
Abstract
The problem of poverty leads to increased use of both legal and illegal drugs. Tobacco and alcohol are legal drugs that cause particular concern. Both drugs are widely abused in Germany by people attempting to escape their everyday problems. For decades it has been known that tobacco and alcohol use are more prevalent in lower socio-economic groups of society (those with low educational achievement, compared with people with further or higher education qualifications). Tobacco and alcohol use is particularly high among the unemployed, either temporarily or long-term, as well as people living alone. Children and women are more concerned about smoking than men. Female loneliness, often accompanied by the appearance of depressive reactions or of depression, increases the likelihood of cigarette smoking. Poor people spend up to 20% of their income on tobacco. In many industrialized countries, the age of onset of smoking is becoming younger and younger, increasing the risk of development of avoidable tobacco-related illnesses at an earlier age. This means that young smokers who develop chronic tobacco-related illnesses will require medical care over many years, increasing the cost of treating tobacco-related disease. Within the next few years, effective prevention programs against smoking must be developed, particularly for the lower socio-economic populations, in order to stop the cost of healthcare systems spiraling over the coming decades. Eur J Cardiovasc Prev Rehabil 13:312–318 © 2006 The European Society of Cardiology
Introduction
Addiction and poverty have grown into a massive global problem. Doctors, sociologists, psychologists and politicians, who are approaching both phenomena from different perspectives, still find themselves in the initial stages of addressing the issues. One of the key factors that causes the problems of addiction and poverty to get little attention in Germany is rooted within the social system which, although it is referred to as a ‘social market economy', does not provide socially underprivileged people (‘the poor') with a lobby. In terms of addiction, alcoholism prevailed over tobacco dependence in the focus of negative social debates. Alcoholism is still being linked to negative aspects, while tobacco addiction is not; cigarette smoking is considered ‘socially acceptable'. In industrialized countries, cigarette smoking represents 95% of tobacco use. In Germany alone, there are more than 22 million smokers: a mass epidemic [1].
Given that there are an estimated 1.4 billion smokers worldwide and that on a global scale there are 4 million tobacco-related deaths every year, cigarette smoking is the second largest cause of death [2].
The grave social problem today is that socially weak members of the population are more likely to abuse the self-destructive legal and illegal drugs than those with higher incomes and better qualifications. Consequently the socially vulnerable are leading the disease statistics in a dual sense under the motto ‘Because you are poor, you have to die sooner’ [3, 4]. This affects the unemployed, government support notwithstanding, those living alone (women to a higher degree than men) and, in particular, pregnant women. The latter represent a dual risk, given that they are also responsible for the unborn child, which may be subjected to lifelong physical and psychological disadvantages if the mother smokes during the pregnancy [5].
Low socio-economic status and smoking
The social contradictions are expanding, not only in the United States [6] but on a global scale [7–13]. The fact that people struggling with adverse social conditions smoke more is well-known internationally [14–16]. In Germany these interdependencies have been researched as part of the Mikrozensus Studie (Micro-census Study) [17, 18], which showed that increased consumption of cigarettes goes hand in hand with a person's declining social status. Smoking is turning into a growing threat in some countries, despite an overall decrease in the number of smokers; the reason being that cigarette consumption per smoker is simultaneously on the rise. Nonetheless, the general downward trend in smoking may have an impact on reducing smoking among socially vulnerable groups [6, 14, 16].
Early studies focused almost entirely on the decreased life expectancy of smokers, while the temporary and changing processes that are part of cigarette smoking (initiation, continuation, cessation) received little attention from the scientific viewpoint [6, 16, 19]. Even if an individual starts to smoke during adolescence (initiation) [6, 20, 21], the progress of the smoking career as the person ages, which is affected by social differences, is still open to variations. In the interim, socio-economic status has been identified as a key indicator for the smoking career (i.e. continuation or cessation of smoking). Criteria for such smoking behavior have not yet been established, despite investigation into problems of the individuals’ environment and health risks [22].
Research into the influence of social status on the different phases of cigarette smoking [23] showed that negative social status was significantly related to an increased risk of initiation, a greater probability of progressing to habitual cigarette smoking and a decline in willpower to stop smoking. Moreover, the poor social and educational status of a child (equivalent to the parents’ status) correlates with all three phases of cigarette use (initiation, habitual smoking, smoking cessation).
A low socio-economic status in the first 7 years of a child's life represents a high risk for early smoking initiation, and people with this status displayed the least interest in smoking cessation [24]. Although the Whitehall II study [25] of British employees revealed that paternal smoking status had a more significant impact on the smoking behavior of girls than the socio-economic status of the family, this theory has been disputed [26, 27].
