under oral anti-diabetic treatment. Informed consent was obtained from all patients, as approved by the Human Study Committee of our institution.
Study design
The study was designed as a randomized, controlled parallel two-group study. Patients were randomly assigned to continuous or interval training. A randomized stratification was used in order to eliminate differences in baseline characteristics of the two groups, including aetiology of heart failure (dilated or ischaemic cardiomyopathy) and peak work rate WRp; ≥ or > 70 watts achieved by the ramp incremental cycle ergometer test at baseline.
Exercise prescription
All patients underwent exercise endurance training on electro-magnetically braked cycle ergometers (Cateye Ergociser, EC1600; Tokyo, Japan) three times per week, for a total of 36 sessions. Any missed sessions were added to the end of the program, so that the 36 sessions were fulfilled. Patients assigned to continuous training, exercised at intensity, which was initially 50% of baseline WRp for 40 min per day. On the other side, patients assigned to interval training, exercised at a 100% of baseline WRp, alternating 30s of exercise with 30s of rest, for the same duration. Therefore, the total amount of work achieved by session was equal in the two groups. The training intensity was increased every month by an equal magnitude in both groups (by 5% in the continuous and by 10% of WRp in the interval training group). Baseline characteristics for patients of both training groups are reported in Table 1. No statistical difference was found for age and body mass index between the two groups. Supervision during exercise sessions was conducted by physical therapists, exercise physiologists and physicians and included continuous recording of ECG, periodical blood pressure measurements, peripheral oxygen saturation monitoring and Borg evaluation scale.
Baseline characteristics in all patients and according to type of training
Unless specified otherwise, values are presented as means ± SD. BMI, body mass index; NYHA, New York Heart Association; LVEF, left ventricular ejection fraction; ACE, angiotensin-converting enzyme. All differences between group of patients assigned to continuous training and group of patients assigned to interval training were statistically non-significant.
Cardiopulmonary exercise testing
All patients, before and after the completion of the program performed a symptom-limited, ramp-incremental CPET on an electro-magnetically braked cycle ergometer (Ergoline 800; Sensor Medics, Anaheim, California, USA). In order to attain test duration of 8–12 min, the work rate increment was estimated by using Wassermann et al.'s equation [28].
Gas exchange was studied with the patient breathing through a low resistance valve with the nose clamped, using a model Vmax 229 instrument (Sensormedics, Yorba Linda, California, USA) calibrated with a known gas mixture before each test. Oxygen uptake (VO2), carbon dioxide output (VCO2) and ventilation (VE) were measured breath-by-breath with the on-line system.
All measurements were recorded for 2 min at rest and for 2 min unloaded pedalling before exercise, throughout exercise, and for the first 5 min of recovery. Baseline VO2 was the average of measurements for 2min before exercise, with the patient standing. Ventilation frequency was recorded throughout the exercise test and during recovery. Peripheral O2 saturation was monitored continuously by pulse oxymetry. Heart rate (HR) and rhythm were monitored by a MAX 1, 12-lead ECG system (Marquette) and blood pressure was measured every 2 min with a mercury sphygmomanometer. All patients were verbally encouraged to exercise to exhaustion, as defined by intolerable leg fatigue or dyspnoea.
Cardiopulmonary measurements
The gas exchange measurements served to calculate VO2 at peak exercise (VO2p), anaerobic threshold (AT), peak oxygen-pulse (peak VO2/HR) and VE/VCO2 slope between exercise onset and AT. The peak values for VO2, VCO2 and VE were calculated as the average of measurements made during the 20-s period before exercise was terminated. The AT was determined using the V-slope technique [29], and the result was confirmed graphically from a plot of ventilatory equivalent for oxygen (VE/VO2) and carbon dioxide (VE/VCO2) against time. The ventilatory response to exercise was calculated as the slope by linear regression of VE versus VCO2 from the beginning of exercise to AT, where the relationship is linear [30,31]. Peak work rate was defined as the highest work level achieved and maintained at a pedalling frequency of no less than 50 rpm for 30s.
