
Abstract

Introduction
Although considerable epidemiologic evidence suggests that structured aerobic exercise, increased lifestyle activity, or both, may help protect against the development of ischemic heart disease (IHD) and its adverse sequelae, exertion-related cardiovascular events have been reported in the medical literature and the lay press, suggesting that strenuous physical activity may actually precipitate sudden cardiac death (SCD) or acute myocardial infarction (AMI) in selected individuals. Numerous independent studies have now shown that SCD or AMI can be triggered by vigorous physical exertion, especially among habitually sedentary individuals with underlying IHD or structural cardiovascular abnormalities, and that the risk decreases with increasing levels of regular exercise [1]. Thus, it is critical to provide safe and effective physical activity recommendations to persons with known or suspected IHD.
The ‘Recommendations for participation in leisure time physical activity and competitive sports for patients with ischemic heart disease', written by a prestigious European Society of Cardiology (ESC) Study Group [2] of scientists, clinicians, researchers and practitioners, who are authorities in their respective fields, provides a timely, needed and important contribution to the medical literature. Accordingly, Börjesson et al. [2] offer research and clinically based recommendations for leisure-time physical activity for persons with known or suspected IHD, with specific reference to the clinical evaluation [e.g. medical history, resting and exercise electrocardiogram (ECG), coronary angiography], risk stratification profile and the advisability of, and eligibility criteria for, competitive sports. The authors address these issues in patients with documented IHD, including those who have suffered previous AMI and/or undergone coronary revascularization, as well as those with silent ischemia, unstable angina, or stable angina. Similarly, in asymptomatic patients without overt IHD, but with one or more conventional coronary risk factors, the SCORE system is advocated to estimate the 10-year IHD risk, and appropriate preparticipation screening and activity recommendations are provided. Finally, the authors address a number of topics that are clinically germane, including the ‘safest’ effective exercise intensity and its relationship to the ventilatory, anginal and ischemic ECG thresholds, influence of concomitant beta-blocker therapy, benefits of exercise in the primary and secondary prevention of IHD, and practical recommendations to reduce the risk of exercise-related cardiovascular complications. However, several of these issues merit additional commentary.
Pathophysiologic basis for exertion-related cardiovascular events: the risk—protection paradox
Pathophysiologic evidence suggests that in middle-aged and older adults with coronary atherosclerosis, vigorous physical activity, by increasing myocardial oxygen consumption and simultaneously shortening diastole and coronary perfusion time, may evoke a transient oxygen deficiency at the subendocardial level, which is exacerbated by a decreased venous return, secondary to abrupt cessation of activity. Ischemia can alter depolarization, repolarization and conduction velocity (Fig. 1), triggering threatening ventricular arrhythmias, which, in extreme cases, may be harbingers of ventricular tachycardia or fibrillation [3]. In addition, symptomatic or silent myocardial ischemia [4], sodium—potassium imbalance, increased catecholamine excretion and circulating free fatty acids may all be arrhythmogenic. On the other hand, inherited structural cardiovascular abnormalities (e.g. hypertrophic cardiomyopathy) are the major cause of SCD during exercise in younger individuals [5].