Where the smoking behavior of adolescents was analyzed in relation to their parents’ educational level, the parental profession was important in terms of the onset of smoking (initiation phase). Maternal rearing of the child allowed identification of the progress to habitual smoking and household poverty during childhood made it possible to predict the development from smoking initiation to cessation [28].
Social processes express themselves in a variety of forms. How a child is raised is reflected in the intellectual environment of the child, whereas the parent's profession and income determine the material foundation of a child's life [29], hypotheses that must be confirmed through additional research [23]. The inadequate material foundations are supposed to explain the poor social status of the parents and the initiation of smoking, while the negative social conditions foster the habitual use of cigarettes [30].
When comparing the socio-economic status and upbringing of the interviewee, but not the profession, both parameters correlate with habitual cigarette smoking and reduced efforts to stop smoking. Some investigators reported the status of education attained in adulthood to be more important than profession or income [16], while others found all three factors, educational status, profession and income, were equally important in terms of the risk of smoking initiation [26]. The recent PRIME study pointed in the same direction for coronary disease, indicating that socially disadvantaged groups experience these diseases more frequently than individuals with higher professional qualifications [31].
Unemployment and smoking
The worldwide economic crisis of the 1920s and the current crisis linked to worldwide globalization that started in the 1990s caused widespread unemployment in many industrialized nations. The lifestyle adaptation driven by the conditions of unemployment that goes hand in hand with increased abuse of alcohol and cigarettes are part of the negative consequences [32, 33]. On one hand, this kind of development is influenced by risks that arise in the social environment, by the individual risk-taking behavior, and on the other hand by learning processes linked to dealing with risks. Consequently, in the USA increased tobacco consumption has decreased male life expectancy [34].
This lack of healthy behavior patterns may no longer be considered merely a risk factor, but must be regarded as a way of life and lifestyle. Consequently health-related behavior is no longer only a medical problem, but also a cultural, psychological and sociological issue. The rating of the importance of health by the individual is a deciding factor that sometimes has self-destructive consequences. Figure 1 [35] shows the relationship between employed and unemployed status (shown as a relative risk calculated using logistic regression). A higher risk for depression, increased consumption of psychotropic drugs and substantial tobacco or alcohol consumption were observed in 586 40–59-year old unemployed men [36]. Actual unemployment was preceded by increased smoking [odds ratio (OR) 2.59; 1.42–4.69] and high levels of alcohol consumption (OR 2.11; 1.05–4.25) accompanied by simultaneous physical problems (OR 7.75; 1.51–39.93). The unemployed men were controlled by a vicious circle; stress preceded the loss of the job, which in turn compounded the stress symptoms even more [36].