In order to examine VO2 kinetics during the early recovery phase, the first-degree slope of VO2 for the first minute of recovery (VO2/t-slope) was calculated as in previous studies [32–34] by a linear regression model, using an appropriate computerized statistical program. Chronotropic response to exercise was evaluated by the percentage proportion of chronotropic reserve [% CR = (peak HR - resting HR/220 - age - resting HR) × 100] and HR recovery immediately after exercise was evaluated calculating the difference between peak HR and HR one minute later (HRR1).
Statistical analysis
All continuous variables are presented by mean ± SD. Group means of continuous variables were compared by unpaired Student's t-test and categorized variables by χ2 test for baseline characteristics. Cardiopulmonary parameters at baseline and after the completion of the program were compared by using Wilcoxon signed rank test. The level of significance was set at P < 0.05. Percentage difference in continuous variables before and after training interventions is calculated according to the following formula: (post study mean value - pre study mean value) × 100/pre-study mean value. All statistical computations were made by the SPSS statistical package, version 11.0 (SPSS Inc. Chicago, Illinois, USA).
Results
No statistically significant differences were found between patients assigned to continuous and interval training regarding age, body mass index, CHF aetiology, drug treatment, New York Heart Association class and left ventricular ejection fraction, at entry of the study (Table 1). Additionally, before the rehabilitation program there were no statistically significant differences in the two groups of training regarding exercise cardiopulmonary parameters.
After the completion of the rehabilitation program, both CR and HRR1 in the whole population study were found to be higher by 17% (57.1 ± 18.1 to 67.0 ± 21.3%; P < 0.05) and 32% (17.3 ± 10.3 to 22.9 ± 10.8 bpm; P < 0.05), respectively. Furthermore, there was a significant increase at VO2p by 6% (15.5 ± 4.0 to 16.5 ± 4.2 ml/kg per min; P < 0.001), AT by 10% (10.5 ± 2.6 to 11.4 ± 3.0 ml/kg per min2; P < 0.01), WRp by 25% (81.6 ± 30.1 to 101.8 ± 40.5 watts; P < 0.01) and VO2/t-slope by 35% (0.31 ± 0.15 to 0.42 ± 0.17 ml/kg per min2; P < 0.001).
Specifically, patients assigned to interval training had an improvement at VO2p by 8% (P=0.01) (Fig. 3), AT by 6% (P=NS), WRp by 21% (P < 0.05) and VO2/t-slope by 48% (P=0.02) but there was no significant improvement for CR and HRR1 (Table 2). In contrast, in patients exercised by continuous training there was a significant increase by 61% (P=0.02) and 26% (P=0.02) at HRR1 and CR, respectively (Figs 1 and 2), and by 6% at VO2p (P=0.01) (Fig. 3), 10% at AT (P=0.02), 30% in WRp (P=0.01) and 27% at VO2/t-slope (P=0.03) (Table 3).
In both types of exercise, there was no significant improvement at ventilatory response to exercise as assessed by VE/VCO2 slope (32.7 ± 4.9 to 33.2 ± 6.2; P = NS, for continuous training and 34.2 ± 5.6 to 33.4 ± 5.2; P = NS, for interval training).
In patients exercised to continuous training, resting HR decreased after the completion of the program, although it did not reach a statistically significant difference (76.0 ± 14.0 to 71.0 ± 16.0 bpm; P = 0.07), compared with patients exercised to interval training who presented a mild increase at resting HR, although not statistically significant (66.0 ± 17.0 to 70.0 ± 14.0 bpm; P = NS). After the completion of the rehabilitation program, no statistically significant differences were noted between the two groups for the exercise parameters, but heart rate at peak exercise was found to be higher in the group of continuous training (P < 0.05). CR to exercise and HRR1 were also higher after continuous training in contrast to interval training but their difference did not reach statistically significance, [(P = 0.08) and (P = 0.1), respectively; Tables 2 and 3].
