
Abstract
Background
It is unclear how much of the reduction in cardiac mortality in coronary heart disease (CHD) patients with exercise training is the result of direct effects on the heart and coronary vasculature, or to indirect effects, via primary risk factors.
Objective
The aim of this article was to quantify the cardiac mortality benefits of exercise-based rehabilitation attributable to risk factor reductions versus the direct effects on the heart and vasculature.
Methods
The IMPACT coronary heart disease model was used to examine the reduction in cardiac mortality attributable to changes in risk factors from a meta-analysis of cardiac rehabilitation randomized, controlled trials. Patients were receiving rehabilitation following an acute myocardial infarction, angina pectoris or revascularization. Outcomes considered were primary risk factors (total cholesterol, systolic blood pressure and smoking behaviour) and cardiac mortality.
Results
Nineteen exercise-only cardiac rehabilitation trials (including 2984 patients) were identified. Across these trials, exercise training reduced pooled cardiac mortality by 28% (relative risk, 0.72, 95% confidence interval 0.55–0.95), with 30 fewer deaths than in the control group. Applying the CHD model, approximately 17 (58%) of these 30 fewer deaths were attributable to reductions in major cardiovascular risk factors: 7.1 deaths (minimum estimate 6.2, maximum estimate 9.5) attributable to an 18% reduction in smoking prevalence; 5.9 deaths (minimum −0.6, maximum 12.6) to a 0.11 mmol/l reduction in cholesterol, and 4.4 deaths (−1.0 minimum, 6.7 maximum) to a 2.0 mmHg reduction in systolic blood pressure.
Conclusions
Approximately half of the 28% reduction in cardiac mortality achieved with exercise-based cardiac rehabilitation may be attributed to reductions in major risk factors, particularly smoking. Eur J Cardiovasc Prev Rehabil 13:369–374 © 2006 The European Society of Cardiology
Keywords
Introduction
Exercise-based rehabilitation is widely recognized to play a key role in the management of coronary heart disease (CHD) [1–3]. This role is supported by a substantive body of randomized, controlled trial (RCT) evidence that exercise training in CHD patients can result in a 25% reduction in cardiac mortality, equivalent to many cardiovascular drugs [4, 5]. The precise mechanisms by which exercise training improves mortality in CHD patients, however, has not been fully elucidated [6, 7]. Exercise training is known to have a number of direct effects on the heart and coronary vasculature, including reductions in myocardial oxygen demand. Furthermore in patients with CHD and endothelial dysfunction, exercise attenuates or reverses the abnormal vasoconstrictive response to acetylcholine [6, 7]. A recent systematic review of RCTs confirmed the significant reduction in all cause mortality and cardiac mortality with exercise-based rehabilitation, compared to usual care [8]. Moreover, improvements were also reported in primary coronary risk factors: smoking, total cholesterol and systolic blood pressure [8]. It is well recognized that mortality risk is reduced by 36% or more in CHD patients who stop smoking [9], or decrease their total cholesterol [10], and by at least 20% from a decrease in blood pressure [11]. The important question thus remains: does exercise training principally decrease cardiac mortality in CHD patients by direct effects on the heart and coronary vasculature, or indirectly, via primary risk factors?
Worked example of calculation of deaths prevented or postponed by risk factor reduction in patients also undergoing exercise-based rehabilitation
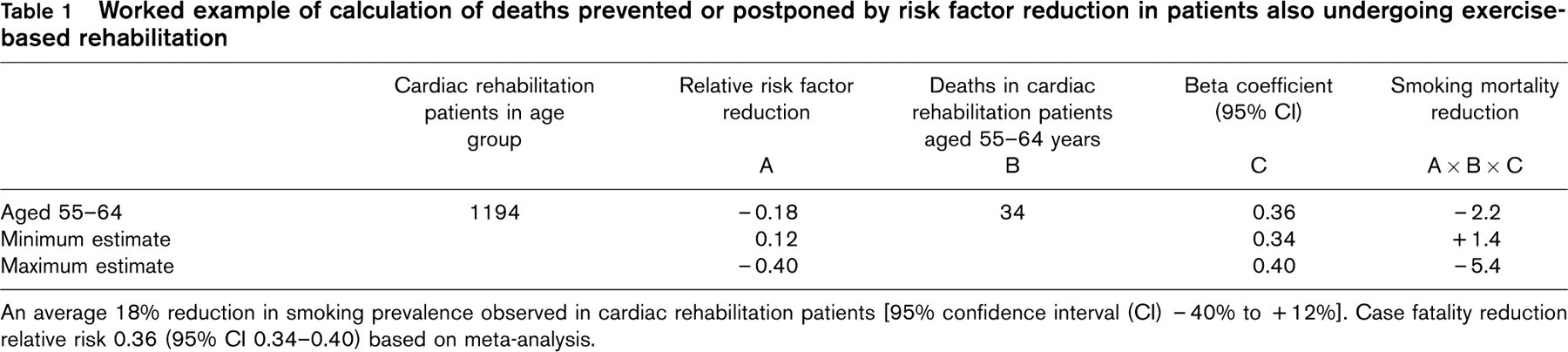
An average 18% reduction in smoking prevalence observed in cardiac rehabilitation patients [95% confidence interval (CI) − 40% to + 12%]. Case fatality reduction relative risk 0.36 (95% CI 0.34–0.40) based on meta-analysis.