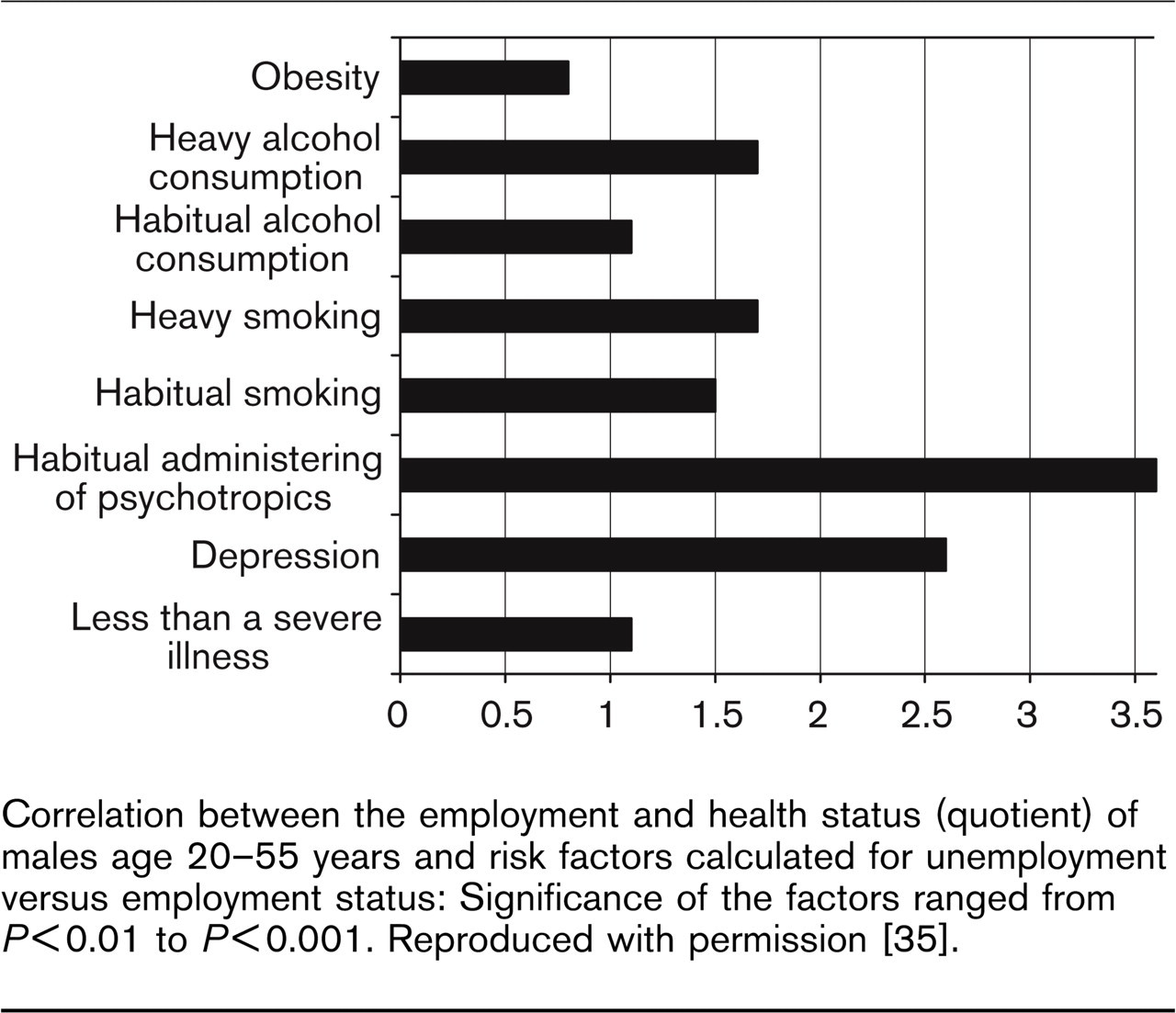
Correlation between the employment and health status (quotient) of males age 20–55 years and risk factors calculated for unemployment versus employment status: Significance of the factors ranged from P>0.01 to P >0.001. Reproduced with permission [35].
A Swedish study [37] that was carried out over a 14-year period, and which followed 1044 pupils who were included at the age of 16 years, determined that long-term unemployment in subsequent years led to increased cigarette consumption in addition to psychological problems. The CARDIA study, which involved 5115 young people (aged 18–30), also found that the unemployed smoked substantially more than those who were employed (adjusted OR 1.5; 1.0–2.1) [38].
A 20-year survey of Finnish adults found that individuals who had little or no scholastic education made up the largest group of smokers [39], and that women with the lowest level of qualification stood out in particular. There is also evidence that being a smoker and the consumption of large amounts of alcohol increases the mortality rate of the temporarily unemployed [40]. Moreover, if young people become unemployed their cigarette consumption increases [41, 42].
Socially disadvantaged children and smoking
The conditions of the home environment have a substantial impact on children who consciously or subconsciously mimic the habits of their parents. Parental smoking has an impact on the family's household income and on the distribution of financial resources as well as on the children's upbringing and their career choices [43, 44]. In socially weak groups or families, the prevalence of smoking is extremely high (60%), and these smokers spend approximately 15% of their income on cigarettes [45].
Worldwide studies show that children who grow up in low-income families are also far more willing to spend money on tobacco products than those who grow up in more financially prosperous families [46]. For example, in Bangladesh more than 100 000 children are ‘sacrificed’ for parental smoking habits every year [47], and in New Zealand parents in poor families are 2.6 times more likely to smoke than better-off parents [44]; poor families spend 9.1% of their disposable household budget on smoking. Children who grow up in such families are highly likely to become smokers themselves [48].
Based on our own survey of 1857 students, the percentage of smokers is almost twice as high at German basic education schools (Hauptschulen, where children will finish eight courses) than it is at standard (Realschulen, where children will finish 10 courses) or advanced educational level schools (Gymnasien, where children will finish 12 courses) (Fig. 2). Moreover, the percentage of addicted smokers at Hauptschulen also exceeded those at both of the other school types (OR 2.9; 2.1–4.1). The risk of becoming a habitual smoker as a child was increased sevenfold with extended exposure to smoke in smoke-filled residences (>3 h daily; OR 7.0; 5.3–9.2), and almost tripled by parental smoking (OR 2.9; 2.3–3.6 or 1.9; 1.5–2.4 for maternal or paternal smoking, respectively) [49].