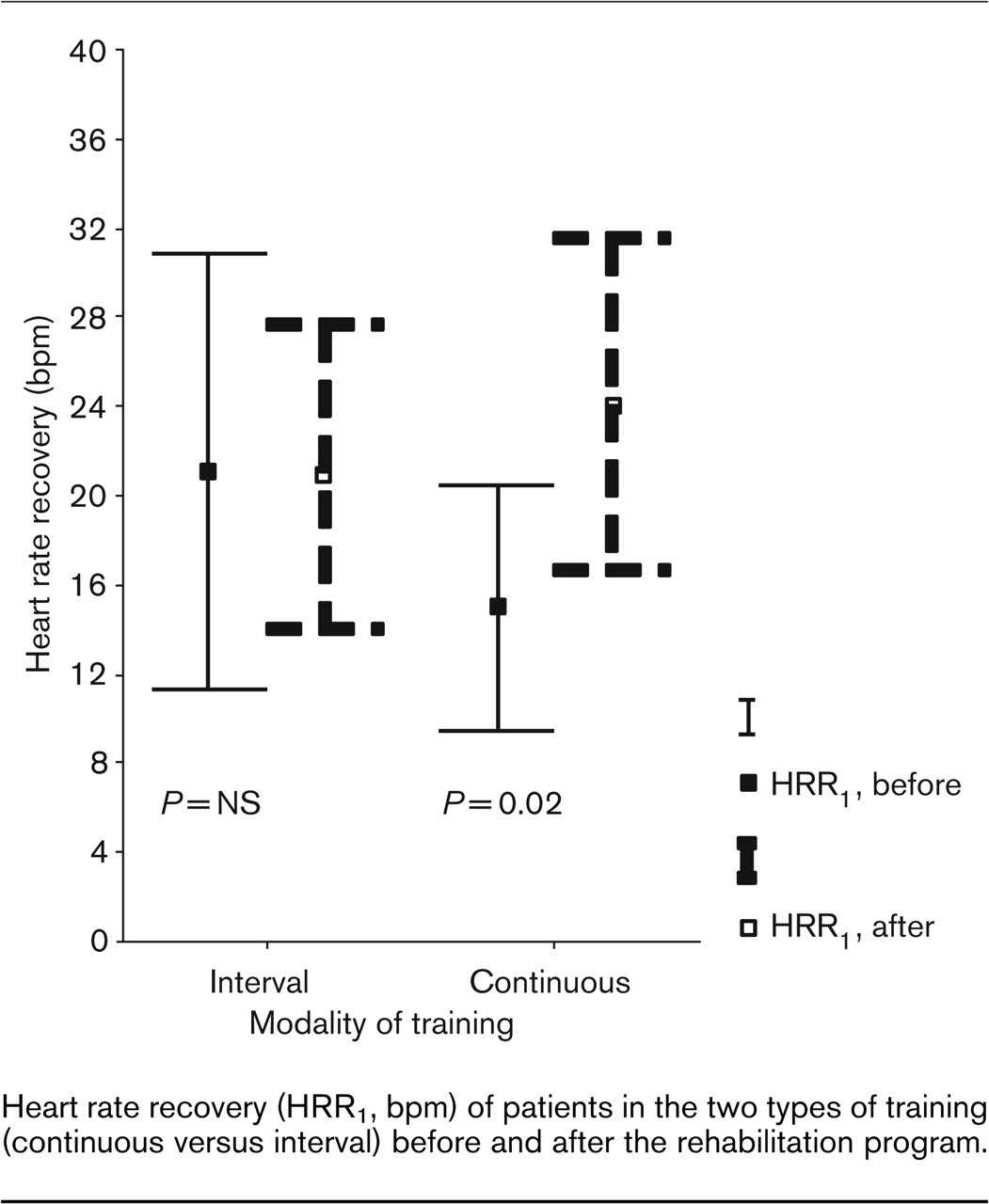
Heart rate recovery (HRR1, bpm) of patients in the two types of training (continuous versus interval) before and after the rehabilitation program.
