
Abstract
Background
Elevated postprandial lipemia is an independent risk factor for coronary heart disease, and bouts of moderate intensity exercise of 60 min or more are often reported to lower postprandial lipemia. Information on moderate intensity exercise bouts of shorter duration corresponding to the current recommendations of health-maintaining exercise (i.e. 30 min or energy expenditure of approximately 630 kJ), however, is scarce. Therefore, we searched for the lowest exercise intensity during 30 min of light to moderate intensity cycling that still reduced postprandial lipemia.
Design
We employed a repeated measures cross-over design.
Methods
Twelve healthy, not endurance trained, young men performed three activity trials (30 min cycling with a target energy expenditure of 420, 630 and 840 kJ) before ingestion of two mixed meals with a macronutrient composition corresponding to current recommendations and a control trial (no physical activity before meal ingestion). Capillary triacylglycerol was measured in the fasting state and hourly for 6 h after the first meal. Respiratory gases were analyzed in the fasting state, and 3 and 6 h after the first meal. Triacylglycerol and respiratory responses between the trials were compared with analyses of variance.
Results
Postprandial lipemia and the incremental area under the triacylglycerol curve were not significantly different with the activity trials compared with the control trial. The postprandial respiratory exchange ratio was also not significantly affected by activity.
Conclusions
Thirty minutes of light to moderate intensity cycling did not reduce postprandial lipemia after two mixed meals with a moderate fat content in healthy, not endurance trained, young men. Eur J Cardiovasc Prev Rehabil 13:363-368 © 2006 The European Society of Cardiology
Keywords
Introduction
The association between postprandial lipid metabolism and atherogenesis was first proposed 25 years ago [1] and it has become evident that elevated postprandial lipemia is an independent risk factor for the development and progression of atherogenesis [2] and coronary heart disease [3, 4]. Regular endurance exercise reduces the risk of cardiovascular diseases [5–8] and one mechanism responsible for this reduction could be a reduced postprandial lipemia, which is consistently lower in athletes compared with sedentary individuals [9]. Although regular endurance type activities represent an excellent form of health enhancement [10], it is unrealistic that the broad population would regularly engage in such activity. Fortunately, a substantial health benefit can already be obtained from physical activity of moderate intensity only. Epidemiological data suggest that as little as 30 min per day of moderate intensity physical activity reduces the incidence of clinical cardiovascular events in men and women [6]. This type of activity can be incorporated into daily life routines such as walking or cycling to work [11, 12].
In sedentary or recreationally active people, exercise bouts of light to moderate intensity performed just before ingestion of a meal attenuated postprandial lipemia, but the majority of the studies focused on activities of longer duration (45 min or more) [13–16]. Studies of moderate intensity exercise with shorter duration are scarce. Thirty minutes of brisk walking at 60% V O2max before ingestion of three mixed meals (breakfast, lunch, and dinner) decreased postprandial lipemia throughout the day in normolipidemic, middle-aged and overweight men and women [17]. Data about the lipemia-reducing effect of 30 min moderate exercise with other population groups are lacking. Furthermore, the minimal dose of physical activity at light or moderate intensity that still reduces postprandial lipemia is unknown.
The magnitude and duration of the lipemic response to fat-rich meals are also related to the ingested amount of fat: the higher the fat content of the meal, the greater the lipemic response [18]. In postprandial lipemia studies high fat meals (e.g. 1 g of fat per kilogram body mass (kg BM)) are often used [19], probably to induce a greater lipemia. Such high fat meals, however, do not correspond to the current recommendation of fat intake [20], and the amount ingested in these meals largely exceeds the usual fat intakes [19]. Because just 15–30 g of fat in a mixed meal increases postprandial triacylglycerol (TAG) [19], high-fat meals are not necessary to study postprandial lipemia.
The aim of the present study was to search for the lowest exercise intensity during 30 min of light to moderate intensity cycling that would still significantly lower postprandial lipemia in healthy, not endurance trained young men. The energy expenditure during the cycling bout corresponded to an energy expenditure of less (420 kJ), equivalent (630 kJ), or more (840 kJ) than the minimal recommendation of daily physical activity (i.e. energy expenditure of approximately 630 kJ) [21]. To simulate a real day situation as well as possible, two mixed meals with moderate fat content were used. One meal provided approximately one-third of the individual daily energy requirement and had a macronutrient composition according to the current nutritional recommendations [20].
Methods
The study was approved by the Ethical Committee of the ETH Zurich and was carried out according to a repeated measures cross-over design.
