
Abstract
Background
Self management of oral anticoagulation (OAC) decreases complication rates and improves quality of life. Manual and cognitive abilities of patients and patient training in a structured format are a precondition for this concept. Up to now, there is no evidence about knowledge increase from teaching programs.
Methods
Seventy-six patients (mean age, 57.4 years, 71% male) who started long-term OAC were included in the prospective multi-center study at three teaching centers representing different populations of anticoagulation patients: a department of cardiovascular surgery, an inpatient rehabilitation center and an anticoagulation clinic. The patients were trained in a structured education program for two days. For the evaluation, the patients performed standardized tests including 16 questions prior to start (T0), after each training unit (T1/T2) and 6 weeks later (T3). The primary endpoint was the percentage of > 75% of patients who could answer > 50% of questions correctly at T3. Secondary endpoints were the overall and item-specific percentages of correct answers at the end of each training unit (T1, T2) and at T3. In addition, the teaching program was rated by the patients on a six-point rating scale.
Results
Seventy-four out of 76 patients gave at least 50% correct answers at T3 (97.4%; 95% confidence interval, 90.8–99.7%). The average rates of correct answers developed from 40% (T0), 86% (T1), 94% (T2) to 96% (T3). The greatest increase of knowledge was observed with blood components, interpretation of International Normalized Ratio (INR) value, and the interaction of anticoagulation with other variables (e.g. drugs or infection). Patients rated the teaching program between 1 (best rating) and 2 at all time points. At T3, the patients reported less fear of complications and less limitations in their daily life than in earlier evaluations.
Conclusion
The structured training program IN Ratio appears to be an appropriate instrument for instruction of INR self management. In comparison with baseline knowledge, the percentage of correctly answered questions was twice as high directly after the end of training and remained at a high level of > 90% for at least 6 weeks.
Introduction
Therapy with warfarin and phenprocoumon is established in patients with atrial fibrillation, mechanical heart valve replacements and and/or thromboembolic events (stroke, deep vein thrombosis or pulmonary embolism) and indicated in a fast-growing number of patients [1]. A high dose guarantees a substantial reduction in the number of thromboembolic events, but could cause hemorrhagic and potentially fatal complications [2,3]. Oral anticoagulations have a narrow therapeutic range and a high intra- and interindividual variability [4]. Therefore, for patients under oral anticoagulation frequent monitoring of anticoagulation intensity is necessary in order to achieve maximal efficiency and high security in dose adjustment to the individual therapeutic range.
For several years portable coagulometers have been available that make it possible to measure the International Normalized Ratio (INR) value by taking one drop of capillary blood from the finger tip [5,6]. Trained patients are able to self-monitor and perform self-adjustment of medication dosages in order to determine INR values, similar to the self-management of diabetes mellitus. Studies of patients with self-management have shown that values are in the therapeutic range more frequently. Moreover, the number of undesired consecutive events is reduced significantly [7–10. The number of patients performing self-management is gradually increasing, and has reached 100 000 patients worldwide.
Modern devices comply with conditions that are important for self-management such as high accuracy and simple handling [5]. The INRatio system from Hemosense, Inc. (San Jose, CA, USA) which was used in this study features innovative improvements: in addition to the patient test channel, the test strip also contains two reference channels, in which quality control checks will be performed simultaneously. These should avoid incorrect readings due to damaged test strips that have been exposed erroneously to high humidity or temperature.
A structured training program for patients is a precondition for self-management [11]. Until now, there has been no evidence about patient knowledge before starting oral anticoagulation. Moreover, there is no data to determine whether their knowledge can be enhanced by a structured training program and whether this knowledge can be sustained.
The aim of this study was to evaluate the training program tailored to the INRatio system with respect to mediation and sustainability of specific patient knowledge and acceptance of the program by participants.
Methods
Patients
The study included 54 men (71.1%) and 22 women (28.9 %) over 18 years with indications for long-term oral anticoagulation and the ability to read and write the German language.
On-going heparin therapy and hematocrit values outside the range 30–55% at the start (T0) led to exclusion from the study. In addition to the inclusion and exclusion criteria, patient history contained demographic data (date of birth, sex, weight, size, married/single, retired yes/no, blue-collar/white-collar worker/self-employed, highest level of education) and the indication for anticoagulation, individual therapeutic range, risk factors/comorbidity and other medication(s) were recorded. The initial laboratory data contained blood count, measured hematocrit value, hemoglobin, platelets and INR-value.
