
Abstract
Basic and practical information related to equipment, methodology, exercise protocols, conduct of the test and quality control issues for cardiopulmonary exercise testing (CPET) will be addressed in this II part of the statement. CPET users have the responsibility for assuring that measurements remain accurate. CPT, especially when it features breath-by-breath gas exchange analysis, requires meticulous attention to calibration procedures to assure accurate and reproducible measurements. Skills and knowledge of personnel for supervision and test interpretation, as well as patient preparation and information are key features for a correct CPET conduction: all these issues will be faced. Finally, after the test, the investigator needs to format the results in a manner that optimises the ability to discriminate essential response features; that is, to establish ‘interpretive clusters’ of the variables of interest. An example of a cardiopulmonary summary exercise test data report will be provided, defining the most important information that should be incorporated in a final report. Eur J Cardiovasc Prev Rehabil 13:300-311 © 2006 The European Society of Cardiology
Why cardiopulmonary exercise testing in chronic heart failure?
Exercise limitation with dyspnoea, and fatigue which occurs at low level of effort or even at rest, are cardinal symptoms of chronic heart failure (CHF). Based on these characteristics, the current definition of this clinical condition is a syndrome where cardiac and peripheral compensatory mechanisms are activated, to partly or fully compensate for impaired left ventricular (LV) performance. There is a wide range of exercise capacity in patients with reduced left ventricular ejection fraction (LVEF), with some patients having a near-normal peak exercise capacity. Fatigue and dyspnoea on exercise are not simply related to cardiac factors but several mechanisms are involved [1], including the central role of peripheral skeletal muscle changes (i.e. early muscle acidification), described by abnormal cardiopulmonary exercise testing (CPET) results [low maximal oxygen uptake (Vo2max) and disproportionate increase in minute ventilation (VE) at submaximal and peak work loads] (Table 1).
The exertional increase in ventilation is secondary to the CO2 increase. However, for the same workload and CO2 production, CHF patients show greater ventilation due to a higher respiratory rate. The VE/Vco2 slope (minute ventilation/carbon dioxide output slope) is one of the determinants of the exercise tolerance, and one of the most powerful CHF prognosticators [2, 3]. The metabolic state of skeletal muscle is centrally monitored by the activation of ergoreceptors, whose fibres, travelling in the lateral spinothalamic tract, increase ventilation and sympathetic outflow, producing vasoconstriction in distant, non-exercising vascular beds, with consequent effects on blood pressure and possibly a small increase in heart rate. They are sensitive to the metabolic state of the muscle, but their triggers are still unclear. They have the properties necessary to link the skeletal muscle abnormality to the fatigue, dyspnoea, hyperpnoea, and sympathoexcitation characteristic of CHF. This ‘muscle hypothesis’ proposes another cycle of deterioration similar to that of neuroendocrine activation (Fig. 1) [4]. A reduction in left ventricular function sets in motion a series of metabolic events that leads to wasting of skeletal muscle and resultant abnormalities of muscular metabolism and function.
Predictors of exercise intolerance (Vo2peak) or increased ventilatory response to exercise in chronic heart failure (CHF)
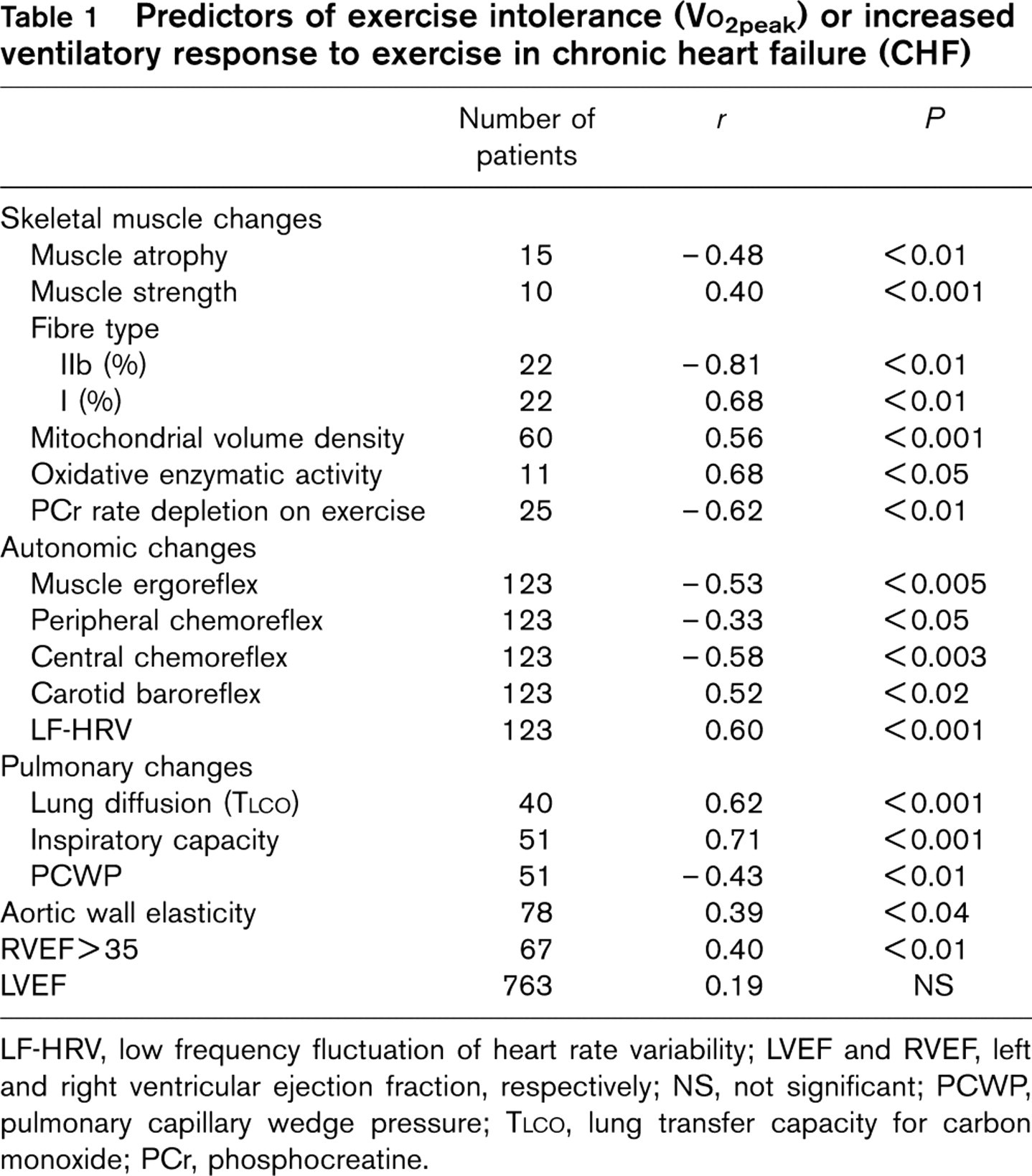
LF-HRV, low frequency fluctuation of heart rate variability; LVEF and RVEF, left and right ventricular ejection fraction, respectively; NS, not significant; PCWP, pulmonary capillary wedge pressure; TLCO, lung transfer capacity for carbon monoxide; PCr, phosphocreatine.
In response to early metabolic distress in exercising muscle, an exaggerated ergoreflex activation occurs that is perceived by the patient as both muscle fatigue and dyspnoea and that leads reflexively to excessive sympathetic vasoconstrictor drive to non-exercising beds and increased ventilatory drive in response to exercise.
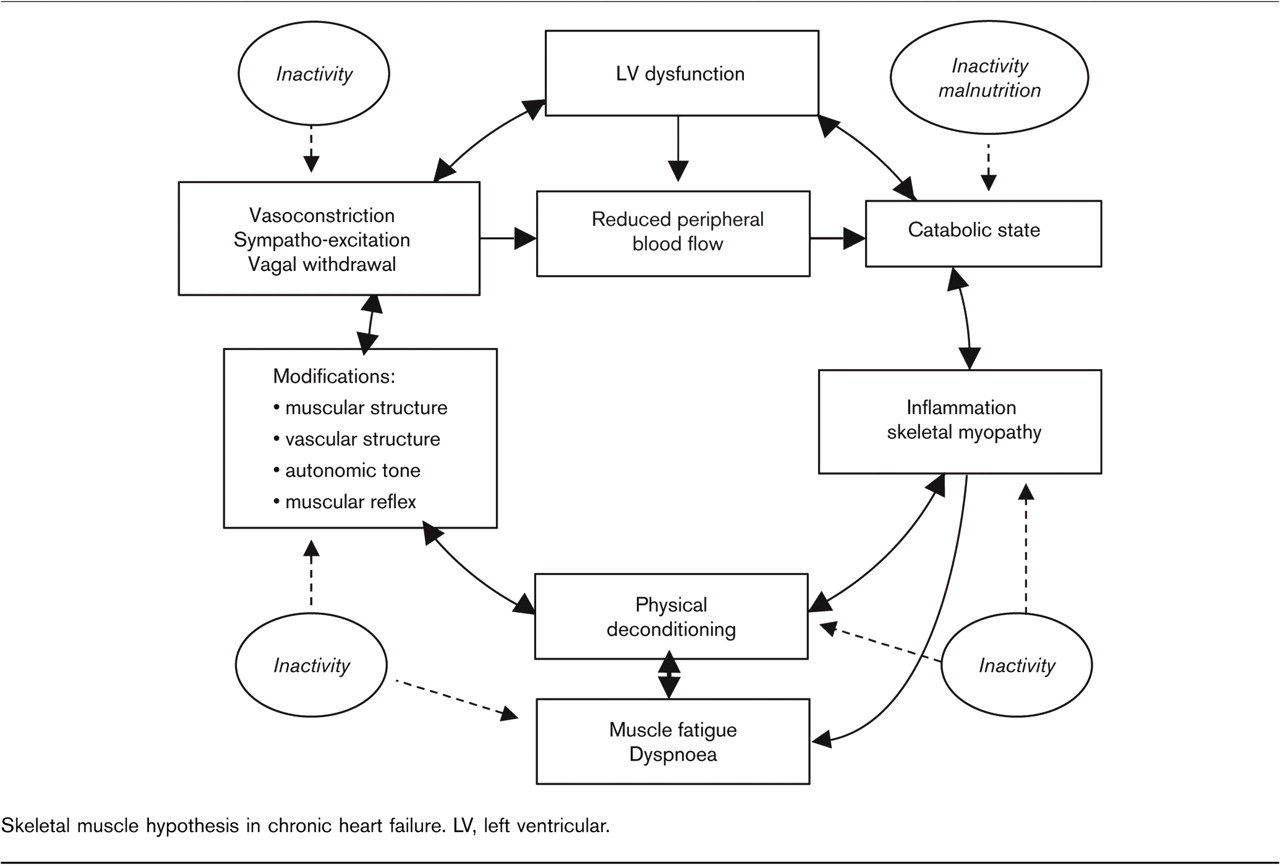
Skeletal muscle hypothesis in chronic heart failure. LV, left ventricular.