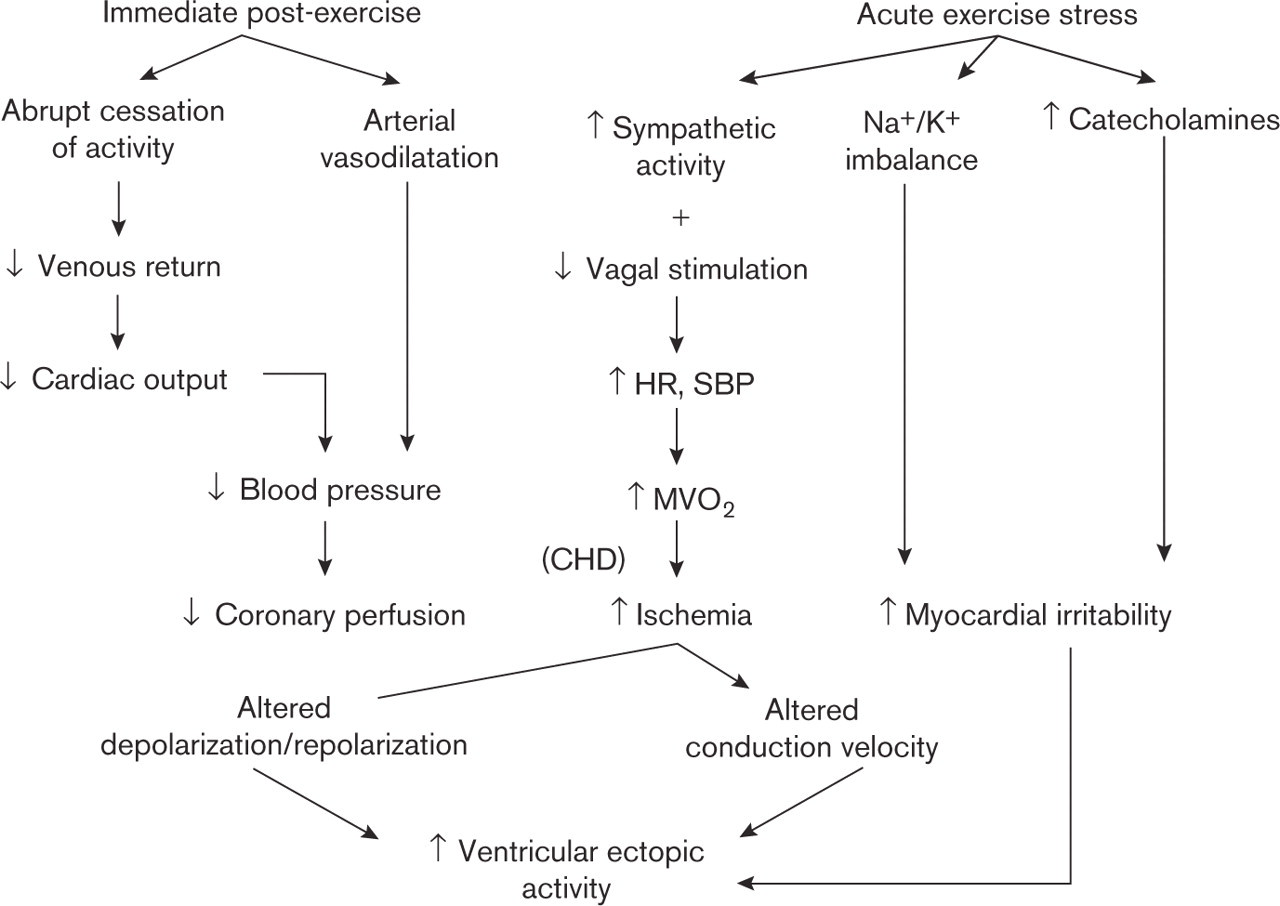
Physiological alterations accompanying acute exercise and recovery and their possible sequelae. HR, heart rate; SBP, systolic blood pressure; MVO2, myocardial oxygen consumption; CHD, coronary heart disease.
Although the reasons why strenuous physical exertion sometimes precipitates AMI are unknown, it is reasonable to suggest that the increases in heart rate and blood pressure that accompany acute exercise may give rise to hemodynamic stresses that disrupt vulnerable atherosclerotic plaque and lead to thrombotic occlusion of a coronary vessel. An increase in platelet activation and hyper-reactivity, which could contribute to (or even initiate) coronary thrombosis, has also been reported in sedentary individuals who engaged in unaccustomed high-intensity exercise, but not in their physically trained counterparts [6].
The incidence of AMI and SCD during exercise is considerably greater among persons with known IHD than among presumably healthy adults. However, the relative risk varies inversely with the individual's usual frequency of physical activity [7, 8], highlighting the protective effect of regular exercise in decreasing the risk of acute cardiovascular events.
Cardioprotective effects of exercise
Two meta-analyses [9, 10] have now shown that regular exercise participation, and especially increased cardio-respiratory fitness [11], can decrease the overall risk of cardiovascular events by up to 50%, presumably from multiple mechanisms including anti-atherosclerotic, anti-ischemic, anti-arrhythmic, anti-thrombotic and psychosocial effects (Fig. 2). Decreased vulnerability to arrhythmias [12] and increased resistance to ventricular fibrillation [13] have also been postulated to reflect exercise-related adaptations in autonomic control, providing protection against SCD. Moreover, in persons with and without documented IHD, each 1 metabolic equivalent (MET; 1 MET = 3.5 ml O2/kg per min) increase in exercise capacity appears to confer an 8–17% reduction in mortality [14]. Thus, considering the cardiovascular benefits and risks of exercise, the former outweighs the latter for the vast majority of individuals with known or suspected IHD, especially if a light-to-moderate exercise intensity is employed.