Protocol
Intensive theoretical training took place at T1 and T2 according to the curriculum for trainers and with the use of a ‘Practice Manual for Patients'. Training duration was half a day each with an interval of 2–7 days including practice to individually determine the INR value (Fig. 1). Both sessions were subjected to an evaluation using a standardized patient questionnaire. At the end of the training, patients self-determined their INR value. The results were checked for accuracy by comparing with reference values taken in the laboratory.
The training was followed by a 6-week-period of individual practice. Reference values were taken every second week by the individual centers and compared with the self-determined values.
After 6 weeks (T3), a final evaluation was made, which included the ability to correctly measure and adjust the therapy in addition to knowledge loss or knowledge increase.
Coagulometer/clinical samples
Capillary blood was drawn by a standardized technique from the finger tip and analyzed immediately by Hemosense INRatio. Every patient received their own coagulometer and test strips. The INRatio is a point-of-care system that processes fresh capillary blood and determines only INR values. The device is calibrated through a charge-specific code and observes the reaction electronically.
The INR values from the local laboratory were determined from citrated plasma samples taken from venous blood and analyzed within 6 h. The plasma samples for the reference laboratory were shock-frozen, stored under low-temperature conditions and analyzed at a later time. The laboratory used a thromboplastin reagent Innovin (Dade-Behring, Marburg, Germany) with the coagulation analyzer STA Compact (Stago, Paris, France).
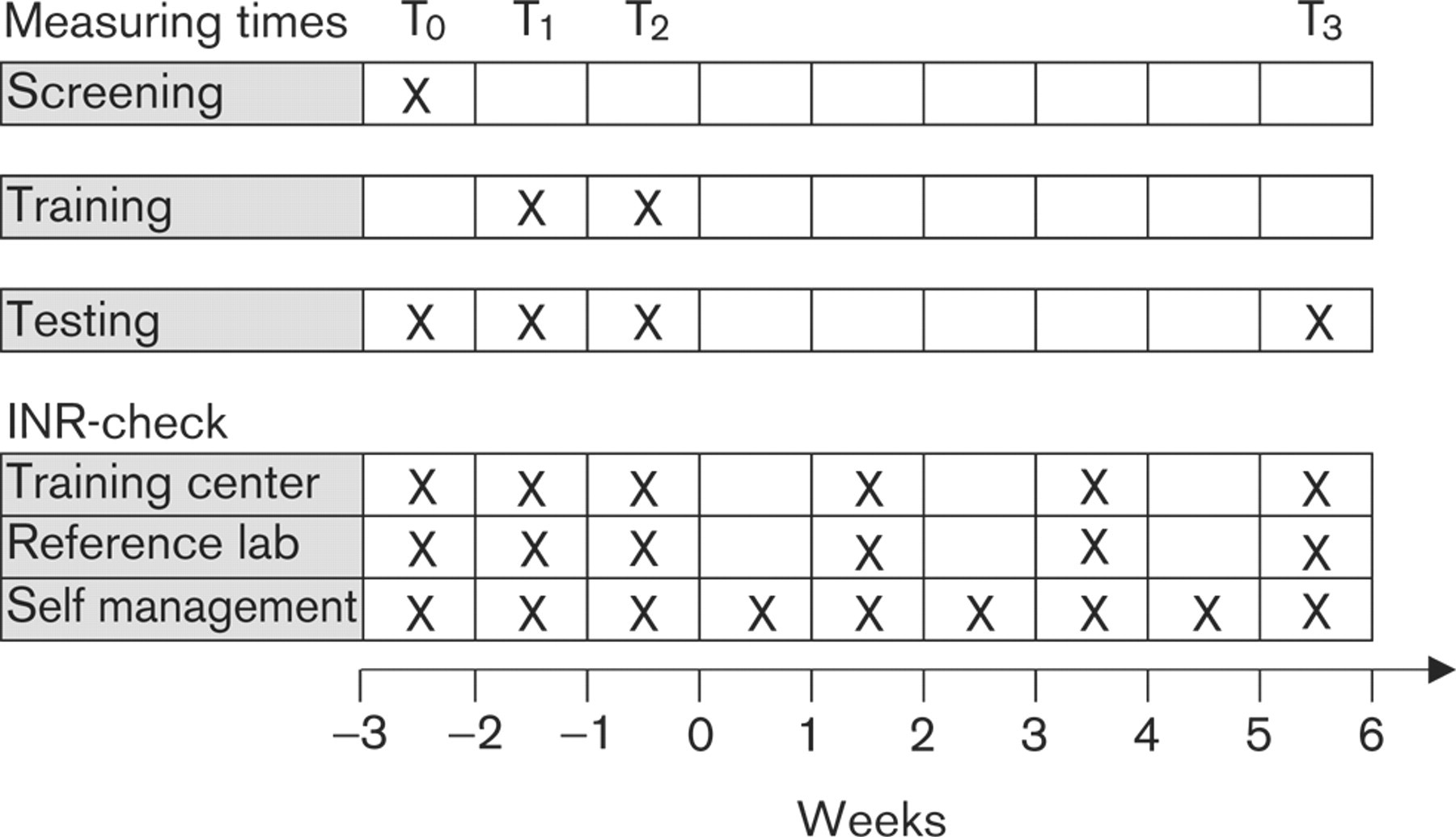
Times (T) of training, testing, and International Normalized Ratio (INR) check.