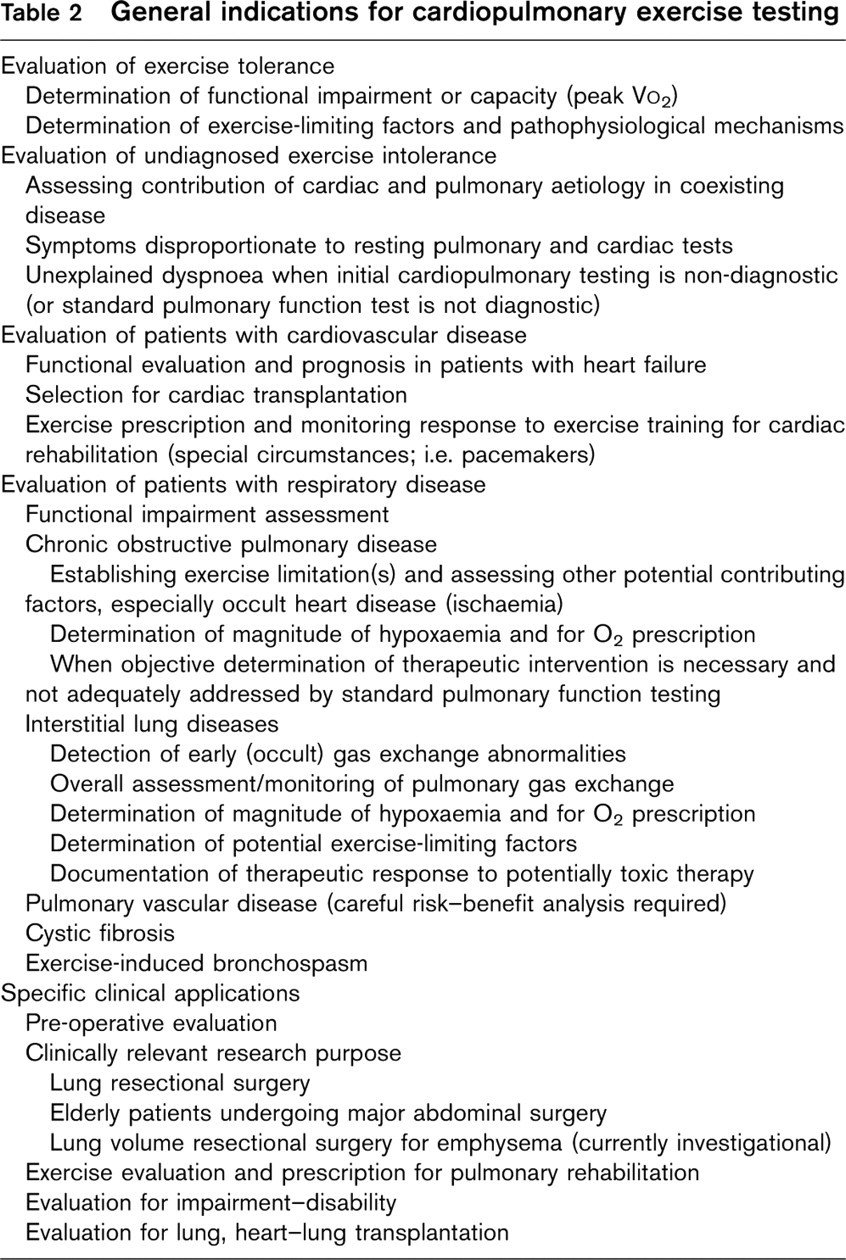
General indications for cardiopulmonary exercise testing
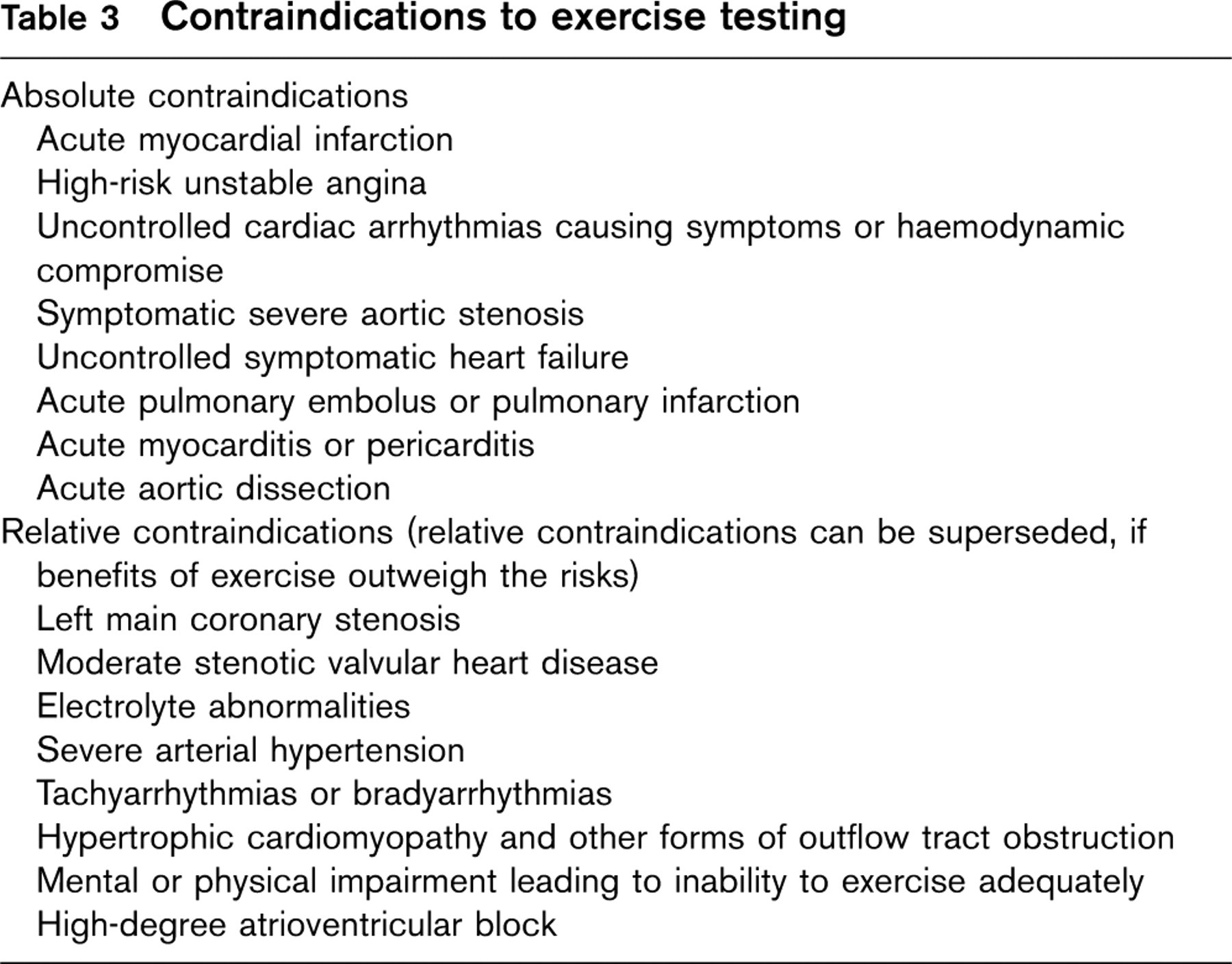
Contraindications to exercise testing
Indications for terminating exercise testing
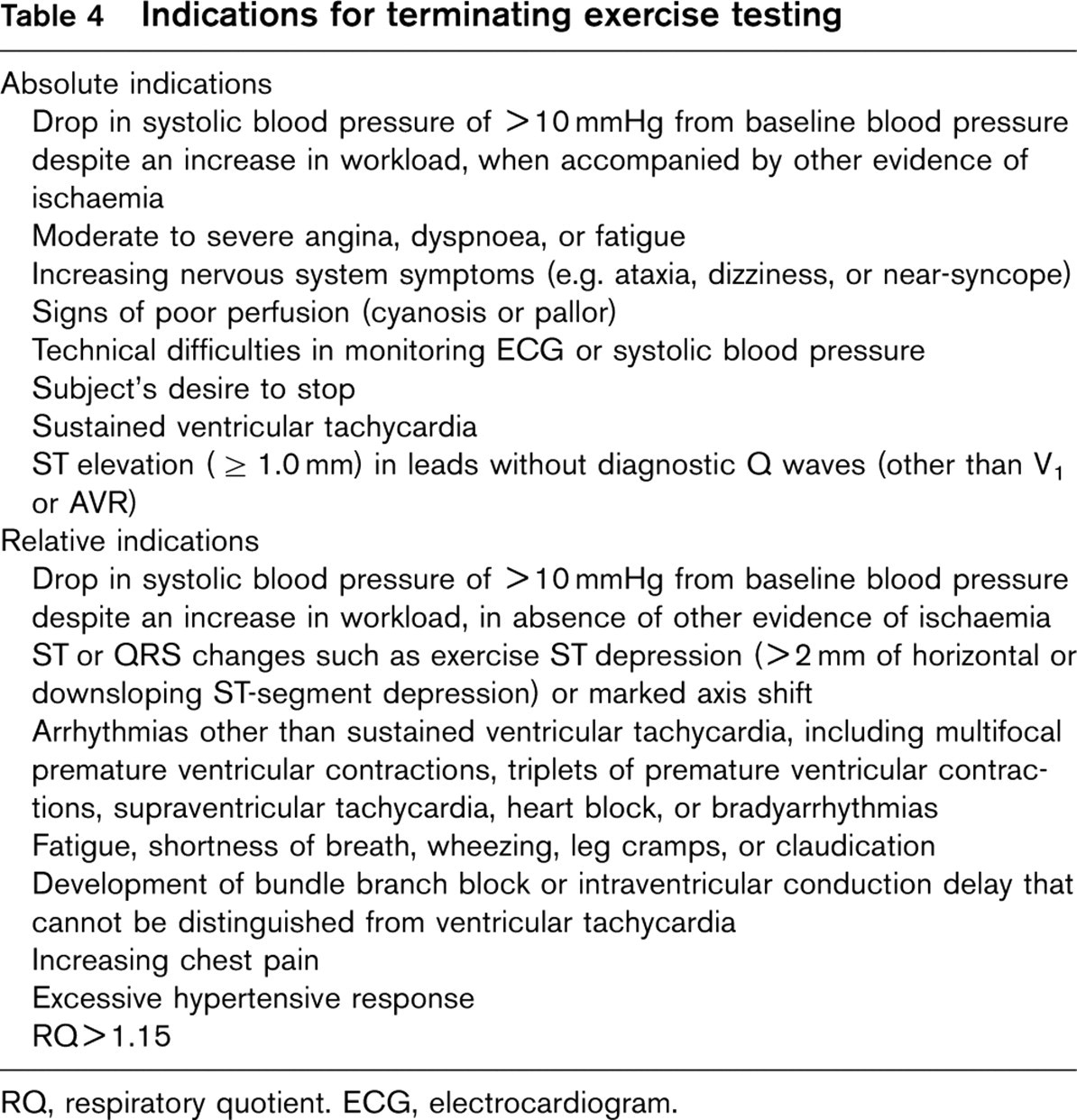
RQ, respiratory quotient. ECG, electrocardiogram.