Subjects
Twelve healthy, normal weight and not endurance trained men participated in the study (Table 1). They were non-smokers and all normotriacylglycerolemic according to the classification of the National Cholesterol Education Program [22]. All participants of the study gave written informed consent.
Characteristics of the subjects (men, n= 12)
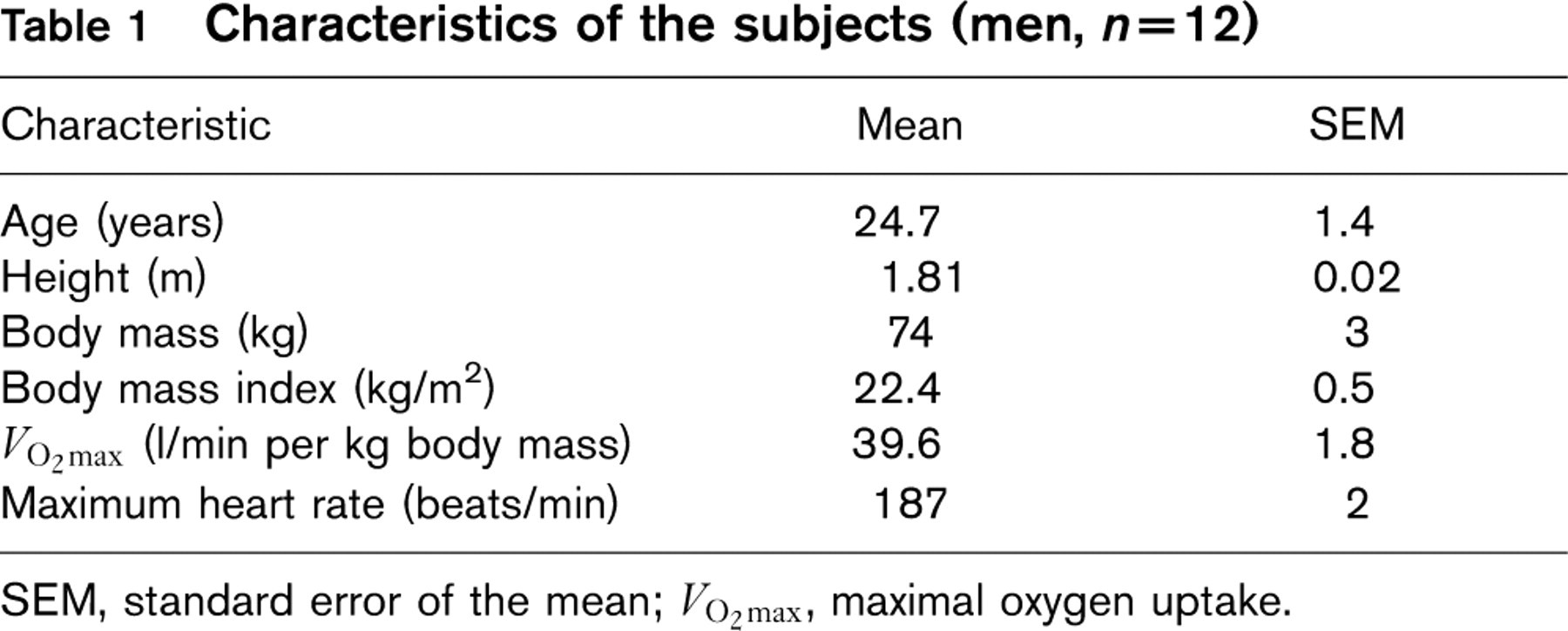
SEM, standard error of the mean; V O2max, maximal oxygen uptake.
Preliminary tests
Each subject performed two preliminary tests on the cycle ergometer. Maximal oxygen uptake (V O2max) was determined in the first test. Subjects started cycling at 80W and the work rate was increased by 30W every 2 min until exhaustion. The cadence was kept at 75 revolutions per minute. V O2max was considered to be valid when at least two of the following three criteria were met: respiratory exchange ratio (RER) >1.1; heart rate within 10 beats per minute of the predicted maximum (220 beats per minute minus age); rating of perceived exertion ≥19 on the Borg 6–20 scale. In the second preliminary test the steady-state relationship between work rate and energy expenditure for each subject was determined. Subjects cycled three times for 10min at the work rate of 45, 75 and 105W. The results of that test provided a regression line showing the dependency of energy expenditure and work rate for each subject. The regression line was used to determine the work rate in the activity trials resulting in the target energy expenditure.
