
Abstract
Background
We assessed the association of systolic blood pressure response to exercise with the risk of an acute myocardial infarction.
Design
We conducted a population-based follow-up study.
Methods
This study was based on 1731 middle-aged men without history of coronary heart disease who underwent a cycle ergometer exercise test. Systolic blood pressure was measured every 2 min during a cycle ergometer exercise test in 1731 men followed for 12.7 years on average. A total of 188 acute myocardial infarctions were observed.
Results
The total change in systolic blood pressure, the slope of the rise in systolic blood pressure per minute and maximal systolic blood pressure during exercise in quintiles were related to the risk of acute myocardial infarction. Maximal systolic blood pressure of over 230 mmHg was associated with a 2.47 [95% confidence interval (CI) 1.46-4.18] fold risk of acute myocardial infarction, after adjustment for age, other risk factors including the use of antihypertensive medications and systolic blood pressure at rest. Among men with elevated systolic blood pressure at rest, the relative risk for an acute myocardial infarction was 4.31 (95% CI 2.04-9.07) times higher for those who had a steep slope of systolic blood pressure rise (>9.4 mmHg per min of exercise) as compared with those who had a more gradual rise in systolic blood pressure. Conclusions Both rate and levels of rise in systolic blood pressure during a progressive exercise test were risk predictors for acute myocardial infarction. These measurements provide an incremental predictive value for an acute myocardial infarction to elevated resting systolic blood pressure, emphasizing the importance of regular blood pressure measurements during exercise testing. Eur J Cardiovasc Prev Rehabil 13:421-428 © 2006 The European Society of Cardiology
Introduction
Systolic blood pressure (SBP) response to increasing workloads is analogous with blood pressure responsiveness to daily physical conditions [1, 2]. An exercise-induced rise in SBP has also been found to be a predictor of future hypertension [3–6], left ventricular hypertrophy (LVH) [7–9], stroke [10], and cardiovascular disease (CVD) mortality [11–13] in apparently healthy people. Some studies have reported, however, that an increased SBP response during exercise is associated with a lower probability of severe coronary artery disease on angiography and a better prognosis in patients with known or suspected coronary heart disease (CHD) [14–16].
The prognostic importance of the extent of the rise in SBP during exercise remains unclear in subjects without underlying CHD. Furthermore, it is not known whether the increased risk associated with elevated SBP during exercise is due to elevation of the pre-exercise level of blood pressure or to an exaggerated rise in blood pressure during exercise or both. In addition, little is known about the implications of SBP rise during an exercise test for future risk of acute coronary events.
We investigated the prognostic significance of the rate and maximal increase of SBP during a standardized cycle ergometer exercise test with regard to the future risk of acute myocardial infarction (AMI) in a population-based sample of men. We also compared SBP responses to exercise testing and resting levels of SBP as predictors of AMI.
Methods
Participants
The analysis were carried out with the participants of the Kuopio Ischaemic Heart Disease Risk Factor Study (KIHD), a longitudinal observational population-based study designed to investigate risk factors for CVD, and related outcomes. The study involves men from eastern Finland, an area known for high prevalence and incidence of atherosclerotic vascular diseases [17]. The study group is a representative sample of men living in the city of Kuopio and its surrounding rural communities, who were 42-61 years of age at baseline. The examinations were performed between March 1984 and December 1989. Of 3235 potentially eligible men, 2682 (83%) volunteered to participate in the study. The KIHD was approved by the Research Ethics Committee of the University of Kuopio, and each participant gave written informed consent.
The study reported here is based on data obtained from 1731 participants without CHD, who had complete data at baseline on resting and exercise test SBP measurements. Men with coronary heart disease (CHD) (n=677) and who did not performed the exercise test due to severe CVD or some other disease (n=25) were excluded. Men without CHD and with missing values on exercise testing variables (n = 249) were excluded from the analysis. CHD was defined as having a history of myocardial infarction [documented by standard criteria including typical symptoms, electrocardiogram (ECG) findings or elevations of cardiac enzymes], angina pectoris on effort or the use of nitroglycerin for chest pain once a week or more frequently.