Traditional exercise electrocardiogram (ECG) stress testing does not provide reproducible indications of exercise intolerance. For this the CPET has been introduced in the functional assessment of CHF patients, for risk stratification and therapeutic choices. General indications for CPET are listed in Table 2.
Safety first: risk and contraindications
In general, symptom-limited CPET is a relatively safe procedure [5]. Absolute and relative contraindications to testing have been revised by the American College of Cardiology/American Heart Association (ACC/AHA, 2002) and should be ruled out by reference to medical history and physical examination (Table 3). Although CPET performance in CHF patients is commonly limited by fatigue or shortness of breath, it should be recognized that other end-points are strongly preferred (Table 4).
Environmental conditions
The laboratory in which the CPET is carried out should have room enough for all the required equipment plus allow easy patient access in the case of emergency. The resuscitation and exercise equipment must be arranged so as to facilitate cardiopulmonary resuscitation in the space immediately adjacent to the exercise equipment. All clinical exercise stress laboratories should be equipped with some type of alarm so that the help of nearby personnel can be summoned speedily. Table 5 provides a detailed list of the necessary equipment and personnel for a CPET laboratory.
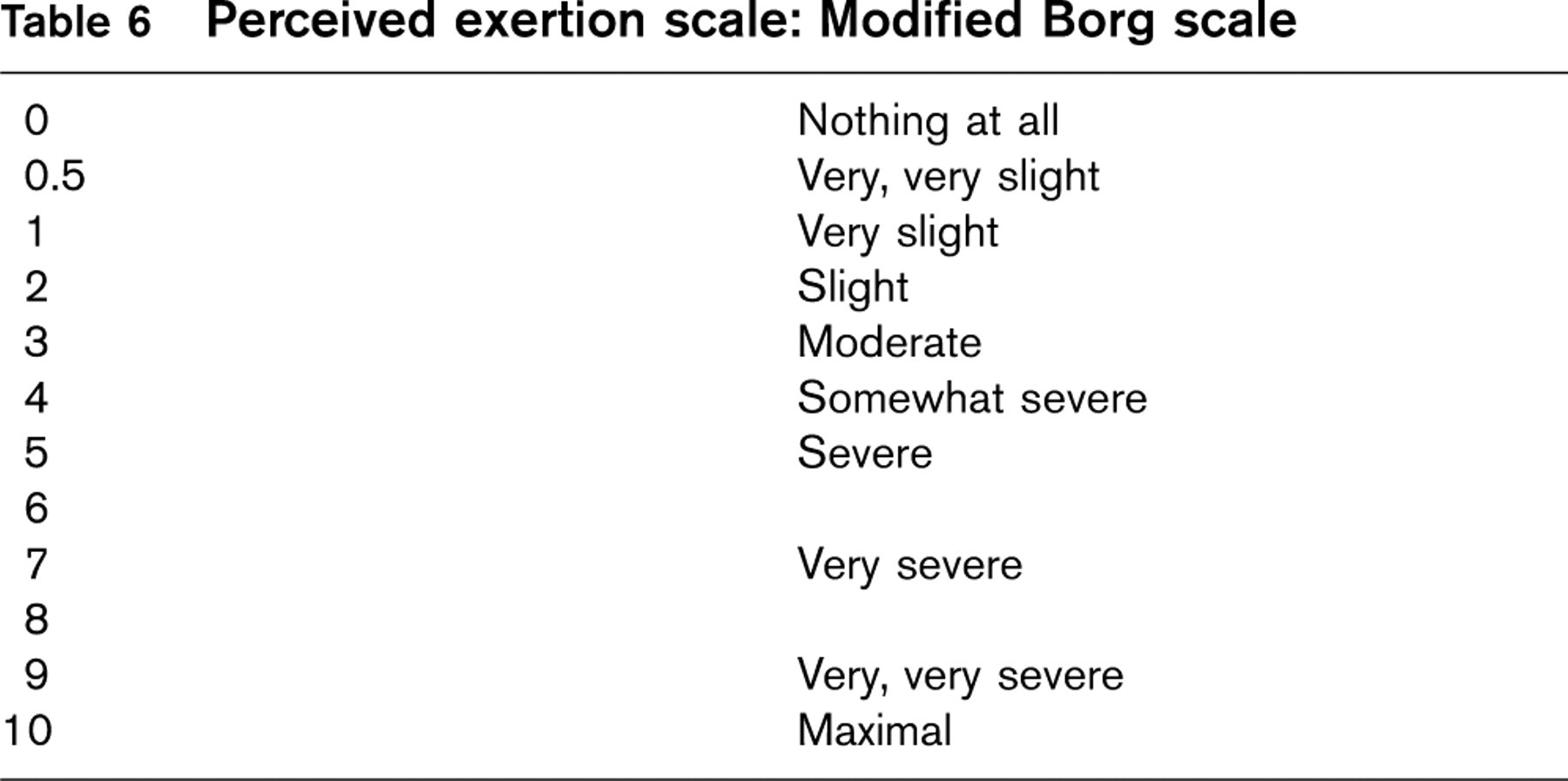
The laboratory should be well illuminated, with temperature and humidity control: a barometer station with thermometer and hygrometer are required for calibration of the gas-exchange analyser and control of environmental conditions. Generally, a temperature of 22°C is considered adequate for exercise, although for brief spells of exercise temperatures up to 26°C are acceptable if there is adequate circulation of fresh air. A table for evaluating the perceived effort should be clearly visible so that the intensity of the exercise performed can be defined precisely [6] (Table 6). Analogue scale tables can be used to evaluate the intensity of symptoms such as fatigue, dyspnoea and lower limb pain.
Ergospirometry laboratory: equipment and personnel
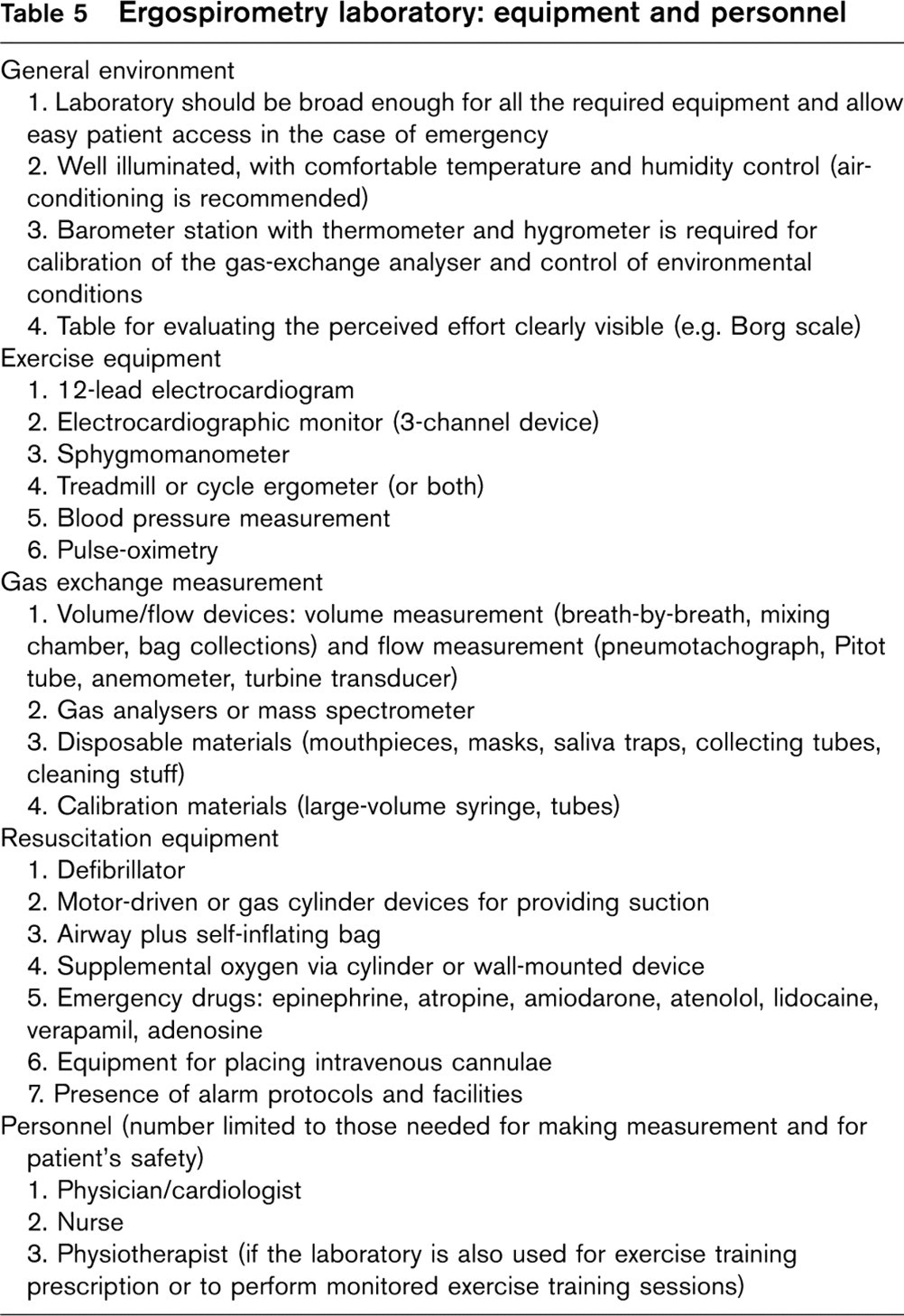
Table 6 Perceived exertion scale: Modified Borg scale
Personnel
The technique of respiratory gas measurement requires meticulous maintenance and calibration for optimal use, and skilled and trained personnel to administer tests and interpret results. The clinical laboratory should be under the direction of a cardiologist certified in advanced cardiovascular life support, with expert knowledge of exercise physiology and with training in calibration, quality control, performance and interpretation of cardio-pulmonary exercise testing. Skills and knowledge necessary for supervision and to interpret the exercise test are reported in the ACC/AHA clinical competence statement [7]. The number of procedures necessary to ensure competence has not been established by objective criteria. For a cardiologist who finished training without the opportunity for formal training on CPET, 3 years’ (minimum 150 procedures) experience may be necessary in lieu of formal training. Continuing competence in CPET requires regular, continued performance: performance of only a rare test can lead to missed or inappropriate interpretation. The appropriate number of exercise tests that individuals should perform to maintain competence in supervision and interpretation has not been established (by evidence-based criteria). Because of the amount of data needed for interpretation of metabolic measurements, meticulous post-test computer processing is necessary. The ACC/AHA clinical competence statement [7] acknowledges that two physicians may collaborate to ensure the proper performance of cardiopulmonary exercise testing in clinical practice: one to supervise the test and the other to interpret the results. The first has responsibility for conducting the test and, due to the characteristic of CHF patients, he/she should be present during the entire test procedure, to observe the patient continuously, so as to be able to respond in case of emergency. The presence of the latter is not strictly required. Beside physicians, staff may include a properly trained nurse, exercise physiologists, physical therapists or specialized medical technicians. The number of persons present in the laboratory is determined by measurements to be carried out (assessment of invasive parameters in exercise, e.g. lactic acidaemia or blood gas analysis) and by the patient's clinical condition.