Main trials
Each subject undertook four trials: one control trial with no activity and three activity trials with intervals of at least 4 days. To ensure similar baseline conditions, subjects were only allowed to follow activities of daily living on the 2 days prior to the test days. The day before the first test day, subjects recorded their food intake and were told to repeat the food intake on the days preceding subsequent test days. The day preceding the test day they were only allowed to drink moderate amounts of alcohol (maximum one to two glasses of beer or wine) and caffeine drinks (maximum two cups of coffee or four cups of tea, or 1 1 of a caffeine-containing soft drink). Additionally, subjects received a standardized evening meal (spaghetti, tomato sauce, cheese, and apple sauce), to prepare at home, providing 0.2 g fat per kg BM, 2.4 g carbohydrates per kgBM, 0.5g protein per kgBM, and 55 kJ per kg BM. After an overnight fast of at least 12h, the subjects arrived at the laboratory via public transportation. The compliance with the instructions was checked through questionnaires that were filled out by the subjects just after the arrival at the laboratory.
After a rest of 10min, fasting capillary TAG was measured and subsequent respiratory measurements were made for 10 min in the resting state while sitting. Then subjects cycled for 30 min on a cycle ergometer (Ergometrics 800 S; Ergoline, Bitz, Germany) in the activity trials, or rested meanwhile in the control trial. The work rate was set resulting in a target energy expenditure of 420 kJ (EE420), 630kJ (EE630), or 840kJ (EE840) in the activity trials. During cycling, respiration and heart rate were measured continuously. A second fasting capillary TAG measurement was taken 1h after the first TAG measurement, just before serving breakfast. The breakfast consisted of commercially available cereals, yogurt, cream and a chocolate drink providing 0.5 g fat per kg BM, 1.8 g carbohydrates per kg BM, 0.5 g protein per kg BM, and 56 kJ per kg BM. Subjects received lunch 3 h after breakfast. The meal served at lunch time consisted of commercially available wholemeal wheat crackers, chocolate cream, cream, biscuits and orange juice providing 0.5 g fat per kg BM, 1.9 g carbohydrates per kg BM, 0.3 g protein per kg BM and 56 kJ per kg BM. The food was obtained at one of the two largest supermarkets in Switzerland, and each food item was precisely weighed. During 6 h after breakfast, finger capillary TAG measurements were performed every hour to assess the postprandial period. Three and six hours after breakfast respiratory measurements in the resting state were made for 10 min. During the postprandial period water was available ad libitum in the first trial, and the ingested amount was replicated in the following trials. The subjects performed seated activities until the end of each test day.
Indirect calorimetry, energy expenditure calculations, and heart rate measurement
Oxygen uptake and carbon dioxide production during physical activity and at rest were determined using a pulmonary gas exchange system (Quark b2; Cosmed, Rome, Italy). Respiration gases in the resting state were determined during a 10-min period. For calculation of RER, the median from minutes 4 to 9 was used. Energy expenditure, fat oxidation, and carbohydrate oxidation during physical activity were calculated according to the Weir formula [23] and a table of the non-protein respiratory quotient [24], with the assumption that the urinary nitrogen excretion was negligible. Heart rate during physical activity was measured with Polar Vantage NV (Polar Electro Oy, Kempele, Finland).
Triacylglycerol measurement
Capillary TAG concentration was determined enzymatically with the Accutrend GCT system (Roche Diagnostics, Mannheim, Germany) using a reflection–photometric method. The measurements – blood sampling on finger and handling of the device – were performed according to the manufacturer's instruction manual and by the same investigator with all subjects. TAG measurements by Accutrend GCT have been validated against standard enzymatic methods and a correlation coefficient of ≥0.94 was found between the methods [25–27]. The coefficient of variation for the Accutrend GCT system has been reported to be ≤ 6% [25, 27], which is not substantially different from the required coefficient of variation of ≤ 5% for TAG measurement methods [28]. The Accutrend system detects TAG reliably, regardless of the nature of the TAG-carrying lipoprotein species [chylomicrons or very low density lipoproteins (VLDL)] [25]. Therefore, it is suitable for the determination of both fasting and postprandial TAG [25]. The measurement range for capillary TAG is 0.80 to 6.68 mmol/l. If TAG values were below the detection limit, then 0.80 mmol/l was used for calculations.
Data analyses and statistics
The area under the TAG curve (AUC) and the incremental area under the TAG curve (dAUC) were calculated using the trapezoidal method [29]. Statistical analyses were performed with Systat software version 10 (SPSS Inc., Chicago, Illinois, USA). The results of the four different trials were compared with an analysis of variance (general linear model; GLM) with the activity intervention, subject, and trial order as grouping factors. Postprandial TAG values and RER fasting, and 3 and 6 h postprandial were compared with GLM for repeated measurements to detect activity effects and activity by time interaction. When significant overall differences between the trials were found, the data were further analyzed with Bonferroni's post-hoc test. Data are presented as mean (SEM). A P-value of less than 0.05 was considered significant.