The nascent smoker develops during adolescence and by the age of 16 it is possible to predict the relative risk for an individual being a habitual smoker by the age of 30 (Fig. 3) [50]. In this context, in addition to smoking, the simultaneous consumption of alcohol plays an important role for starting a career as a cigarette smoker.
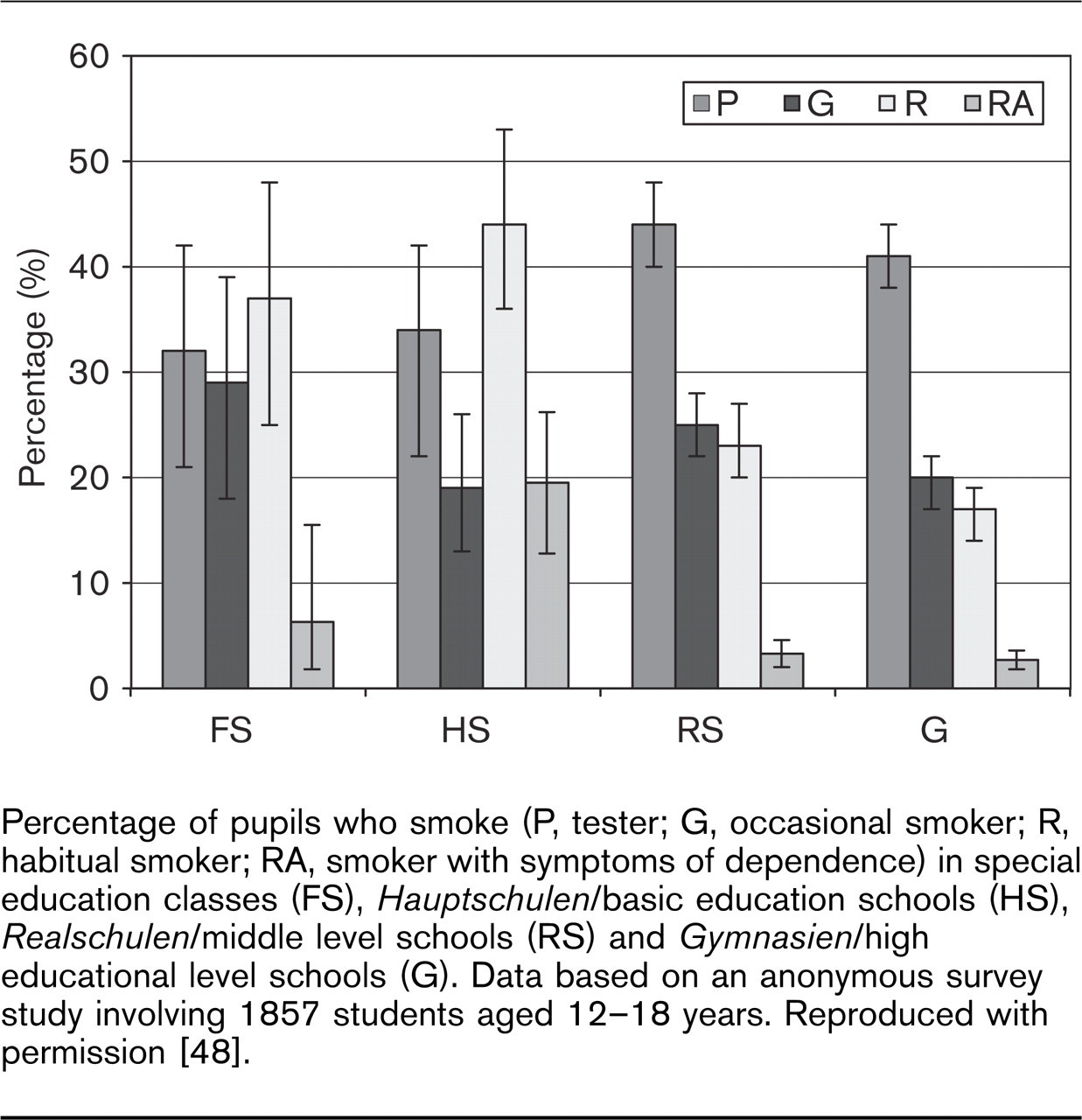
Percentage of pupils who smoke (P, tester; G, occasional smoker; R, habitual smoker; RA, smoker with symptoms of dependence) in special education classes (FS), Hauptschulen/basic education schools (HS), Realschulen/middle level schools (RS) and Gymnasien/high educational level schools (G). Data based on an anonymous survey study involving 1857 students aged 12–18 years. Reproduced with permission [48].