Patient preparation and information
Patient collaboration is essential to optimize the clinical–diagnostic value of CPET. Usually, if patients are adequately informed and instructed, they will perform the maximum effort possible in relation to their condition, thus providing adequate information and enabling a reliable interpretation of the test. For this reason, the patient should be prepared carefully [8] (Table 7): in order to obtain homogeneous information from the test and reduce patient anxiety to a minimum, it is advisable to give the patient both written (before the test) and oral (during the test) information. In the preliminary phase, it is important to establish a simple and effective mode of communication, given that use of the mask or mouthpiece makes it impossible for patients to express themselves: the patient's attention should be drawn to the tables for evaluating level of symptoms and intensity of exercise performed (Table 6). The patient is also required to undergo a session of familiarization with the equipment (Table 7). Complete spirometry assessment with determination of the maximum voluntary ventilation (MVV); blood gas analysis at rest, in the case of suspected hypoxaemia; blood cell count; and knowledge of the pharmacological treatment can support CPET interpretation (Table 7). Finally, information on the patient's habitual level of physical activity will help in choosing the most appropriate exercise protocol.
The patient should abstain from smoking at least 8 h before the test. A light breakfast is usually allowed 2 h before the test.
Pre-test information: what should be known before CPET for appropriate conduction of the test.
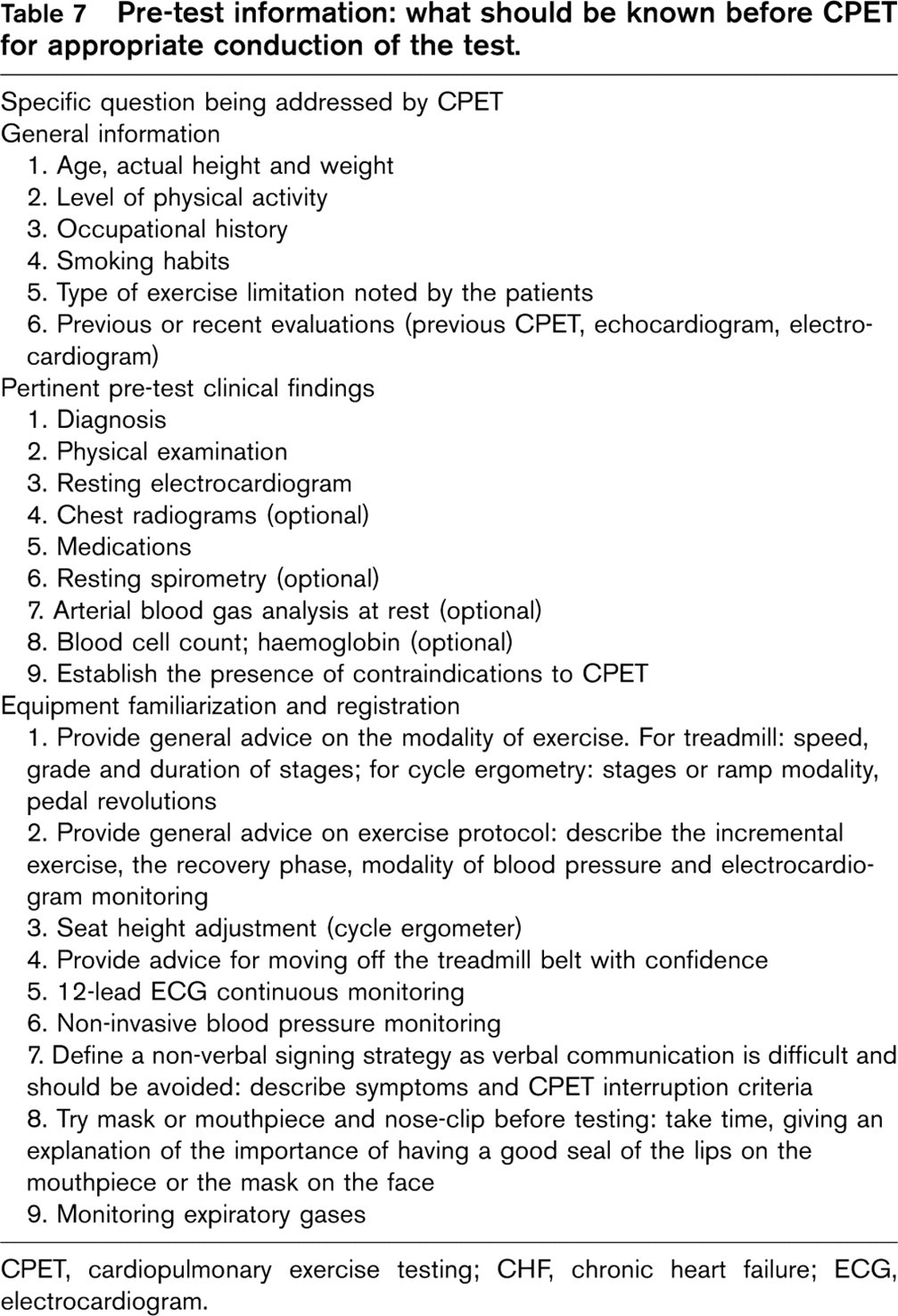
CPET, cardiopulmonary exercise testing; CHF, chronic heart failure; ECG, electrocardiogram.
Equipment
The proper interpretation of CPET data depends on accurate data collection and correct calculation: consequently, an adequate knowledge of exercise equipment and the mode of test conduction is a fundamental prerequisite for optimal clinical utilization of CPET.
Collection of expired ventilation
The measurement of VE during exercise requires that the patient's mouth and nose be sealed tightly with a clip and a mouthpiece, so that all inspired and expired are routed to the breathing valve.
Gas is sampled through a facial mask or a mouthpiece. A mouthpiece, with a nose-clip, is the equipment of preference because of the lack of leaks, especially at high levels of ventilation. However, this is uncomfortable for the patient, stressful, and generates hypersalivation. Face masks are better tolerated, but it is often difficult to rule out leaks at high levels of exercise.
The ideal breathing valve prevents contamination of inspired and expired gas, has no resistance to breathing, low valve dead space, low size and weight, does not generate turbulence in the air stream, is easy to clean and sterilize, and is not expensive. No single valve design is ideal. The available breathing valves have three ports, for inspired, expired air and the patients, respectively, and all have a dead space volume. An appropriate balance between dead space volume and valve's resistance is desirable: while for a healthy, fit subject a low-resistance valve (with higher dead space) is preferred because of the high levels of ventilation that must be accommodated, for CHF patients a low flow-rate valve, with slightly higher resistance, may be preferable.
The dead space is usually slightly more with a mask covering nose and mouth, than with nose-clip and mouthpiece. Newer face masks have a low dead space (40 ml), are less apt to leak and are more comfortable [9].
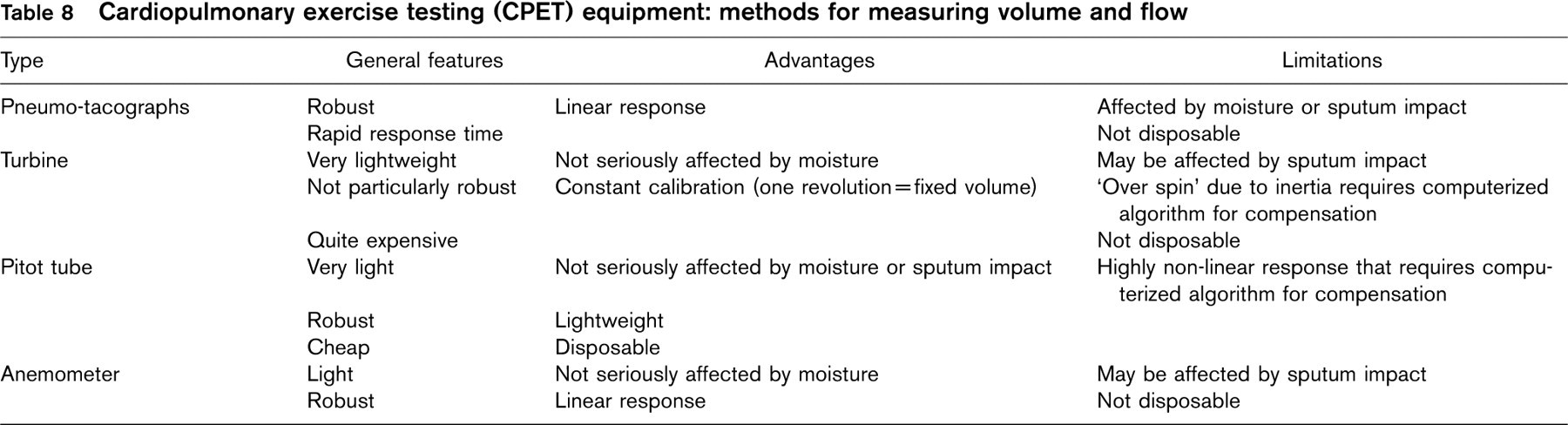
Cardiopulmonary exercise testing (CPET) equipment: methods for measuring volume and flow
Flow-sensing devices
Flow-sensing devices generate a signal that is proportional to the gas flow, which is then integrated over time to produce a gas volume. Four types of flow-sensing spirometers are used in automated metabolic charts: pneumotachometers, turbines, Pitot tubes and anemometers (Table 8). Ideal transducers must be lightweight, have low dead space, and low resistance to flow in the range of flow encountered during exercise, and be immune to the effects of water vapour or pools of saliva that may accumulate during the test.