Results
Triacylglycerol measurements with the Accutrend GCT system
All in all, 45 of the 384 TAG measurements were below the detection limit of 0.8 mmol/l. In the fasting state before and after the activity bout, the number of measurements below the detection limit was similar in all trials (three to five out of 12 in each trial). One hour postprandially, one or two of the 12 measurements were below the detection limit in all trials. All measurements were above the detection limit from 2–5 h postprandially and 6 h postprandially one measurement of the control and EE420 trial was below the detection limit.
Fasting values
Fasting TAG values and fasting RER in rest did not differ between trials (TAG, P = 0.997; RER, P = 0.84). Values for fasting TAG were 1.08 (0.09), 1.07 (0.08), 1.09 (0.10), and 1.08 (0.09) mmol/l, and values for fasting RER in rest were 0.90 (0.02), 0.90 (0.02), 0.92 (0.02), and 0.91 (0.02) with the control, EE420, EE630, and EE840 trials, respectively.
Responses during 30 min of ergometer cycling in the three activity trials (n = 12)
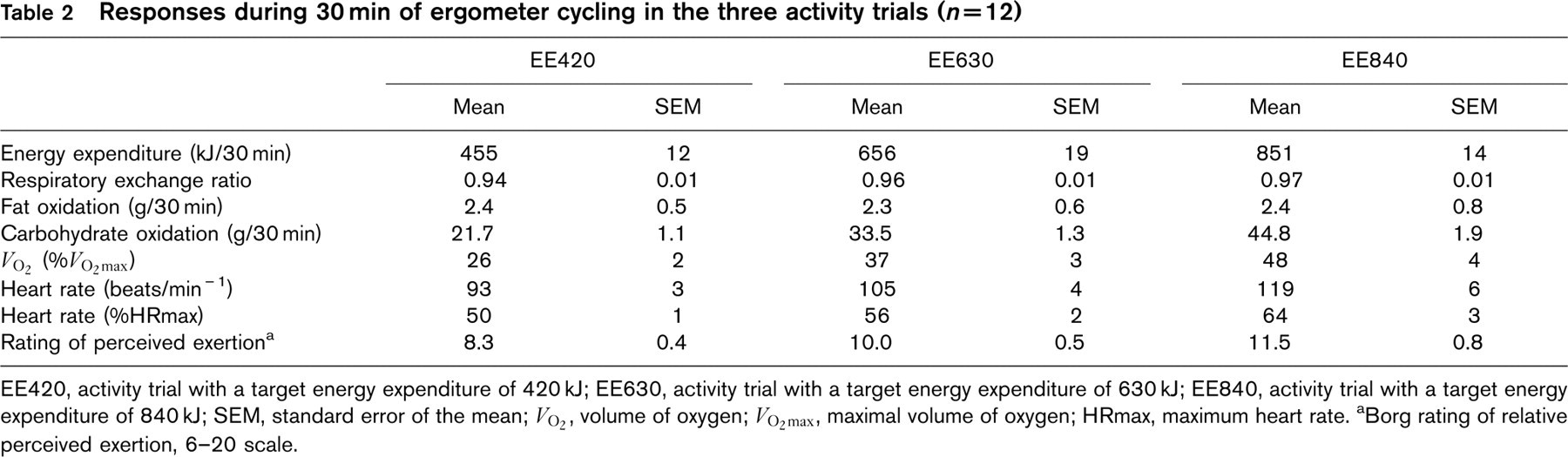
EE420, activity trial with a target energy expenditure of 420 kJ; EE630, activity trial with a target energy expenditure of 630 kJ; EE840, activity trial with a target energy expenditure of 840 kJ; SEM, standard error of the mean; V O2, volume of oxygen; V O2max, maximal volume of oxygen; HRmax, maximum heart rate. aBorg rating of relative perceived exertion, 6–20 scale.
Values during activity
Effective energy expenditure during the 30min of ergometer cycling was 455 (12), 656 (19) and 851 (14) kJ with the EE420, EE630, and EE840 trials, respectively, and corresponded to 26 (2), 37 (3), and 48% (4%) of V O2max (Table 2). According to the classification of physical activity intensity by the American College of Sports Medicine [30], the intensity with the EE420 and EE630 trials was classified as light (20–39% V O2max) and with the EE840 trial as moderate (40–59% V O2max), respectively.