Training
Training took place in groups of between two and a maximum of five persons (mean, 3.7) and included correct blood sampling, accurate handling of the device, self measurement, and dose adjustment. The patient needed to realize the importance of regularly measuring his INR value and remaining within his own therapeutic range. In order to correct the dose precisely, the patient needs know about the effect of the anticoagulant agent in order to restore the INR values to his individual therapeutic range, if necessary.
The performance of a standardized, well-structured and customized training is a key item in the guidelines for self-management of anticoagulation therapy [11]. Experience indicates that training sessions should not exceed 120 min. The quantity of learning material makes it necessary to instruct small groups on at least two different days. The current standard teaching is based on the Structured Teaching and Self-management Program for patients receiving Oral Anticoagulation (SPOG) program with customized features [12].
The program introduced in this study contains different points of emphasis within the training material and, although the contents are standardized, the program leaves it to the trainer to highlight issues that are of specific concern to the particular audience.
The lessons on the first day included coagulation, anticoagulation, the concepts of INR value and individual therapeutic range as well as the documentation of INR values in a patient log book. Moreover, handling of the measuring device was practised. The second set of instruction deals with interaction of anticoagulation, early detection and handling of potential complications, extensive practice of correct dose adjustment and management of extremely high values. The training set was followed by a final exercise of INR self-management using the device.
The instructional aids include the curriculum for the trainer whose version features additional didactic ideas about specific study subjects on the left side of the study booklet that supplement the right side in the patient version. Overhead-projected slides can be used to illustrate ideas visually. After the end of the training the study materials are intended to provide the patient with a comprehensive reference source to use whenever needed.
A patient log book serves as the source of documentation and information for the general practitioner who is responsible for subsequent care of the patient as necessary, along with anticoagulation self-management as recommended by the training center. In addition to the values saved in the device, the log book allows the physician to supervise the process of self-measurement and self-medication. Thus, quality control is ensured through the general physician who can detect and correct training deficiencies, if necessary.
The knowledge provided in the training program was evaluated by standardized questionnaires at T0 (prior to start of training), T1, T2 and T3. They encompassed 13 detailed questions about the subjects taught. The answers were prepared in multiple-choice format.
Statistical evaluation
The primary endpoint was the percentage of trained patients who could answer at least 50% of the questions at T3 (6 weeks after the end of the training program). The study was pre-defined to be regarded as successful if at least 75% of patients were demonstrated to know the answers of more than 50% of the questions after 6 weeks. This criterion was planned to be evaluated using a onesided binominal test (α = 0.05). A sample size calculation before the start of the study revealed that 60 patients were required to demonstrate this criterion with a power of over 90%, if in reality 90% of the patients know at least half of the questions. Seventy-six patients were included in the study to allow for possible withdrawals.
The number of correctly answered questions at the three measuring points and percentage of correct answers per question served as the secondary endpoint. The rates together with two-sided 95% confidence intervals were calculated. The training was evaluated by the patients at T1 and T2 (rank 1–6, 1 = excellent, 6 = poor). Profile diagrams illustrate the results. Ratings were compared using the Wilcoxon signed rank test.
Results
Seventy-six patients, 54 men (71.1%) and 22 women (28.9%) with mean age of 57.4 years, (range 20–78 years) were enrolled in the study (Table 1). Five patients were still on heparin therapy and therefore did not comply with the inclusion criteria. One patient had to be excluded because of urgent surgery. Over the course of the study term there was two drop-outs. One patient cancelled the informed consent and another patient suffered from global respiratory insufficiency.
Indication for long-term anticoagulation was a mechanical heart valve replacement in 64.5% and atrial fibrillation in 18.4% (Table 2). The most frequent co-morbidities were hyperlipidemia, arterial hypertension and diabetes mellitus. Two patients had a history of stroke, one patient suffered from renal failure (Serum creatinine > 2 mg/dl).