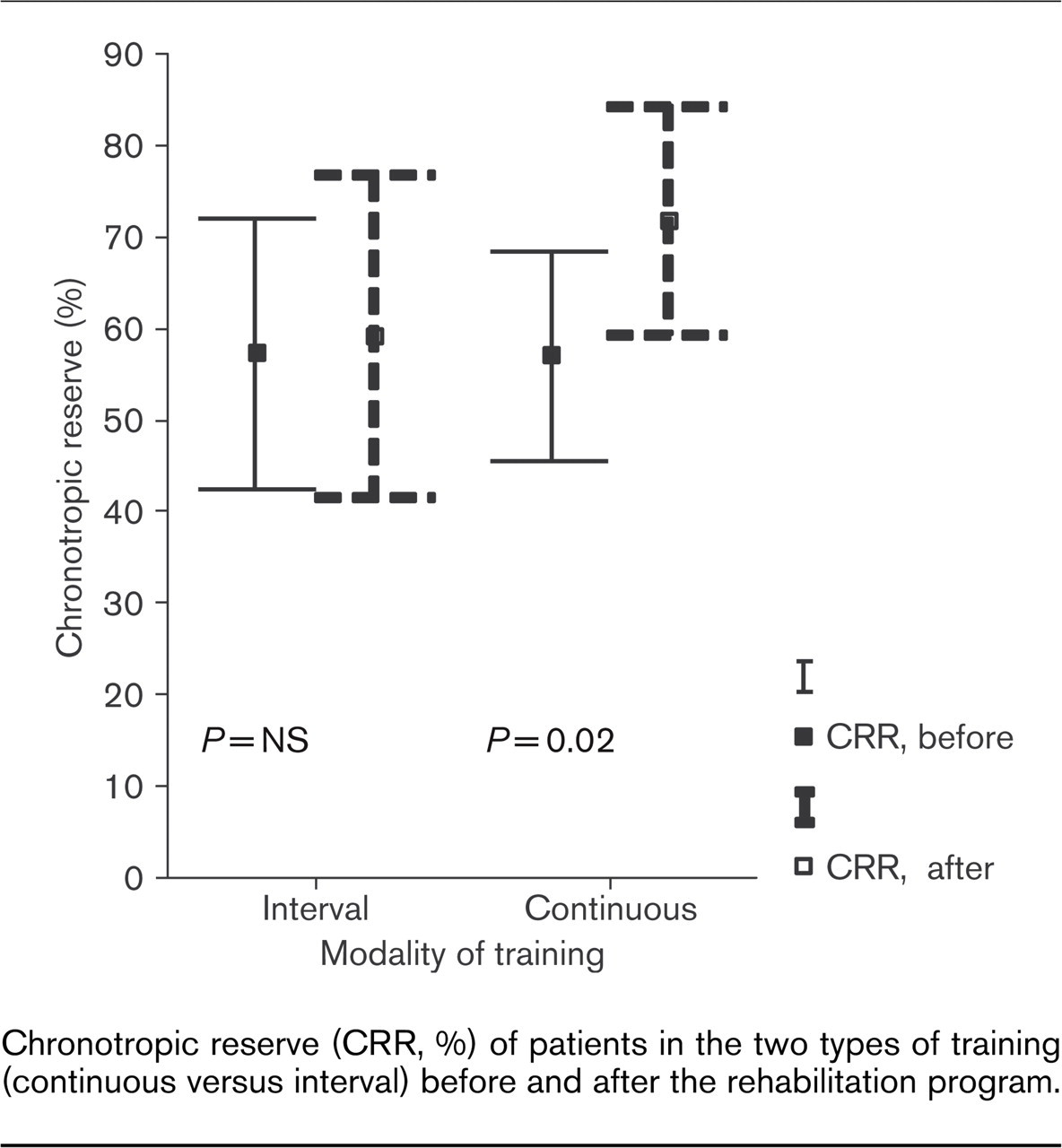
Chronotropic reserve (CRR, %) of patients in the two types of training (continuous versus interval) before and after the rehabilitation program.