The aim of this paper was therefore to determine how much of the cardiac mortality benefits of exercise training in patients with CHD might be attributed to the three major risk factor reductions as opposed to the direct benefits of exercise per se.
Methods
Systematic review of exercise-training and associated risk factor changes
We used data from the recently published update meta-analysis of RCTs of exercise-based cardiac rehabilitation [8]. Methodological details of this systematic review are given elsewhere [8]. In order to specifically assess the effect of exercise training, the subgroup of RCTs was selected for which exercise training was the only therapy (i.e. no co-therapies such as diet and psychological interventions).
The IMPACT coronary heart disease model
The previously validated IMPACT CHD mortality model has been described in detail elsewhere [12, 13]. In brief, it synthesises data on patient numbers, treatments, risk factors and mortality benefits. In this study, the IMPACT model was used to synthesize data on: the risk factor changes achieved in patients undergoing cardiac rehabilitation for whom exercise was the only intervention; and the mortality reductions attributable to changes in specific factor changes. Relative risk reductions quantifying the mortality benefits from risk factor reduction in CHD patients were obtained from large meta-analyses addressing smoking cessation, total cholesterol reduction, and blood pressure reduction [9–12, 14].
Calculating the deaths prevented by risk factor reductions
The deaths prevented or postponed by the reductions in smoking, total cholesterol or blood pressure, stratified by age, were estimated as the product of three variables: the baseline mortality rate (the number of coronary heart disease deaths observed in the control group, stratified by age); the relative reduction in each specific risk factor observed in the patients randomized to exercise; and the relative risk quantifying the relationship between change in that specific risk factor and the consequent change in CHD mortality rate. This gave a 36% mortality reduction for smoking cessation, [95% confidence interval (CI) 29–41%] [9]; a 35% mortality reduction (95% CI 31–39%) for a 0.6 mmol/l reduction in total cholesterol [10] and an 11% mortality reduction (95% CI 9–14%) for a 12 mmHg reduction in systolic blood pressure [11]. A worked example is shown in Table 1.
Statistical analyses
Risk factor changes and cardiac mortality were pooled across exercise-based rehabilitation trials using fixed effects meta-analysis, except where substantial heterogeneity existed according to the χ2 statistic, and a random effects model was used [15].
Because of the uncertainties surrounding the model key parameters, a sensitivity analysis was performed using the 95% confidence intervals for the changes in cholesterol, blood pressure and smoking, and relative risk reduction [13]. These are presented as maximum and minimum estimates (see Table 1).
Results
Exercise was a sole intervention in 19 RCTs [16–34], including 2984 patients with CHD diagnoses of acute myocardial infarction, revascularization or angina. The mean age was 54 years (range 45–71 years) with a mean follow-up of 2 years. A proportion of these trials reported cardiac mortality (eight trials) and risk factor reduction (nine trials).