Pneumotachometers, pressure-differential devices
These are small, resistive elements within a tube, with two small, flexible plastic tubes starting from each end of the element that connect to highly sensitive differential pressure transducers. A series of parallel capillary tubes (Fleisch type) of the resistive element generates a small pressure drop (1.2–1.3 cmH2O) as the gas passes across it: the pressure differential across the element is proportional to the gas flow. Newer pneumotachometers are relatively unaffected by position and humidity variations, and have a reasonable linear response in their functional range [10, 11]. For exercise testing in healthy adults and CHF patients, a No. 3 Fleisch pneumotachograph is appropriate, as this device has a linear response for flows up to 5–10 l/s [12]. Disadvantages of pneumotachometers are that they can be affected by changes in gas temperature and composition: contact of expired air with the pneumotachograph at ambient temperature could result in condensation which, by obstructing the element's tubes, may alter the calibration profile of the device and introduce substantial measurement errors. Adequate and constant warming of the pneumotachograph prevents these problems.
Turbines
These generally use a very lightweight, low resistance, rotating vane or impeller inside the flow tube to measure the gas flow. Each rotation of the vane at the very high flows is detected by a photocell device, and the number of interruptions of the light beam is counted and summed to provide the gas volume. Turbines are relatively insensitive to changes of temperature, humidity and gas composition, but may have linearity problems caused by friction and inertia of the vane.
Pitot tube
This is a device for measuring flow velocity in fluids: the difference in pressure is measured at an opening placed directly facing the fluid stream compared to the pressure at an opening perpendicular to the fluid (static pressure). From Bernoulli's law, the velocity of the fluid movement is proportional to the square root of the pressure difference, and, from the cross-sectional area of the device, the flow can be calculated. The advantage of Pitot tube is to be non-resistive: their alinearity and sensitivity to changing composition of inspired and expired gases requires sophisticated corrections to linearize their output [13].
Anemometer (mass flow sensors)
They rely on the cooling effect caused by laminar gas flow [14, 15]. As gas passes over a very thin, heated wire, the temperature of the wire drops in proportion to the mass and flow of the gas, thus more current is supplied by the feedback circuit to maintain the wire at a constant preset temperature. The supplied current is proportional to the gas flow and is integrated over time to provide gas volumes.
Gas analysers
They allow accurate determination of oxygen consumption, both the fractional concentrations of oxygen (forced expiratory oxygen, FEo2) and carbon dioxide (forced expiratory carbon dioxide, FEco2).
Mass spectrometer
This is an extremely rapid and very accurate analysing device, but its use is impossible in many laboratories because of high cost, size and maintenance. Sampled gases are converted to positively charged ions by an electron beam, accelerated by an electric field and subjected to a magnetic environment: the direction of the ions in the magnetic field is dependent on their mass/charge ratios. The different ions, representing different gases, are detected by appropriately located detectors, each of which produces a high-voltage output proportional to the number of ions that strike the collector per unit time.
Oxygen analysers
Currently, three types of oxygen analysers are commonly used in modern metabolic carts, using several different principles.
Polarographic electrodes, or galvanic ‘fuel cells', are designed to produce a stable current that is proportional to the pressure of oxygen: these electrodes are small, making them suited to portable systems, but they have a short lifetime (6–12 months) and some stability problems [16].
Paramagnetic analysers are the most common type available; these utilize the paramagnetic properties of oxygen, that, in a sample gas, causes the rotation of a nitrogen-filled glass dumb-bell suspended in a magnetic field [17]. The amount of rotation, or the current needed to cancel this rotation, is directly proportional to the oxygen concentration of the sample. These analysers are stable, require little maintenance and have a response fast enough for breath-by-breath studies.
Cardiopulmonary exercise testing (CPET) equipment: methods for metabolic measurement

Zirconia fuel cells use an electrochemical galvanic cell, consisting of a calcium-stabilized oxide electrolyte with porous platinum, which acts as a semipermeable membrane that is selective for oxygen ions. These analysers are both precise and stable, and require little maintenance.
Carbon dioxide analyser
The most modern analysers rely on the fact that carbon dioxide absorbs infrared radiation. Infrared light passes through a cell containing a given amount of carbon dioxide, and the volume of light transmitted is compared with a known constant value. The difference is proportional to the fractional CO2 concentration in the sample.
Metabolic measurement techniques
Three methods for assessing minute ventilation (VE), oxygen consumption (Vo2) and carbon dioxide production (Vco2) are available: the Douglas bag, mixing chamber and breath-by-breath mode (Table 9).
Bag collection
This is the gold standard. It can be performed with simple equipment, requiring the measurement of large gas volumes (variable-sized bags are adopted, usually of capacity 100–300 litres) and assessment of gas concentration without the need for rapidly responding analysers. The basic technique involves collecting expired air into a collection bag and, after a known period of time, the concentration of oxygen consumption (O2) and carbon dioxide (CO2) are measured, and Vo2 and Vco2 are calculated [18, 19].
Mixing chamber
The expired air passes into a baffled chamber (usually of capacity 5–15 litres) and the concentration of O2 and CO2 are measured continuously at the distal end of the mixing chamber. Expired volume is also measured continuously with the above-mentioned flow devices, and the averaged (every 15–20s) concentration of expired gas and corresponding volume are used to calculate Vo2 and Vco2, averaged over 30–60s [20, 21]. For incremental exercise testing, VE and expired O2 and CO2 concentrations change slowly and, therefore, the accuracy and fidelity of a well-designed, fixed volume mixing chamber may comparable to those of the breath-by-breath systems [22].
Breath-by-breath method
This method samples airflow and concentration during each breath, to obtain inspired and expired volumes of O2 and CO2 per breath. The CO2 output and O2 uptake during each breath are calculated, and the cumulated totals of all breaths over a countable time are reported as Vo2 and Vco2 [23]. To make accurate measurements, VE and gas concentrations must be determined as near to continuously as possible. The flow measurement occurs nearly instantaneously, whereas gas concentration signals are delayed by the transit time of the gas along the sampling tube into the instrument. When performing a breath-by-breath integration, it is important to temporally realign the gas concentration and flow signals [24, 25]. Breath-by-breath data collection and analysis is the most popular: the confidence of this method depends on the algorithms developed and implemented to correct the combined measurement errors for each of the determined variables [26–28].
Gas exchange measurements and calculations
Bag collection, mixed chamber and breath-by-breath methods all utilize the same set of basic equations to calculate Vo2 and Vco2. The following equations are used:

VI, VE, and VO2 indicate timed collections of volumes (inspired and expired) and gas, FIO2 and FEO2 represent the O2 concentration in the inhaled and ‘mixed’ exhaled gas, respectively, t is the time period of gas volume measurement. This equation has both inspired and expired gas volumes, but only one of these volumes needs to be measured, usually expired volume:
VI (STPD) =VE (STPD)xFEN2/FIN2

where FIN2 is inspired N2 concentration and FEN2 is the mixed expired N2 (in the bag) while STPD stands for standardized to standard temperature (0°C), barometric pressure at sea level (101.3 kPa) and dry gas.
Calibration procedures and quality control
Gas-exchange analysis is an imperfect science. Considerable errors can occur if specific procedures are not followed to minimize them. The two main causes of errors in CPET results are errors in calibration and leaks. To ensure that obtained data are valid, the technician must possess basic skills in gas-exchange analysis, maintain quality control, and have the ability to identify errors and reasons underlying them. The errors should be recognized in the calibration before the test, as well as during the conduction of the test and while interpreting the results. A manufacturer's ability to provide a technical service should also be considered, as even the experienced user will, at times, find it necessary to contact the company's service department for assistance. Whenever possible, a service contract should be included when negotiating the purchase of a metabolic system.
Periodic quality control testing often makes the assumption that either the metabolic measuring equipment or the ergometer is operating properly. For instance, it is common to validate metabolic systems by having a normal subject exercise at a given fixed intensity while measuring expired gas and volumes, and comparing obtained values with those expected at the work-intensity setting [29, 30]. If the ergometer is not properly calibrated, an ‘error’ would be detected in the metabolic measurements.
