
Abstract
Background
Cigarette smoking is associated with an increased risk of peripheral arterial disease, but the relationship between smoking cessation and preclinical peripheral atherosclerosis is uncertain.
Design and methods
A cross-sectional, population-based study to examine the effect of smoking and smoking cessation on the prevalence of peripheral arterial disease among 1215 men aged 60–79 years in two Japanese communities in 1999–2000. The ankle-to-arm systolic blood pressure index (AAI) was used as an estimate of the presence of peripheral atherosclerosis.
Results
The mean AAI correlated inversely and linearly with smoking status and pack-years of smoking. The multivariate prevalence odds ratio [95% confidence interval (CI)] of low AAI (<0.90) compared with never-smokers was 3.7 (95% CI 1.1–12.7) for current smokers and 4.2 (95% CI 1.2–14.6) for men with 45 or more pack-years of smoking. In men who have quit smoking for 20 years or more, the mean AAI was higher and the prevalence of low AAI (<0.90) was lower than those of current smokers, but similar to those of never-smokers.
Conclusions
Our results confirm that current smoking and pack-years of smoking correlate with the presence of peripheral artery disease. The results suggest that smoking cessation for 20 years or more is associated with the regression of atherosclerosis in peripheral arteries. This finding needs to be confirmed by a prospective study.
Introduction
Previous epidemiological studies have indicated that cigarette smoking is associated with a two to fourfold increase in the prevalence of atherosclerotic peripheral arterial disease [1–6]. Smokers suffering from intermittent claudication are prone to develop disabling claudication and limb-threatening ischaemia, leading to surgical intervention [7, 8]. Peripheral arterial disease is also associated with an increased risk of mortality from cardiovascular disease and other causes [9, 10], and is a consistent risk factor for incident cardiovascular disease [11].
The prevalence of smoking is high (54.0%) among Japanese men; and cardiovascular disease comprised 30% of all deaths according to the 1999 National Health Survey of Japan [12]. Although clinical studies have shown a definite benefit of smoking cessation to reduce the progression of clinical peripheral artery disease and the risk of amputation [13], little evidence is available on whether smoking cessation reduces the development of preclinical peripheral atherosclerosis.
The ratio of ankle-to-arm systolic blood pressure measured by a Doppler ultrasound device, namely the ankle–arm index (AAI), has been used to estimate the presence of peripheral atherosclerosis [1–6, 10, 11, 14]. The present study is a cross-sectional, population-based study of elderly Japanese men. The study was designed to examine the association between smoking and smoking cessation with AAI, an indicator of peripheral atherosclerosis.
Methods
The subjects were population-based samples of Japanese men aged 60–79 years, living in two farming communities of Ikawa, northeast Japan (1995 census population: n=642) and Kyowa, central Japan (n=1492). Annual cardiovascular risk surveys have been conducted since 1963 in Ikawa and since 1981 in Kyowa by a research team of the Osaka Medical Center for Health Science and Promotion, and the University of Tsukuba. Participants in the 1999–2000 surveys who underwent AAI measurement (n = 377 in Ikawa, participation rate 59%, and n = 842 in Kyowa, 56%) were enrolled in the present study. We restricted the subjects to men in the present study because of the higher priority for examination as a result of the threefold higher reported prevalence of peripheral arterial disease in men than in women [1]. Informed consent was obtained from the participants. In the present study, no participants reported a history of clinical peripheral arterial disease.
