
Abstract
Objective
Background
Methods
Results
Conclusions
Keywords
Introduction
The global prevalence of diabetes mellitus (DM) in the adult population is predicted to increase from 4.0% in 1995 to 5.4% in 2025 [1] and exceed 7% by the year 2050 [2]. The rapidly increasing prevalence of type 2 diabetes strongly relates to coronary artery disease (CAD) since DM is one of the major contributors [3].
Considering that diabetes is associated with an at least doubled incidence of cardiovascular events and a two-to fourfold risk of cardiovascular death, this perspective is indeed threatening for the health of the general population [4, 5]. With this evidence there is little doubt that cardiovascular risk factors should be treated aggressively in patients with diabetes. Since the presence of diabetes has been found to be associated with as high a risk for myocardial infarction as for non-diabetic patients with a previous myocardial infarction, it has been recommended that patients with diabetes, in a preventive perspective, should be managed as if they had established coronary heart disease [6, 7]. In contrast to the steadily declining age-adjusted mortality among patients without diabetes, trends were reported in a recent national survey [8] suggesting that patients with diabetes and coronary artery disease benefit from modern therapeutic innovations to a considerably lesser extent, or not at all. One reason may be that despite proven efficacy of evidence-based treatment even in diabetic patients, as reflected by the United Kingdom Prospective Diabetes Study (UKPDS) [9], (Heart Outcomes Prevention Evaluation) MICRO-HOPE [10], the Heart Protection Study (HPS) [11], the Collaborative Atorvastatin Diabetes Study (CARDS) [12], the Hypertension Optimal Treatment (HOT) [13] and Diabetes Mellitus Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) [14] studies, such therapy has been less often used than in patients without concomitant diabetes [15–18].
The main aim of this report from the Euro Heart Survey on diabetes and the heart was to assess clinical practice in relation to existing guidelines and identify opportunities to improve patient management, with special attention to the presence or absence of DM. The report focuses on the management strategies used for patients admitted with acute coronary syndromes (ACS) and the secondary prevention of confirmed CAD.
Methods
The Diabetes and Heart Survey is a multi-centre prospective observational study involving 110 centres in 25 European Society of Cardiology (ESC) member countries, as reported in detail elsewhere [19]. Each centre was asked to recruit at least 20 patients over 2-12 weeks. Consecutive patients of more than 18 years of age were screened for a diagnosis of coronary artery disease (CAD) when referred to a cardiologist while admitted to the hospital wards or visiting the outpatient clinic. On the basis of the clinical presentation at enrolment, patients were ascribed to one of two cohorts: acute or stable. Of the total population of 4961 patients with CAD 2107 (42%) belonged to the acute and 2854 (58%) to the stable cohort. The prevalence of prior DM was 31% in the acute and 30% in the stable subgroup. The reasons for consultation are shown in Table 1. All patients enrolled were assessed, investigated and treated at the discretion of the physicians in charge and according to the usual institutional practice of the centres. In the acute cohort, in 1872 (89%) patients the reason was ACS, defined following the Joint ESC/ACC definitions [20]. Out of the 235 (11%) patients that did not receive a preliminary diagnosis at admission of ACS, only 84 (36%) patients did not have a final diagnosis of ACS. To clearly define the management of acute CAD, these 235 patients, 118 (50%) with DM, were not included. Accordingly, the numbers in this report may differ somewhat from previously published data from the survey.
Reason for consultation in the acute and stable patient cohorts
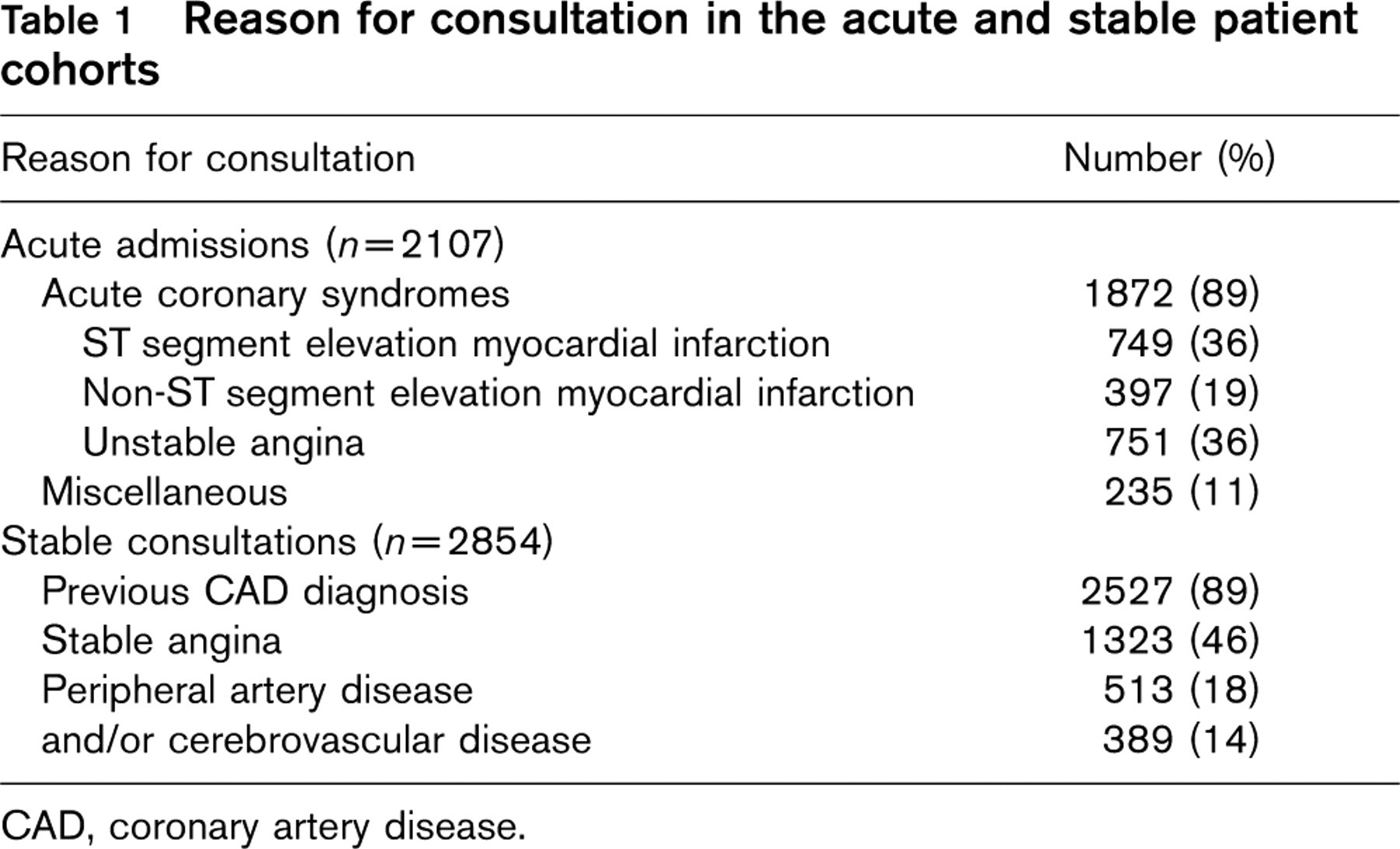
CAD, coronary artery disease.