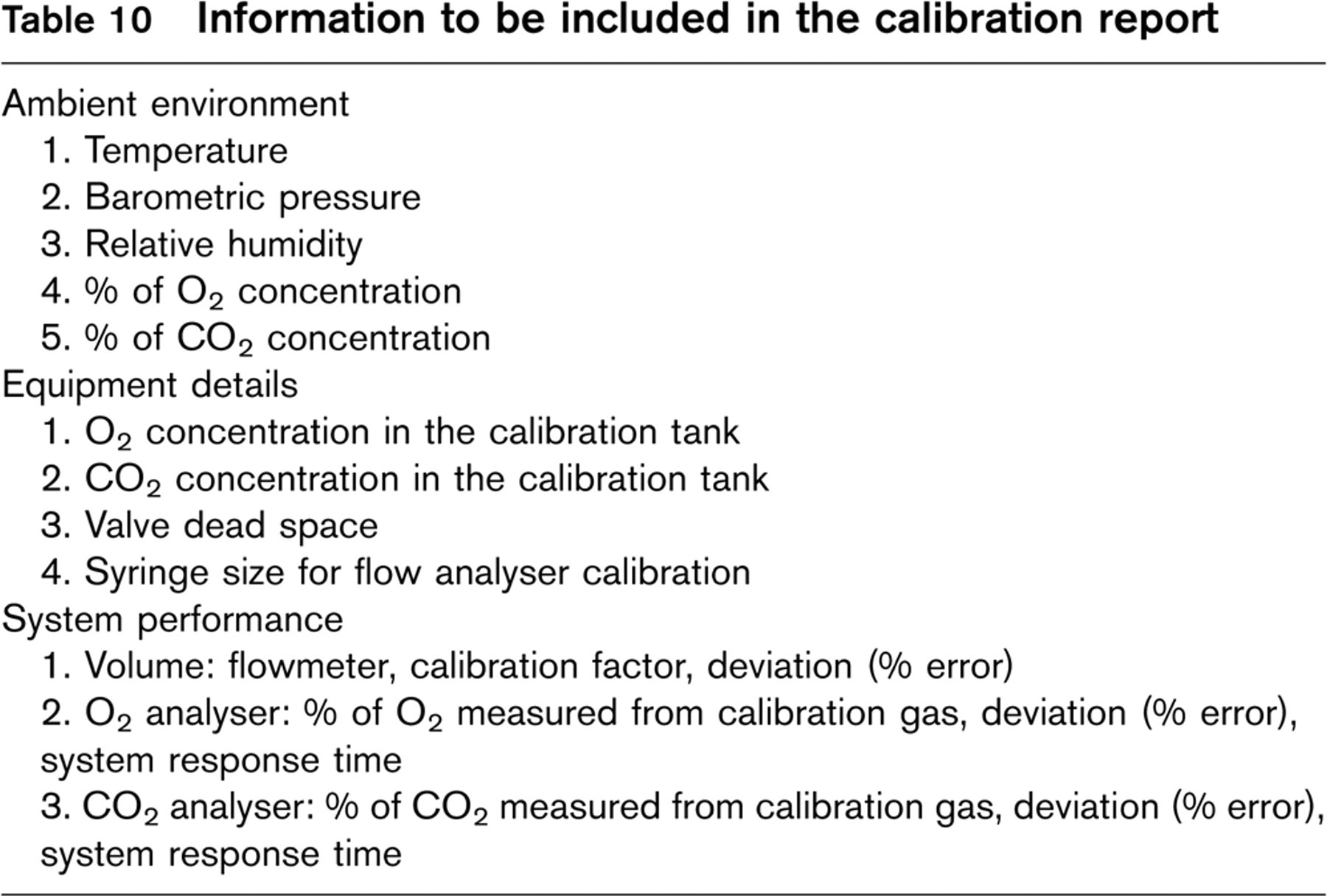
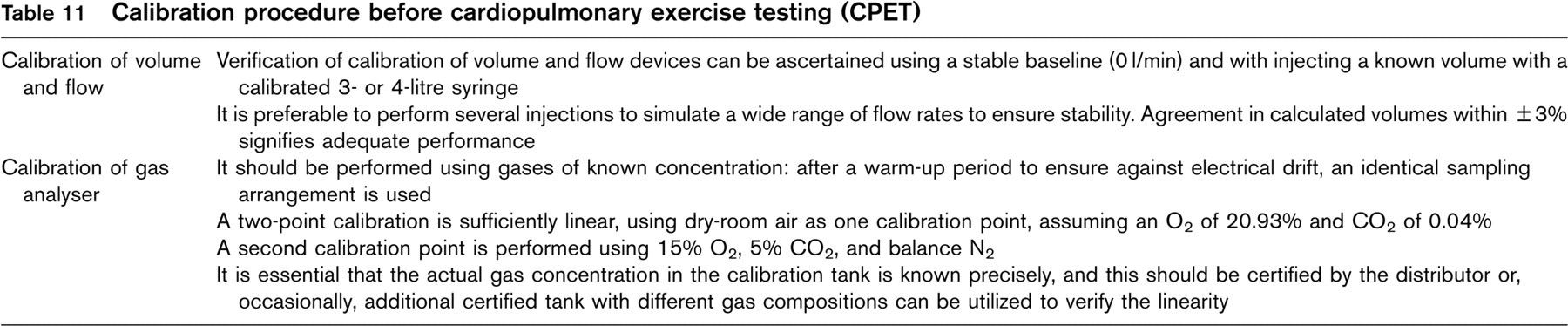
A good practice is to calibrate the system daily and to compile a calibration book so long-term trends can be monitored. The calibration report should include the documentation of ambient environment, and accuracy of airflow and O2 and CO2 analysers (Table 10). Daily calibration begins with the determination of ambient barometric pressure, temperature, and relative humidity; thus, it is necessary to have a barometer, thermometer and hygrometer in the laboratory. The procedures of calibration of volume and flow devices and gas analyser before CPET are reported in Table 11. Other calibration procedures need to be performed, but on a less frequent basis. Bicycle ergometer and treadmill should calibrated yearly.
Analysis of the resting phase is important and provides some insights. It is necessary to wait 3–4 min of resting while gas exchange is measured to ensure stability. Baseline Vo2 should be between 3 and 5 ml/kg per min but lower values can be found in patients with severe heart failure, the respiratory exchange ratio (RER) should be below 0.90, if the ventilation is ventilating correctly. Ventilatory oscillations can be observed at this stage (Fig. 2); this is the consequence of a periodic way of breathing and is always associated with severe circulatory failure and/or pulmonary hypertension. The mechanism of this profile is not exactly known, but seems to be related mainly to very low kinetics of oxygen transport, together with increased stimulation of chemoreflexes [31], it tends to diminish or disappear during the increase in work rate [32].
kinetic parameters ± SEM of LDH (against
Calibration procedure before cardiopulmonary exercise testing (CPET)
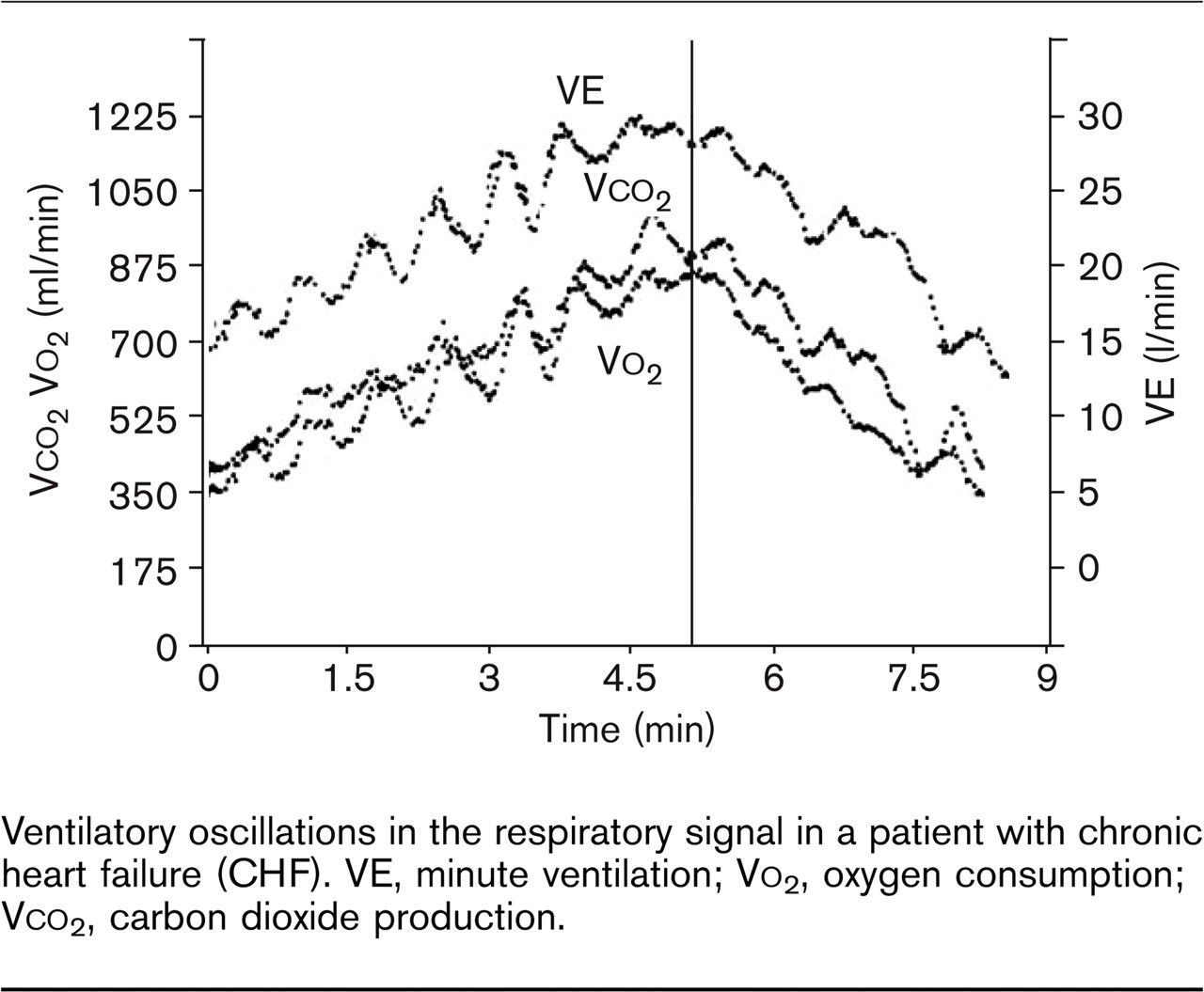
Ventilatory oscillations in the respiratory signal in a patient with chronic heart failure (CHF). VE, minute ventilation; Vo2, oxygen consumption; Vco2, carbon dioxide production.
