
Abstract
Background
The purpose of the present study was to assess the training and detraining effects on physiological parameters resulting from a combined strength and aerobic exercise programme in patients with coronary artery disease.
Design and methods
Thirty male coronary artery disease patients were randomly assigned to an exercise (n = 16) and control group (n = 14). Patients in the exercise group participated in a supervised exercise programme for 8 months and were followed for 3 months after training cessation. The programme consisted of two sessions of circuit weight training and two sessions of aerobic training. Cardiopulmonary testing and muscular strength were assessed at baseline and after 4 and 8 months of training as well as after 3 months of detraining.
Results
The exercise training programme resulted in significant improvement in cardiorespiratory fitness (V O2peak 15.4% and exercise time 14%) after 8 months. Muscular strength also increased significantly in all exercises by an average of 28% (upper body 25.5% and lower body 35.4%). Three months of detraining, however, resulted in a 10% regression in V O2peak , 6.7% in exercise time, 12% in upper body strength and 15.7% in lower body strength.
Conclusions
The above results indicate that a significant part of the favourable adaptations obtained after prolonged training is practically lost within 3 months of detraining. Therefore, patients with coronary artery disease should follow a systematic exercise programme throughout life in order to improve cardiovascular function, muscular strength and ameliorate their health status. Eur J Cardiovasc Prev Rehabil 13:375–380 © 2006 The European Society of Cardiology
Introduction
During recent decades, the positive effects of aerobic exercise in patients with coronary artery disease (CAD) have been well documented [1–4]. Aerobic training, however, may not be sufficient for improving muscular strength, which is required for various daily activities. According to recent scientific evidence, a complete rehabilitation programme for patients with CAD should combine both strength and aerobic exercise [5]. Therefore, the American Heart Association recommends strength training as part of an exercise programme at least two times a week [5].
Despite the relatively short training period (8–12 weeks) used by most studies and the lack of a control group by some [6, 7] a combined strength and aerobic exercise programme resulted in positive physiological adaptations for CAD patients [8–12]. In fact, the combination of both strength and aerobic exercise proved to be more efficient than aerobic training alone as it resulted in greater improvement of exercise tolerance, muscular strength and quality of life [9, 11].
Since interruptions in training are likely to occur in most patients, it is important to quantify changes in physiological parameters resulting from the cessation of exercise. We recently reported a significant reversal of the training-induced adaptations on lipid levels after a short period of training cessation in cardiac patients [13]. To the best of our knowledge, there are no data concerning the loss of physiological adaptations which occurs after exercise cessation in CAD patients, who have previously trained for a long period of time. In the present study we assess the long-term training effects (8 months) as well as the detraining effects after 3 months of an exercise programme that combines strength and aerobic training in patients with CAD. We evaluated changes in cardiopulmonary function, exercise tolerance, haemodynamic responses and muscular strength.
Methods
Subjects
Thirty male patients with documented CAD participated in the study at least 9 months after their cardiac event. They had myocardial infarction (MI), or had undergone percutaneous transluminal coronary angioplasty (PTCA) or coronary artery bypass grafting (CABG). Those patients who had unstable angina, high blood pressure at rest (systolic >160 mmHg, diastolic >100 mmHg), left ventricular ejection fraction less than 50%, abnormal responses during exercise stress testing (ST depression >1mm, blood pressure failing more than 20 mmHg between two sequential measurements) and any condition precluding regular exercise were excluded from the study.
Each participant signed a written informed consent approved by the institutional ethics committee. The patients were then randomly assigned to an exercise (n=16) or control (n=14) group. Twenty-seven of the initial 30 patients completed all testing and training requirements of the study and were included in the final analysis.