Definitions
The presence of diabetes was recognized if the diagnosis was established prior to enrolment according to the World Health Organization (WHO) classification [21], reported in medical records, declared directly by the patient or revealed by the use of glucose-lowering drugs.
The use of diagnostic procedures, interventions and pharmacological treatment was also analysed with respect to the clinical status within the ACS subgroup with ST segment elevation myocardial infarction (STEMI, n = 749). Patients were allocated to the STEMI subgroup if presenting with a ST segment elevation in ≥ 2 adjacent electrocardiographic leads (≥ 0.2 mV in leads V1-V3 or ≥ 0.1 mV in other leads) at admission.
Drug treatment was recorded as used prior to enrolment and as recommended after the index consultation. In the case of hospitalized patients, intensive treatment with intravenously (i.v.) administered drugs was also reported. Diagnostic and revascularization procedures [percutaneous coronary intervention (PCI) or coronary artery bypass (CABG)] were reported as performed during consultation or scheduled in the next few months.
Measurements
The case record form included measurements of blood glucose at enrolment (fasting or random). Glucose concentrations measured according to local routines were converted to venous plasma glucose by the conversion factors proposed by the European Diabetes Epidemiology Group [19] and expressed in mmol/l. Haemoglobin A1c (HbA1c) was analysed by high-performance liquid chromatography in a core laboratory (Department of Clinical Chemistry, Karolinska University Hospital, Solna, Sweden) as previously reported [19] with a normal limit < 5.2%. The results obtained with this method can be compared and recalculated to the International Federation of Clinical Chemistry (IFCC) and Diabetes Control and Complications Trial (DCCT) standard, using the respective converting formulas [22]. Lipid parameters, including total, high-density lipoprotein (HDL), low-density lipoprotein (LDL) cholesterol and triglycerides, were analysed locally from fasting blood samples at the time of enrolment.
Blood pressure was measured, following 5 min of sitting rest, to the nearest 2 mmHg; recommendations were to take two measurements and register an average.
Clinical targets
The lipid and blood pressure targets for secondary preventive measures in the stable cohort of patients refer to those recommended in the ESC guidelines available at the time of patient recruitment [23]. The lack of clear recommendations for patients with stable CAD and DM in the ESC 1998 guidelines, regarding the targets for fasting blood glucose (a range of values is indicated only for DM type 1) and HbA1c levels (recommended between 6.2 and 7.5%) is the reason for referring to the American Diabetes Association (ADA) recommendations from 2002 [24]. The clinical targets referred to are presented in Table 2.
Statistical methods
Continuous variables, including age, body mass index (BMI) and waist circumference, are expressed as medians with lower and upper quartiles (Q1, Q3), and categorical parameters as percentages of the respective strata. The categorical variables were compared between patient strata by means of the maximum-likelihood chi squared test.
In order to control for confounding variables that may have influenced the choice of medication, diagnostic procedures or interventions (performed or planned), multiple logistic regression analyses were performed, based on clinically relevant differences in the baseline characteristics between patients with and without diabetes (see Fig. 3b). The best subset models were run applying odds ratio (OR) likelihood scores. Contraindication to the use of specific medication had a similar distribution in relation to DM status, and was regarded as missing data in the multiple logistic regression analysis.
The daily dosages at enrolment and discharge were compared in relation to diabetes status with the Mann-Whitney unpaired rank sum test.
All statistical analyses were performed using STATISTICA (StatSoft Inc, Tulsa, Oklahoma, USA; version 7.1).
Ethical consideration
The National Survey co-ordinators took the responsibility for assuring compliance with the ethical requirements in each country. The patients were enrolled following an oral and/or written informed consent with respect to the local rules, and were informed about the follow-up after 1 year.
Results
The ACS cohort
Baseline characteristics of the ACS group are presented in Table 3. The diabetic patients were older with higher prevalence of hypertension, hyperlipidaemia and previously established cardiovascular diseases and prior interventions (PCI or CABG). Treatment prior to the index hospital admission and at hospital discharge is shown in Fig. 1. At admission, diabetic patients were more often treated with aspirin, renin-angiotensin-aldosterone system (RAA) antagonists, statins and a combination of three blood pressure-lowering agents than the non-DM patients (7 versus 4%, P = 0.01). However, at discharge, they less often received aspirin, beta-blockers and statins than their non-DM counterparts. In the DM patients, drug therapy more often remained unchanged from that at hospital admission than in the non-DM group (11 versus 7%; P < 0.01).
Clinical targets for lipid, blood pressure and glucometabolic status according to European Society of Cardiology guidelines available when the recruitment period of the survey started [21]
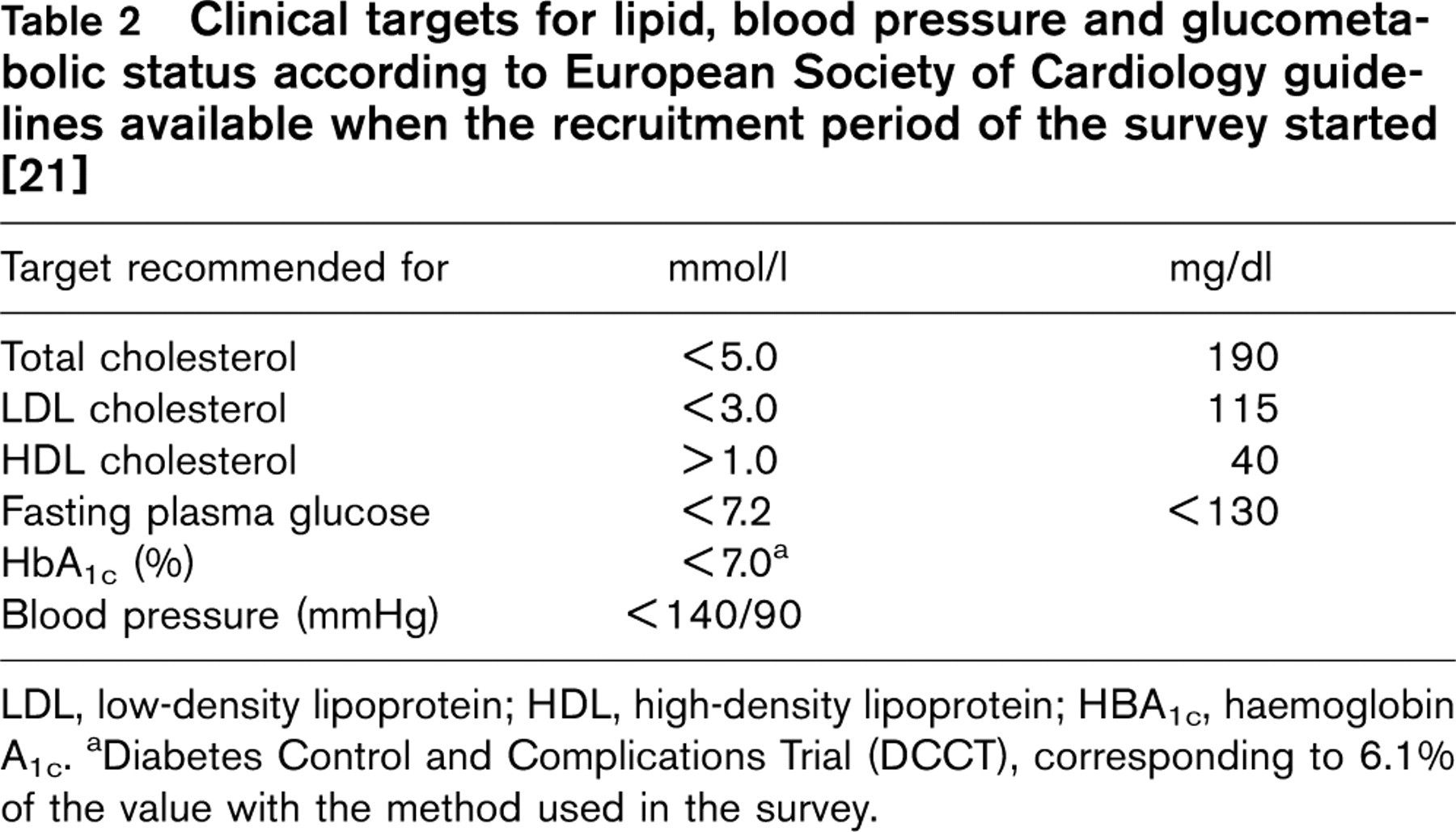
LDL, low-density lipoprotein; HDL, high-density lipoprotein; HBA1c, haemoglobin A1c. aDiabetes Control and Complications Trial (DCCT), corresponding to 6.1% of the value with the method used in the survey.