The target INR range was 2–3 for 42.1% of patients, 2.5–3.5 for 68% of patients and 3–4 for 9.3 % of patients.
Knowledge testing
Questions on coagulation and anticoagulation therapy were answered correctly by 39.8% of patients prior to training, by 86.7% after the first training day and, by 94.3% after the second training day (Fig. 2). After 6 weeks, 95.3% still gave correct answers, 74 of 76 patients gave at least 50% correct answers (97.4%, one-sided 95% confidence interval 90.8–99.7%). The binominal test resulted in P < 0.00001. Thus, the primary aim of the study was accomplished.
The analysis of individual items revealed a significant increase of knowledge regarding blood components, interpretation of INR value and corresponding dose adjustment and interaction of anticoagulation with other variables (e.g. drugs or infection) (Table 3). However, questions on the effect of oral anticoagulation and adjustment of INR value produced correct answers less frequently over the course of training. Patients were familiar with the indication for anticoagulation and INR test frequency even prior to training.
Patient characteristics
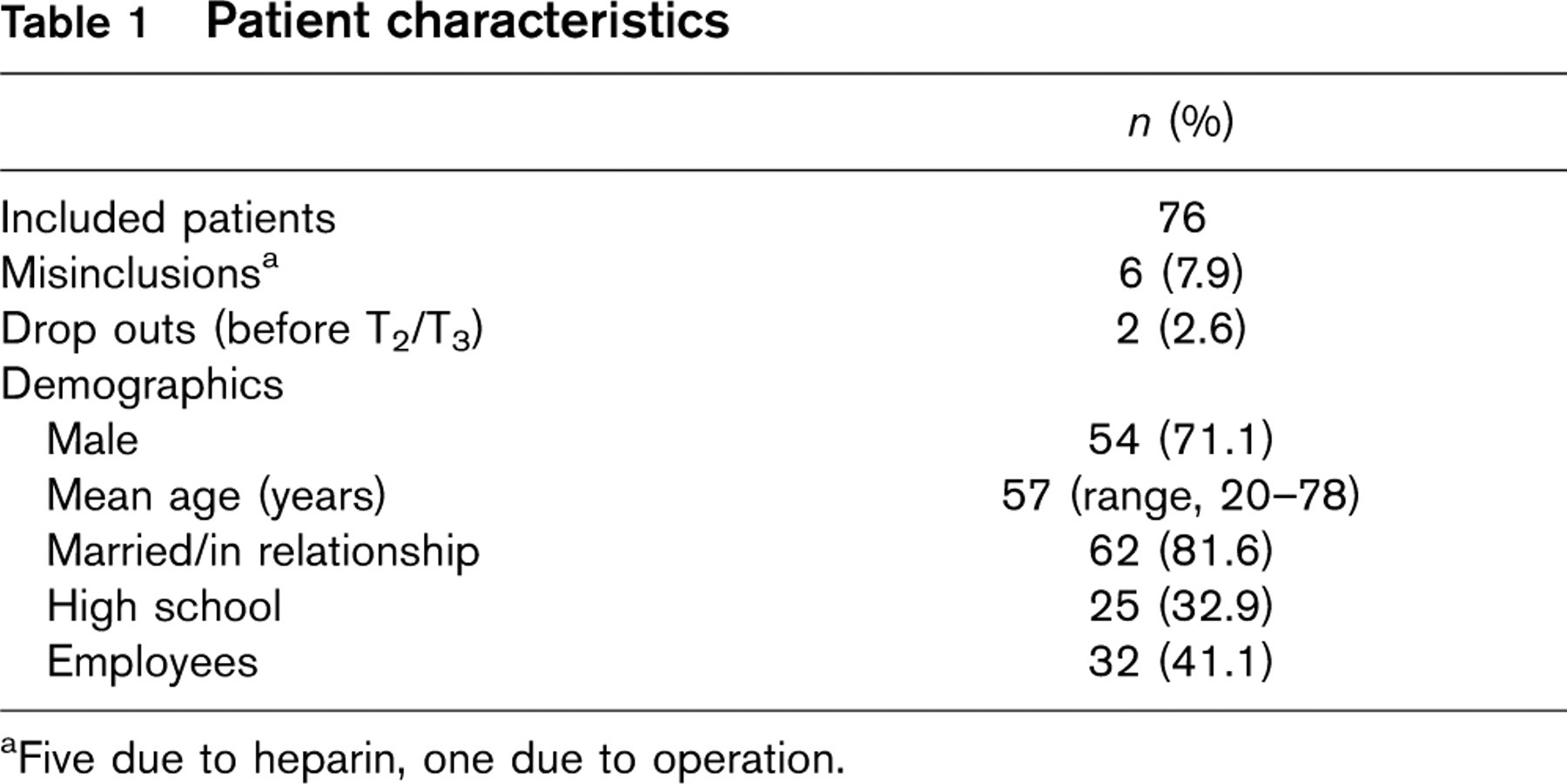
aFive due to heparin, one due to operation.