At baseline the two groups were comparable in age (exercise versus control, 56.2 ± 8.6 versus 56.9 ± 12.3 years), body mass (82.5 ± 10.2 versus 79.8 ± 11.7 kg), V O2peak (25.2 ± 5.7 versus 24.9 ± 6.5 ml/kg per min), time after the cardiac event (19.3 ± 10.2 versus 18.4 ± 7.6 months), history of CAD (four versus three patients with MI, four versus three with PTCA, and six versus seven with CABG), and medication (six versus four were taking nitrates, seven versus five β-blockers, six versus six angiotensin-converting enzyme inhibitors, six versus two calcium-blockers, and two versus one diuretics). Patients were in their usual medication, which was not changed throughout the study. All assessments were made while the patients were on their respective medication. No patient was involved in any form of systematic exercise programme prior to the study.
Study design
The exercise group participated in a systematic training programme of 8 months. The programme consisted of four sessions per week; two sessions involved aerobic exercise and two consisted of circuit weight training. Both aerobic and strength exercise lasted 60 min and included a warm-up period (10 min), the main programme (40 min) and a cool-down period (10 min). Aerobic exercise consisted of walking/running on the treadmill and cycling on the cycle ergometer. The exercise intensity of the aerobic programme was 60–75% of the maximal heart rate achieved during a symptom-limited grade exercise test for the first 4 months and increased to 70–85% for the remaining 4 months. Strength training consisted of eight exercise stations performed in the following order: bench press, seated row, leg extension, pull down, ‘pec-deck', hamstrings curl, curl-ups and back extension. Patients performed three sets (cycles), 12 to 15 repetitions per exercise. Initial resistance for each station was set at 60% of the maximum weight that the individual could lift in one repetition. After 4 months of training, the one repetition maximum was reassessed for each participant and resistance was adjusted accordingly. The rest period between exercises was under 30 s with periods of 5 min rest between each cycle. Two exercise specialists supervised each training session. Heart rate was monitored throughout training with heart-rate monitors (Polar-Electro, Finland). Blood pressure was measured by a sphygmomanometer at the beginning, randomly or at subjective discomfort during exercise, and at the end of each training session.
Peak aerobic capacity (V O2peak ) and muscular strength were assessed prior to exercise training, after 4 and 8 months of training, as well as 3 months after the cessation of training in order to examine the negative effects of deconditioning. During the interruption of the exercise programme instructions were given to the patients to refrain from any systematic exercise and follow only their usual walking activities. The total hours spent on walking during detraining were assessed using a questionnaire. The control group underwent the same assessments twice, at the beginning and after 8 months, and they did not participate in any kind of exercise programme throughout the study.
Measurement of peak oxygen uptake and lactate
Peak oxygen uptake was assessed on the treadmill using the Bruce protocol. All patients underwent a symptom-limited exercise test with electrocardiogram (ECG) monitoring and expired gas analysis. Blood pressure was measured by auscultation using a mercury sphygmomanometer at rest and then at 3-min intervals during stress test. A 12-lead electrocardiograph with an automatic ST-segment analysis measured heart rate continuously. The product of heart rate and systolic blood pressure determined the rate-pressure product. Expired minute ventilation, oxygen consumption and carbon dioxide production were continuously monitored throughout exercise by an Oxycon Champion analyser (IEC 601–1; Erich Jaeger, Bunnick, The Netherlands). The analyser was calibrated using both a standard air volume pump and reference gases before each test. At the sixth minute of the stress test and at exhaustion 20 μl blood samples were collected for the determination of blood lactate concentration. The samples were analysed immediately after collection using an enzymatic method (Dr. Lange, M8, Berlin).
Measurement of muscle strength
Muscle strength was measured with the one-repetition maximum method. For most patients, the one-repetition maximum was determined after four to five trials and strength was recorded as the maximal weight lifted in one full range of motion. One minute rest followed after each trial and the resistance was increased by approximately 5 kg, or 2.5 kg when the patient was near to maximum.
Statistical analysis
Descriptive statistics (mean and SD) were used for the presentation of the data. Group differences were assessed by a two-way analysis of variance (ANOVA) for repeated measures when the control group was included in the analysis (baseline versus 8 months). Training and detraining data were treated with one-way ANOVA for repeated measures. When significant differences were revealed, the Tukey post-hoc test was applied. Statistical significance was assumed for P >0.05.