This study sample was somewhat younger (52.2 versus 54.9 years) and were less likely to have hypertension (29 versus 40%), medically treated for hypertension (13 versus 46%) and smokers (29 versus 38%) as compared with those who were excluded from the present study. Resting systolic blood pressure (133 versus 134mmHg) and total serum cholesterol (5.8 versus 6.0mmol/l) levels were similar in both groups
Exercise test
A maximal symptom-limited exercise test was performed at baseline between 0800 and 1000 h using an electrically braked cycle ergometer (Tunturi EL 400; Turku, Finland and Medical Fitness Equipment 400 L, Mearn, The Netherlands) as described previously [18, 19]. The standardized testing protocol consisted of a progressive increase in the workload of 20 W/min. The tests were supervised by an experienced physician with the assistance of a trained nurse. The ECG was registered continuously during the test. The ECG criteria for ischemia during exercise were horizontal or downsloping ST depression >1.0 mm at 80 ms after J point or any ST depression of more than 1.0 mm at 80 ms after J point. Heart rate (HR) was recorded by ECG at rest and during exercise. Maximal oxygen uptake (VO2max) was defined as the highest value or the plateau of directly measured oxygen consumption using a respiratory gas analyser (Gebr Mijnhardt, The Netherlands and Medical Graphics, St. Paul, Minnesota, USA) [19].
Blood pressure determination
Resting blood pressure was measured by an experienced nurse using a random-zero sphygmomanometer (cuff size 14 × 54 cm; Hawksley, Lancing, UK) after 5 and 10 min of rest in a seated position in a quiet, thermal-neutral room between 0800 and 1000 h a week earlier than the exercise stress test [20]. The mean of these two values was used as resting blood pressure. Pre-exercise blood pressure was measured manually by the cuff stethoscope method when a subject was sitting on the cycle ergometer immediately before the test. Blood pressure was measured every 2 min during the exercise test. The maximal SBP was the highest value achieved during the test. The SBP change was the difference between maximal SBP during exercise and the pre-exercise SBP. All obtained SBP values between the start and the end of exercise were used in defining of the curve for SBP rise. The rate of the rise in SBP during exercise was defined as an average rise of SBP per minute of exercise from the start of the exercise to the highest SBP value. All men achieved a minimum exercise duration of at least 4 min.
Assessment of covariates
The collection of blood specimens and measurement of fasting levels of serum lipids [21] and assessment of smoking, alcohol consumption and physical activity and presence of diabetes mellitus [19–21] are described elsewhere. The number of cigarettes, cigars, and pipefuls of tobacco smoked daily and the duration of regular smoking in years were recorded using a self-administered questionnaire. Years smoked were defined as the sum of the years of smoking. The lifelong exposure to smoking was estimated as the product of years smoked and the number of tobacco products smoked daily at the time of the examination. Alcohol consumption was assessed with a structured quantity-frequency method using the Nordic Alcohol Consumption Inventory on drinking behaviour over the previous 12 months. Physical activity was assessed using the KIHD 12-month Leisure-Time Physical Activity Questionnaire. This detailed quantitative questionnaire deals with the most common physical activities of middle-aged Finnish men and enables the assessment of all components of physical activity. A family history of CHD was defined as premature CHD in parents or in the first-degree relatives before the age of 55 years in men or the age of 65 years in women. Diabetes was defined as fasting blood glucose of over or equal to 6.7 mmol/l or a clinical diagnosis of diabetes with either dietary, oral or insulin treatment. Body mass index (BMI) was computed as weight in kilograms divided by the square of height in meters. LVH was defined according to electrocardiographic voltage criteria (SV1 + (RV5 or RV6) >3.5 mV).
Ascertainment of follow-up events
Acute myocardial infarction
The collection of data on and the diagnostic classification of non-fatal and fatal coronary events by the end of 1992 were carried out as part of the multinational WHO Monitoring of Trends and Determinants in Cardiovascular Diseases (MONICA) project, in which detailed information on all CHD events were collected prospectively [22]. At baseline, regional coronary register teams collected data on coronary events from hospitals and health centers, and classified the events on all KIHD participants living in the province of Kuopio, one of the monitoring areas of the Finnish part of the WHO MONICA project (FINMONICA). In the FINMONICA study, as explained in detail elsewhere [22], the sources of information included interviews, hospital documents, death certificates, autopsy reports and medico-legal records. The diagnostic classification of coronary events was based on cardiac symptoms, ECG findings, cardiac enzyme elevations, autopsy findings and history of CHD. The FINMONICA coronary register data were annually cross-checked with the data obtained from the computerized national hospital discharge and death registers. Data on non-fatal and fatal coronary events from the beginning of 1993 to the end of 2000 were obtained by computer linkage to the national hospital discharge and death certificate registers. Diagnostic information was collected from hospitals and classified using identical diagnostic criteria. If a subject had multiple non-fatal coronary events during the follow-up period, the first event after baseline was defined as the outcome event. A total of 188 acute myocardial infarctions (AMIs) were reported in this cohort during an average follow-up period of 12.7 years (range 0.7-16.8 years).