Measurement of ankle-arm index
Trained technicians using a standard protocol determined the AAI ratio [2], as described in our previous study [6]. In 1999, systolic blood pressure was measured at the right brachial artery using a standard sphygmomanometer and right and left posterior tibial arteries using a bidirectional Doppler ES-100V II (Hayashi Denki Co., Japan). Standard 12-cm blood pressure cuffs were applied to both ankles and an appropriate size cuff to the right arm. After 5 min of rest and while the subject was in the supine position, systolic blood pressure levels were measured in the right arm and both ankles, then repeated 30 s later. The cuff was inflated rapidly to 20 mmHg above the palpated systolic blood pressure and deflated at 2 mmHg per pulse. The first appearance of Korotkoff sounds was recorded as the systolic pressure. In 2000, AAI was measured automatically using the Form PWV/ABI device (Colin Co., Japan), in which the automatic sphygmomanometer (BP-203RPE) with standard 12-cm blood pressure cuffs was applied to both ankles and one arm to calculate AAI automatically. Comparison of the two measurement systems showed no difference between the AAI values measured by the two techniques. We thus used the data on AAI measured in 1999 and 2000 for the analysis [6]. The lowest AAI in either leg was used for the analysis, and values of AAI less than 0.90 were defined as the presence of peripheral arterial disease [14]. We excluded four participants with AAI greater than 1.50, because an extremely high AAI usually reflects arterial rigidity, preventing arterial compression [2]. The data of 1215 participants were thus used for the analysis.
Measurement of atherosclerosis risk factors
Risk factors for atherosclerosis were measured in the 1999 and 2000 surveys. An interview was conducted to ascertain the smoking history and number of cigarettes smoked per day. Individuals who smoked one or more cigarettes per day were defined as current smokers, whereas those who had quit smoking for at least 3 months were defined as ex-smokers. The pack-year of smoking was calculated as the number of packs smoked per day, multiplied by the years of smoking.
We measured several potential confounders as described in detail in our previous study [6]: body mass index, arterial blood pressure, serum total cholesterol and high-density lipoprotein (HDL) cholesterol, ethanol intake, and diabetes mellitus. Body mass index was calculated as weight (kg) divided by the height squared (m2). Hypertension was defined as systolic blood pressure of 140 mmHg or greater and diastolic blood pressure of 90 mmHg or greater, or current treatment with anti-hypertensive medication, whereas normotension was defined as systolic blood pressure of less than 140 mmHg and diastolic blood pressure of less than 90 mmHg and no antihypertensive medication.
For the measurement of serum lipids and glucose, non-fasting blood was drawn from seated participants into a plain, siliconized glass tube, and the serum was separated. Total cholesterol and HDL cholesterol were measured using enzymatic methods by an automatic analyser (Hitachi 7250; Hitachi Medical Corp., Ibaraki, Japan) at the Osaka Medical Center for Health Science and Promotion, an international member of the US National Cholesterol Reference Method Laboratory Network [15]. Serum glucose was measured using the hexokinase method by the same instrument.
An interview was conducted to ascertain the amount of alcohol consumed per day, the use of medication for hypertension and diabetes mellitus, and a past history of stroke and coronary heart disease. The interviewer assessed the average weekly intake of alcohol in units of ‘go', a traditional Japanese unit of volume corresponding to 23 g of ethanol, and converted to grams of ethanol per day. Diabetes mellitus was defined as a fasting glucose level of 7.0 mmol/l or greater, a non-fasting glucose level of 11.1 mmol/l or greater, or the use of medication for diabetes. The information on a past history of stroke and coronary heart disease was supplemented by systemic surveillance data for the incidence of these endpoints since 1963. In that surveillance system, the final diagnoses were made by the standardized criteria based on clinical symptoms, computed tomography or magnetic resonance imaging, electrocardiogram and cardiac enzymes [16, 17].