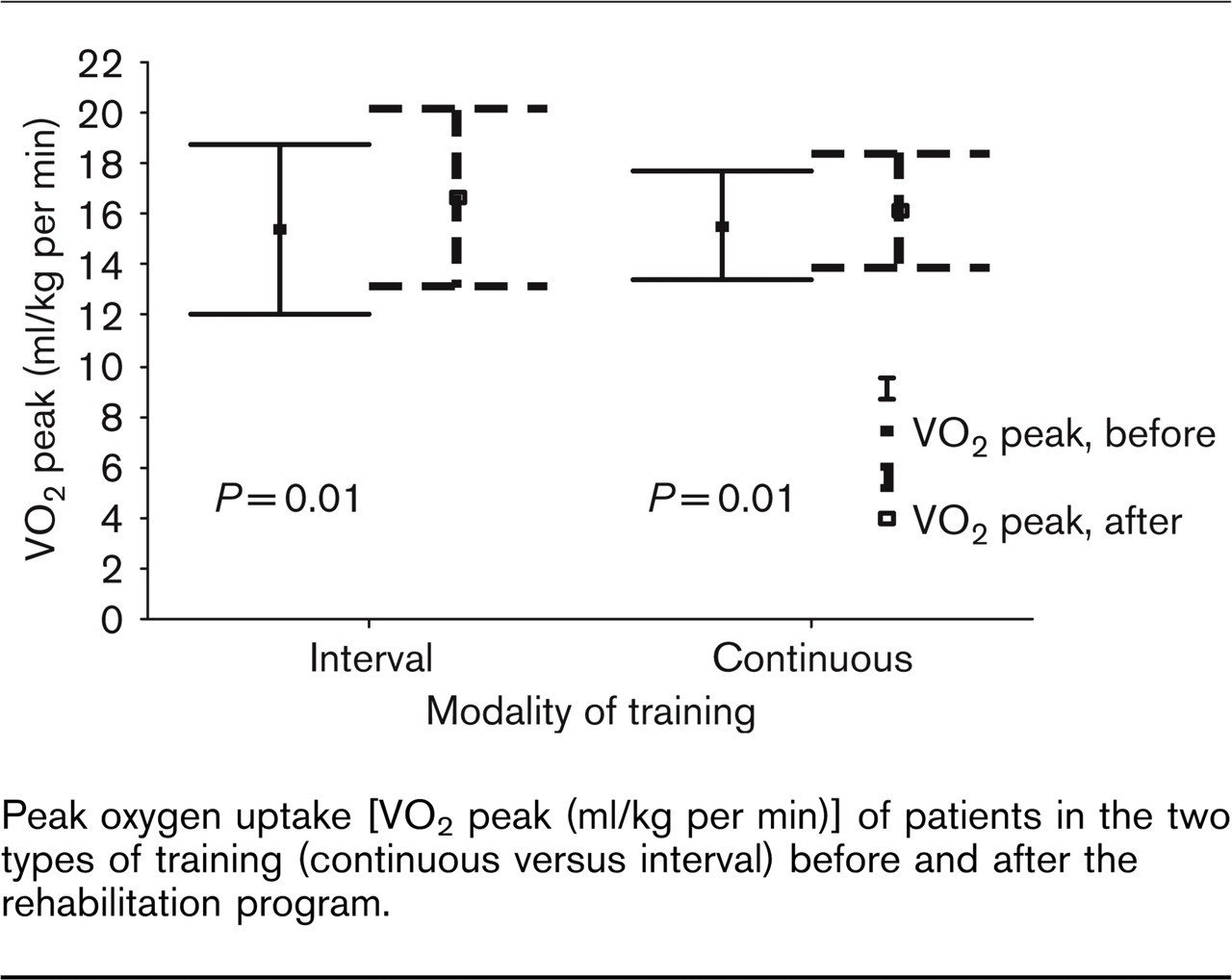
Peak oxygen uptake [VO2 peak (ml/kg per min)] of patients in the two types of training (continuous versus interval) before and after the rehabilitation program.