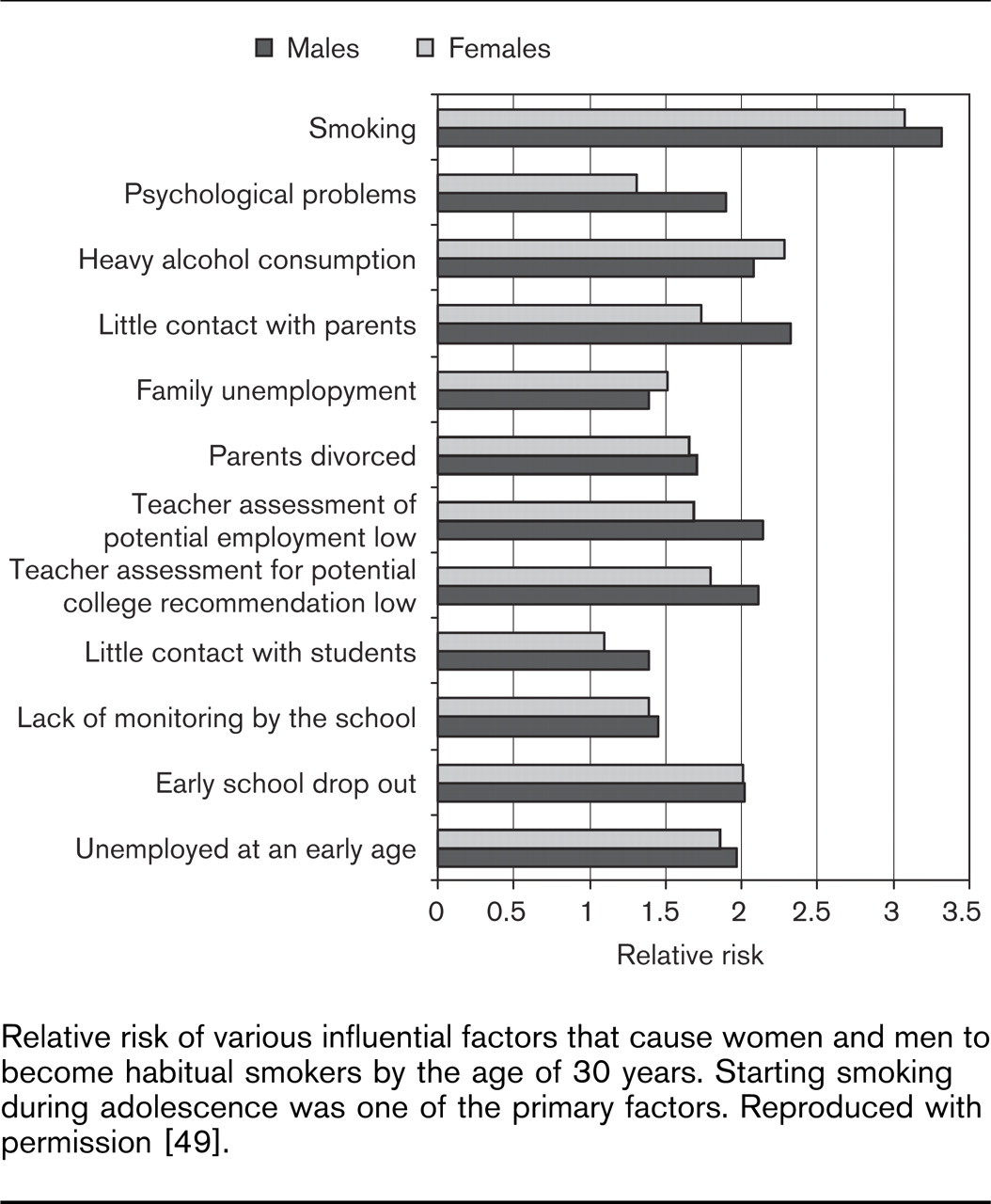
Relative risk of various influential factors that cause women and men to become habitual smokers by the age of 30 years. Starting smoking during adolescence was one of the primary factors. Reproduced with permission [49].