Results
Twenty-seven patients (14 exercise, 13 control) completed the study. Two patients in the exercise group stopped training (4 and 6 weeks after the initiation of the programme) for medical but not cardiac reasons and one patient in the control group refused to complete the follow-up testing. In addition, one patient in the exercise group failed to be retested after training cessation. The patients in the exercise group completed 112.3 ± 15.8 of the 135 training sessions over 8 months (83% attendance rate). No orthopedic injuries or cardiovascular complications occurred during the exercise sessions.
Detraining data were obtained 3 months after the cessation of training only for the exercise group. The analysis of the activity status during this period revealed that the patients followed a mild walking regimen (3–5 km/h, 2–3 times per week) and the total time spent on walking was 34.14 ± 8.05 h.
Cardiorespiratory adaptations and lactate concentration
Exercise time, V O2peak , minute ventilation and respiratory quotient increased significantly after 4 months of exercise training. Significant improvements in these parameters were also evident at the end of the study (Table 1). Submaximal lactate levels decreased significantly from 2.9 ± 1.0 to 2.3 ± 0.8 mmol/l (P >0.05) after 8 months of training, whereas the increase in maximal lactate concentration was not significant (7.0 ± 2.7 versus 8.7 ± 2.4 mmol/l, P >0.05).
A 3-month cessation of training reversed the improvement in cardiovascular endurance (exercise time 47% and V O2peak 65% of the total gain) indicating that patients kept some of their beneficial adaptation observed after 8 months of systematic training (Fig. 1). The sub-maximal and maximal lactate levels were not significantly altered after detraining (Table 1). A negative correlation (r = − 0.63, P >0.05) was obtained between V O2peak changes and hours spent on walking during the detraining period in the exercise group (Fig. 2).
Haemodynamic alterations
The rate pressure product decreased significantly (P >0.05) after training during sub-maximal exercise, whereas detraining reversed the positive adaptations significantly (P >0.05) at the third and ninth minute during stress testing (Fig. 3).
Muscular function
Muscular strength increased significantly in all exercises by an average of 14% (range 12–16%) after 4 months and by 29% (range 22–36%) after 8 months of training. This improvement was observed in both the upper and lower body. A marked reduction (about 14%, range 10–16%) of muscular strength was observed after 3 months of training cessation (Table 2).
Changes in exercise time, cardiorespiratory parameters and lactate observed in the exercise group during training and detraining
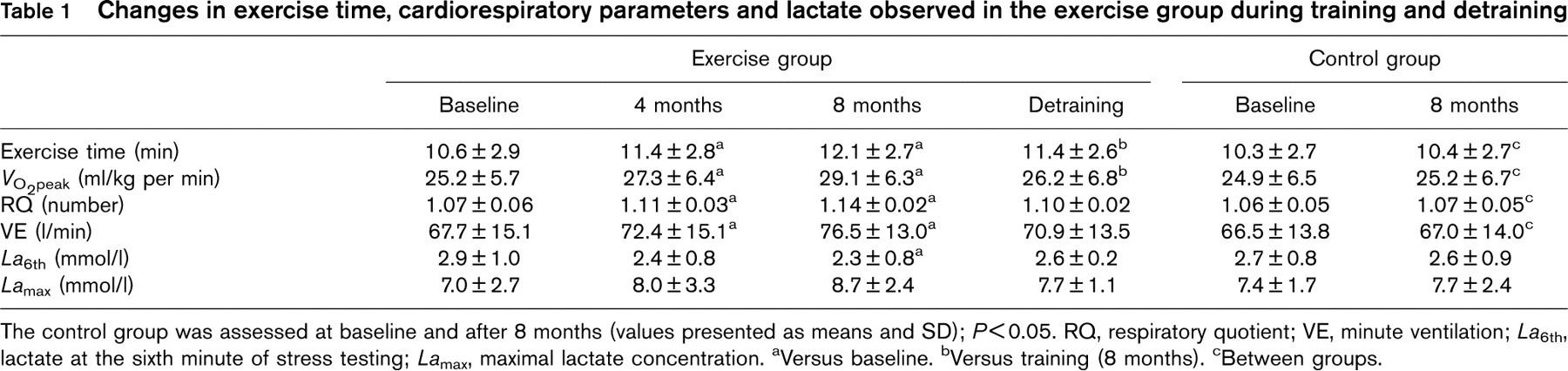
The control group was assessed at baseline and after 8 months (values presented as means and SD); P>0.05. RQ, respiratory quotient; VE, minute ventilation; La 6th, lactate at the sixth minute of stress testing; La max, maximal lactate concentration. aVersus baseline. bVersus training (8 months). cBetween groups.