Comparison of cardiopulmonary exercise parameters before and after the completion of the program for patients assigned to continuous training
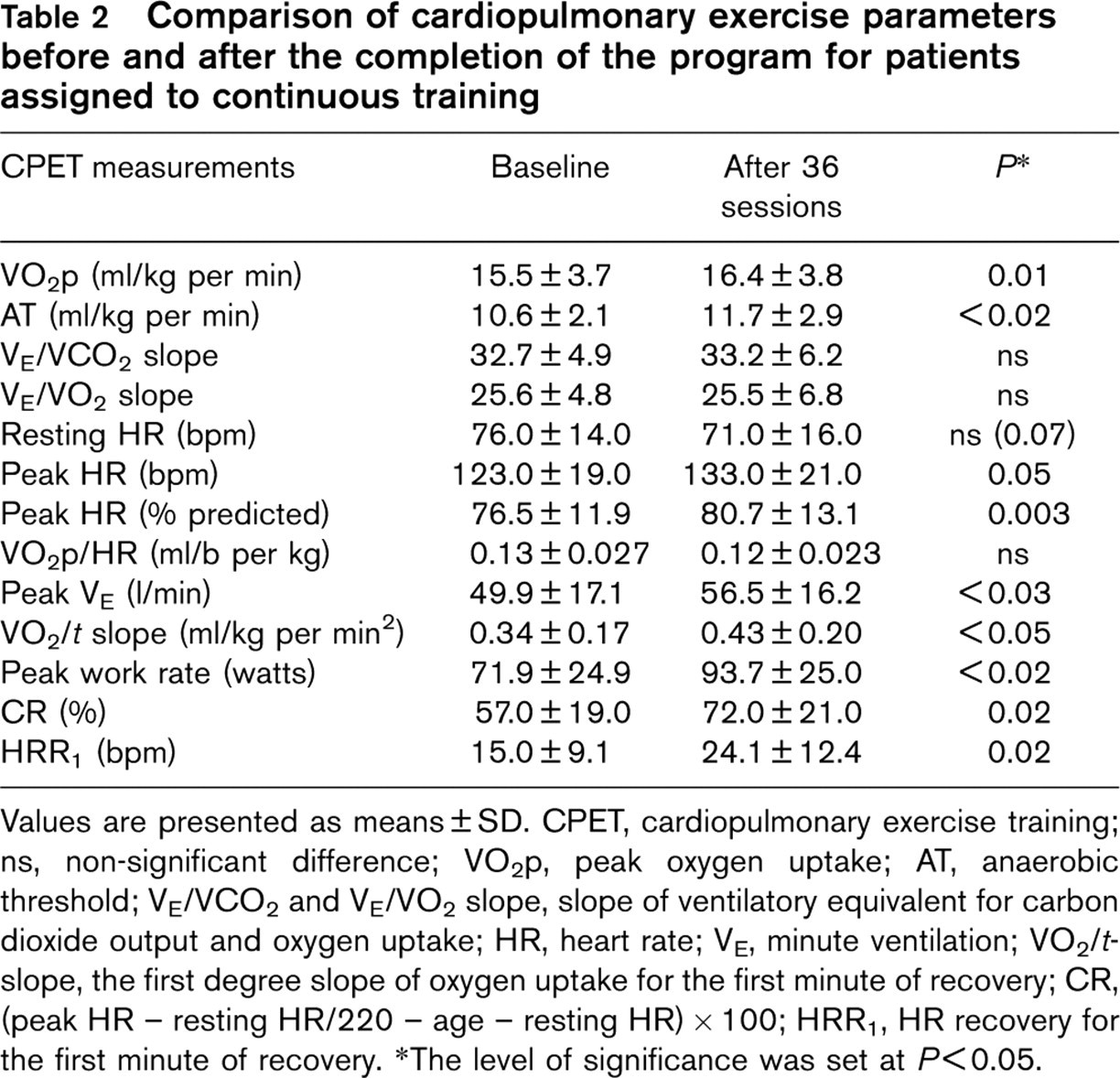
Values are presented as means ± SD. CPET, cardiopulmonary exercise training; ns, non-significant difference; VO2p, peak oxygen uptake; AT, anaerobic threshold; VE/VCO2 and VE/VO2 slope, slope of ventilatory equivalent for carbon dioxide output and oxygen uptake; HR, heart rate; VE, minute ventilation; VO2/t-slope, the first degree slope of oxygen uptake for the first minute of recovery; CR, (peak HR - resting HR/220 - age - resting HR) × 100; HRR1, HR recovery for the first minute of recovery. ∗The level of significance was set at P < 0.05.