Exercise intensity: considerations regarding safety, effectiveness and medications
Börjesson and colleagues [2] recommend that individuals with IHD exercise at a moderate intensity, that is, at or below their ventilatory threshold, since exercise above this level increases the risk of cardiovascular complications. Moreover, the ESC Study Group suggested that the prescribed heart rate for training be maintained at least 10 beats/min below the anginal or ischemic ECG threshold. Although these recommendations are valid, the rationale for them requires additional clarification.
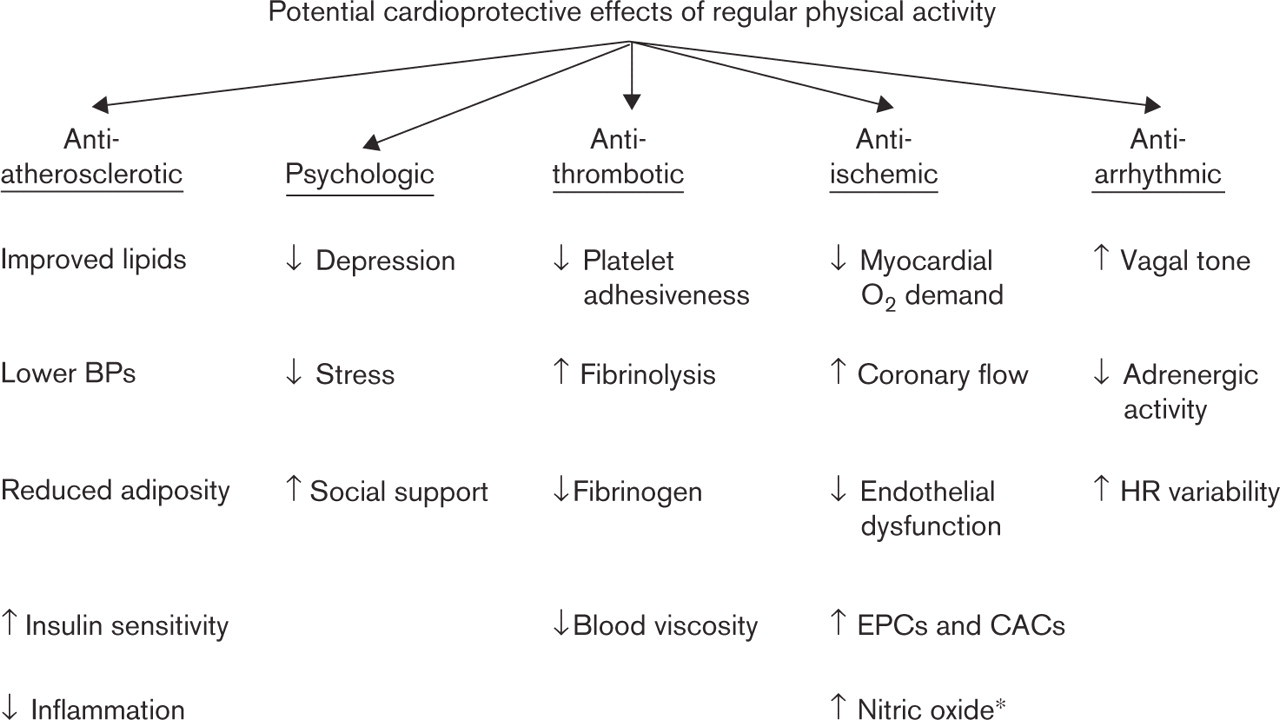
Multiple mechanisms by which regular physical activity/aerobic exercise may reduce the risk for non-fatal and fatal cardiovascular events. BP, blood pressure; EPCs, endothelial progenitor cells; CACs, cultured/circulating angiogenic cells; ú, increased; á, decreased; O2, oxygen. ∗Also has anti-thrombotic effects.