Clinical characteristics at admission in the acute coronary syndrome (ACS) cohort with and without diabetes mellitus (data presented as count and percentage unless stated otherwise)
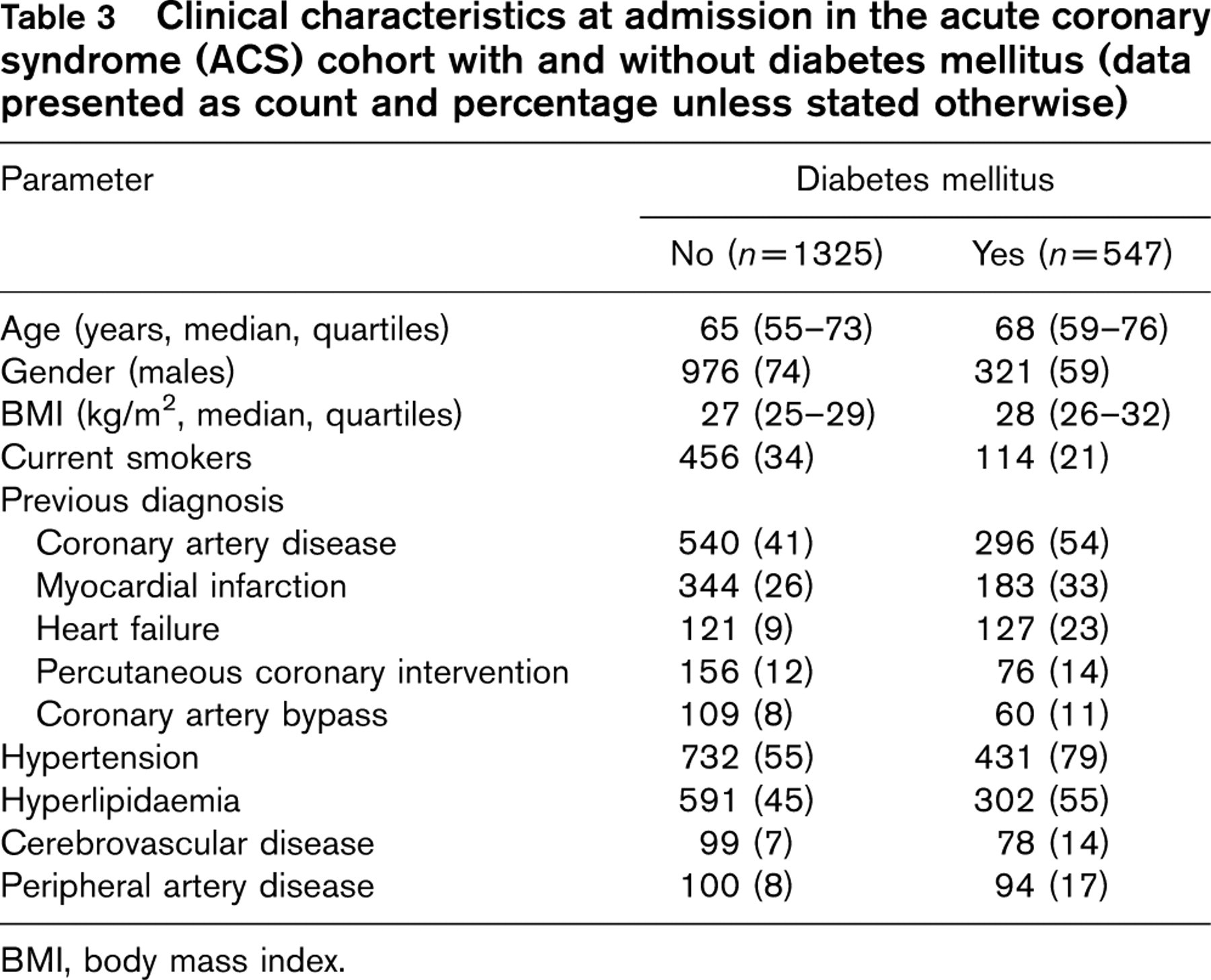
BMI, body mass index.