Women, pregnancy and smoking
Even though highly restrictive policies in some countries, led by the USA, have resulted in a decline in the overall number of smokers in the past 30 years, this decline does not apply to all social segments of the population [45]. If the income status of the US population is divided into four segments, it is apparent that the prevalence of smoking among single female smokers in the lowest income bracket far exceeds that among women smokers in all other segments.
Several studies have researched the behavior of women smokers and their handling of their household budgets; in general, the probability of smoking increases with increasing expenditure for living, medical support, rent and so forth. One report on the economic causes of smoking noted that prevalence increased in parallel with rising income, but dropped along with the income bracket [51]. Single women typically ‘sacrifice’ about 21% of their income to purchase cigarettes [45]. In this context, healthy female smokers were more willing to stop smoking than those in poor health [52]. Moreover, it was more difficult to convince female heavy smokers to stop smoking successfully than ‘lighter’ female smokers [52]. In households with growing numbers of children, however, a positive turnaround in the attitude toward smoking was observed [53].
Life cycle behavior patterns that reached their plateau at the age of 31 were observed in relation to smoking: women who are more educated and who work are less likely to smoke [54]. The presence of a man in the household reduced the likelihood of smoking [53], and smoking is less common among married individuals than singles. Investigation of the level of schooling and its correlation to smoking [55] showed that individual differences play a role, especially in terms of discussion of health issues during childhood and the consequent awareness of smoking-related problems among adolescents [56]. Poorer, less educated and younger people were less concerned with the future costs of smoking than more affluent, better educated adolescents [57, 58]. The less educated focused exclusively on the current price of tobacco products, while the better educated paid more attention to future health problems they might encounter. These findings were also the basis of claims that increases in cigarette price were measures to reduce cigarette consumption [58].
Consecutive years of uninterrupted smoking naturally fostered the ‘experiences in dealing with addiction in younger female smokers’ [58], whereas the smoking habit was rarely picked up over the age of 23 [59]. Among girls who dropped out of school before the age of 16 years, the desire to smoke increased simultaneously.
Another factor, in addition to lack of education and professional qualifications, is lack of understanding of information about the dangers of smoking [55, 60]. In the poorly educated, understanding of these dangers was less good than in the better educated. There is no plausible explanation for the fact that people pick up the habit of smoking regardless of budget.