Age and community-adjusted mean values and prevalence (%) of atherosclerosis risk factors according to smoking status among 1215 men aged 60–79 years in Japan
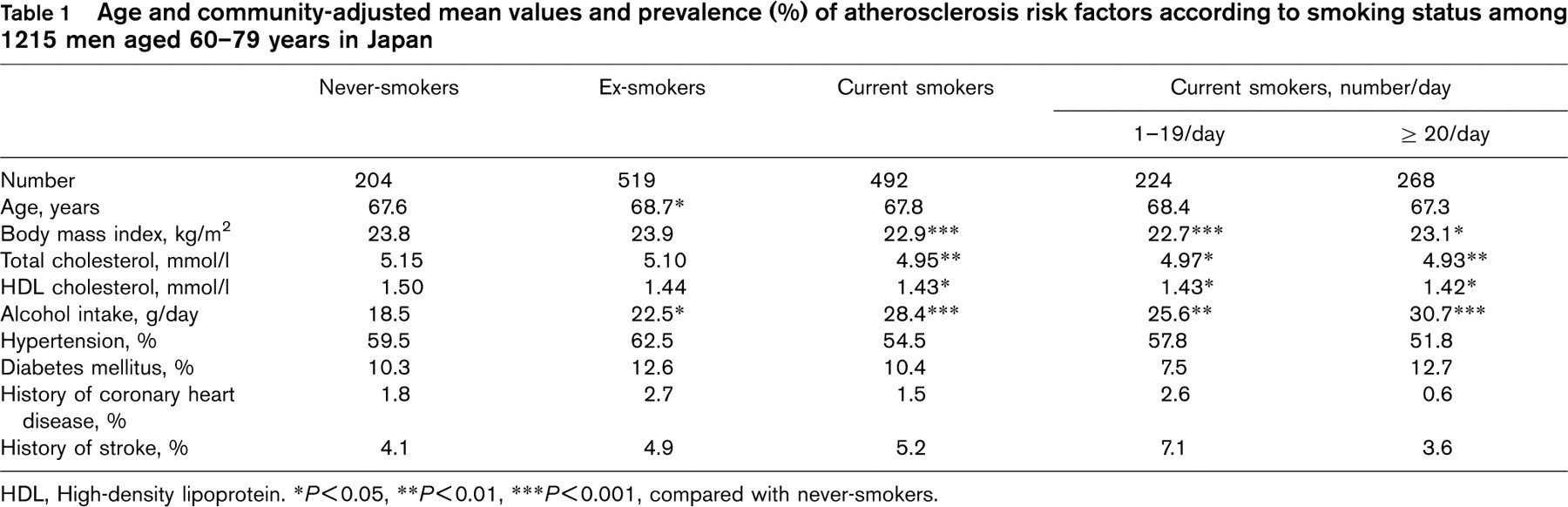
HDL, High-density lipoprotein. ∗P < 0.05, ∗∗P < 0.01, ∗∗∗P < 0.001, compared with never-smokers.
Statistical analysis
Using the analysis of covariance, we calculated the age and communities-adjusted mean values of AAI and the prevalence of low AAI (< 0.90) and atherosclerosis risk factors according to categories of smoking-status (never-smokers, ex-smokers, current smokers of <20 and ≥20 cigarettes per day), pack-years (never-smokers, pack-years <26, 26–44 and ≥45) and years since smoking cessation (current smokers, years since smoking cessation <10, 10–19 and ≥20 years, and never-smokers). Differences in age and multivariate-adjusted mean values and the prevalence of low AAI (< 0.90) were tested among four categories of smoking by the analysis of covariance. When an overall statistical difference existed, pairwise comparisons of the means and the prevalence of low AAI between never-smokers and other smoking categories were made using the t-test and chi-squared test. The prevalence odds ratios of the low AAI (< 0.90) were also calculated according to smoking categories using logistic regression analysis. A test for trend across the smoking categories was conducted by assigning median values for pack-years: 0 for never-smokers, 15 for the first smoking category, 35 for the second category, and 61 for the third category. Median values for years since smoking cessation were 0 for never-smokers, 4, 15 and 29 for less than 10, 10–19 and 20 or more years since quitting, respectively. The potential confounding factors included age (years), body mass index (kg/m2), serum total and HDL cholesterol levels (mmol/l), ethanol intake (g/day), hypertension (yes or no), diabetes mellitus (yes or no), a history of stroke and coronary heart disease (yes or no), and communities. The number of cigarettes smoked per day (0, 1–19 and ≥20) was also adjusted when we assessed the association of smoking cessation with AAI. All analyses were conducted using the SAS statistical package version 8.2 (SAS Institute Inc., Cary, North Carolina, USA). All P values for statistical tests were two-tailed, and P < 0.05 was regarded as the statistical significance level.