Comparison of cardiopulmonary exercise parameters before and after the completion of the program for patients assigned to interval training
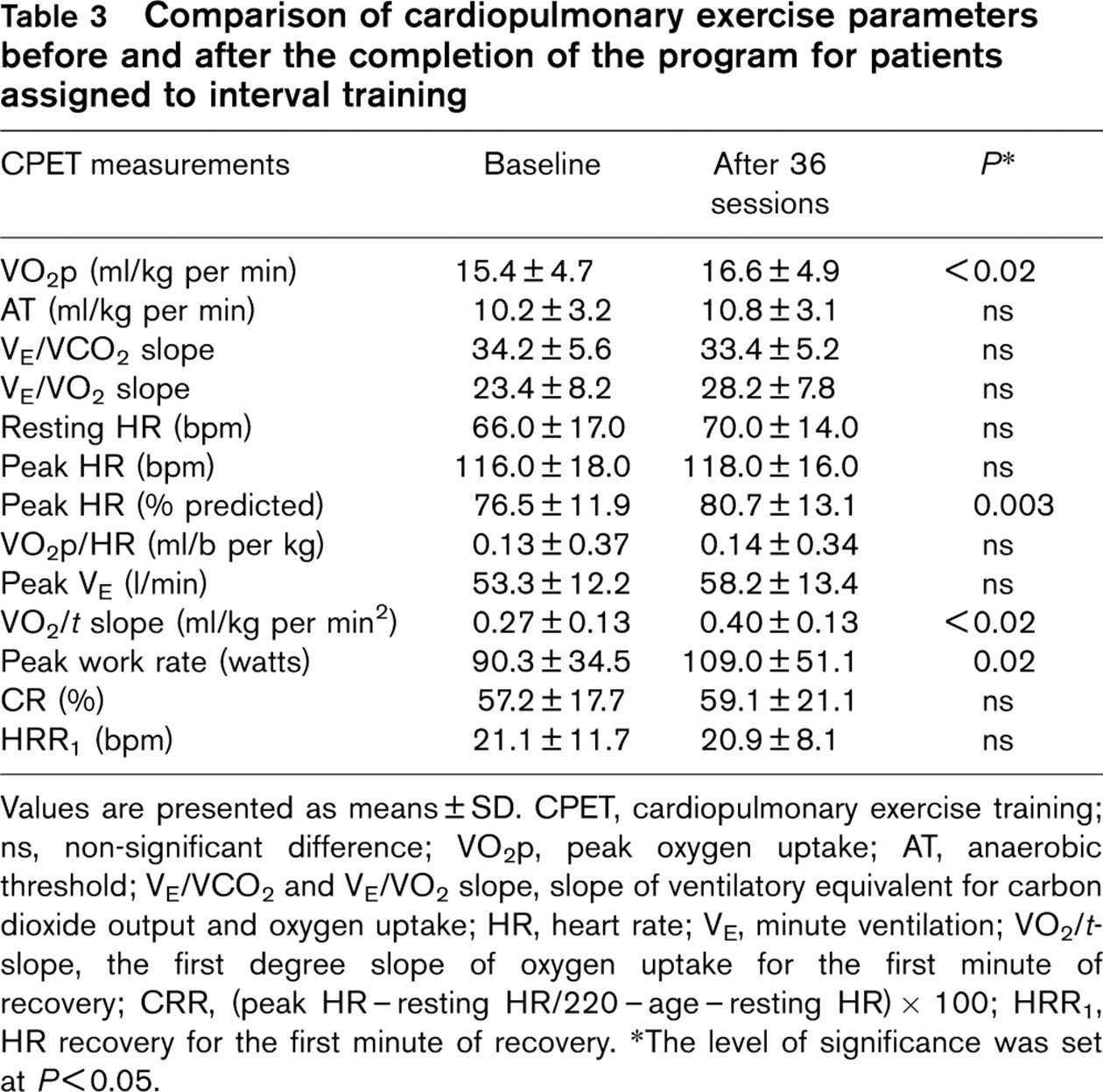
Values are presented as means ± SD. CPET, cardiopulmonary exercise training; ns, non-significant difference; VO2p, peak oxygen uptake; AT, anaerobic threshold; VE/VCO2 and VE/VO2 slope, slope of ventilatory equivalent for carbon dioxide output and oxygen uptake; HR, heart rate; VE, minute ventilation; VO2/t-slope, the first degree slope of oxygen uptake for the first minute of recovery; CRR, (peak HR-resting HR/220-age-resting HR) × 100; HRR1, HR recovery for the first minute of recovery. ∗The level of significance was set at P≤0.05.