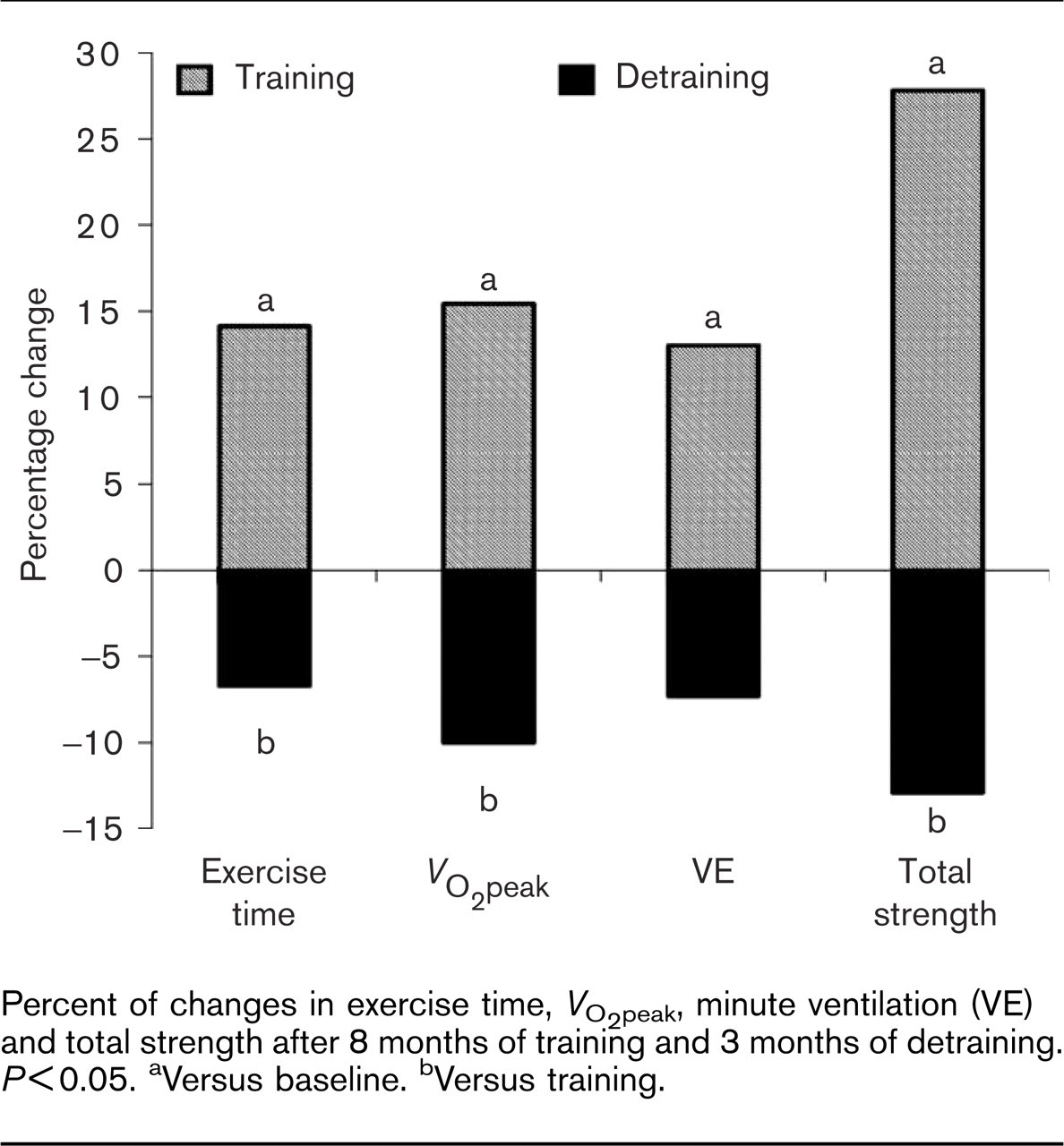
Percent of changes in exercise time, V O2peak , minute ventilation (VE) and total strength after 8 months of training and 3 months of detraining. P>0.05. aVersus baseline. bVersus training.