Results
Table 1 shows the mean age, and age and community-adjusted values of selected atherosclerosis risk factors for the four smoking categories. Ex-smokers were 1 year older than never-smokers. Current smokers had a higher mean ethanol intake, and lower mean values of body mass index and total and HDL cholesterol than never-smokers. The prevalence of hypertension, diabetes, history of stroke and coronary heart disease were not significantly different among the smoking categories. Table 2 shows the age and multivariate-adjusted mean values of AAI and the prevalence of low AAI (< 0.90) according to smoking categories. Age-adjusted mean values of AAI correlated inversely and linearly with smoking status. The prevalence of low AAI (< 0.90) was 5% (60/1215) for total subjects, and higher in current smokers than in never-smokers with no dose–response relationship with the number of cigarettes smoked. Further adjustment for body mass index, total and HDL cholesterol, ethanol intake, hypertension, diabetes, history of stroke and coronary heart disease, and communities did not alter these relationships substantially. The multivariate prevalence odds ratio of low AAI (< 0.90) in comparison with never-smokers was 3.7 [95% confidence interval (CI) 1.1–12.7] for current smokers. The relationships between AAI and pack-years of smoking are shown in Table 3. Age-adjusted mean values of AAI correlated inversely and linearly with pack-years of smoking. The prevalence of low AAI (<0.90) was higher in men with 45 or more pack-years