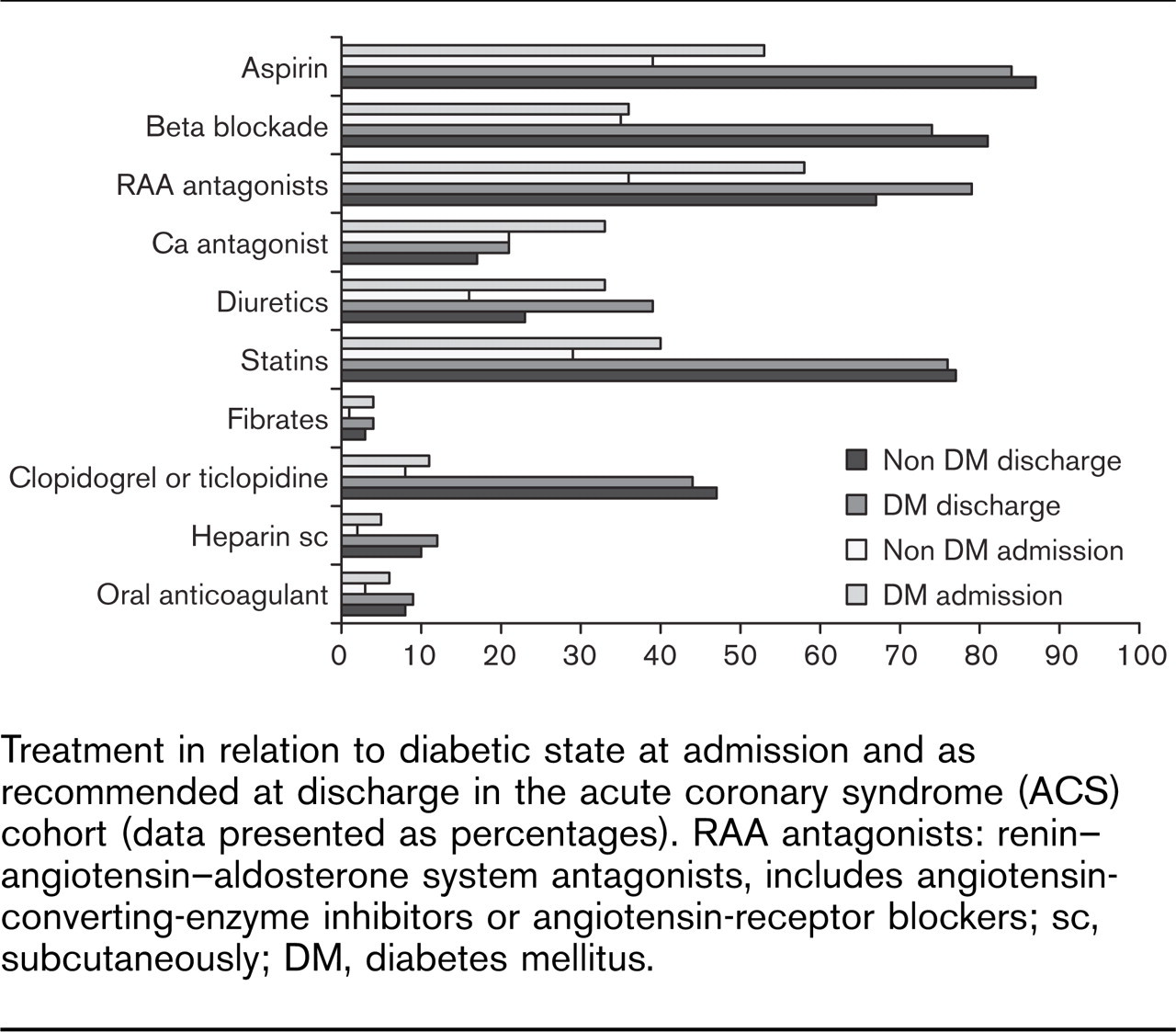
Treatment in relation to diabetic state at admission and as recommended at discharge in the acute coronary syndrome (ACS) cohort (data presented as percentages). RAA antagonists: renin–angiotensin–aldosterone system antagonists, includes angiotensin-converting-enzyme inhibitors or angiotensin-receptor blockers; sc, subcutaneously; DM, diabetes mellitus.
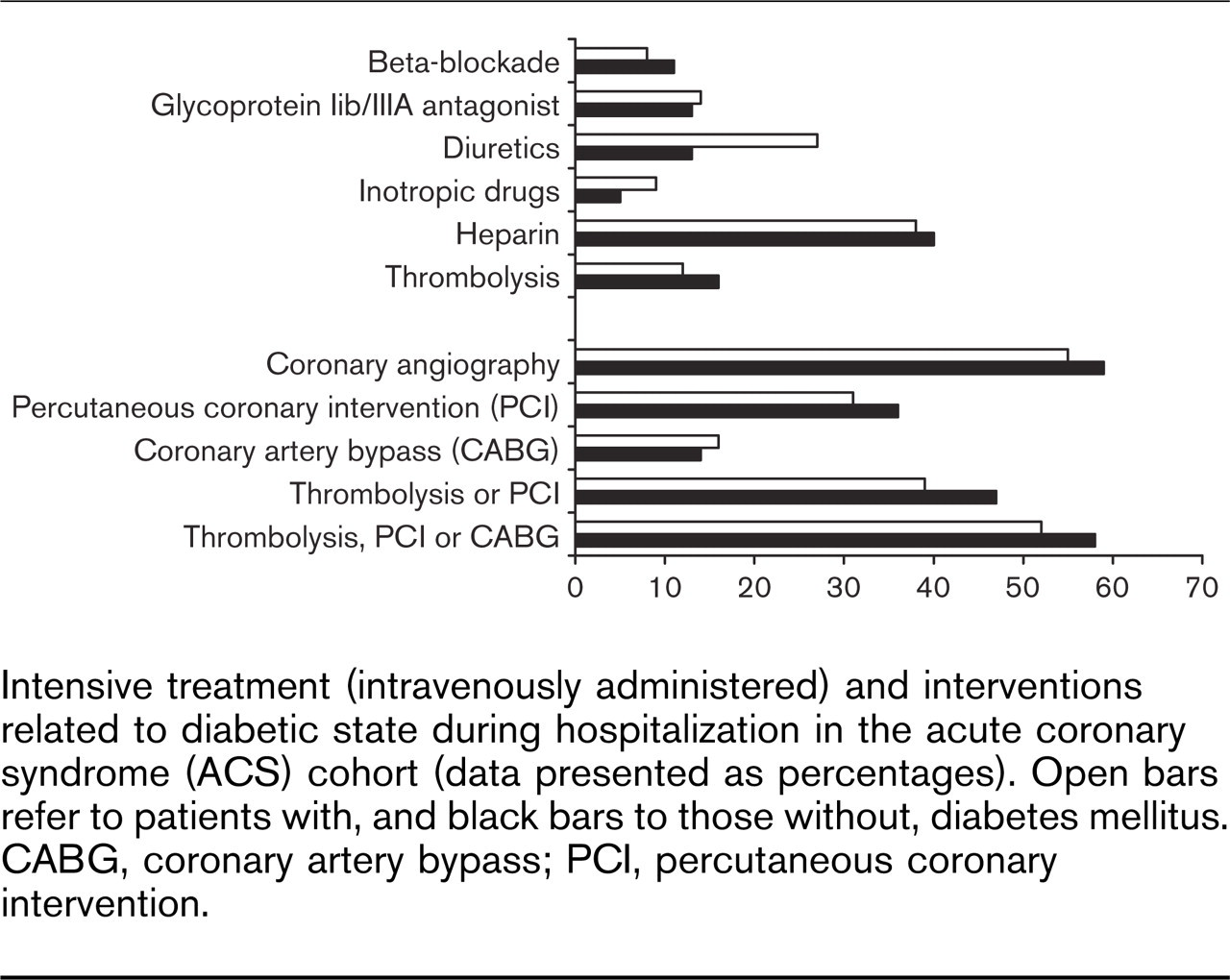
Intensive treatment (intravenously administered) and interventions related to diabetic state during hospitalization in the acute coronary syndrome (ACS) cohort (data presented as percentages). Open bars refer to patients with, and black bars to those without, diabetes mellitus. CABG, coronary artery bypass; PCI, percutaneous coronary intervention.