Fat oxidation and RER during the activity bout were not statistically different between the three trials (fat oxidation, P = 0.97; RER, P = 0.08). Carbohydrate oxidation and energy expenditure increased significantly, however, with increasing intensity (P >0.001).
Postprandial triacylglycerol values
Postprandial TAG values did not differ statistically between the trials (P = 0.92; Fig. 1). Highest values were observed 5h postprandially and were 2.92 (0.51), 2.98 (0.37), 2.90 (0.46), and 3.00 (0.43) mmol/l with the control, EE420, EE630, and EE840 trials, respectively. There were no statistically significant differences in the AUC (P = 0.93) or dAUC (P = 0.97) between the four trials (Fig. 2). To detect a statistically significant difference in dAUC between the inactivity and the EE840 trials a sample size of 780 subjects would have been required (power, 0.80).
Postprandial respiratory exchange ratio values
There were no statistically significant differences between the trials in resting RER 3 or 6 h postprandially (P = 0.97; Fig. 3). RER was highest 6 h postprandially in all trials.
Discussion
Our findings indicate that 30min of cycling with a light to moderate intensity and an energy expenditure of less, equal, or more than the current recommendation of minimal daily physical activity (i.e. energy expenditure of approximately 630 kJ [21]) did not attenuate postprandial lipemia associated with the consumption of two ordinary mixed meals with a moderate fat content. Further, RER in the postprandial state was also unaffected by the activity compared with the control trial. This is in contrast to the study from Murphy et al. [17] that had a similar study design concerning the duration of exercise (30 min), the timing of the activity bout (just before the test meal), the type of meals (ordinary mixed meals with a moderate fat content), and the number of meals (more than one, simulating the normal course of a day). That study showed that 30 min of brisk walking undertaken in one session before breakfast or three 10-min sessions before breakfast, lunch, and dinner reduced the postprandial TAG concentration and RER in ten middle-aged men and women. Though the designs of both studies were similar, however, the exercise mode (walking versus cycling) and the study subjects differed in several aspects: our subjects were not overweight or of older age and, additionally, the exercise intensity was slightly lower in our study (EE840: 48% V O2max compared to 60% of V O2max). Even though the mechanism responsible for the exercise-induced TAG reduction is still not entirely understood [9], the lower relative fat oxidation rate in our subjects both in the fasting and postprandial state, which was indicated by a higher RER, could have contributed to the lack of influence on postprandial lipemia. Goedecke et al. [31] showed a large variation of fasting RER in rest in trained cyclists that ranged from 0.72 to 0.93 corresponding to a relative fat oxidation rate of 93 to 23%. Furthermore, the variability in RER persisted during sub-maximal exercise ranging from 0.82 to 0.98 at 63% V O2max. A large variation of RER that ranged from 0.83 to 0.95 was also observed in untrained subjects during 60 min of cycling at 55 % of V O2max [32]. In our study, RERs during activity were 0.94, 0.96, and 0.97 with the EE420, EE630, and EE840 trials, respectively, and corresponded to a relative fat oxidation rate of 18, 12, and 8%. Absolute fat oxidation rate during activity was 0.08 g/min in all trials. This is little compared with the maximum fat oxidation rate of 0.46 g/min in 300 healthy, trained and untrained men and women of all ages found by Venables et al. [33]. The low fat oxidation rate in our subjects is explainable because the exercise intensities were not chosen to reach the maximum fat oxidation rate. Additionally, in the study of Venables et al. [33] the maximum fat oxidation rate achieved during activity in healthy trained and untrained men and women varied tenfold and ranged from 0.18 to 1.01 g/min, and, accordingly, the maximum fat oxidation rate occurred in a wide range of 25% to 77% of V O2max. Since our subjects were untrained, we assume them to have a rather low fat oxidation capacity as Bergman et al. [34] showed lower relative and absolute fat oxidation rates in fasting, untrained compared with trained men during a cycling exercise at 22 or 40% of V O2peak.