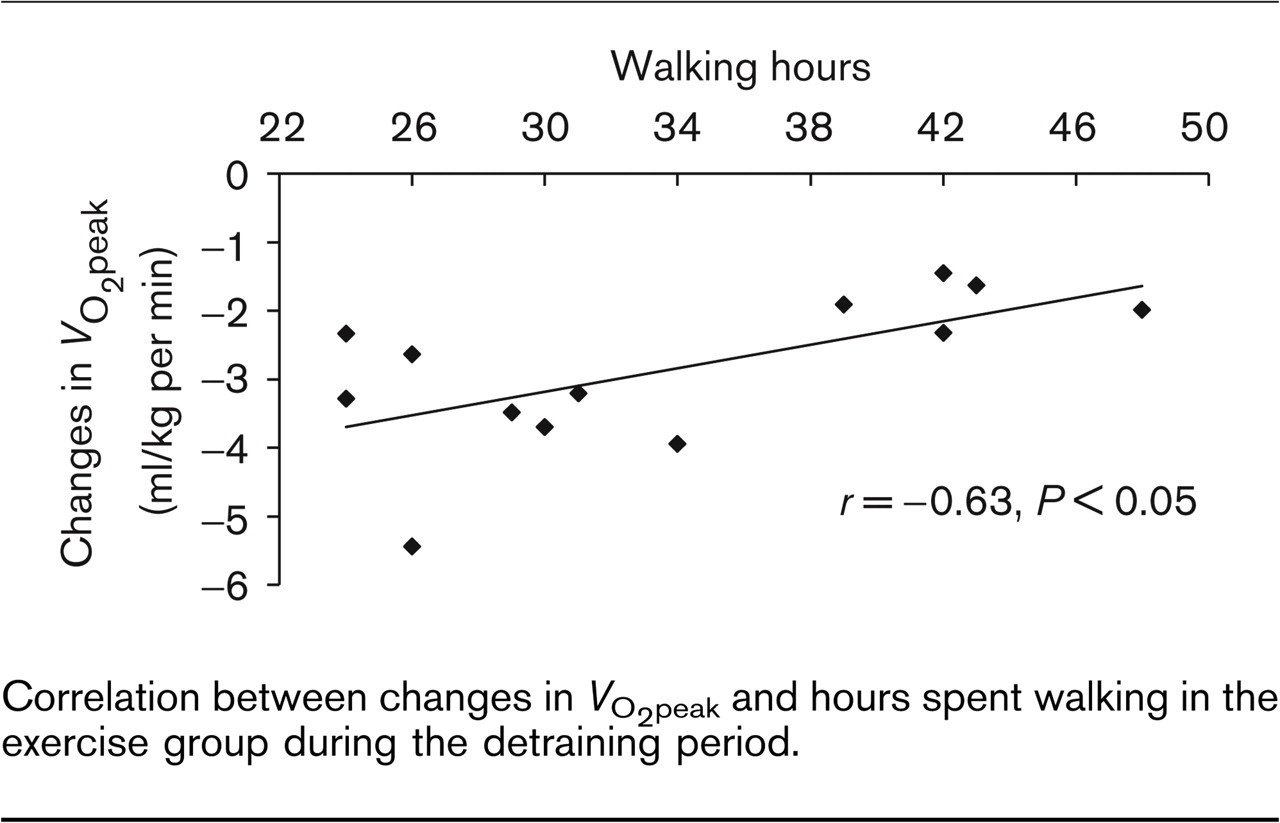
Correlation between changes in V O2peak and hours spent walking in the exercise group during the detraining period.