Our recent studies have shown that the threshold or minimal effective intensity for improving cardiorespiratory fitness in unfit and fit individuals with and without IHD is lower than previously thought, approximating 30–45% of the oxygen uptake or heart rate reserve [15, 16]. Thus, the majority of inactive adults with IHD can achieve favorable adaptation and improvement by brisk walking on level ground [17]. Because symptomatic or silent myocardial ischemia may be arrhythmogenic [4], the prescribed heart rate for leisure-time activities should be set safely below (≥ 10 beats/min) the ischemic ECG or anginal threshold [18]. This may, however, be difficult (or impossible) to achieve during some competitive sports which are influenced, to a large extent, by a host of extraneous variables, including team members, opponent expertise, and superimposed environmental stressors (e.g. cold, heat, humidity, altitude).
Although a sustained increase in heart rate has traditionally been acknowledged as a prerequisite to achieving a ‘training effect', it should be noted that the heart rate response to aerobic exercise serves merely as a hemodynamic correlate and monitor for the more likely training stimulus, increased somatic oxygen uptake. Since aerobic capacity is little affected by beta-blockade, it appears that patients on beta-blockers can still achieve the increase in metabolic rate for training by compensatory increases in stroke volume or arteriovenous oxygen difference, or both. This premise has been substantiated by numerous reports demonstrating that cardiac patients may derive considerable physiologic benefit from an exercise training program in the presence of long-term beta-blocker therapy [19]. Nevertheless, prescribed heart rates for training should be based on an exercise test conducted under conditions as similar as possible, with respect to the timing of beta-blocker therapy, to those under which the subject will be exercising [20, 21].
Identifying the patient ‘at risk'
Due to the vagaries of the atherosclerotic process, the accuracy in predicting which persons will have a cardiovascular complication during exercise remains imperfect. The recommendations of the ESC Study Group [2] include exercise stress testing and coronary angiography as diagnostic and/or evaluation methods for IHD. Yet, both have significant limitations in identifying individuals ‘at risk'. Although exercise testing may be helpful in identifying silent ischemia and malignant ventricular arrhythmias, a truly positive exercise test requires a hemodynamically significant coronary lesion (e.g. >75% stenosis), whereas nearly 90% of AMIs occur at the site of previously non-obstructive, angiographically documented plaques [22]. Moreover, important lumen stenosis may be delayed until plaque occupies more than 40% of the internal elastic lamina area [23]. Consequently, conventional coronary angiography may, in revealing a normal or near-normal lumen cross-sectional area, vastly underestimate underlying atherosclerotic coronary artery disease.
Thompson and associates [24] noted that neither superior athletic ability, habitual physical activity, nor the absence of cardiac risk factors guarantees protection against an exercise death. Forewarning symptoms appeared to present the only clue to impending, exercise-related cardiovascular events. Accordingly, physicians and allied health professionals should counsel their patients to discontinue their exercise and seek medical advice if they experience prodromal cardiac signs or symptoms, including arrhythmias (palpitations), dizziness or angina.
Recommendations to potentially reduce the incidence of exercise-related cardiovascular events
Although regular exercisers enjoy a reduced overall risk of cardiovascular events, the risk of AMI and SCD appears to transiently increase during strenuous physical exertion [1], as compared with the risk at other times, especially in individuals with underlying structural cardiovascular abnormalities or IHD. Additional recommendations to potentially reduce the risk of cardiovascular events during exercise include [3]: encourage sedentary individuals to engage in regular moderate intensity activity so as to move them out of the least fit, least active, ‘high risk’ cohort; counsel unfit middle-aged and older individuals to refrain from unaccustomed, hard-to-maximal intensity activities (e.g. racquet sports, jogging, snow removal); advocate appropriate warm-up and cool-down procedures; emphasize strict adherence to exercise at or below the ventilatory threshold, using prescribed heart rates and/or perceived exertion as adjunctive intensity modulators; minimize or proscribe competitive sports in individuals ‘at risk'; and reduce the exercise intensity in settings with superimposed environmental stressors. Because automated external defibrillators have become easier to use, safer, relatively inexpensive, and more effective at improving survival from SCD, it seems that athletic stadiums, competitive sporting events, and health/fitness facilities should join the escalating number of public places that are equipped with these life-saving devices [25].