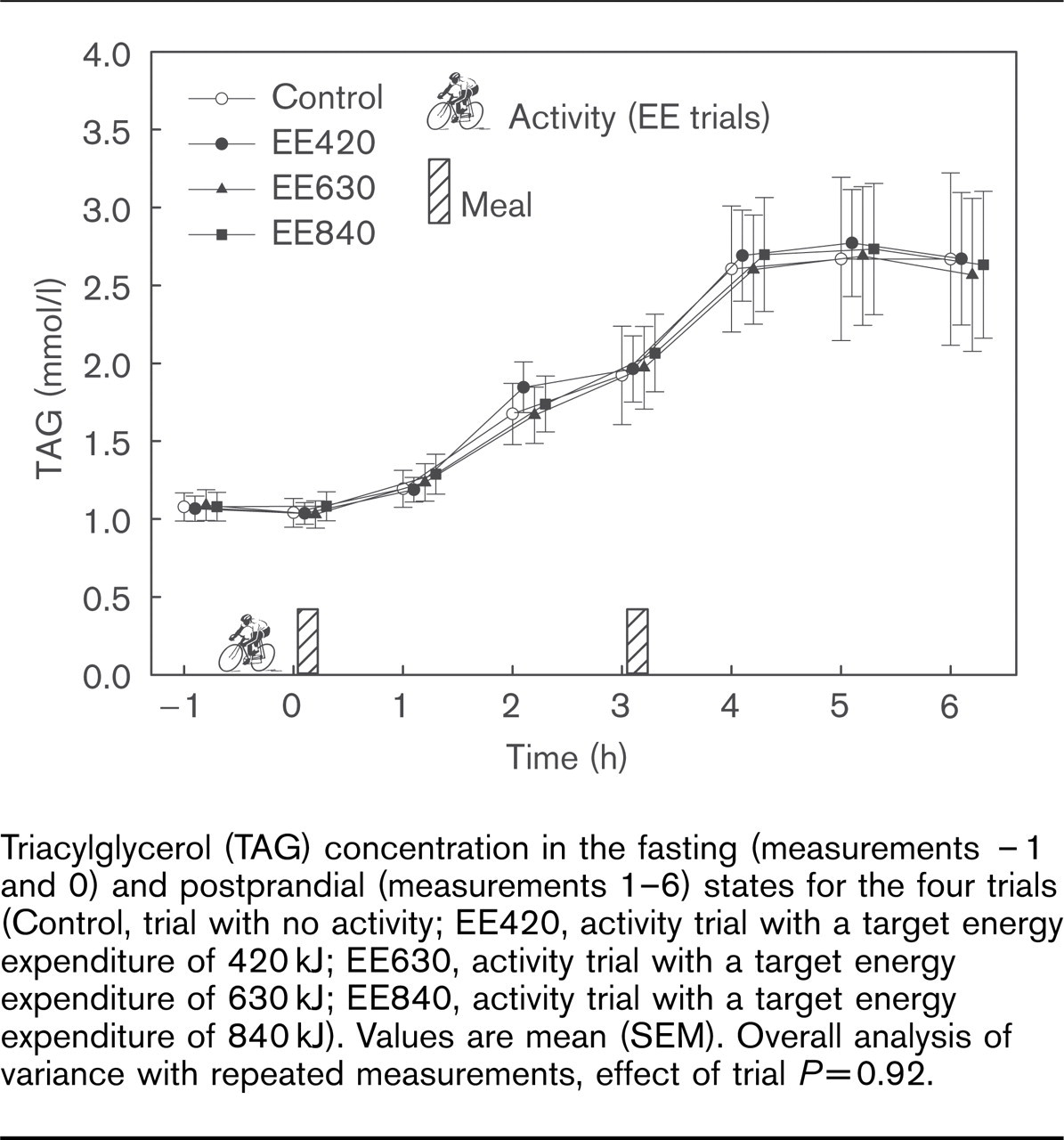
Triacylglycerol (TAG) concentration in the fasting (measurements – 1 and 0) and postprandial (measurements 1–6) states for the four trials (Control, trial with no activity; EE420, activity trial with a target energy expenditure of 420 kJ; EE630, activity trial with a target energy expenditure of 630 kJ; EE840, activity trial with a target energy expenditure of 840 kJ). Values are mean (SEM). Overall analysis of variance with repeated measurements, effect of trial P =0.92.