Reduced birth weight is the most crucial morbidity and mortality factor for children of smoking mothers in the Western hemisphere [61]. A comprehensive epidemiological study [62] performed in Germany showed that neonate body weight declines according to the number of cigarettes per day the mother smokes during the pregnancy.
Several studies over the past 20 years showed that reduced birth weights were influenced by a low level of education (OR 1.38; 0.71–2.69) [43, 63–65] and by smoking during pregnancy (OR 1.98; 1.35–2.91) (compare Table 1) [43, 63–65]. For early deliveries (>37 weeks) smoking was determined to be the only independent factor [66, 67]. Furthermore, in the USA, about one-fifth of unmarried and unemployed pregnant women suffered from previously untreated depression, came from negative social backgrounds, had problems with alcohol abuse and smoked [68].
Correlation between low birth weight of infants born to female smokers and various influential factors
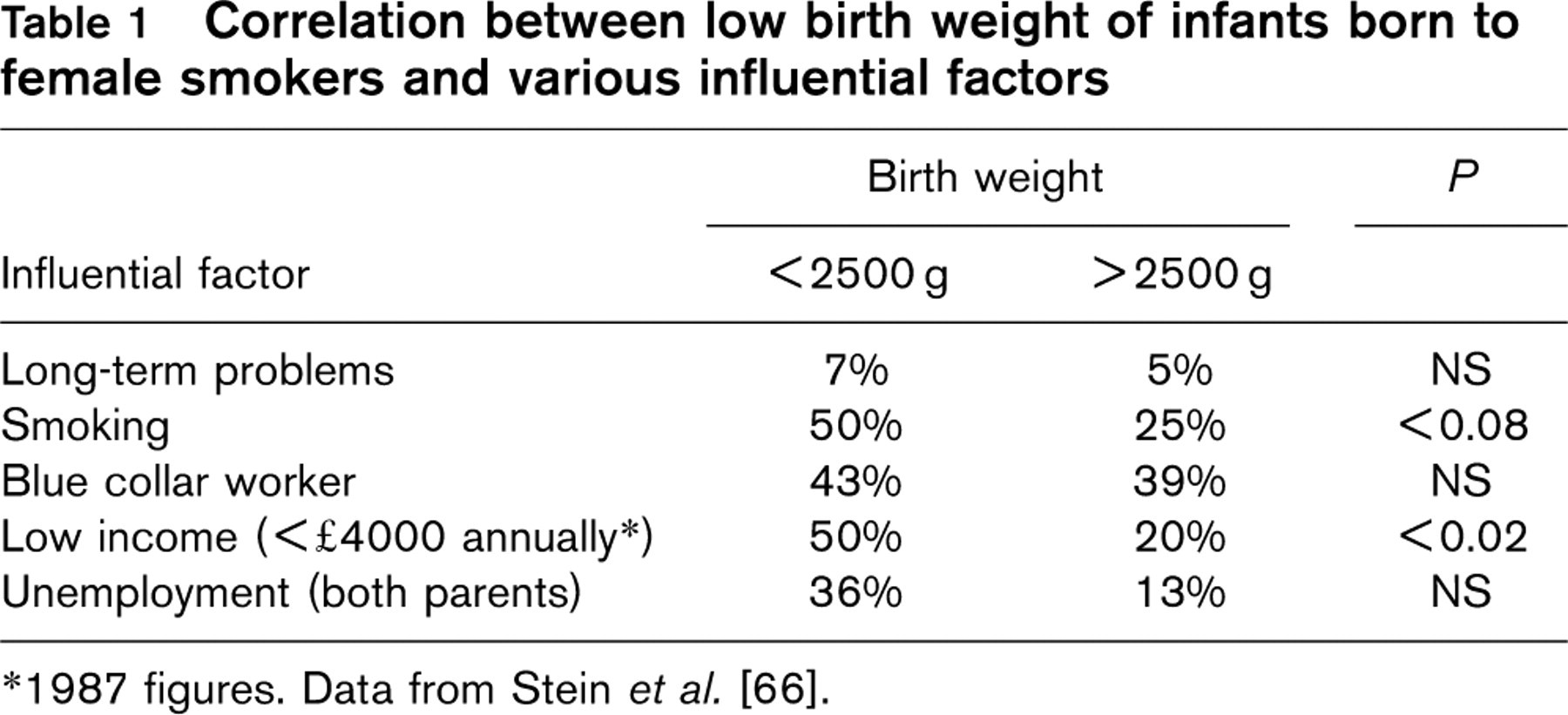
1987 figures. Data from Stein et al. [66].
Overall, low socio-economic status is a primary causal factor for several healthcare problems in pregnant women, which also harm the fetus.
Conclusions with respect to current health policies
As far as future funding of the health and social security systems in industrial nations is concerned, four major preventable health hazards play a deciding and limiting role: tobacco smoking, excessive alcohol consumption, obesity, and lack of exercise. The consequences of regular cigarette consumption, particularly in the early part of life, will advance the appearance of tobacco-related diseases by approximately one decade, which means that appropriate medical treatment will have to be financed for 10 more years than in the past. In the foreseeable future this will lead to the collapse of the healthcare system as we know it, despite medical progress. It remains to be seen to what extent the ‘solidarity community’ (of the social health insurance system beneficiaries in Germany) is prepared to continue to finance these immense costs in the future, especially since the majority of the population is substantially not involved in the self-inflicted development of preventable diseases. In discussing the funding for the costs of treating tobacco-related illnesses, there are limits to applying the ‘solidarity pact’ principles.
The anti-smoking movement, as a secondary preventative measure in particular, does not currently receive effective support from either politicians or insurance providers. Smokers also display different levels of ability to stop smoking. The data summarized in Table 2 show that professional and better educated individuals have a higher chance of stopping smoking than their socially weaker and less qualified counterparts [69]. It is difficult to estimate whether sanction-oriented anti-smoking policies would deliver initial results as early as within the first 2–3 years of implementation. It is equally complex to draw up a concept for a socially specific and anti-discriminatory, anti-tobacco strategy [70].