of smoking than in never-smokers. Further adjustment for atherosclerosis risk factors did not change these relationships materially. The multivariate prevalence odds ratio of low AAI (< 0.90) in comparison with never-smokers was 4.2 (95% CI 1.2–14.6) for men with 45 or more pack-years of smoking.
Age and multivariate-adjusted mean values of ankle–arm index (AAI) and the prevalence (%) of low AAI (<0.90), and prevalence odds ratio (95% confidence interval) of low AAI (< 0.90) according to smoking status
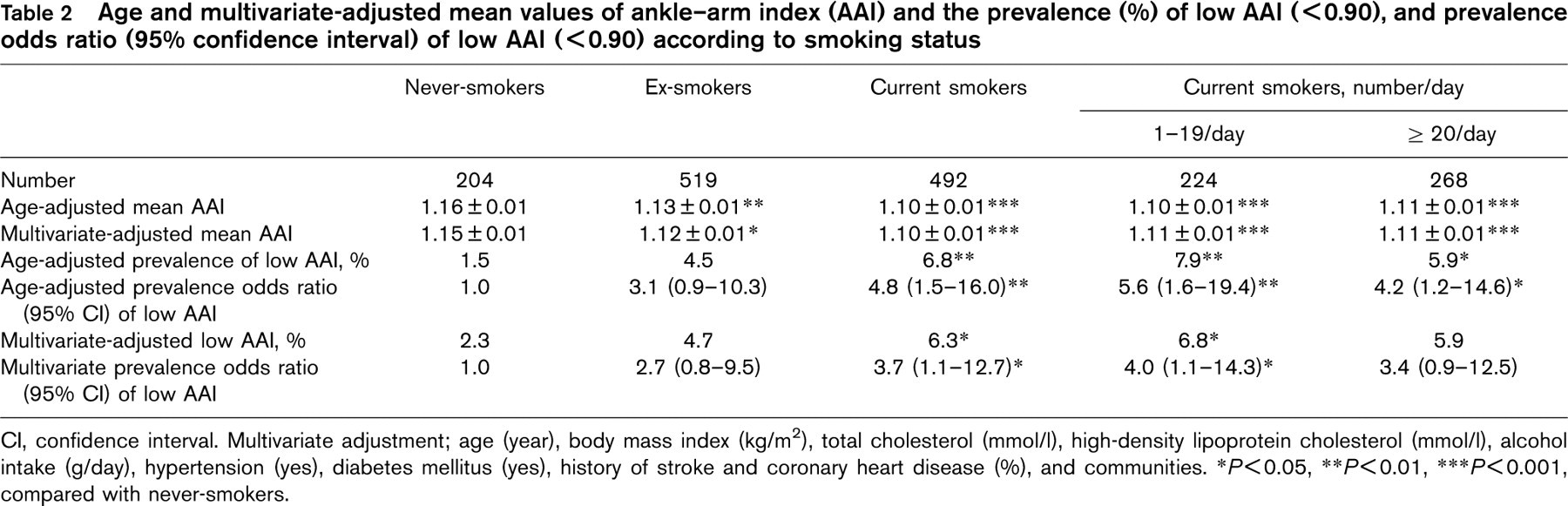
Cl, confidence interval. Multivariate adjustment; age (year), body mass index (kg/m2), total cholesterol (mmol/l), high-density lipoprotein cholesterol (mmol/l), alcohol intake (g/day), hypertension (yes), diabetes mellitus (yes), history of stroke and coronary heart disease (%), and communities. ∗P < 0.05, ∗∗P < 0.01, ∗∗∗P < 0.001, compared with never-smokers.
Age and multivariate-adjusted mean values of ankle–arm index and the prevalence of low ankle–arm index (<0.90), and prevalence odds ratio (95% confidence interval) according to pack-years of smoking
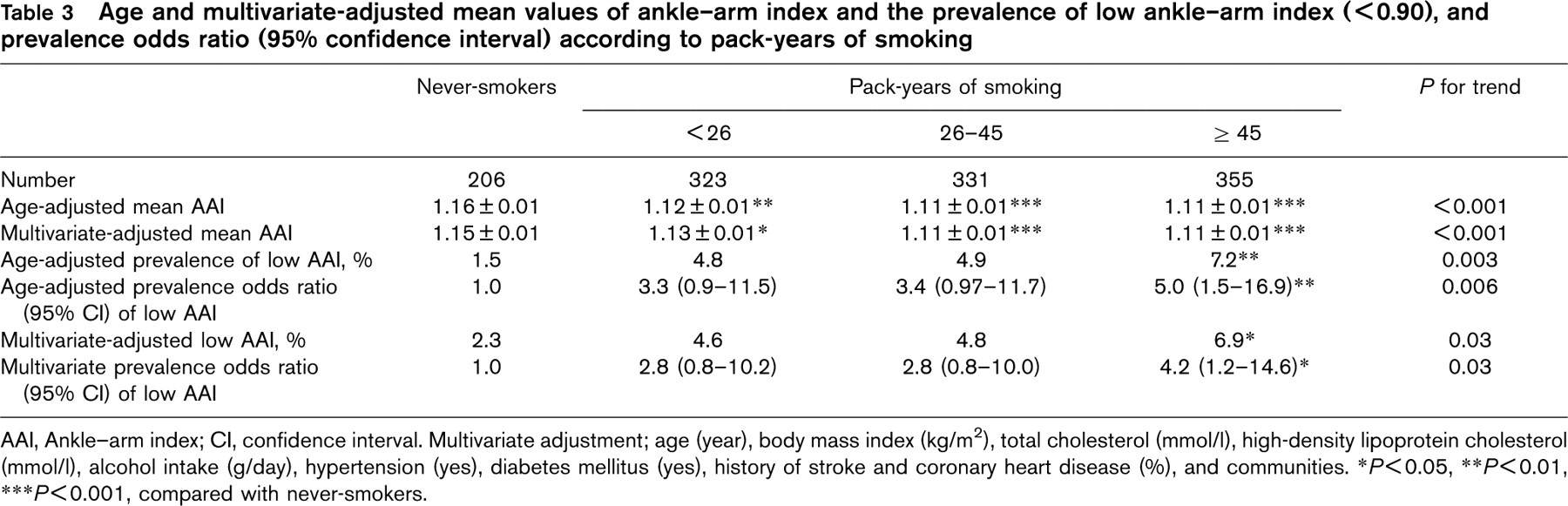
AAI, Ankle–arm index; Cl, confidence interval. Multivariate adjustment; age (year), body mass index (kg/m2), total cholesterol (mmol/l), high-density lipoprotein cholesterol (mmol/l), alcohol intake (g/day), hypertension (yes), diabetes mellitus (yes), history of stroke and coronary heart disease (%), and communities. ∗P < 0.05, ∗∗P < 0.01, ∗∗∗P< 0.001, compared with never-smokers.