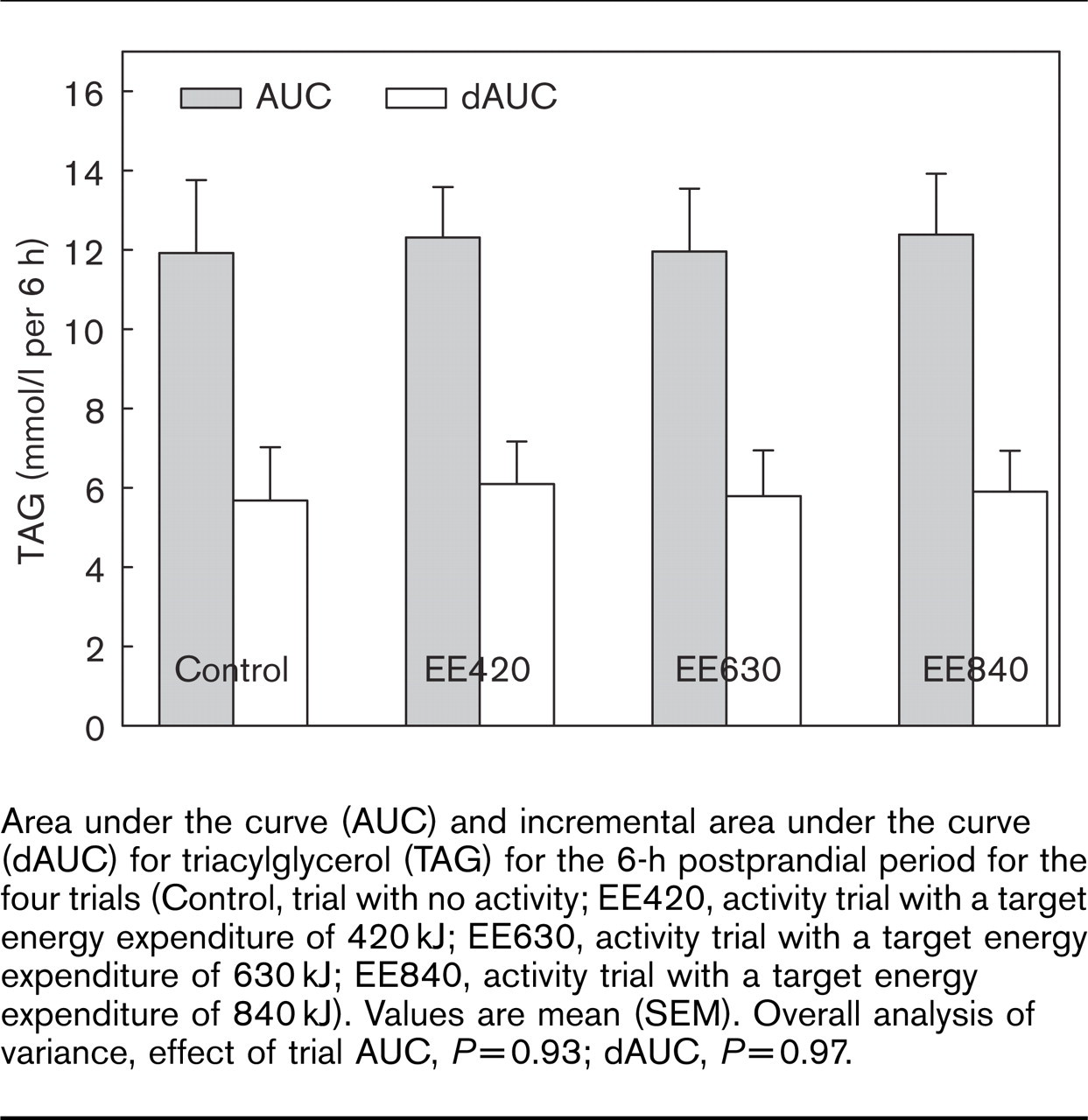
Area under the curve (AUC) and incremental area under the curve (dAUC) for triacylglycerol (TAG) for the 6-h postprandial period for the four trials (Control, trial with no activity; EE420, activity trial with a target energy expenditure of 420 kJ; EE630, activity trial with a target energy expenditure of 630 kJ; EE840, activity trial with a target energy expenditure of 840 kJ). Values are mean (SEM). Overall analysis of variance, effect of trial AUC, P = 0.93; dAUC, P = 0.97.