Indication for anticoagulation, cardiovascular risk profile and International Normalized Ratio (INR) target range
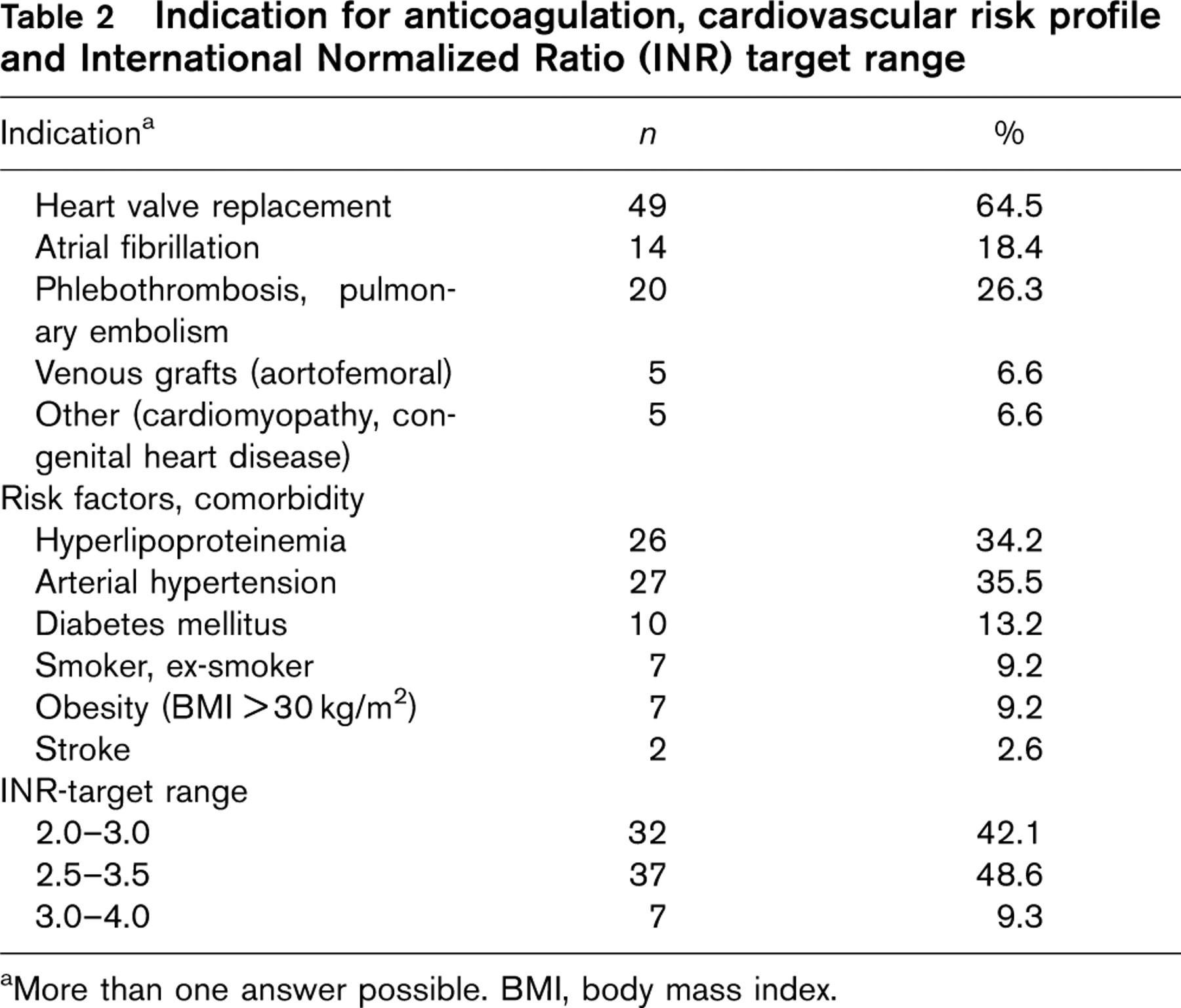
aMore than one answer possible. BMI, body mass index.