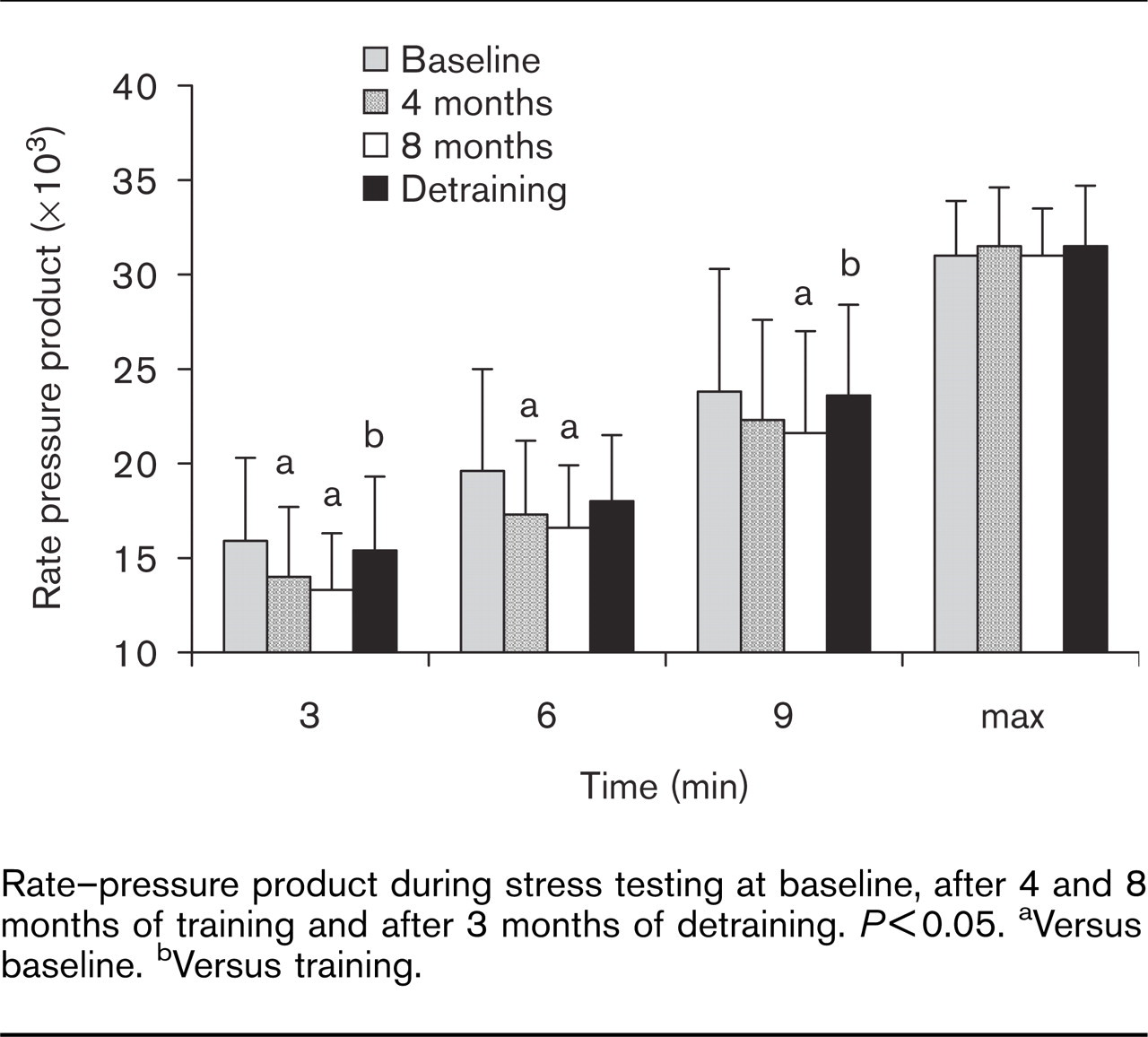
Rate-pressure product during stress testing at baseline, after 4 and 8 months of training and after 3 months of detraining. P>0.05. aVersus baseline. bVersus training.