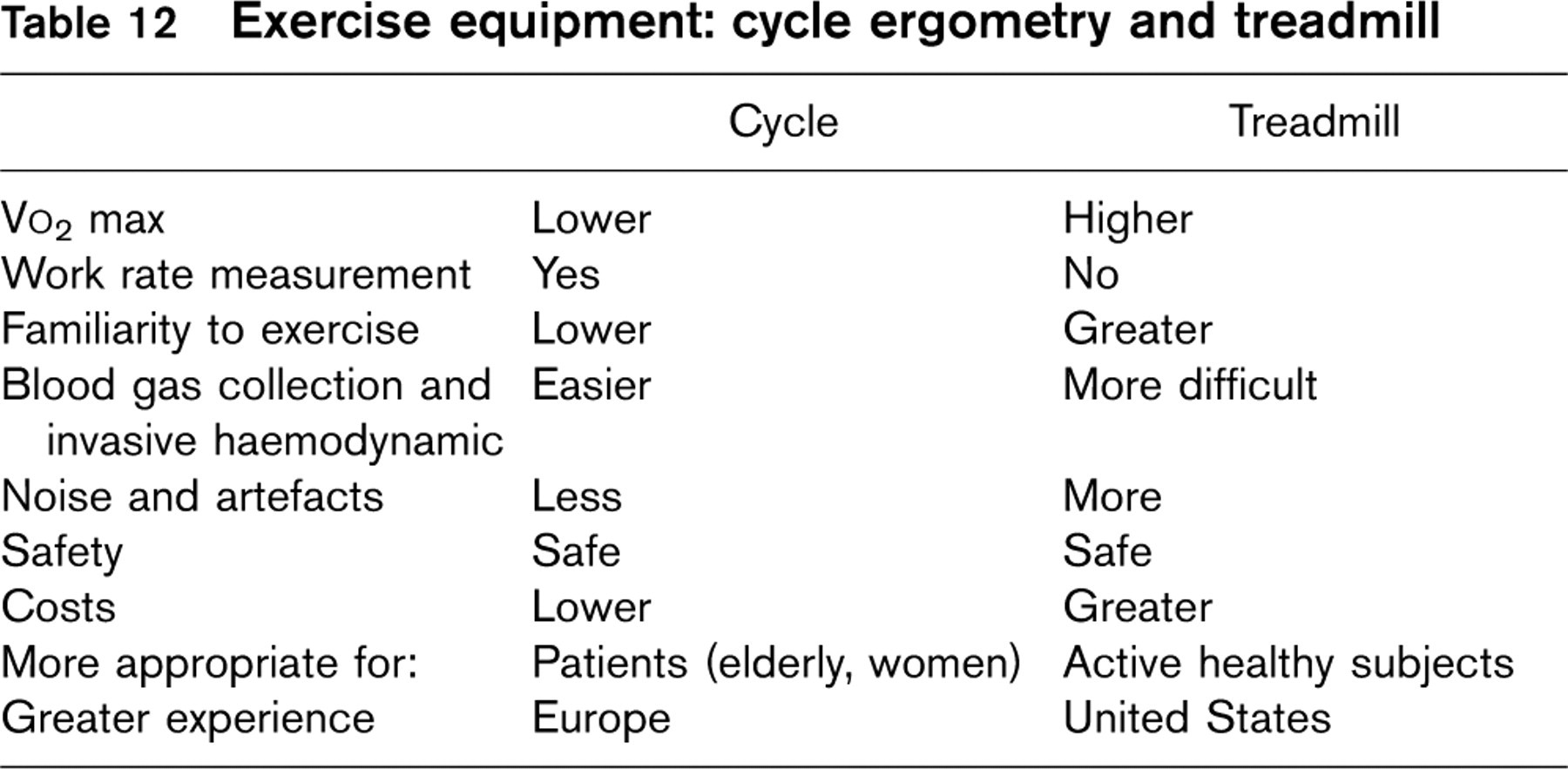
Exercise equipment: cycle ergometry and treadmill
Exercise protocols
Both treadmill and cycle ergometer devices are available for exercise testing (Table 12). The cycle ergometer is generally less expensive, smaller, and less noisy than treadmills and produces less motion of the upper body. On the other hand, treadmill exercise is a more natural form of exercise and allows a higher maximum Vo2 to be attained due to the greater influence of body weight and the additional use of the upper limbs. The type of walk can also influence the maximum Vo2. Treadmill exercise results in values of Vo2peak approximately 8–12% higher, independently of the type of protocol used. CHF patients often stop exercising on the treadmill because of dyspnoea, whereas on the bicycle, even if the main reported symptom is dyspnoea, patients generally stop exercising because of leg fatigue.
Treadmill exercise disadvantages are the monitoring of arterial pressure, ECG and Vo2 and Vco2 kinetics, and the sampling of eventual invasive parameters through blood tests, which may be problematic. For a quantitative assessment of exercise response, and to establish a level of bicycle training, electronically braked cycle ergometry may be preferable.
Generic types of protocols
Several types of exercise protocols can be used: progressive, incremental, multistage (every 3 min, with a ‘pseudo’ steady-state metabolic level at each stage). Maximal incremental protocols are used widely in clinical practice, as a progressively increasing work rate protocol enables rapid acquisition of diagnostic data. Because the response of the key respiratory variables (Vo2, Vco2 and VE) lag behind changes in work rate, it is important to adopt a protocol in which work rate increases at a constant rate.
Specific exercise protocols
Several different protocols have been proposed and adopted in clinical and research settings. The suitability of a protocol should be selected in order to maintain the exercise time between 6 and 12 min [33], considered an ‘optimal’ exercise time for obtaining efficient and useful metabolic and functional information. Both treadmill and cycle ergometer protocols should be preceded by an initial warm-up phase at 0 watts for 1–3 min, and followed by an adequate phase of recovery of at least 5 min at reduced work load. The design of the incremental protocol is important in that it can modify symptoms during exercise and substantially affect the assessment of aerobic capacity. As a consequence, the type of protocol applied should be borne in mind when interpreting the CPET.
Treadmill exercise
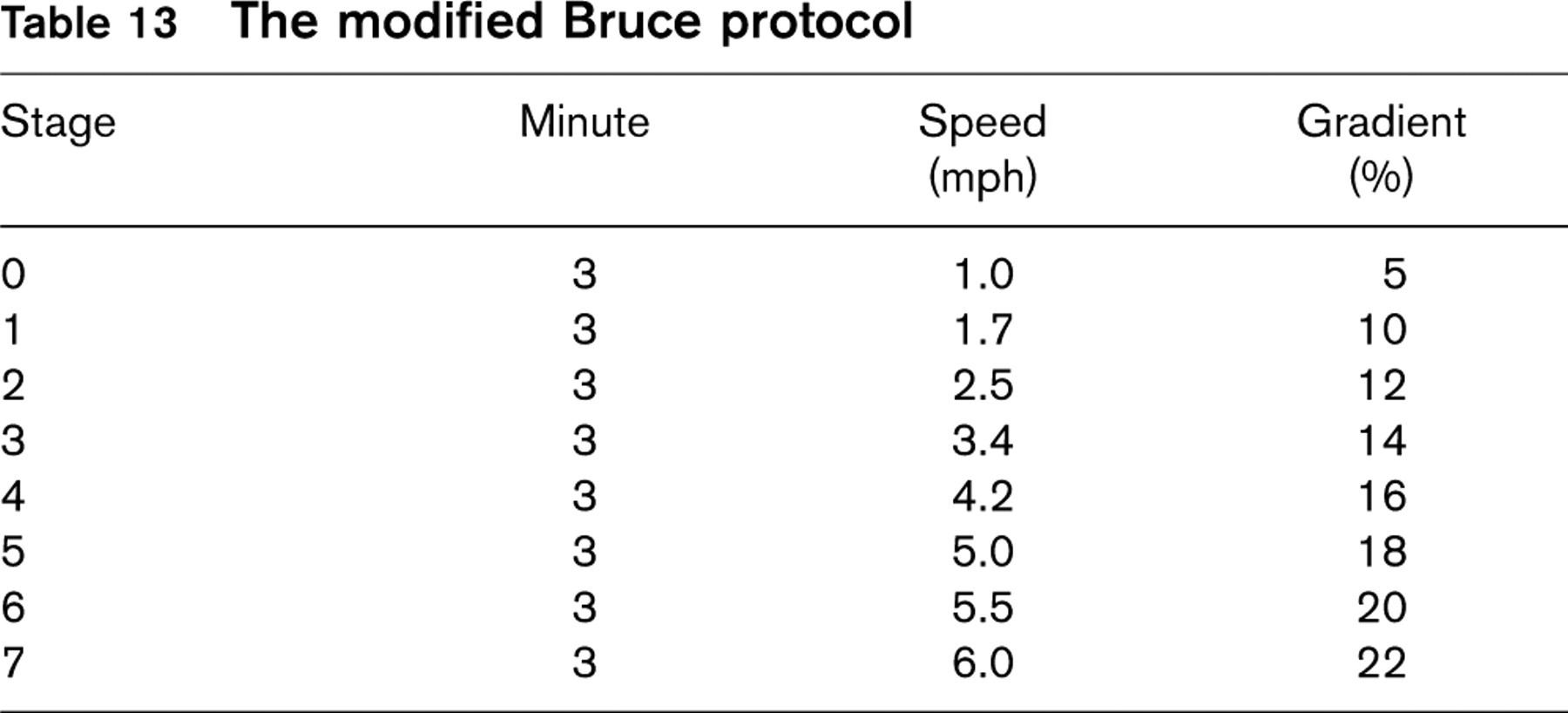
A modified Bruce protocol [with an additional stage 0: 1 mile/h (1.61 km/h), 5% gradient] [2] is universally applied because the work rate of the first stage of the classical protocol [34] (5 metabolic equivalents: METS) appears excessive for patients with CHF in the advanced class of the New York Heart Association functional classification. However, gas kinetics are disturbed by the dyshomogeneity of these workloads (Table 13).
In the Balke protocol [35], the speed is kept constant and elevation is increased by 1% every minute: the protocol has been modified repeatedly [36]. Naughton's protocol [37] may be utilized in CHF patients, as the initial work rate and subsequent increments are more than 1 but less than 2 METs. It appears from the literature that a drawback of both Balke and Naughton protocols is that the mean exercise duration is excessive.
Cycle ergometer
Using the cycle ergometer, incremental CPET can be carried out with variable workloads from 5 to 25 watts every 1–2 min, depending on the functional capacity of the CHF patient. With the introduction of computer-controlled cycle ergometers, the ramp protocol has been widely adopted in clinical practice. It consists in continuous increments of workload, each second, and is carried out on a cycle ergometer equipped with electronic breaks. In CHF patients, the ramp protocol with a cycle ergometer is equivalent, in terms of the cardiopulmonary and metabolic response and total mean duration of exercise, to the step protocol with small increments of workload (5–10 watts every 1 min).
Modality of performance: how to conduct the test
Personnel
Exercise testing should be conducted by personnel with a basic knowledge of exercise physiology. This should include: (1) the physician also involved in the clinical care and follow-up of the patients (preferably a cardiologist); (2) a nurse or a technician (with specific skill and experience in CPET and prompt emergency intervention) (see above). Equipment, medications and personnel trained to provide cardiopulmonary resuscitation must be available (Table 5).
