
Abstract
Background
A parental history of cardiovascular disease has a strong relationship with risk factor clusters in the offspring. This study was performed to identify major cardiovascular risk factors in middle school-aged children and their parents in both high and low-risk families.
Design
A school-based, cross-sectional study.
Methods
The middle schools of the 6th district of Tehran were divided randomly into two groups. A total of 169 high-risk children with their families were recruited from the first group and 105 low-risk children with their families were recruited from the second group of schools. Anthropometric and metabolic measurements were performed.
Results
The means of the waist circumference and waist-to-hip ratio were significantly higher in high-risk fathers. The means of total and low-density lipoprotein (LDL) cholesterol were significantly higher in both parents and children of the high-risk group. The means of the fasting plasma glucose were significantly higher in fathers and offspring of high-risk families. More fathers in high-risk families were smokers. The prevalence of increased total cholesterol, LDL-cholesterol and hyperglycemia (≥100mg/dl) were higher in high-risk parents and children. The prevalence of increased body mass index (≥25 kg/m2 for parents and 85th percentile for children) was higher in fathers and children of high-risk families.
Conclusions
Cardiovascular risk factors are more prevalent and clustered in high-risk families. The screening of high-risk families is essential to prevent the progression of atherosclerosis from childhood and reduce the burden of cardiovascular disease in adulthood.
Introduction
There has been an alarming increase in the incidence of coronary heart disease (CHD) in Asian countries and the Middle East crescent during the past few decades [1, 2]. This is attributed to urbanization, worldwide technological changes, economic growth and its effects on the lifestyle of people in this region. Currently, cardiovascular disorders are the leading cause of death in Iran, accounting for nearly 46% of total deaths [3]. CHD is the predominant form, with approximately 2.5 deaths for every stroke death [3]. Atherosclerosis begins early in life, and children exhibit cardiovascular risk factors at similar frequencies to adults [4, 5]. Clusters of multiple risk factors often track into adulthood and are predictive of future cardiovascular risk [6–9].
Lifestyle and health-related behaviours gradually take form from childhood, consolidate before the age of 10 years, and the attitudes of adults in the families play the key role in the development of behavioural risk factors in their offspring [10, 11]. On the other hand, there is compelling evidence for familial aggregation of CHD favoured by genetic and environmental factors [12, 13]. The available data suggest that there are certain at-risk families that are responsible for much of the CHD burden in different communities [14]. A positive family history of CHD is generally associated with a 1.5 to twofold increase in the risk of CHD among first-degree relatives [15]. A parental history of cardiovascular disease (CVD) at less than 65 years of age has a strong relationship with the risk factor clusters in the offspring [16].
The detection and treatment of CHD risk factors from early childhood is essential to reduce the prevalence of disease in adulthood. In recent years, a number of studies have shown an increasing trend in CHD risk factors among Iranian children [17]; however, screening for risk factors is generally not performed in this country, even in families with a high prevalence of CHD. In this study we aimed to identify and evaluate major cardiovascular risk factors among middle school-aged children and their parents. We also evaluated whether the involvement of the children can be an effective means to increase participation of the families in the screening programme.
Methods
This study was conducted with middle school-aged children, that is, sixth to eighth graders, and their parents in the sixth district of Tehran. The schools were randomly divided into two groups A and B to recruit high and low-risk families, respectively. In this way we tried to reduce the effect of the interaction between high and low-risk families, because it was our hypothesis that high-risk families would probably take part in the study more than low-risk families. In each household the offspring and his/her parents with other siblings were investigated for cardiovascular risk factors. High-risk families were defined as those with a positive history of major cardiovascular endpoints that had occurred before 65 years of age for women or before 55 years of age for men in the household, or the presence of at least two classic CVD risk factors, namely dyslipidemia, hypertension, diabetes and smoking in at least one of the parents or grandparents of the children. The presence of CVD or its risk factors was detected through a self-administered questionnaire that was completed by the parents in the home.
The research team attended the schools to invite families of children to take part in the study. A detailed verbal explanation about the growing CVD burden in the country, its risk factors, and the necessity of implementing preventative measures from early childhood was given to the pupils in the morning ceremony at the schools. A brochure was then distributed to pupils that included a brief description of the above items in common language and the concept of being at high risk. Each pupil was requested to deliver this brochure to his/her parents and to explain its contents to them. In group A schools, families were invited to attend a school-based clinic if they were high risk. In group B schools, the households that were free of a history of cardiovascular endpoints or CVD risk factors were invited to the clinic. Written informed consent was obtained from each of the households signed by the father of the family.