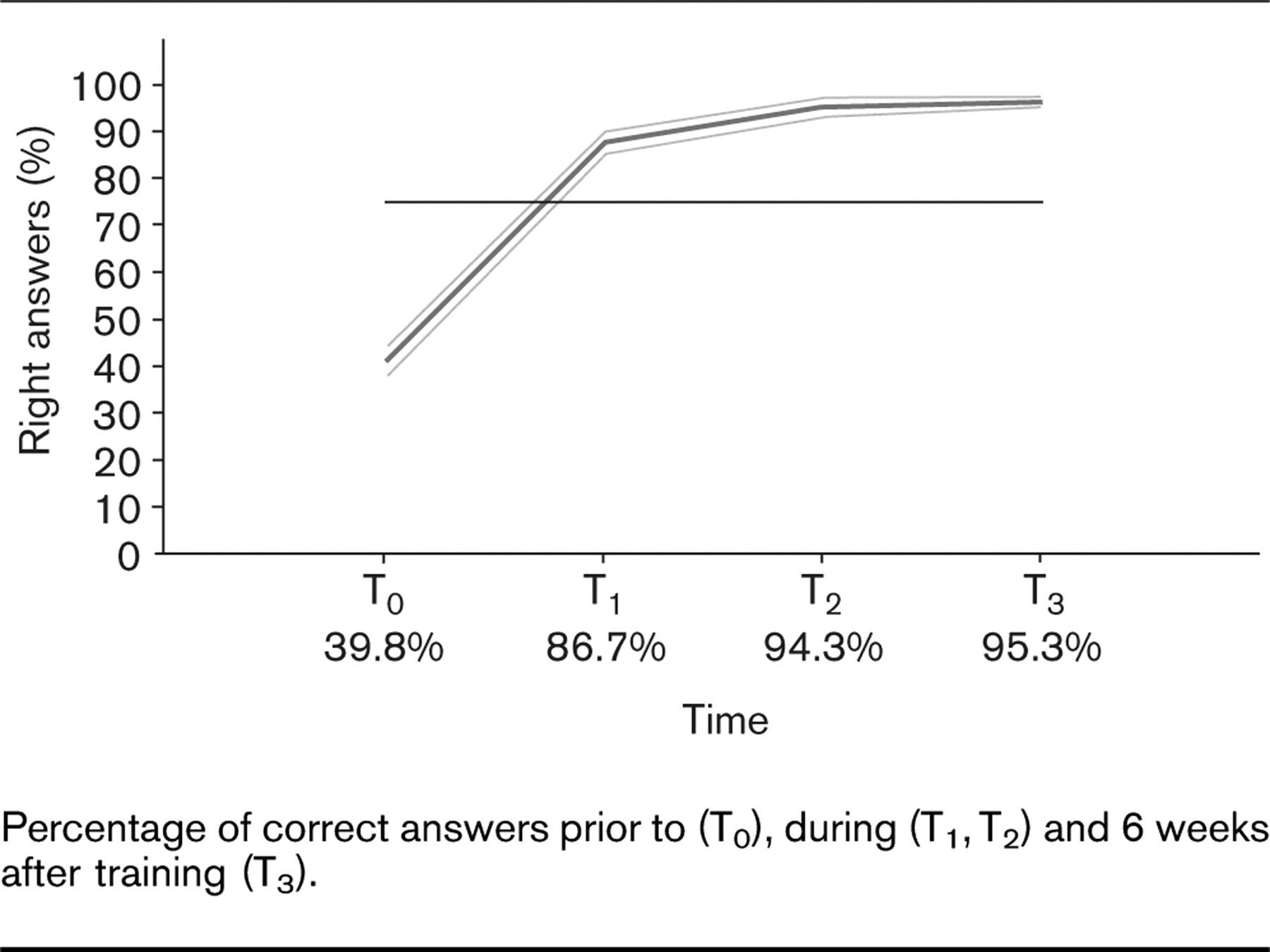
Percentage of correct answers prior to (T0), during (T1, T2) and 6 weeks after training (T3).
Evaluation of curriculum and monitor
The patient's quality of life, as well as fear of hemorrhagic or thromboembolic complications, revealed positive outcomes during the course of the training. Thus, perceived constraints due to therapy were significantly lower after training. Fear of thromboembolism and bleeding was reduced significantly (Fig. 3). During this study no complications occurred. Evaluation of the instruction related to comprehension, visual aids, and studying material produced good and very good results overall. Handling of the device was rated well (rank 1–2). Initially, a few problems were encountered regarding the practicality of the device because extracting a sufficient amount of blood was not always successful at the first attempt. The proportion of INR values in the target range was increased from 36.1% in T1 to 60.3% after 6 weeks.