Acute treatment during hospitalization including coronary interventions is detailed in Fig. 2. Patients with DM were less often subjected to thrombolysis, coronary angiography and angioplasty and received inotropic drugs and diuretics more often than those free from DM. When analysing the STEMI subgroup separately, there were no significant differences in the use of interventions. Even in this subgroup, patients with DM less frequently received thrombolysis than those without DM (29 versus 37%; P =0.03).
Revascularization as a combination of thrombolysis or coronary angioplasty was less commonly applied in patients with DM in the entire ACS group as well as in the STEMI subgroup (60 versus 68%; P = 0.04).
The results of the multiple logistic regression analysis with and without correction for potential confounders (age, gender, previously known CAD, heart failure, hypertension, cerebrovascular disease, peripheral artery disease and diabetes; when analysing the use of statins added correction for total, HDL and LDL cholesterol; when considering PCI and CABG corrected also for previous PCI or CABG) are shown in Fig. 3. The presence of DM had a smaller impact on the choice of treatment and use of interventions than other baseline characteristics. The diabetic state itself influenced only the recommendation at discharge for RAA antagonists [OR 1.33; 95% confidence interval (CI) 1.03–1.71; P =0.03].
The case record form included daily dosages of the most commonly used drugs (Table 4). No difference (P > 0.05 performing Mann-Whitney U test, data not shown) emerged in patients with and without DM for beta-blockers, RAA antagonists, calcium antagonists and statins. The dosages of the drugs used at admission were not increased due to the exacerbation causing the acute admission, both in patients with and without DM. Following a multiple logistic regression analysis correcting for potential confounders, prior diabetes did not impact the use of drugs.
The stable cohort
In the stable cohort of patients 1894 (66%) were on statin treatment at admission. Of these patients, 55% of those with and 47% of those without DM had total cholesterol levels above recommended targets; and 57% of those with and 51% of those without DM had LDL cholesterol levels above recommended targets. Regardless of the diabetic state, more than one-third (35%) of patients had HDL cholesterol below target. In patients on treatment, blood lipids were higher among those with DM: total cholesterol 5.2 (4.3–6.2) versus 4.9 (4.2–5.9; P < 0.01) mmol/l and LDL cholesterol 3.3 (2.5–4.4) versus 3.1 (2.4–3.9; P < 0.01) mmol/l. Even after the consultation and despite cholesterol values above recommended target, the recommended dosages of statins were not increased similarly in patients with and without DM.
Of the stable cohort 2127 (75%) patients were on blood pressure-lowering agents at admission. Approximately 30% of the patients had a blood pressure above the guideline recommendations, regardless of the combination of different drugs and diabetic state (patients with and without DM treated with beta-blockers 29 and 27%; RAA antagonists 33 and 28%; both these classes 31 and 29%; both previous classes and diuretics 33 and 36%, respectively). The dosages of blood pressure-lowering agents prescribed after the consultation were not increased despite blood pressure levels exceeding recommended targets and regardless of the diabetic state.
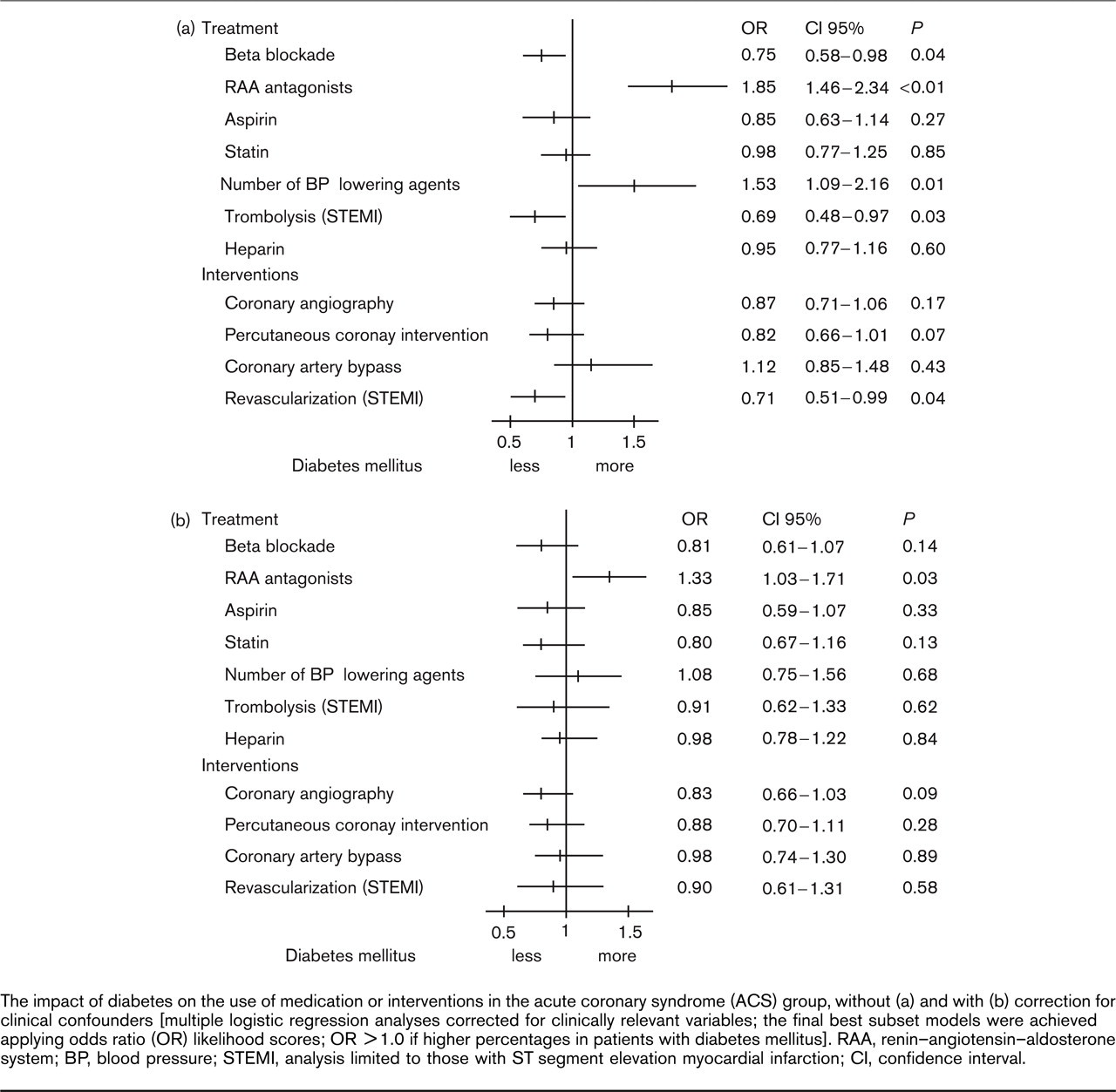
The impact of diabetes on the use of medication or interventions in the acute coronary syndrome (ACS) group, without (a) and with (b) correction for clinical confounders [multiple logistic regression analyses corrected for clinically relevant variables; the final best subset models were achieved applying odds ratio (OR) likelihood scores; OR > 1.0 if higher percentages in patients with diabetes mellitus]. RAA, renin–angiotensin–aldosterone system; BP, blood pressure; STEMI, analysis limited to those with ST segment elevation myocardial infarction; CI, confidence interval.