Discussion
Our findings support the concept that patients with documented CAD can benefit greatly by a combined strength and aerobic exercise programme designed to improve cardiovascular and muscular fitness. Improvements assessed in the cardiovascular and muscular parameters are evident within 4 months of training with additional improvements observed after 8 months. The most important observation of our study was that a great part of these favourable adaptations concerning haemodynamic alterations, exercise tolerance, V O2peak and muscular strength was lost within 3 months of exercise cessation.
Effects of training
The positive haemodynamic changes observed in our study during sub-maximal exercise (Fig. 3) are in accordance with the findings reported by others following aerobic training [2, 14]. Interestingly, lower sub-maximal exercise heart rate and rate pressure product have been recently reported in CAD patients after a 6-month strength and aerobic exercise programme, but not after aerobic exercise alone [12]. In the present study, the lower rate-pressure product observed following a combined strength and aerobic training programme leads to reduced circulatory and muscular oxygen demands and allows CAD patients to tolerate higher workloads. The clinical significance of this change can be observed during the daily activities of these patients.
It is assumed that the significant improvement in V O2peak after a training programme, which includes resistance exercise in patients with CAD, is mainly due to the low initial fitness levels of the patients as well as to the improvements of muscular endurance of the lower extremities. Haennel et al. [15] who compared the improvement in V O2peak following 8 weeks of aerobic and strength training reported an increase of 11% after strength training and 20% after aerobic exercise. The combination of both strength and aerobic training in our study for a period of 8 months induced positive haemodynamic and cardiorespiratory adaptations that were comparable to other studies, in which both strength and aerobic exercise were used [12, 16]. In addition, the lower lactate concentration at sub-maximal intensity observed after 8 months of training, indicated a peripheral metabolic adaptation and shift from anaerobic to aerobic metabolism.
Alterations in maximal strength in the exercise group obtained after training and detraining
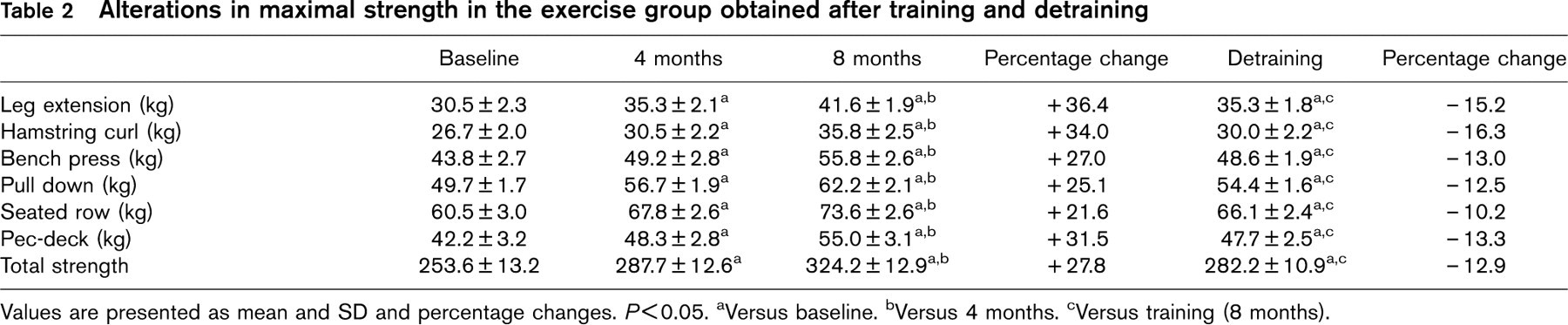
Values are presented as mean and SD and percentage changes. P >0.05. aVersus baseline. bVersus 4 months. cVersus training (8 months).