We also examined the relationship between AAI and years since smoking cessation (Table 4). Compared with current smokers, age and multivariate-adjusted mean values of AAI were higher and the prevalence of low AAI was lower for men who had quit smoking 20 or more years ago, with AAI values similar to never-smokers. The multivariate prevalence odds ratio of low AAI (< 0.90) was 0.3 (95% CI 0.1–0.9) for men who had quit smoking 20 or more years ago.
Discussion
The present population-based study showed that mean AAI correlated inversely and linearly with cigarettes smoking and pack-years of smoking, and the prevalence of low AAI was higher in current smokers and men with 45 or more pack-years of smoking than never-smokers. Furthermore, we found men who had quit smoking for 20 years or more had a higher mean AAI, a lower prevalence of low AAI (< 0.90) than did current smokers, and their AAI values were similar to those of never-smokers. The latter findings suggest that the prevalence of peripheral arterial disease in men who had stopped smoking for 20 years or more is similar to that of never-smokers.
The current smokers had a fourfold higher prevalence of low AAI than never-smokers, but no dose–response relationship was found between the number of cigarettes smoked per day and a low AAI. However, the prevalence of low AAI was linearly and positively associated with pack-years of smoking. Our results are consistent with previous findings that current smoking is associated with a two to fourfold increased risk of peripheral arterial disease [1–6]. Patients with intermittent claudication, when they continue smoking, are likely to develop disabling claudication, and limb-threatening ischaemia, often necessitating surgical intervention [7, 8]. The mechanisms underlying an adverse effect of smoking on the risk of peripheral arterial disease are uncertain, although several possibilities have be proposed. Smoking may increase the risk of peripheral arterial disease because of the short-term effects of vascular construction [18] and accelerated thrombus formation through increased plasma fibrinogen concentration [19–21], increased haematocrit [22, 23] and decreased fibrinolytic activity [24, 25]. A longer-term effect is atheroma formation through direct injury of endothelial cells [26, 27] and lowering HDL cholesterol levels [21, 28].