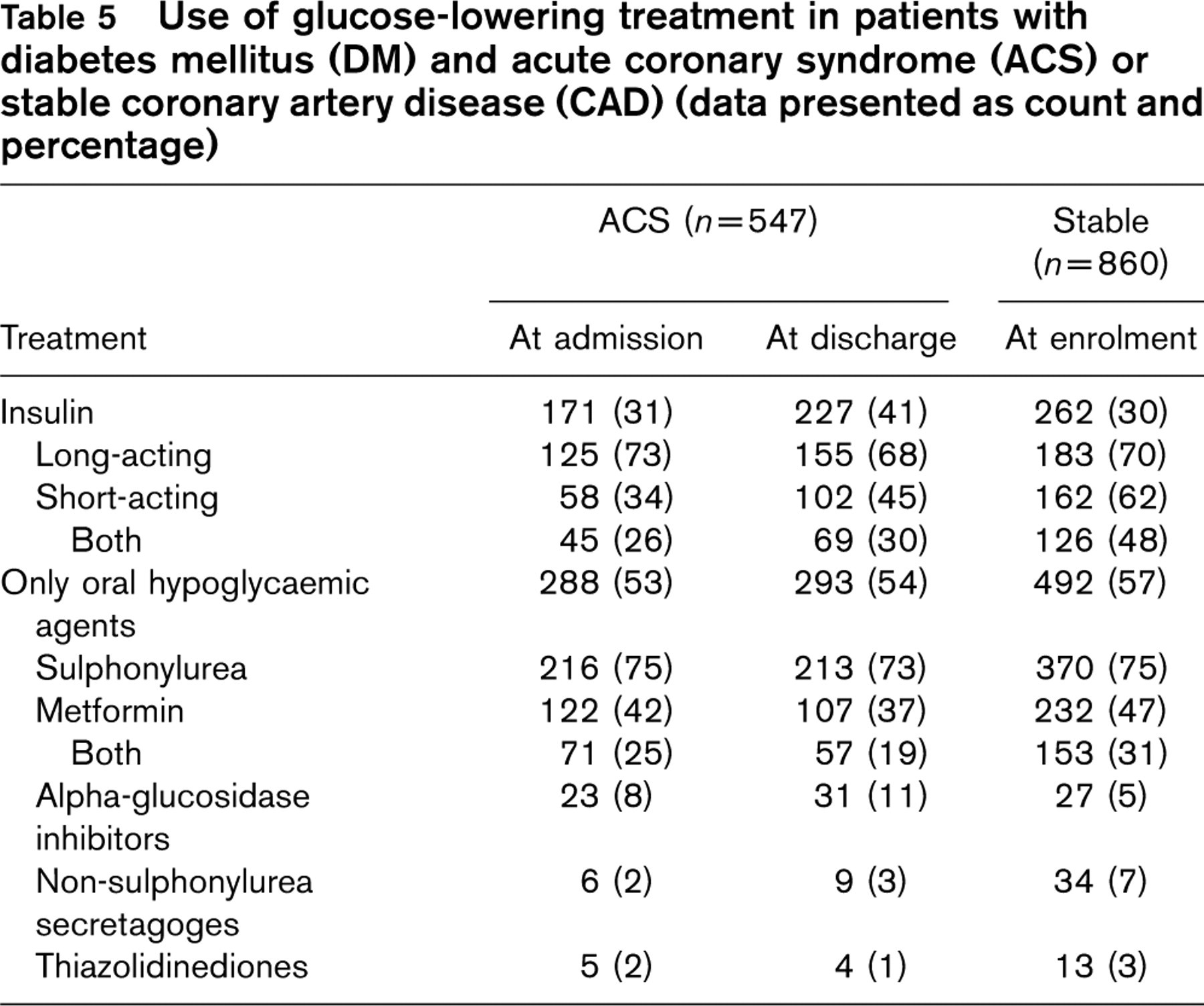
Glucose-lowering treatment in patients with DM and ACS or stable CAD is summarized in Table 5. Out of the 860 (30%) patients with DM and stable CAD, about half of patients using subcutaneous insulin (n = 262; 30%) or oral glucose-lowering agents (n = 492; 57%) had a fasting blood glucose (FBG) above the target and, especially those on insulin, had a considerably higher HbA1c level (Fig. 4). Regardless of the unsatisfactory glucose control, the total dose of insulin was not increased after the consultation (e.g. from 43 to 45 median daily units in patients with elevated FBG and from 42 to 42 in those with a high HbA1c).
Discussion
This survey revealed that patients with DM admitted for CAD across Europe receive less acute in-hospital management compared to their non-diabetic counterparts. These differences are, however, largely explained by differences in baseline characteristics. Regarding secondary prevention, patients with DM and CAD are poorly treated and, considering their high cardiovascular risk, unsatisfactorily managed. Moreover, the DM patients are poorly handled as regards their glucometabolic situation. Finally, the propensity to improve treatment in connection with a hospitalization or outpatient consultation was surprisingly low.