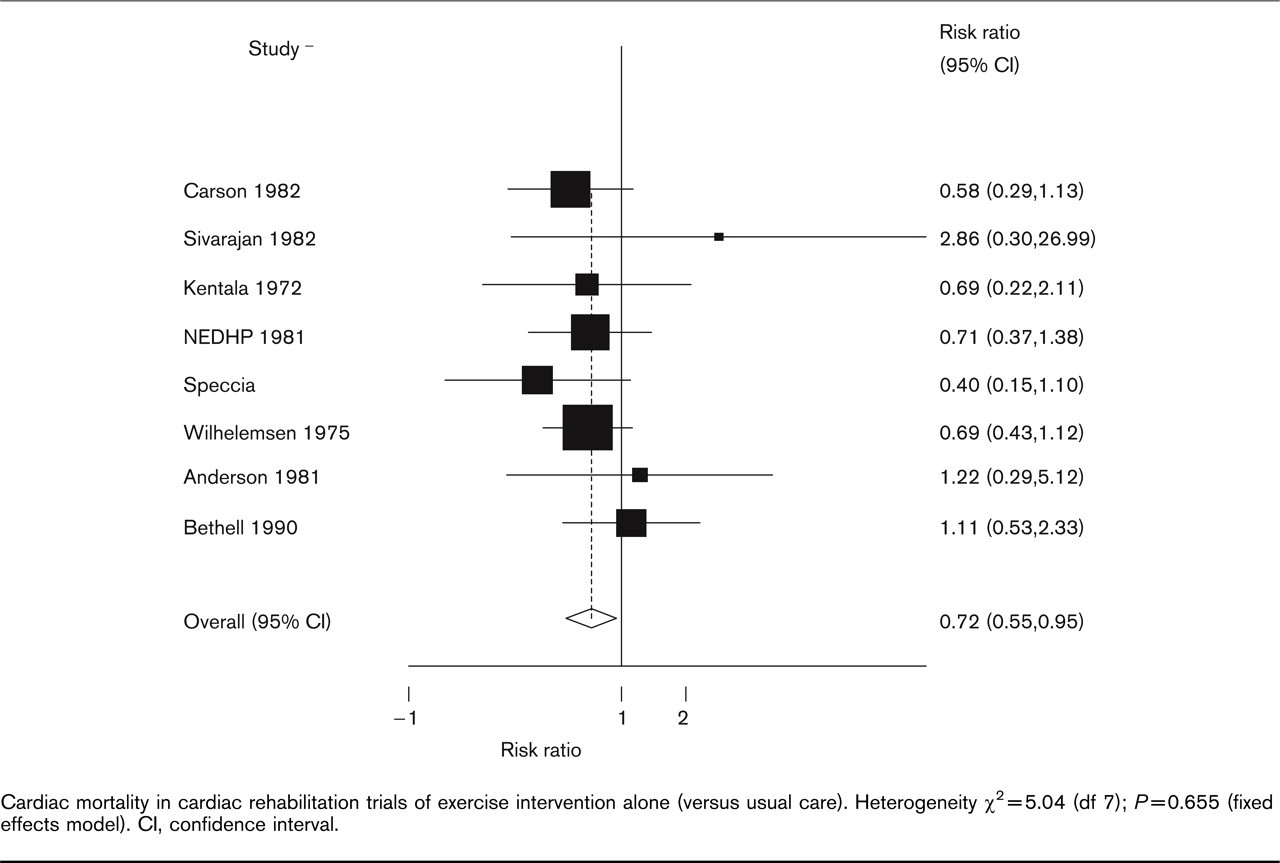
Cardiac mortality in cardiac rehabilitation trials of exercise intervention alone (versus usual care). Heterogeneity χ2 = 5.04 (df 7); P = 0.655 (fixed effects model). CI, confidence interval.
Exercise reduced cardiac mortality by 28% (95% CI 5–45%) (Fig. 1); 80 deaths were observed in the intervention group, 30 less than the 110 observed in the control group. Greater risk factor decreases were seen in the exercise training than in the usual care group (a pooled 18% decrease in smoking prevalence; and pooled mean differences of 0.11 mmol/l for cholesterol and 2.0 mmHg for systolic blood pressure) (Fig. 2).
These declines in the three major risk factors explained approximately 16 of the 30 fewer deaths in the model analysis; with 7.1 fewer deaths (minimum estimate: 6.2, maximum estimate: 9.5) attributable to the 18% reduction in smoking prevalence, 4.4 fewer deaths (min − 1.0, max 6.7) to the 2.0 mmHg reduction in systolic blood pressure and 5.9 fewer deaths (min − 0.6, max 12.6) attributable to the 0.11 mmol/l reduction in cholesterol (Table 2).
Reduced smoking therefore accounted for approximately 24% of the mortality reduction, systolic blood pressure reduction for 15% and cholesterol for a further 19.7%. The three together accounted for approximately 17 fewer deaths, which represented approximately 58% of the total mortality reduction.