Age and multivariate-adjusted mean values of ankle–arm index and the prevalence of low ankle–arm index (<0.90), and prevalence odds ratio (95% confidence interval) according to years since smoking cessation
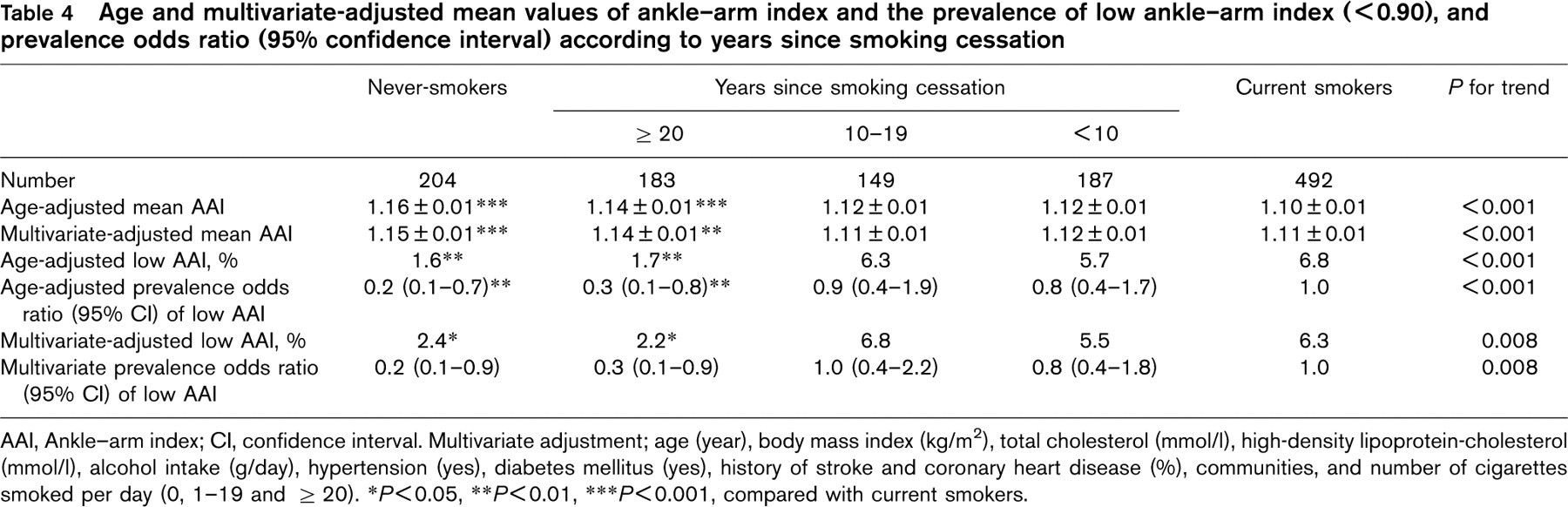
AAI, Ankle–arm index; Cl, confidence interval. Multivariate adjustment; age (year), body mass index (kg/m2), total cholesterol (mmol/l), high-density lipoprotein-cholesterol (mmol/l), alcohol intake (g/day), hypertension (yes), diabetes mellitus (yes), history of stroke and coronary heart disease (%), communities, and number of cigarettes smoked per day (0, 1–19 and ≥20). ∗P< 0.05, ∗∗P< 0.01, ∗∗∗P<0.001, compared with current smokers.
Smoking cessation can stabilize or improve claudication symptoms in patients with atherosclerotic peripheral artery disease, probably because of reduced vascular constriction and thrombus function [29]. A follow-up study of 343 patients with intermittent claudication showed no rest pain after 12 months of smoking cessation [30].
The present study showed another benefit of smoking cessation; a reduction of low AAI appeared after 20 or more years of smoking cessation. The long lag time for the appraisal of the benefit of smoking cessation on AAI may be a result of the long duration needed for the regression of atherosclerosis in peripheral arteries. The short-term effects of smoking cessation, namely reduced vascular constriction and prothrombotic status, are unlikely to be associated with low AAI or peripheral arterial disease. This implication is supported by no dose–response relationship between the number of cigarettes smoked per day and low AAI. A low AAI is also a marker of vascular stiffness rather than atherosclerosis [31].
The strength of the present study is that we first examined the relationship between AAI and smoking cessation in a population-based sample. The weakness of the study is, however, that we could not establish a causal relationship because of the cross-sectional design. In addition, the study included a limited number of subjects with low AAI.
In conclusion, we confirmed that current smoking and pack-years of smoking were associated with the prevalence of low AAI, an indicator of peripheral artery disease. In addition, we found that smoking cessation for 20 years or more was associated with the normalization of AAI, suggesting the regression of atherosclerosis in peripheral arteries. This finding needs to be confirmed by a prospective study.