The use of drugs and their daily dosages at admission and discharge for the acute coronary syndrome (ACS) group in relation to diabetes mellitus (DM) (data presented in percentage, dosages in median and quartiles of mg/day)
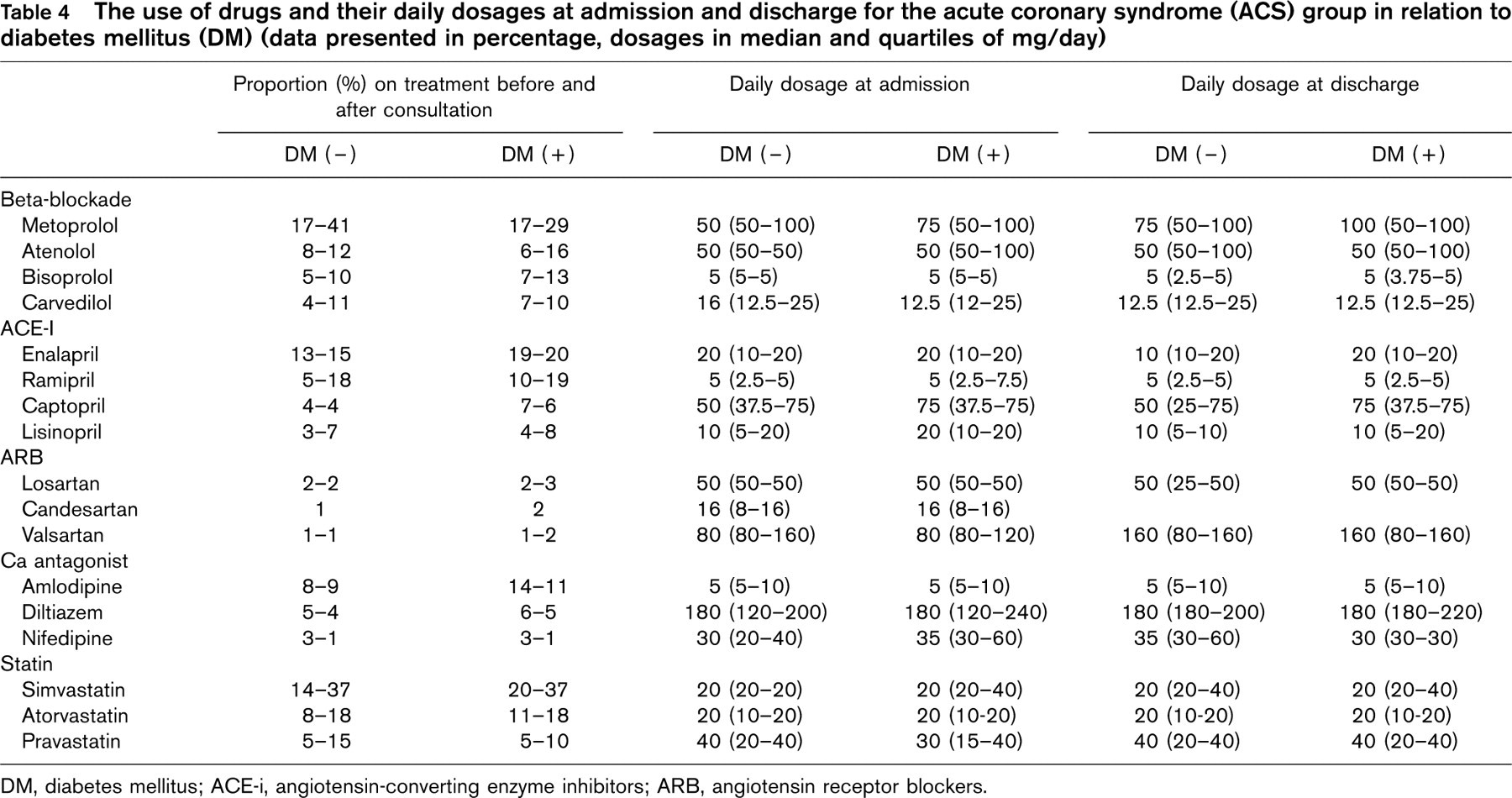
DM, diabetes mellitus; ACE-i, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers.
Use of glucose-lowering treatment in patients with diabetes mellitus (DM) and acute coronary syndrome (ACS) or stable coronary artery disease (CAD) (data presented as count and percentage)
At least 25% of patients with an established diagnosis of CAD have either a history of diabetes or meet diagnostic criteria based on blood glucose testing [25]. This means that about 1 in 4, if not 1 in 3, patients treated by cardiologists across Europe has DM. In addition, the proportion of patients with previously undetected impaired glucose regulation (22%) and DM (15%) is high in patients with CAD [19]. Regarding this high prevalence, it seems relevant to know how the diagnosis of DM influences patient management. An important question is whether the survey is representative for a general population of patients with CAD. Intentionally, the period of recruitment was kept short and the number of patients asked for from each centre was modest, to simplify the process and to help ensure high-quality data and that consecutive patients were enrolled. The strength of surveys of the present kind is that they recruit patients seen in everyday clinical practice without any exclusion criteria. However, since most patients originated from hospital settings, it should be acknowledged that they may not be representative of those cared for in primary care. Anyhow, the size and the wide geographical recruitment area in this survey make it reasonable to assume that patterns disclosed represent a true picture of the actual clinical situation.
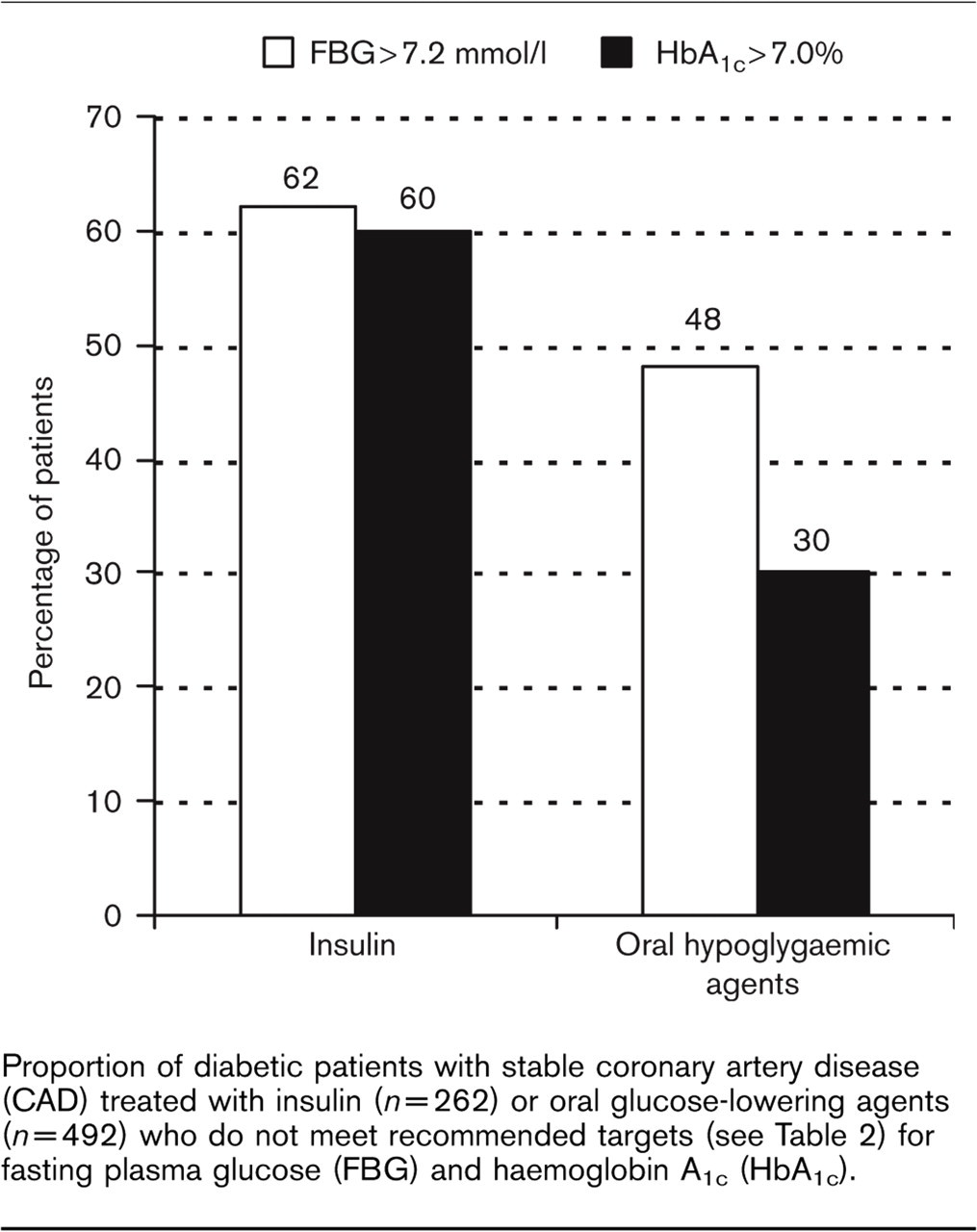
Proportion of diabetic patients with stable coronary artery disease (CAD) treated with insulin (n =262) or oral glucose-lowering agents (n = 492) who do not meet recommended targets (see Table 2) for fasting plasma glucose (FBG) and haemoglobin A1c (HbA1c).