Discussion
Exercise-based rehabilitation in CHD patients reduces cardiac mortality by some 28% over an average period of 2 years follow-up. This study suggests that approximately half this mortality reduction may be attributable to reductions in smoking, cholesterol and blood pressure, and hence, by implication, improvements in atherosclerosis and thrombosis. The remainder of the mortality reduction in these CHD patients may therefore be attributable to the beneficial effects of exercise acting through non-risk factor mechanisms. Such effects could plausibly include decreased myocardial oxygen demand, reduced propensity towards ventricular arrhythmias, reduced platelet aggregation, increased fibrinolytic activity and improved myocardial perfusion (via regression of artherosclerotic disease, improved collateralization improvement in endothetial stability and depression) [6, 7, 35]. Depression may operate through antidepressant cardiotoxicity; reduced functional capacity; an association with greater disease severity; non-adherence to therapies; impaired autonomic tone; increased platelet aggregation; or inflammatory processes [36]. Our results appear to support the very limited evidence that already exists in this area. In their trial of exercise training in patients following coronary angioplasty, Belardinelli et al. [37] reported, in spite of controlling for changes in risk factors, exercise remained an independent predictor of re-stenosis and, therefore, potential future cardiac events [37].
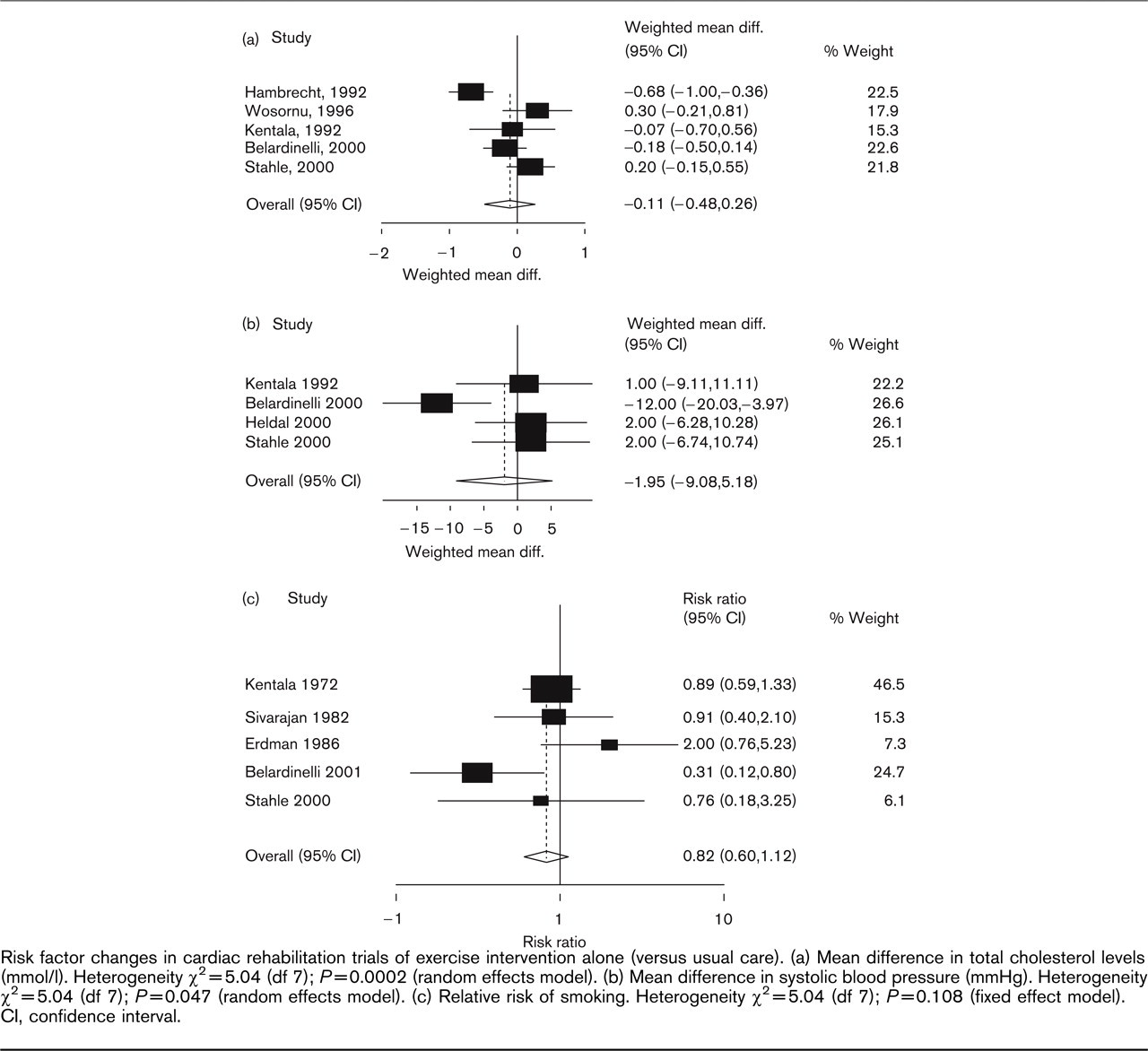
Risk factor changes in cardiac rehabilitation trials of exercise intervention alone (versus usual care). (a) Mean difference in total cholesterol levels (mmol/l). Heterogeneity χ2 = 5.04 (df 7); P = 0.0002 (random effects model). (b) Mean difference in systolic blood pressure (mmHg). Heterogeneity χ2 = 5.04 (df 7); P = 0.047 (random effects model). (c) Relative risk of smoking. Heterogeneity χ2 = 5.04 (df 7); P = 0.108 (fixed effect model). CI, confidence interval.