Statistical analysis
The correlations between SBP measurements were analyzed using Pearson's correlation test. The associations of SBP during the exercise test with the risk of AMI were analyzed using multivariable Cox proportional hazards models (SPSS 11.5 for Windows; SPSS Inc., Chicago, Illinois, USA). To demonstrate the independent predictive value of exercise SBP, it was entered with and without resting SBP into a forced Cox model including age, examination years at baseline (1985 to 1989), the use of antihypertensive medication (β-blockers, diuretics, angiotensin-converting enzyme-inhibitors or calcium-channel blockers), and other covariates (alcohol consumption, cigarette smoking, serum high (HDL) and low (LDL) density lipoprotein cholesterol, the presence of diabetes, BMI, myocardial ischemia demonstrated on the ECG during exercise, LVH, VO2max, maximal HR, and the energy expenditure of reported leisure-time physical activity). Exercise SBPs were categorized according to quintiles. Risk factors were entered as uncategorized covariates into the Cox models, with the exception of diabetes and LVH by ECG. To test an interaction between the SBP rise during exercise and resting SBP, the interaction term was included in an additional multivariable model. The predictive value of SBPs during exercise in continuous variables were tested according to the use of medication for hypertension. Relative hazards, adjusted for risk factors, were estimated as antilogarithms of coefficients for independent variables. Their confidence intervals (CIs) were estimated under the assumption of asymptotic normality of the estimates.
Results
Baseline characteristics
At baseline, the mean age of the subjects was 52.3 (SD 5.3) years. The major baseline characteristics are shown in Table 1. The energy expenditure of leisure time physical activity was 1058 (SD 1209) kcal/week among men (n = 1597) who had any physical activities, alcohol consumption was 84.2 (SD 120.1) g/week among those who drank alcohol (n=1509) and cigarette smoking was 27.2 (SD 192.1) pack-years among smokers (n=518). There were a total of 23 men whose SBP did not increase during the exercise test, and seven of these men were using β-blockers.