The ACS cohort
Considering the differences in baseline characteristics between patients with and without DM, we performed a multiple logistic regression analysis including the major confounders detected in the preliminary description, to get a reliable picture of treatment and intervention patterns in patients with ACS. Somewhat surprisingly, DM did not significantly impact the in-hospital pharmacological treatment and propensity to perform interventions after this correction.
The baseline characteristics in the present survey are comparable to those in a large (10 484 patients) prospective Euro Heart Survey of ACS [26] reporting prior myocardial infarction in 22 and 36%, prior heart failure in 8 and 12% and hypertension in 52 and 64% of patients with STEMI and non-ST elevation myocardial infarction (NSTEMI), respectively. The treatment pattern at admission, with a more frequent use of drugs active on the RAA system, beta-blockers, statins and aspirin in DM patients, is concordant with the findings of other studies [16, 26]. A higher use (49 versus 35%; P < 0.001) of angiotensin-converting enzyme inhibitors (ACE-i) was, however, described in the EUROASPIRE I and II studies [27].
The intensive in-hospital i.v. treatment is consistent with findings reported by the Euro Heart Survey of ACS [26], where generally insufficient use of heparins (84-87%), i.v. beta-blockers (6-14%) and glycoprotein IIb/IIIa inhibitors (10-20%) was described in relation to existing European guidelines [28]. The present data indicate that there are no specific differences related to the DM state.
Although patients with DM were more often treated with aspirin, beta-blockade and statins at hospital admission, prescription of these drugs at the time of hospital discharge was less than to patients without DM. However, following correction for clinical confounders these differences did not remain significant. In the Maximal Individual Therapy in Acute Myocardial Infarction (MITRA) study [29] the patients, all admitted for STEMI, differed from the present population and confounders introduced in the multiple regression model are not directly comparable. Still, in this model the DM status influenced only the use of beta-blockers (OR 0.78; 95% CI 0.68–0.88) and ACE-i (OR 1.3; 95% CI 1.11–1.53).
Contemplating doses of drugs used in the DM and non-DM groups, no difference emerged, but overall doses were lower than those with a evidence-based effect. Even considering the difficulties of dosage analyses (gender, weight and co-morbidities are potential confounders), the propensity to titrate the dose towards an optimum seemed limited, especially for captopril [30] (target 150 mg/daily), metoprolol [31] (target 200 mg/daily) and carvedilol [32] (target 50 mg/daily) in relation to dosages proven beneficial in clinical trials.
In contrast to our data, an under-utilization of evidence-based drugs, heparins, i.v. beta-blockers, and thrombolysis has been highlighted in a large (25 633 patients) Swedish Register (RIKS-HIA) [16]. In RIKS-HIA, admission characteristics differed from the present as regards the prevalence of hypertension (46%), prior CABG (6%) or PCI (5%) and lipid-lowering treatment (11%). These differences are reasonably related to selection of a different group of patients (all admissions to coronary care units) and to a different period of recruitment (e.g. for the use of statins). The present data relate to a period of time about 5 years later. Moreover, prior heart failure, cerebrovascular disease and peripheral artery disease were not introduced among confounders used in the RIKS-HIA multiple regression model. An under-utilization was also described regarding coronary angiography, PCI and stenting in the Munich registry from 1999. The differences between DM and non-DM patients had, however, decreased 2 years later [17]. Similarly, revascularization was less often used (13 versus 15%; P < 0.01) in DM patients admitted for acute myocardial infarction in a large (25 697 patients) study from Ontario in 1992-1993 [33] but baseline characteristics and treatment refer to a situation 10 years distant from the present.
Thus, based on the present survey, it may be concluded that the diabetic state does not seem to influence the management of patients with ACS when taking into account differences in medical history and clinical presentation. It should, however, not be forgotten that the substantially higher cardiovascular risk and concomitant dismal prognosis in DM patients make them particularly suited for even more aggressive treatment.
The stable cohort
The stable cohort (n = 2854) can be considered as representative for analysing the treatment of the major cardiovascular risk factors in European patients with stable CAD, with and without DM. Secondary prevention in patients with stable CAD is clearly described in the European guidelines [23], both regarding the treatment and the targets to be reached. The present survey demonstrates that, even if the use of the drugs recommended is acceptable, the clinical targets are poorly reached, and if the most recent update on cardiovascular disease prevention, issued from the ESC in 2003 [34], had been referred to, the outcome would have been even worse. A similar situation, both in non-DM and DM subjects, was shown in the EUROASPIRE I and II surveys [27], even if not related to the medications at enrolment: for example, in these studies blood pressure ≥ 140/90 mmHg was found in 57 and 49% of patients and elevated total cholesterol (> 5.0 mmol/l) in 55 and 59% of the patients. Also, the results of the Euro heart survey of stable angina [35] suggests an underestimation of importance of established risk factors in patients with stable angina, since patients commonly did not have recent (< 4 weeks) cholesterol (27%) or glucose (33%) samples.
Even if relating to different targets (those recommended by ADA 2004 for adults with DM [36]), another study revealed that a very low proportion of DM patients reached an optimal glucometabolic control (59% of patients with HbA1c > 7 mmol/l; 73% with FPG > 7.2 mmol/l) [37]. The poor outcome of glycaemic control may reflect partly the lack of evidence-based data [38] on decreasing macrovascular-related clinical endpoints following aggressive glucose control if not accompanied by a multifactorial intervention on blood pressure and lipid values (STENO-2) [39]. The difficulty of success with a multi-targeted approach on cardiovascular risk factors in type 2 DM in clinical practice was reported in an Italian study [40]. In this study, only 0.8% of the patients reached all the European Consensus recommendations for lipid status, blood pressure, HbA1c and BMI [41].
The evidence that glucose status targets are less often reached in patients with stable CAD and DM treated with insulin than those treated with oral glucose-lowering agents is presumably explained by the lower extent of metabolic impairment in the former, and the fact that insulin is usually instituted at a late stage when the metabolic derangement is more difficult to control. Contemplating the use of glucose-lowering drugs (Table 5), the new insulin-sensitizing, glucose-lowering agents (thiazolidinediones) were rarely prescribed in the DM patients enrolled in the survey, due perhaps to the relatively short time after introduction in Europe. These agents have potentially advantageous effects on multiple components of the metabolic syndrome, and may provide better long-term glycaemic stability, but clinical trials with cardiovascular end points are awaited.
In conclusion, the treatment and intervention patterns in acute admissions do not differ in relation to the diabetic state when corrected for various clinical confounders. Furthermore, the survey shows a high prevalence of adverse lifestyle and modifiable risk factors among both diabetic and non-diabetic patients, with a more adverse risk-factor status among the former, which therefore are in particular need of accurate management. Clear recommendations on the management of diabetic patients with coronary artery disease are needed to reinforce a more aggressive approach, seemingly required especially for secondary prevention.