Exercise-based cardiac rehabilitation trials: number of deaths prevented or postponed attributable to risk factor changes

BP, blood pressure.
Our analysis was deliberately confined to patients undergoing exercise-based rehabilitation, rather than more comprehensive rehabilitation that included secondary preventative interventions specifically designed to modify major lifestyle factors, such as nutritional counselling, risk factor education and psychosocial management [38]. Nevertheless, small, but potentially important, risk factor reductions occurred in these 2984 patients undergoing exercise-based intervention alone. Furthermore, it is well documented that exercise can exert a beneficial effect on blood pressure, cholesterol and smoking behaviour of CHD patients [6].
The study has a number of potential limitations. Most trials pooled in the meta-analysis had relatively short follow-up, with a median of only 2 years. Longer-term benefits remain speculative at present. Secondly, the statistical power was not ideal. Even after pooling all eligible trials, less than 3000 patients were included, with a total mortality reduction observed of only 30 deaths. Not all trials reported risk factor changes. Furthermore, modest changes in risk factors levels were consequently statistically borderline for cholesterol and blood pressure, though rather more substantial for smoking. The model was also based on mean values arising from the large meta-analysis, rather then the ideal, an analysis of changes in individual subjects. The findings remained relatively robust however, even when more extreme values were combined in the sensitivity analyses (Table 1). Thirdly, using just three major risk factors, the results explained some 50% of the mortality reduction. It is possible, but unlikely, that other risk factors, such as diet, might have explained some of the remaining mortality benefit. Very few included trials reported details of other lifestyle behaviour modifications. Fourthly, few trials reported changes in high-density lipoprotein/low-density lipoprotein ratios; however, the reduction in total cholesterol will have captured most of the benefit [10]. Fifthly, the relationship between the change in risks factor and the consequent change in CHD mortality rate was sourced from systematic reviews of treatment studies, many of which were undertaken at least a decade ago. Because these were expressed as relative risks, however, this relationship is likely to hold true in more recent years, even in spite of potential reductions in risk factor prevalence. Finally, although the relative risk reduction quantifying the risk factor effect on cardiac mortality was assumed to be independent, some residual confounding may have persisted [9–12].
Many of these limitations might be resolved by an individual patient analysis based on a very large and definitive trial. Given the current level of evidence, however, further trials of exercise training compared with conventional care alone in CHD patients are becoming ethically unacceptable [39].
In spite of these limitations, our study has three important service implications. Firstly, given that exercise appears to have an independent mortality benefit, it reinforces the current clinical guideline recommendation that exercise training should form the core of the rehabilitative process for CHD patients [1–3]. Secondly, rehabilitation practitioners should welcome even small improvements in patients’ individual risk factors, because these may together produce substantial cumulative mortality benefits. The addition of secondary preventative medical and behavioural interventions that target primary risk factors will provide further gains. The main policy implication is also clear. Cardiac rehabilitation needs a supportive social and economic context, with more energetic national and European policies on healthy diet, physical activity, transport and smoking cessation.
In conclusion, approximately half of the 28% reduction in cardiac mortality achieved with exercise-based cardiac rehabilitation may well be attributed to reductions in major risk factors, principally smoking.