An average maximal HR during exercise was 160 beats per minute and mean maximal oxygen uptake was 32.0ml/kg per min (Table 2). The summary of the most important exercise testing data including exercise SBP values are shown in Table 2.
Characteristics of the study population
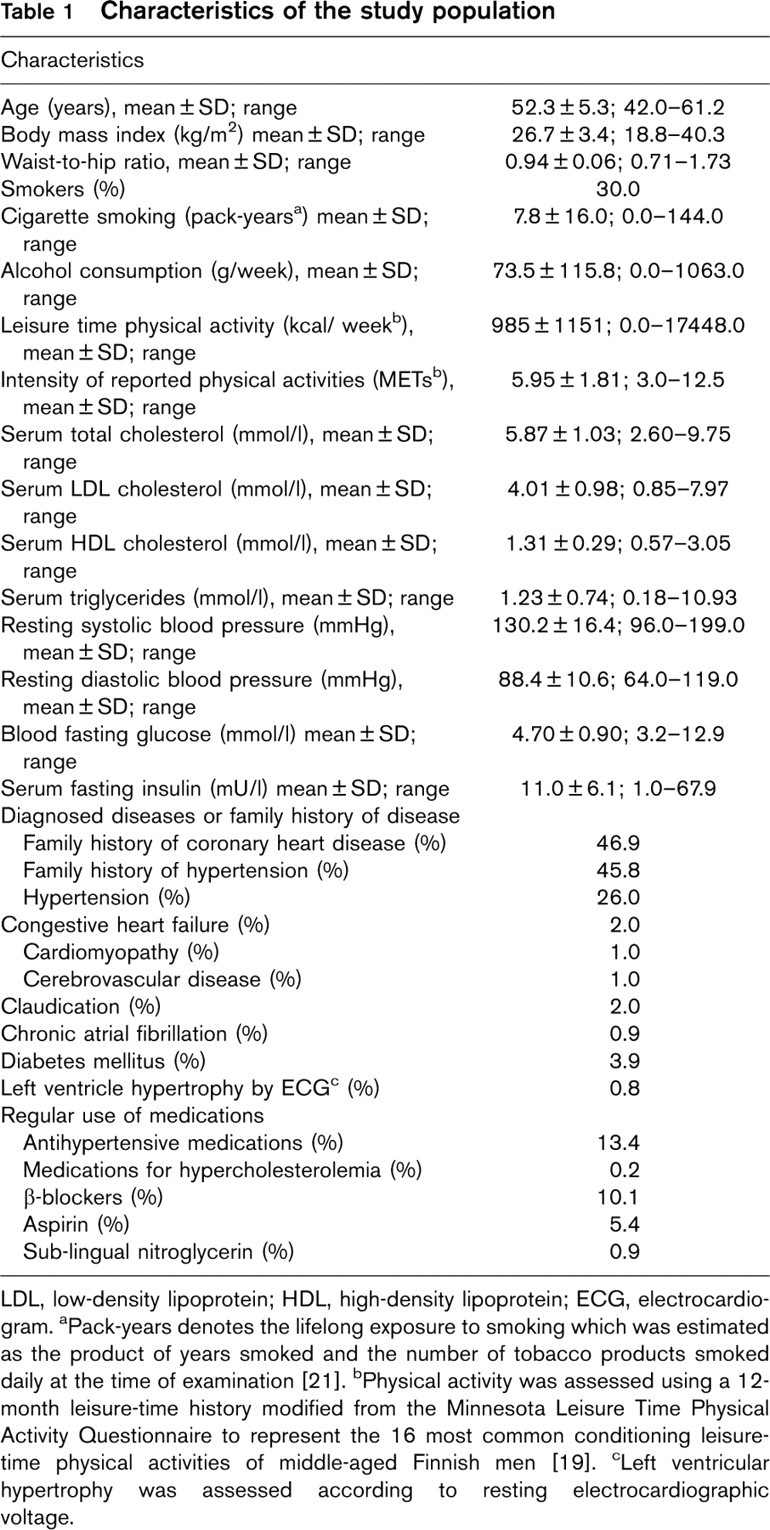
LDL, low-density lipoprotein; HDL, high-density lipoprotein; ECG, electrocardiogram. aPack-years denotes the lifelong exposure to smoking which was estimated as the product of years smoked and the number of tobacco products smoked daily at the time of examination [21]. bPhysical activity was assessed using a 12-month leisure-time history modified from the Minnesota Leisure Time Physical Activity Questionnaire to represent the 16 most common conditioning leisure-time physical activities of middle-aged Finnish men [19]. cLeft ventricular hypertrophy was assessed according to resting electrocardiographic voltage.
Correlations
Resting SBP had a positive correlation with the SBP at 4 min of exercise (r = 0.63, P >0.001) and maximal SBP (r = 0.45, P >0.001) and a weak negative correlation with the change in SBP during exercise (r = − 0.13, P >0.001), but it did not correlate with the rate of rise in SBP during exercise. Pre-exercise SBP correlated with resting SBP (r = 0.70, P >0.001), the SBP at 4min of exercise (0.70, P >0.001), maximal SBP (r = 0.46, P >0.001) and the change in SBP during exercise (r = −0.37, P >0.001). The slope of SBP rise was positively correlated with maximal SBP (r = 0.43, P >0.001) and negatively with pre-exercise SBP (r = −0.20, P >0.001).
The parameters from exercise test
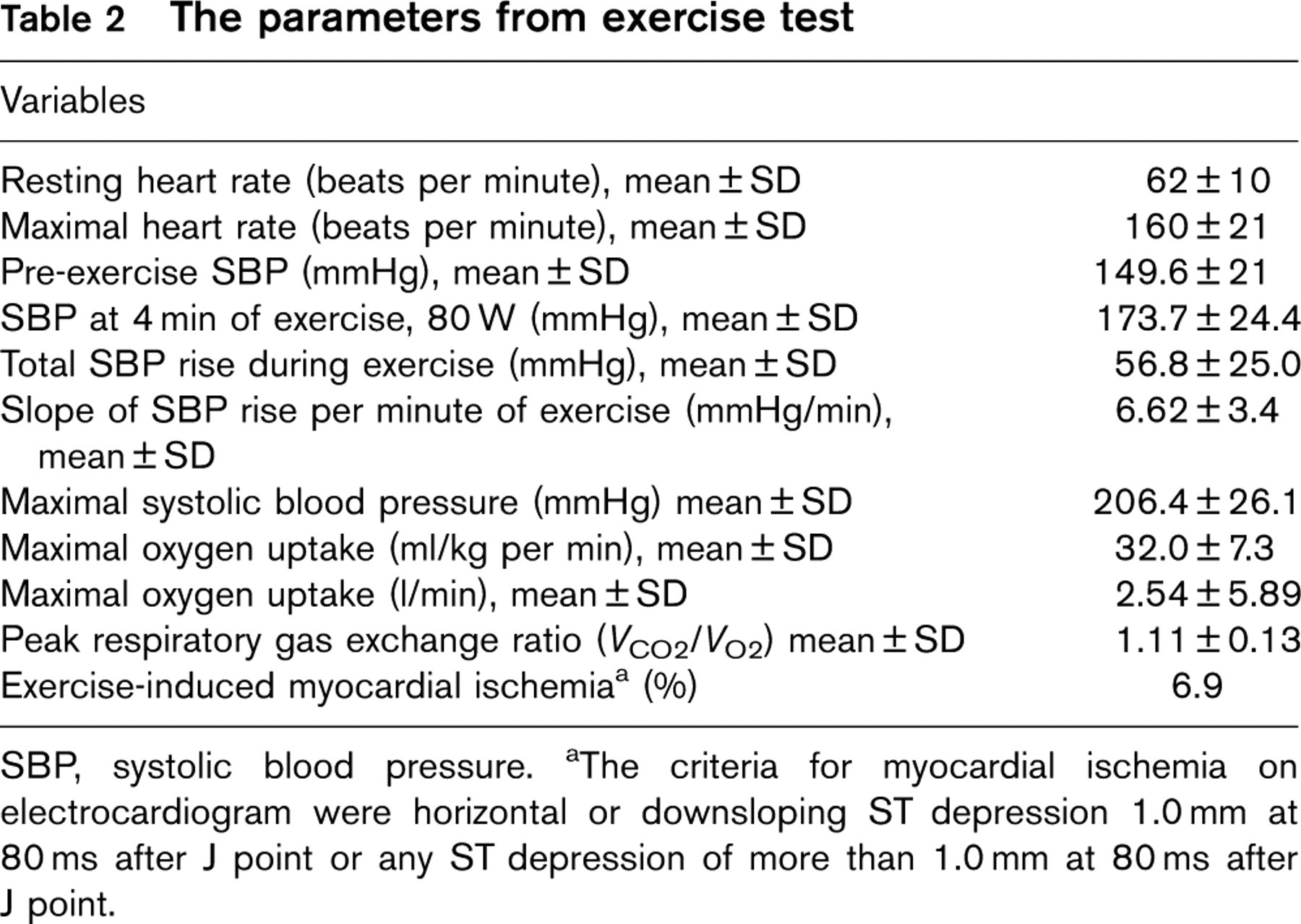
SBP, systolic blood pressure. aThe criteria for myocardial ischemia on electrocardiogram were horizontal or downsloping ST depression 1.0 mm at 80 ms after J point or any ST depression of more than 1.0 mm at 80 ms after J point.