Discussion
Up to now, there has been no data concerning the quantitative effect of a structured training in the area of anticoagulation. The present results show for the first time that knowledge on the part of the patients is not only increased significantly (from 40 up to 90%), but even remains on a high level without the need for refresher courses.
In the absence of direct evidence of training success, until now it was rated as an indirect training outcome that the number of INR values in the individual target range for patients with self-management was higher in comparison with those in the usual care of a general physician [12].
Percentage of correct answers for questions about coagulation and anticoagulation therapy at different times
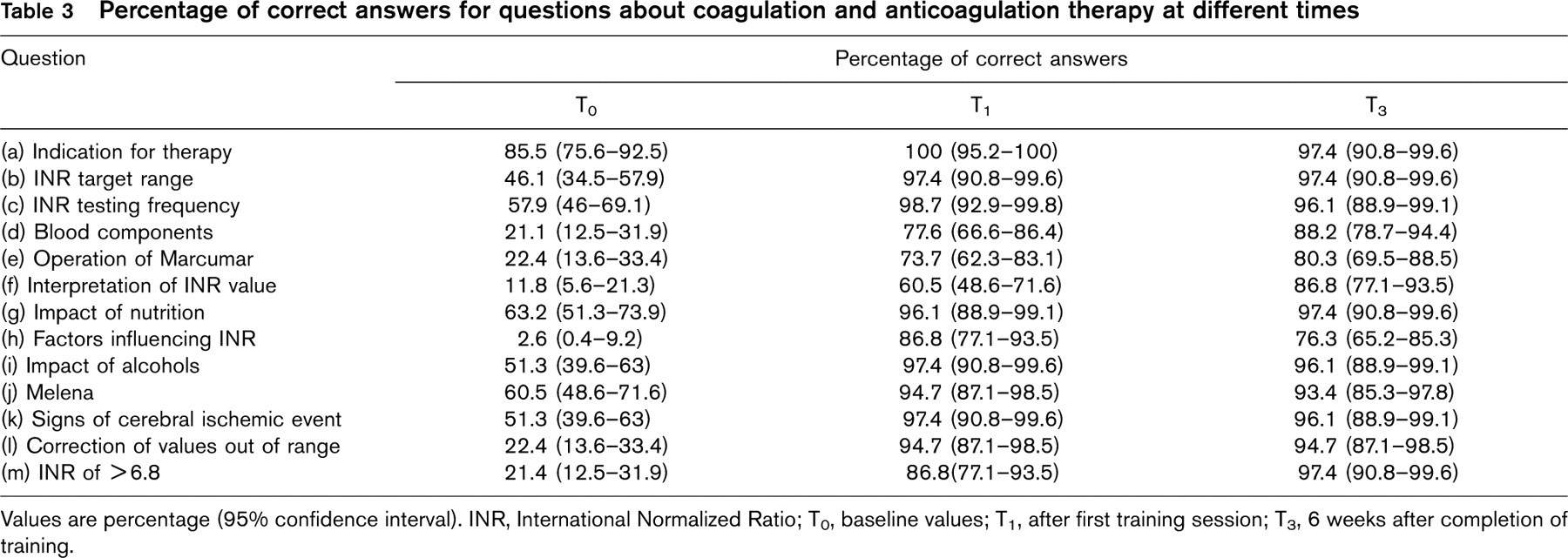
Values are percentage (95% confidence interval). INR, International Normalized Ratio; T0, baseline values; T1, after first training session; T3, 6 weeks after completion of training.