Smoking cessation depending on social class: indication of odds ratios for the likelihood of smoking cessation within 5 years
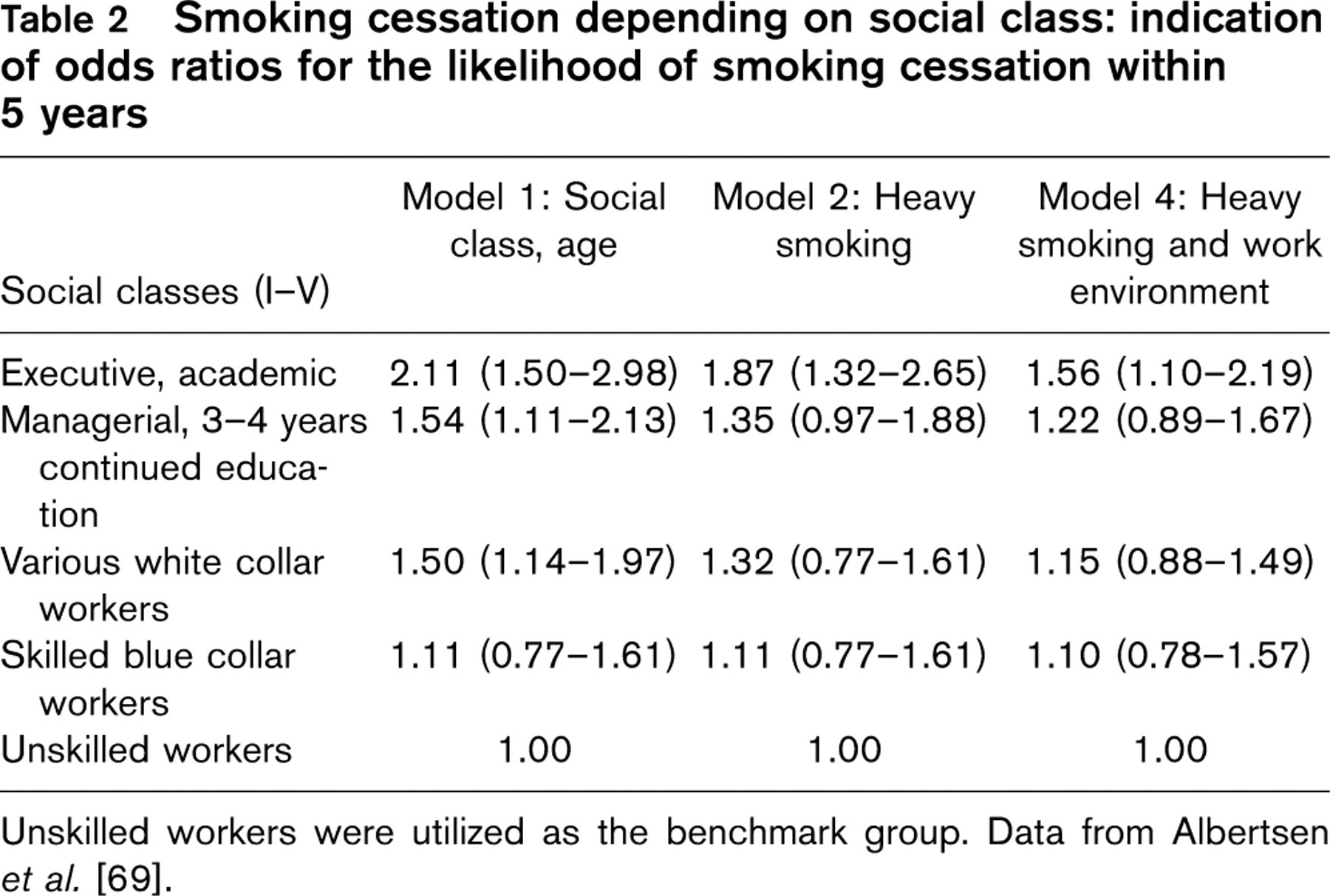
Unskilled workers were utilized as the benchmark group. Data from Albertsen et al. [69].
The following issues should be reconsidered by politicians responsible for health. The tobacco industry, which is constantly conquering new markets, must be more stringently regulated by policy and government sanctions than in the past, including advertising bans, banning the sale of tobacco to teenagers and sales of cigarettes in tobacco shops. The continual increase in tobacco taxes should be successfully implemented with the objective of reducing the number of smokers in Germany. The question arises as to how far the costs for the treatment of the subsequent illnesses of socially disadvantaged smokers (children, single parents, women) can be imposed on these people. In the interest of the stability of the health system it would have to be striven. Smokers must be made aware of the ‘self-destructive’ consequences of continued smoking on future health provisions through media information campaigns (television, radio, press), along with parallel offers of treatment programs for smokers. Health insurance companies should adopt a more assertive policy in the face of smokers who do not try to quit because they think that medical services, to a large extent, are funded from tobacco taxes and also that smoking is a part of personal liberty. In future, the burden for addressing these problems can no longer rest solely on the shoulders of the solidarity community.