Discussion
By this prospective randomized controlled study it was shown that exercise training improves chronotropic response to exercise and early heart rate recovery after exercise in CHF patients. Specifically, continuous rather interval exercise training improves CR and HRR1 in these patients. Both types of training had a significant improvement in exercise capacity. To the authors’ knowledge, this is the first prospective controlled study that evaluates the effects of exercise training (continuous or interval) on early heart rate recovery in patients with chronic heart failure.
Few controlled studies have been conducted to look at the effects of physical training programs on the autonomic regulation of the cardiovascular function in these patients. A recent review of controlled trials with physical training in CHF patients, reported a partial reversal of the autonomic imbalance after training with a reduction of sympathetic over-activation, an enhancement of chronotropic responsiveness to exercise and an increase in high frequency of heart rate variability indices [35]. Another recent study has shown beneficial changes in cardiovascular autonomic nervous control, evaluating the effects of exercise training on autonomic tone by baroreflex sensitivity, heart rate variability and cardiac pre-synaptic innervation by (11)C-hydroxyephedrine PET in 13 CHF patients [36]. A significant reduction after physical training of the central sympathetic neural outflow measured directly using the technique of microneurography was also found in seven patients studied by Roveda et al. [37]. All these findings support the hypothesis that exercise training can restore autonomic imbalance in CHF patients. These positive effects might have an important prognostic significance as recent prognostic studies suggest [15,16].
Our study has demonstrated that the beneficial effects of exercise training in autonomic tone in CHF patients can be evidenced indirectly by CR and HRR1 improvement, two easily measured parameters, from a symptom-limited exercise testing. Considering the two types of exercise training it was concluded that continuous exercise training rather than interval training contributed mostly to this improvement. The training program effects on the autonomic nervous system in CHF patients have been mainly demonstrated by applying continuous endurance exercise programs [15,16,26,35–37]. A previous study by Meyer et al. [38] in CHF patients who participated in interval training programs have shown that short-term interval training can improve exercise capacity, allowing more intense exercise stimuli to the peripheral muscles with minimal cardiac strain. Our data has confirmed this report, but our results also showed a blunted contribution of interval training to autonomic tone restoration. A possible mechanism that may explain this finding could be the insufficient involvement of the autonomic nervous system in terms of stimulus and time in each exercise session during the interval training, compared to the continuous training program. Further specific studies on autonomic nervous system interval training effects in a larger CHF population will clarify better the specific mechanism.
Recent epidemiological data have demonstrated that heart rate recovery, an index of parasympathetic activity, is an independent predictor of cardiovascular events and mortality [39,40]. We have shown that continuous exercise training, but not interval training, improves this parameter in CHF. The prognostic implications of these changes will require a prospective study. Results do suggest that chronotropic response to exercise and heart rate recovery may be significant targets for therapy in patients with CHF. Another significant finding of this study was the improvement of recovery oxygen uptake kinetics after both continuous or interval training in CHF patients. In previous studies, the delayed recovery oxygen uptake kinetics in CHF patients has been related to an impaired oxygen delivery to skeletal muscles [41], a slow replenishment of energy stores in the active muscles [42], a reduced respiratory muscle performance [32] and indirectly to several histological and biochemical muscle alterations [43]. Therefore, an improvement in recovery oxygen uptake kinetics by continuous or interval training may indicate beneficial effects in one or more of the above pathophysiological mechanisms.
Study limitations
The small number of participants and the gender (most of them were males) may limit the results of this study. From all patients initially participating in the rehabilitation program, five patients dropped-out (four from the interval training group and one from the continuous training group). For this reason, the baseline peak work rate in the two groups had different mean values; however this difference did not reach statistical significance. The small number of patients may also limit the comparison between the two training groups. A larger study will confirm our findings.
In conclusion, a 3-month supervised continuous or interval training program improves exercise capacity of CHF patients. However, only continuous rather than interval training contributes most to autonomic nervous system restoration as evidenced by the chronotropic response to exercise and heart rate recovery improvement.
Footnotes
Acknowledgements
We would like to thank Sotirios Gyftopoulos for his significant technical support and Olga Georgiadou for her significant assistance during the whole rehabilitation program.