Rise in systolic blood pressure during exercise test and acute myocardial infarction
The total change in SBP and the slope of the rise in SBP per minute in quintiles were related to the risk of AMI (Table 3). An increase in SBP of over 64mmHg was associated with a twofold increase in risk of AMI, as compared to an increase of less than 36mmHg of SBP, with and without adjustment for resting SBP and other risk factors. Secondly, the risk of AMI was 1.7 times higher in men with a slope of rise in SBP during exercise of over 9.4 mmHg/min than in men whose slope of rise in SBP was less than 3.8 mmHg/min, after adjustment for age, examination year, the use of any antihypertensive medication and other risk factors, including resting SBP. Men with the slope of SBP rise between 3.8 and 9.4 mmHg had a trend for slight decrease in risk for AMI as compared to men with the slope of SBP rise below 3.8 mmHg (Table 3). It is noteworthy, that the adjustment for resting SBP did not change substantially the predictive value of SBP rise during exercise.
The risk of AMI was 3.1 times higher in men with a slope of SBP rise over 9.4 mmHg/min and elevated SBP (> 140 mmHg) at rest (n=96) than in men who had normal resting SBP and a less steep slope of SBP rise (Fig. 1). Among the sub-group of men with elevated SBP at rest (n=388), the RR was 4.31 (95% CI 2.04-9.07, P >0.001) times higher for AMI in men with a steep slope of SBP rise than in men who had a gentler slope in the rise of SBP, after adjustment for age, examination year, the use of antihypertensive medication and other risk factors.
The adjusted risk of AMI in men with a maximal SBP during exercise of over 230 mmHg was 2.5 times higher than that of men with a maximal SBP below 185 mmHg (Table 3). The adjusted risk of AMI in men with maximal SBP over 230 mmHg was 1.88 times higher (95% CI 1.28-2.72, P = 0.001) as compared with other subjects (four lowest quintiles).