Effects of detraining
Our findings clearly indicated that exercise should be systematic and continuous. Interruption of training for 3 months resulted in a significant loss of the most positive physiological adaptations realized during the training period. Other investigators have also reported a similar reverse of beneficial changes in heart rate and blood pressure following the cessation of exercise in healthy [17, 18] and hypertensive patients [19, 20]. In another study, ischaemic ECG changes occurred more frequently during the stress test in elderly people 3 months after the cessation of exercise [21], whereas Meyer et al. [22] reported a significant reduction (25%) in the distance covered during a 6-min walking test 3 weeks after deconditioning in patients with cardiac failure.
To our knowledge the present study is the first to document reverse training benefits in CAD patients. Indeed, exercise time reduced by 6.7% and V O2peak by 10% after 3 months of training cessation. The significant training-induced adaptations in cardiorespiratory fitness (V O2peak 15.4% and exercise time 14%) represent a loss of the initial gains of about 47 and 65%, respectively. It is important to note, however, that after 3 months of detraining, patients kept some of their beneficial adaptations observed after 8 months of systematic exercise and arrived at values that were above the baseline measures.
This is probably due to the mild walking regime during the deconditioning phase. We observed that patients who spent more hours walking during detraining had less regression of V O2peak (Fig. 2). This fact points out the need for uninterrupted exercise throughout life for these patients in order to preserve a sufficient level of cardiovascular endurance which is necessary to perform daily activities.
Muscular strength after training and detraining
In recent years, resistive training has been established as a safe and effective mode of training for CAD as well as for heart failure patients [5, 23]. In our study, increases in strength for all exercises ranged between 22 and 36% after 8 months of training (Table 2). Similar results were obtained after 1 year of a combined aerobic and weight-training exercise programme in CAD patients [16]. Greater improvements in strength have also been reported with higher intensity circuit weight training [6].
The cessation of exercise resulted in losses of muscular strength gained during training. These losses were between 10.2 and 16.3% for the different muscle groups (Table 2). Somewhat greater losses in muscular strength (30%) were reported by Taafe et al. [24] in 11 elderly individuals after 12 weeks of training interruption, whereas a 13–32% reduction in strength was observed in young women after 6 months of detraining [25]. The detraining effects of the present study are important because data of muscular strength for cardiac patients after the cessation of exercise do not exist [26] and underline the need for regular strength training.
The improvement of muscular strength in CAD patients after training results in a lower muscular demand (i.e. less muscular work is required after training for the same absolute workload). This attenuates the relative workload of daily activities and in turn, reduces the daily haemodynamic load, which is desirable for the CAD patient. Thus, the component of strength training should be an essential part of exercise rehabilitation programmes in patients with CAD in order to maintain their muscular strength.
Conclusion
The application of a specific training programme, which combines both strength and aerobic exercise, for a period of 8 months improves cardiovascular endurance (exercise time and V O2peak ) and reduces significantly the haemodynamic stress during rest and sub-maximal effort. The improvements in muscular strength (of the upper and lower limbs) observed in our patients enables them to cope better with occupational and recreational activities that require muscular strength. It is important to emphasize that these benefits occur in a relatively short period of training (4 months) but are also lost within a detraining period of 3 months. According to our study walking more than two times per week is required to maintain the positive physiological adaptations obtained after supervised and systematic exercise of 8 months. Although, our results were based on a small number of low-risk patients, it is obligatory for CAD patients to follow a regular and uninterrupted exercise programme throughout life in order to improve their physical fitness and health.
Footnotes
Acknowledgements
We wish to thank A. Panagiotidou, MD and D. Goulas, MD for their medical support.