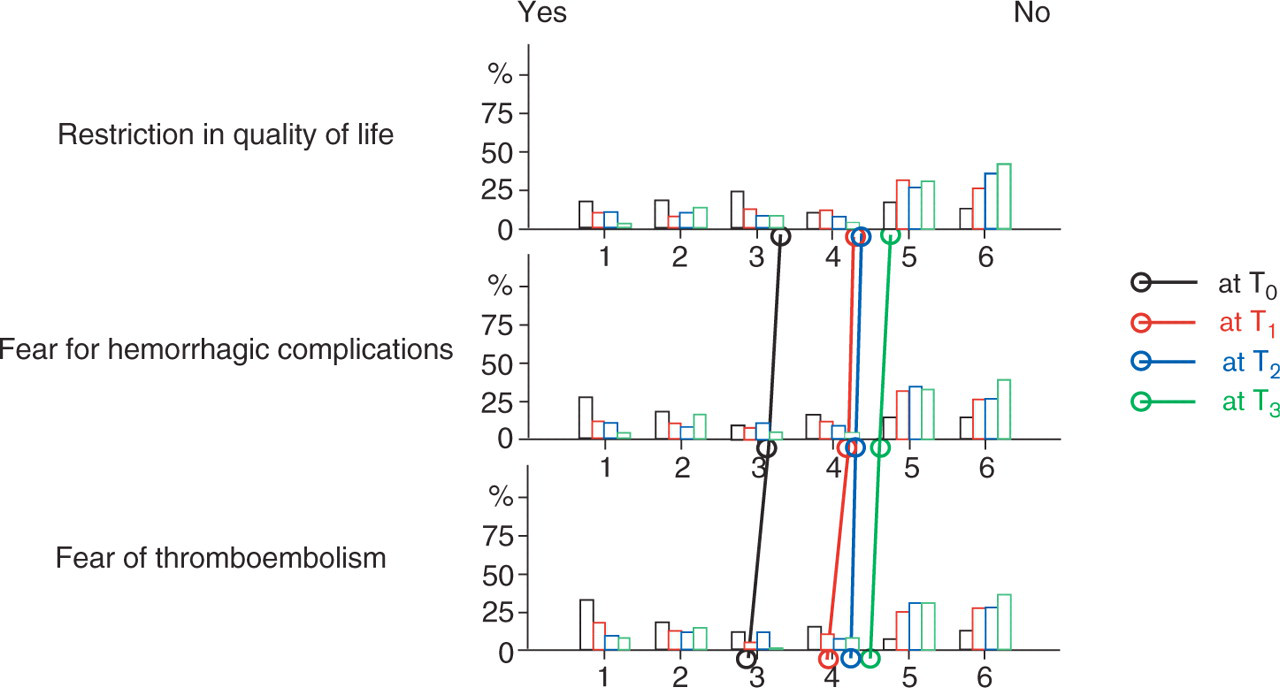
Effects of training on quality of life.
In comparison with the SPOG program, analysis of the questions used in this study allowed a detailed evaluation of patient knowledge for the first time. Although prior to the start of an anticoagulation therapy the majority of patients only know about a small part of the issues relevant to them, a substantial increase of knowledge, in particular in the areas of individual therapeutic range, interpretation of INR-value, factors influencing INR and dose adjustment, can be imparted through a training program that concentrates on the fundamental aspects of anticoagulation. This fact might explain the better control of anticoagulation intensity in patients with self-management not only in comparison with those in the care of a general physician but also to those in the care of an anticoagulation clinic [6, 8,10,13,14]. In a randomized study of 1200 patients with mechanical heart valve replacement, trained patients were able from the seventh post-operative day to be within their INR target range significantly more often than the group under the care of their general physician [13]. With a therapeutic range of two INR, 80% of the measured values were within this range, whereas 60% of INR values were in the narrower range of one unit in our study after 6 weeks. The study by Cromheecke et al. shows that the mean individual percentage of time in the therapeutic range was more than 50% during the self-management phase and significantly higher than under conventional care [14].
Knowledge should be improved with respect to interactions of anticoagulants and co-medication that result in complications. The Rotterdam study on 1124 patients with long-term oral anticoagulation demonstrates that co-medication with antibiotics provoke INR values > 6 in one-third of all patients. In particular, medication with sulfamethoxazol/trimethoprin, vancomycin, amoxicillin, and clarithromyzin lead to a hazard ratio 20 times higher [15].
Trained patients show less fear of complications and the limitations on their daily life are perceived to be less severe. This outcome confirms studies that describe a higher quality of life [16,17]. The four main arguments in favor of self management among patients are that it provides a higher degree of medical safety, the possibility of more frequent checks and adjustment of dosage if necessary. Fewer phlebotomies are needed and it allows the patient to be independent of the general physician, which is a considerable advantage when traveling.
The high acceptance of the training program and coagulometer guarantees compliance by the patient who takes on a high degree of self-responsibility. Nevertheless, control of therapy should still be carried out by the general physician as demanded in guidelines and by the health care provider [11,18]. This prerequisite is fulfilled if using the coagulation monitor INRatio, which found good acceptance among general physicians.
In conclusion, the structured training program INRatio appears to be an appropriate instrument for instruction of INR self-management. Compared to baseline, the percentage of correctly answered questions was twice as high directly after the end of training and remained at a high level of >90% for at least 6 weeks. The high acceptance rate of the training concept and coagulometer by the patient provides for a safe therapy control in cooperation with the general physician.