Relative risks of acute myocardial infarction according to the quintiles of the rise in systolic blood pressure and maximal systolic blood pressure during exercise in 1731 men without coronary heart disease at baseline

SBP, systolic blood pressure; CI, confidence interval. aRelative risks are adjusted for age, examination year and the use of any antihypertensive medication. bRelative risks are adjusted for age, examination year, the use of any antihypertensive medication, alcohol consumption, cigarette smoking, serum low and high density lipoprotein cholesterol, diabetes, body mass index, myocardial ischemia during exercise, left ventricular hypertrophy, maximal oxygen uptake, maximal heart rate, the energy expenditure of physical activity and systolic blood pressure at rest.
Rise in systolic blood pressure during exercise test and the risk of acute myocardial infarction according to the use of antihypertensive medication
Men with antihypertensive medications had higher resting SBP values but lower rise in SBP during exercise. The total SBP increase and maximal SBP achieved during exercise were both related to the risk of AMI, after adjustment for age, examination year, risk factors (alcohol consumption, cigarette smoking, serum HDL and LDL cholesterol, diabetes, BMI, a positive test for myocardial ischemia, LVH, VO2max, maximal HR, the energy expenditure of physical activity and resting SBP) only among the participants who were not using antihypertensive mediations. The risk of AMI was 1.13 (95% CI 1.05-1.25, P = 0.001) per 10 mmHg increase in total SBP change and 1.14 (95% CI 1.06-1.23, P >0.001) per 10mmHg increase in maximal SBP in men without antihypertensive medication, respectively. Elevated pre-exercise SBP was not independently related to the increased risk of AMI. Adjustment for pre-exercise SBP instead of the prior resting SBP value did not change substantially the significance of the results.
Discussion
An excessive rise in SBP, as indicated by total increase or maximal SBP achieved, during progressive exercise was related to an increased risk of AMI in middle-aged men without prior CHD. Our study showed the additive prognostic value of exercise blood pressure after adjusting for the different resting SBP levels.
In previous studies, elevated SBPs at fixed submaximal workloads were associated with increased risk of CVD events [1, 15]. Mundal and coworkers [15] reported that SBP at a moderate workload was independently related to morbidity and mortality from myocardial infarction. Furthermore, Filipowsky and coworkers [12] found that changes in SBP during exercise was related to the risk of CVD after adjustment for resting SBP. Fagard and coworkers [1] observed that SBPs at moderate and peak workloads were directly associated with the risk of cardiovascular events in hypertensive men, although SBP at moderate workload was not predictive when adjustments were made for resting SBP.
Maximal SBP and the SPB rise during progressive exercise indicate blood pressure response to exercise, but the average rise in SBP reflects the continuous span of the SBP rise per minute of exercise. The slope of the rise in SBP with increasing workloads provides information about the hemodynamic response to the increasing physical stress. This provides data when blood pressure response is steep or low with increasing workload. The excess risk was limited to those men with the steepest slope of SBP rise, over 9.4 mmHg/min of exercise, whereas the risk seems to be slightly lower among men with the slope of rise between 3.8 and 9.4 mmHg/min. The risk of an AMI was particularly increased in subjects with elevated SBP at rest and a SBP rise over 9.4mmHg/min of progressive exercise, although the inappropriately attenuated increase in blood pressure with exercise was also not a good sign. This may be due to the greater number of subjects using antihypertensive medications and thus may also have an increased risk of coronary events. On the basis of our findings, however, the SBP rise during progressive exercise provides a non-invasive exercise test measure for identifying subjects at excess risk of AMI. Consistent with results of our previous study [10], maximal SBP rise relative to exercise duration also was predictive for cerebrovascular events.