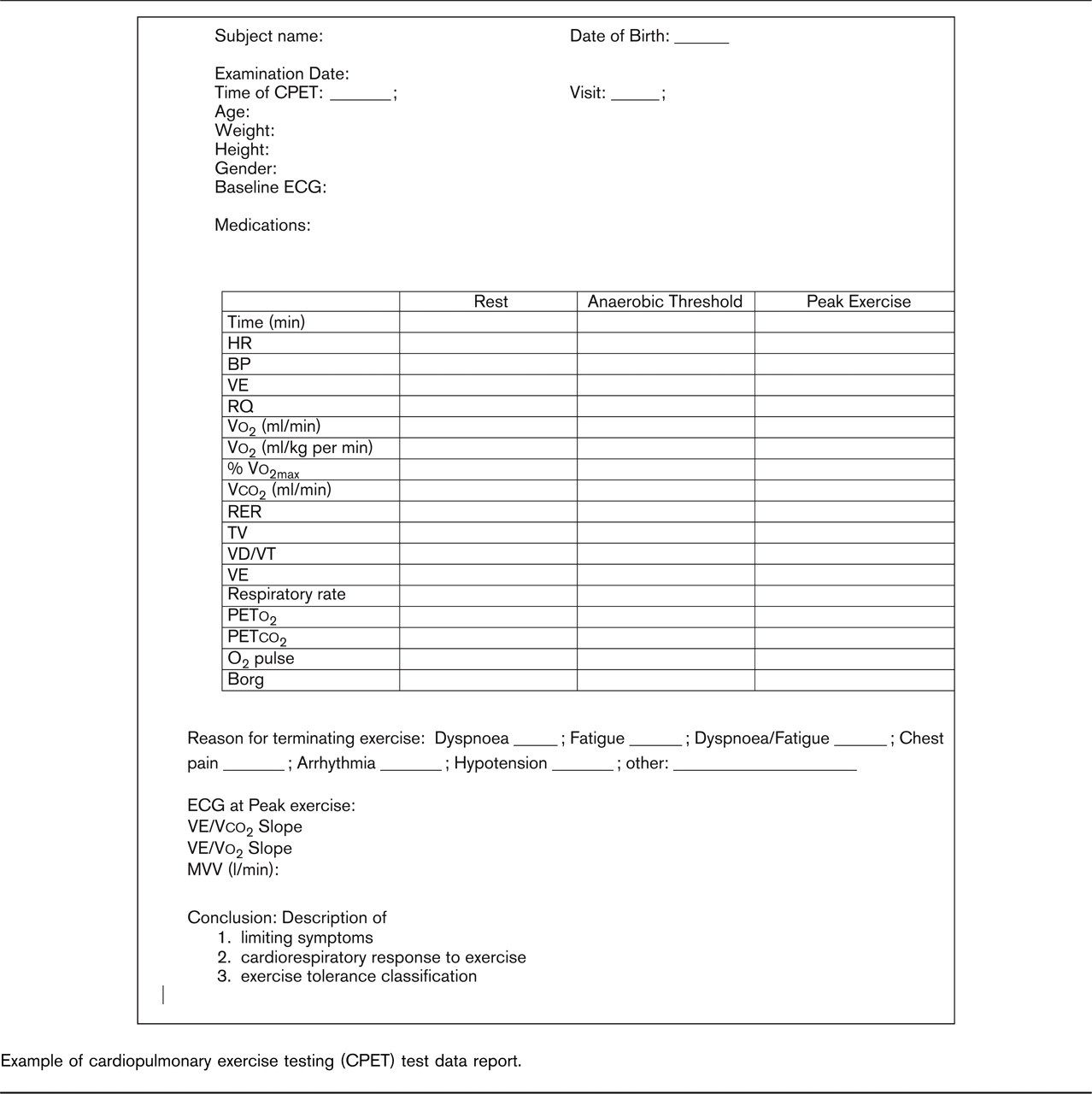
Example of cardiopulmonary exercise testing (CPET) test data report.
The modified Bruce protocol
Confirmation of patient candidacy for cardiopulmonary exercise test
Inclusion (Table 2) and exclusion criteria (Table 3) should be satisfied, including the pre-test information (Table 7). Intermittent blood pressure monitoring while continuous monitoring of 12-lead ECG, and expiratory gases should be ensured.
Exercise modality
Both bicycle and treadmill testing may be used. Whichever protocol is chosen, it is advisable that the same is always used for a single patient in order to fully assess changes in the clinical state.
The treadmill protocol is usually preferred for sicker patients and for those not used to pedalling. The treadmill should have front and/or side rails for subjects to steady themselves. Subjects may also require the assistance of the person administering the test. Subjects should not grasp the rails tightly, since this decreases Vo2 and increases exercise time and muscle artefact. It is helpful if subjects close their fists and place one finger on the rails to maintain balance after they are accustomed to walking on the treadmill.
When exercise stops, the treadmill/bicycle load should be decreased to the lowest level used, and the subjects should keep on walking/pedalling for at least 1 min prior to stopping completely. Enquiry should be made of the causes limiting exercise tolerance, and these should be recorded.
Data monitoring
ECG [thus heart rate (HR)] and blood pressure (BP) should be recorded at rest and during the last minute of each exercise stage. Perceived ratings of dyspnoea and fatigue should be recorded for each stage using the modified Borg scale (Table 6). All measurements (HR, BP, ECG, Borg scale) should also be obtained at peak exercise.
Data reporting
The beginning and end of exercise should be clearly marked. Data averaged over 30s should be tabulated in a time-down table. Data to be included are:
Vo2 in ml/min
Vo2 in ml/kg per min (and % predetermined Vo2max)
Vco2 (ml/min)
RER
VT (tidal volume)
VD/VT (ratio between physiological dead space and tidal volume)
VE
Respiratory rate
PETo2 (end-tidal expiratory oxygen pressure)
PETco2 (end-tidal expiratory carbon dioxide pressure)
O2 pulse
Borg scale (e.g. for dyspnoea)
Peak Vo2 should be the highest continuous 30-s average of Vo2 occurring within the final minute of exercise.
Risk factor levels (mean, SD, or %) and crude percentage of nonfatal and fatal CVD in men and women without a history of myocardial infarction aged 20–65 years by BMI category in the MORGEN project, 1993–1997
ECG, electrocardiogram.
Several plots should be generated to accurately determine the anaerobic threshold (AT):
Graph 1: Vo2, Vco2 versus time
Graph 2: VE/Vo2, VE/Vco2 versus time
Graph 3: PETco2, PETo2 versus time
Graph 4: Vco2 versus Vo2
Graph 5: RER versus time
Graph 6: The composite AT plot will include: Vco2, PETo2, VE/Vo2, RER versus Vo2
The key criteria used to select the anaerobic threshold are the following:
The nadir for the ventilatory equivalent for Vo2 without change in the ventilatory equivalent for Vco2
The nadir for the ventilatory equivalent for PETo2 without change in the ventilatory equivalent for PETco2.
The computerized V slope method: intersection of the lines drawn between 1 min after the end of warm-up and RER of the plot of Vco2 versus Vo2.
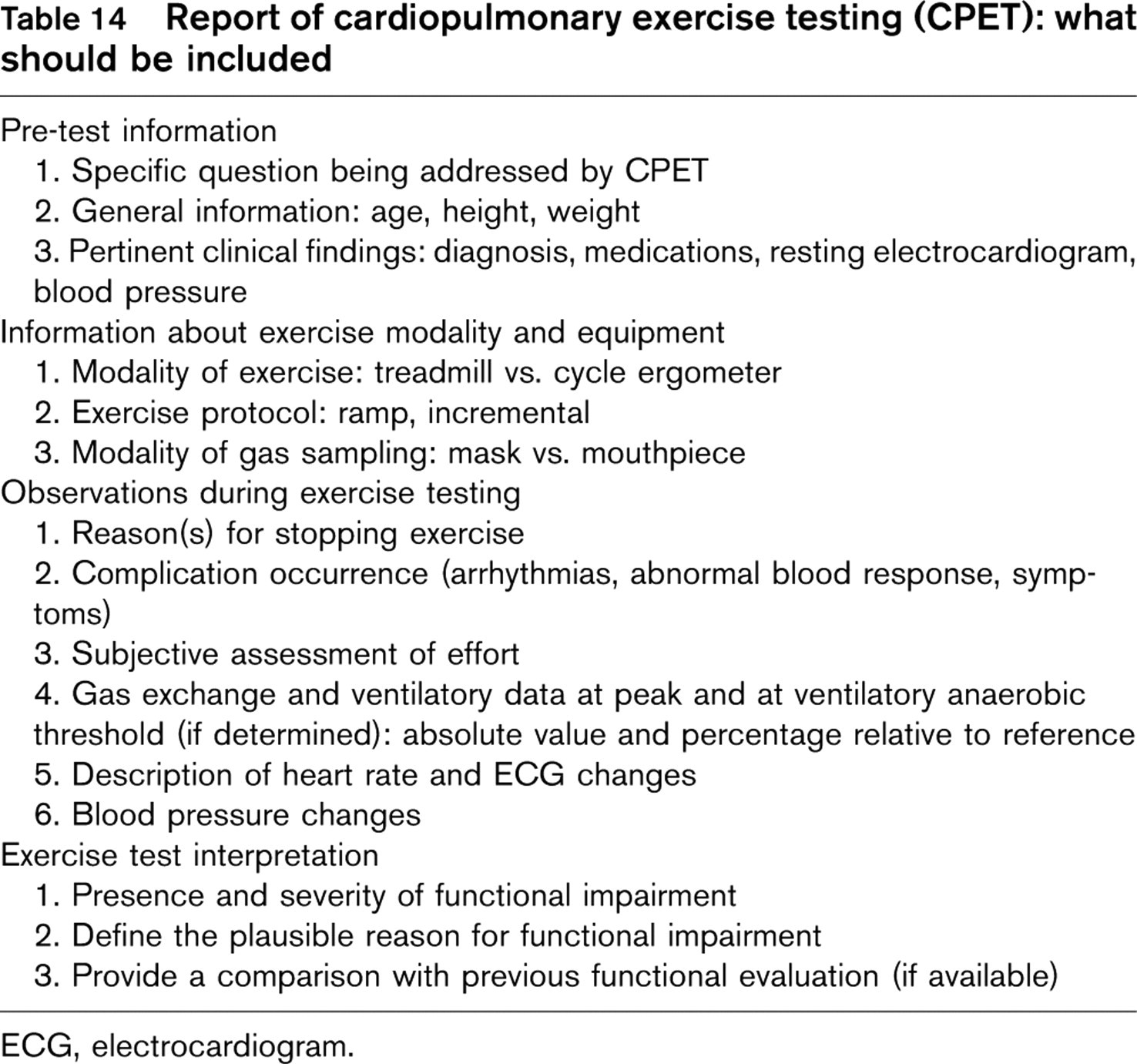
Table 14 summarizes the information that should be included in the final report. Figure 3 is an example of Cardiopulmonary Summary Exercise Test Data Report.
Footnotes
Appendix Writing Committee
Massimo F. Piepoli and Ugo Corrà (Chairmen) (Italy), Pier Giuseppe Agostoni (Italy), Romualdo Belardinelli (Italy), Alain Cohen-Solal (France), Rainer Hambrecht (Germany) and Luc Vanhees (Belgium).
Hans Björnstad (Norway), Andrew J.S. Coats (Australia), Darrel P. Francis (UK), Pantaleo Giannuzzi (Italy), Marco Guazzi (Italy), Marco Metra (Italy), Alessandro Mezzani (Italy), Piotr Ponikowski (Poland) and Hugo Saner (Switzerland).