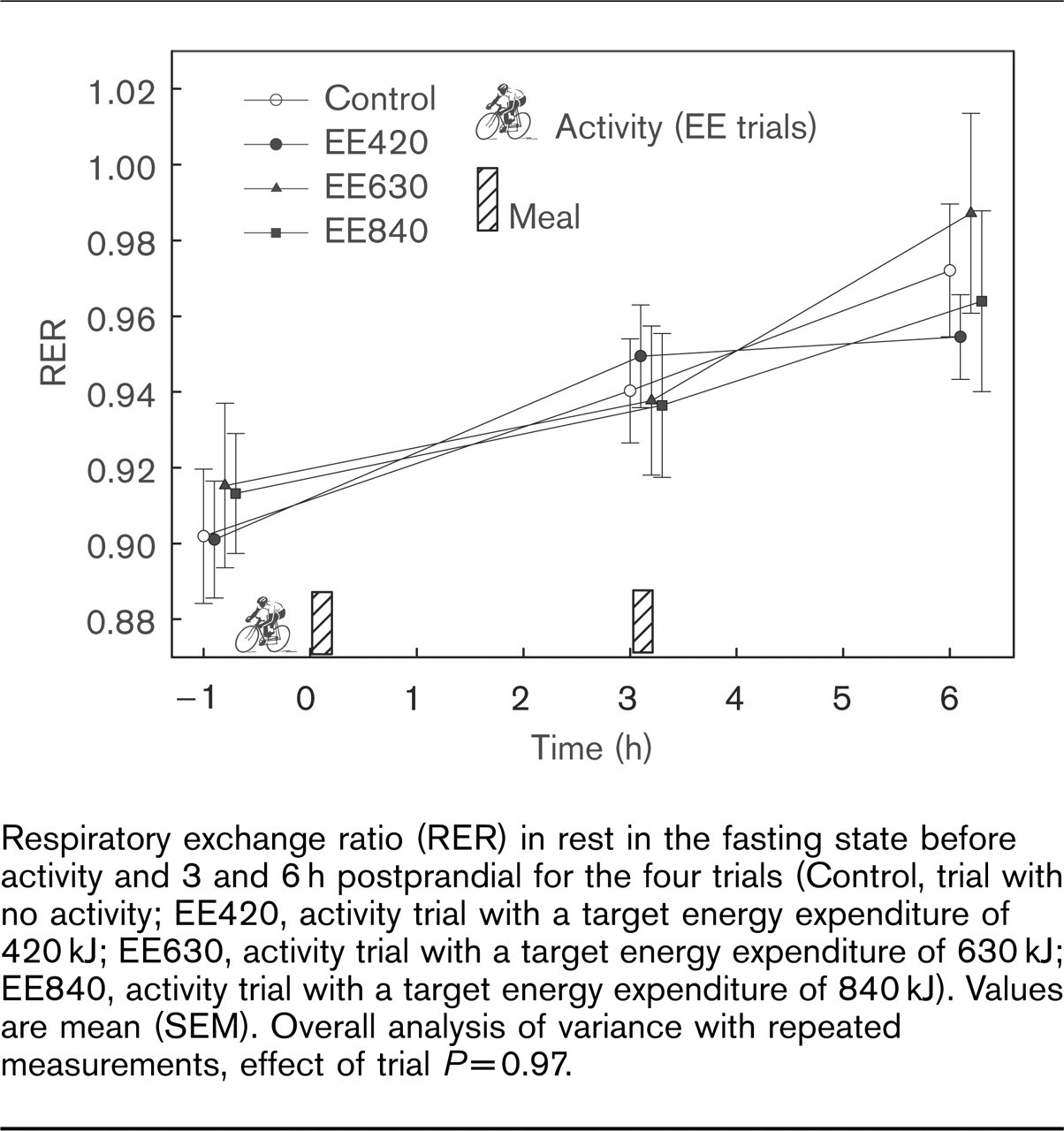
Respiratory exchange ratio (RER) in rest in the fasting state before activity and 3 and 6 h postprandial for the four trials (Control, trial with no activity; EE420, activity trial with a target energy expenditure of 420 kJ; EE630, activity trial with a target energy expenditure of 630 kJ; EE840, activity trial with a target energy expenditure of 840 kJ). Values are mean (SEM). Overall analysis of variance with repeated measurements, effect of trial P = 0.97.
Nevertheless, our results are in accordance with the study of Petridou et al. [16] that was published after having finished our experiment. They examined the influence of 45 min cycling at 62% of predicted maximum heart rate just before ingestion of a meal with a moderate fat content in healthy, young and sedentary men. The exercise bout lowered postprandial lipemia by 17%, but the attenuation did not reach statistical significance.
In summary, we conclude that in healthy, not endurance trained young men, a single bout of 30min light to moderate intensity cycling with an energy expenditure of less, equivalent or more than the minimal recommendation of physical activity did not reduce postprandial lipemia after two meals that had a macronutrient composition corresponding to current recommendations. The reasons we did not observe a reduction in postprandial lipemia could be a too short duration and/or too light intensity of the activity bout or the moderate fat content of the meals. These results do not question the generally acknowledged health-maintaining/health-improving effects of 30min of moderate intensity exercise [21]. It should be reconsidered, however, if the exercise-induced reduction in postprandial lipemia observed after high fat meals can be extrapolated to more realistic daily life settings.