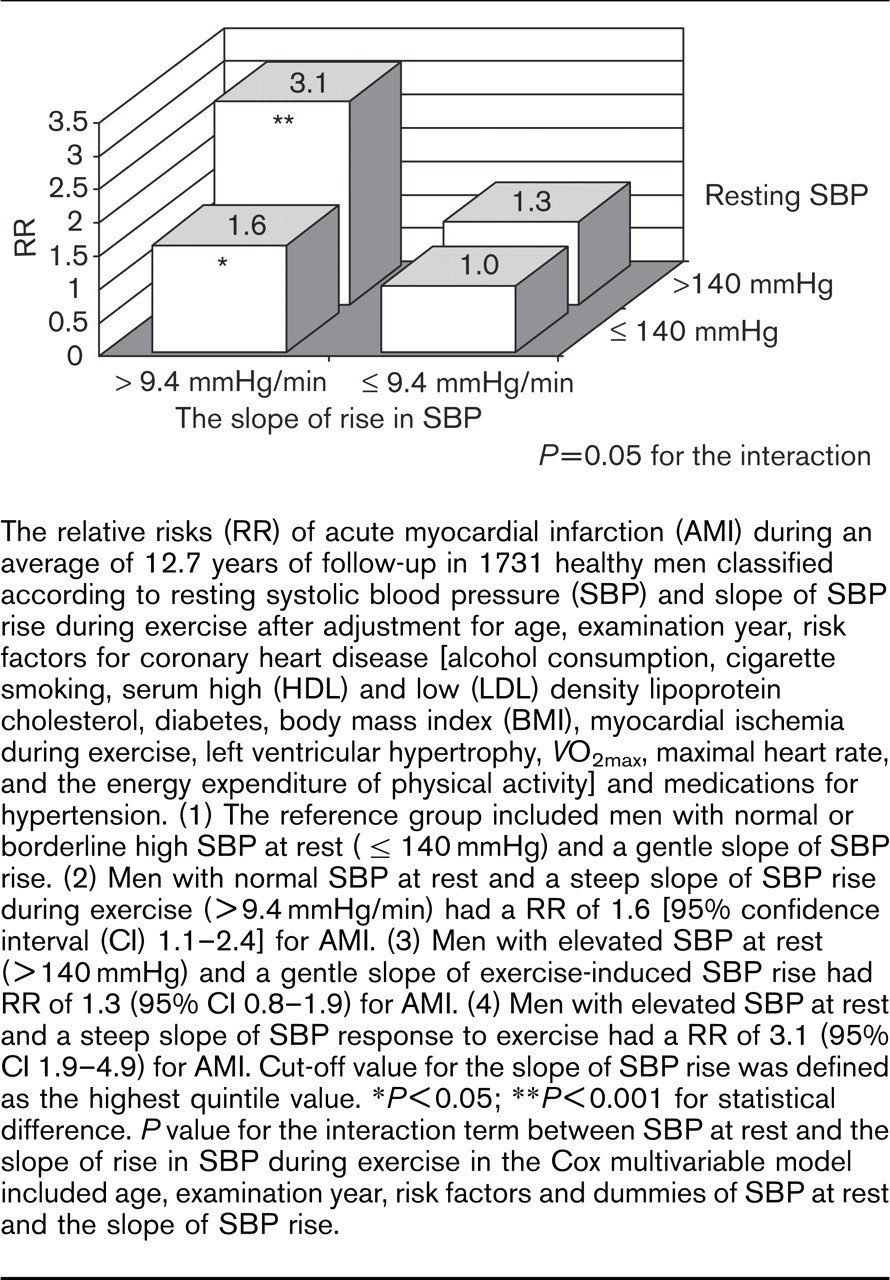
The relative risks (RR) of acute myocardial infarction (AMI) during an average of 12.7 years of follow-up in 1731 healthy men classified according to resting systolic blood pressure (SBP) and slope of SBP rise during exercise after adjustment for age, examination year, risk factors for coronary heart disease [alcohol consumption, cigarette smoking, serum high (HDL) and low (LDL) density lipoprotein cholesterol, diabetes, body mass index (BMI), myocardial ischemia during exercise, left ventricular hypertrophy, VO2max, maximal heart rate, and the energy expenditure of physical activity] and medications for hypertension. (1) The reference group included men with normal or borderline high SBP at rest (>140mmHg) and a gentle slope of SBP rise. (2) Men with normal SBP at rest and a steep slope of SBP rise during exercise (>9.4 mmHg/min) had a RR of 1.6 [95% confidence interval (CI) 1.1-2.4] for AMI. (3) Men with elevated SBP at rest (> 140 mmHg) and a gentle slope of exercise-induced SBP rise had RR of 1.3 (95% CI 0.8-1.9) for AMI. (4) Men with elevated SBP at rest and a steep slope of SBP response to exercise had a RR of 3.1 (95% CI 1.9-4.9) for AMI. Cut-off value for the slope of SBP rise was defined as the highest quintile value. ∗P >0.05; ∗∗P >0.001 for statistical difference. P value for the interaction term between SBP at rest and the slope of rise in SBP during exercise in the Cox multivariable model included age, examination year, risk factors and dummies of SBP at rest and the slope of SBP rise.
It is possible that elevated SBPs at rest and during exercise lead to increased risk of CVD primarily through the same mechanisms. Subjects with exaggerated SBP response to physical stress and their anticipatory response to exercise are likely to develop systemic hypertension [3–6, 20, 23] and LVH [7–9, 24]. Some studies have found a significant association between the SBP response to exercise and LVH, which subsequently lowers coronary vasodilatory reserve and increases the vulnerability of the myocardium to ischemia, cardiac dysfunction, arrhythmias, and the risk of cardiovascular events [7–9]. It is proposed that exaggerated SBP contributes to the development of LVH, although blood pressure reactivity to physical stress is reported not to add substantially to the prediction of left ventricular mass as compared with resting SBP [25–27]. The steep rise in exercise blood pressure also may be due to poor arterial compliance in individuals with underlying subclinical arteriosclerotic changes [15]. Further, elevated SBP during physical stress may lead to arterial wall thickening and vascular smooth muscle hypertrophy, in which case an impaired reduction of vascular resistance during exercise could contribute to increased risk of cardiovascular events [13]. An impaired reduction of systemic vascular resistance and associated higher arterial blood pressure during acute exertion [13] may lower the threshold for myocardial ischemia and could trigger rupture of a vulnerable atherosclerotic plaque.
Differences in health status, age, physical fitness and sex may cause inter-individual variation in SBP responses [26, 28]. It is known that apparently healthy individuals with good cardiorespiratory fitness may achieve a higher total SBP rise due to an increased stroke volume [2, 13, 14, 28]. High SBP during exercise and an excessive rate-pressure product increase myocardial oxygen demand, however, which can result in global sub-endocardial ischemia, wall motion abnormalities, and dysfunction in left ventricular filling among subjects with underlying atherosclerotic CVD [16, 18, 29].
There is growing evidence that aerobic exercise training via an increase in endothelial nitric oxide synthase activity can increase the capacity of endothelial cells to evoke vasodilation and decrease exercise blood pressure [30], although there seems to be heterogenity in the SBP responsiveness to exercise [31]. Furthermore, exercise training and increased aerobic capacity can further improve vascular arterial stiffness, and vasodilatory capabilities, leading to decreased systemic vascular resistance [30, 32]. A greater rise of SBP from start to peak exercise with a long exercise test duration, due to good aerobic power, reflects a good cardiac output and decreased vascular resistance. SBP at a fixed sub-maximal workload represents different levels within spans of the SBP rise between fit and unfit, but the slope of the SBP rise may reduce these differences in exercise capacity [10]. Finally, after adjusting for maximal oxygen consumption, the gold standard for assessing cardiorespiratory fitness, the slope of SBP rise during exercise remained an independent predictor of AMI in the present study.
We used a standardized cycle exercise test protocol with increasing workloads [2, 11–13], which has certain advantages over the treadmill exercise test. With the cycle ergometer it is easier to obtain reliable measurements of blood pressure as compared to treadmill exercise. On the other hand, maximum HR has been shown to be lower, but the rate pressure product to be similar due to a higher blood pressure in the cycle ergometer test [33].
The fatigue of the quadriceps muscles in patients who are not experienced in cycling is a limitation, because inexperienced subjects may stop before reaching their maximal exercise capacity. As in our study [34], the cycle ergometer consists of progressive incremental workloads, which may have an effect on achieved SBPs during the test. Protocols lasting about 10 min are recommendable to avoid greater variability on repeat testing using large incremental increase in workloads [35]. The present results on rise in SBP during exercise should, however, be compared with caution to studies using different exercise testing protocols such as those with using very mild or small increase of workload during exercise [10].
The current study shows that SBP responses during an exercise test provide additional risk markers for identifying asymptomatic individuals at an increased risk for AMI. SBP rise in response to progressive exercise is a predictor of AMI, especially in men with elevated SBP at rest. While moderate rise in SBP is a normal physiological response to exercise, an excessive SBP rise is an abnormal response to exercise with respect to risk of future coronary events. SBP can be recorded at regular intervals during the exercise test to identify subjects with abnormal SBP response to exercise.
Footnotes
Acknowledgements
The authors thank Hannu Litmanen, Riitta Salonen and Esko Taskinen for their participation in supervising the exercise tests, Kristiina Nyyssönen and Kari Seppänen for supervising the laboratory measurements, Kimmo Ronkainen for data management, and Arthur S. Leon and Tomi-Pekka Tuomainen for their critical comments.