In the clinic, a structured questionnaire was filled in by the parents that included enquiries about socio-economic status, educational level, the frequency, quality and level of physical activities, nutrition (i.e. the intake of saturated fatty acid, fibre and salt) and smoking. A general physical examination was also performed for both parents and children. Standing height was measured to the nearest 0.5 cm (Seca Stadiometer) and weight was measured to the nearest 0.5 kg (Seca Beam Balance), wearing minimum indoor clothing and barefoot, and the body mass index (BMI) was calculated. Waist and hip circumferences were measured and the waist-to-hip ratio (WHR) was estimated. The blood pressure was measured twice on the right arm using an appropriate cuff-sized mercury sphygmomanometer with the subject sitting quietly for at least 5 min. The mean of two measurements of Korotkoff's phase I and the mean of two values of phase IV were recorded as systolic and diastolic blood pressure, respectively. Venous blood was collected with minimum stasis to determine the metabolic parameters. Subjects had been fasting for 12 h and had rested for 15 min before the venipuncture. Serum total cholesterol, triglyceride, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol and glucose concentrations were analysed using an auto analyser (BM Hitachi-747; Boehringer Mannheim GmbH, Mannheim, Germany) employing the original kits for enzymatic-colorimetric methods (Boehringer Mannheim).
Definitions
Parents
Cutoff points for lipid parameters were determined according to the National Cholesterol Education Program; Adult Treatment Panel III guidelines [18]. Total cholesterol 200 mg/dl or greater, LDL-cholesterol 160 mg/dl or greater, HDL-cholesterol less than 40 mg/dl and triglycerides 200 mg/dl or greater were considered as dyslipidemia. Hypertension was defined as systolic blood pressure of 140 mmHg or higher or diastolic blood pressure of 90 mmHg or higher or the use of antihypertensive drugs [19]. Regular smokers were those who smoked at least one cigarette per day. Diabetes was defined as fasting plasma glucose (FPG) values of 126 mg/dl or greater or the use of glucose-lowering drugs or insulin. For those not taking glucose-lowering drugs or insulin, FPG between 100 and 125 mg/dl was considered as impaired fasting glucose (IFG) [20]. Overweight, obesity and extreme obesity were defined as a BMI of 25.0–29.9, 30.0 or more, and 40.0 kg/m2 or more, respectively [21]. Visceral obesity assessed by WHR was defined as over 0.95 for men and over 0.85 for women, respectively; or else a waist circumference of 102 cm or more for men and 88cm or more for women were the cutoff points for visceral obesity. Regular physical activity was defined as moderate aerobic exercise performed 5 days a week with a duration of at least 20 min per day according to self-report.
Children
Reference values for dyslipidemia were taken from the National Cholesterol Education Program guidelines [22, 23]. Hypertension was defined as average systolic or diastolic blood pressure greater than or equal to the 95th percentile of age, sex and height on at least three separate occasions [24]. Obesity was regarded as a BMI of the 95th or greater age and sex-specific percentile, whereas over-weight was considered as a BMI between the 85th and 94.9th age and sex-specific percentile [25]. Physical activity in children was defined as in their parents (see above).
Statistical analysis
Statistical analysis was performed using SPSS software, version 12 (SPSS Inc., Chicago, Illinois, USA). Measurements of continuous variables were expressed as means and standard deviations (SD). Significance of differences was tested using Student's t-test if the variable was continuous; and in the case of nominal variables by the chi-squared test and expressed as P values. Binomial logistic regression analysis was used to determine the relationship between independent parental factors and being a high-risk child.
Results
As a whole, 169 (84%) high and 105 (71%) low-risk families participated in the survey (P < 0.03). There was no statistically significant difference between the high and low-risk families with relation to socio-economic status. The means of age, anthropometric and blood pressure values of both groups are presented in Table 1. There were no statistically significant differences in the means of age, BMI and blood pressure of the parents and children between the two groups. The means of waist circumference and WHR were significantly higher in the fathers of high than those of low-risk families (P = 0.003 and P < 0.05, respectively). The means of metabolic values between the groups are presented in Table 2. Total cholesterol and LDL-cholesterol were much higher in the parents and children of the high-risk group (P < 0.001 for all). FPG levels were higher in the fathers and children of high than low-risk families (P < 0.001 for all).
The prevalence of CHD risk factors in the parents and children of the two groups are represented in Tables 3 and 4. More fathers in the high-risk families were active smokers. In fathers of the high-risk group 108 (63.9%) were overweight, 18 (10.6%) were obese and four (2.3%) were morbidly obese, whereas in the low-risk group 53 (50.4%) were overweight, eight (7.6%) were obese and one (0.9%) had morbid obesity (P < 0.01). In mothers of the high-risk group 70 (41.1%) were overweight, 46 (27.5%) were obese and three (1.8%) were morbidly obese, whereas in the low-risk group 48 (54.3%) were overweight and 13 (15.2%) were obese (P<0.05). In children of the high-risk group 34 (20.1%) were overweight and six (1.5%) were obese, whereas in children of the low-risk group 10 (9.5%) were overweight and three (2.8%) were obese (P<0.001).
Of the fathers in the high-risk group 25 (14%) had diabetes and 76 (45%) had IFG, whereas in the low-risk group three (2.9%) fathers had diabetes and 18 (17%) had IFG (P < 0.0001). Of the high-risk mothers, nine (5.3%) had diabetes and 55 (32.5%) had IFG, whereas in the low-risk mothers, nine (8.6%) had diabetes and 16 (15.1%) had IFG (P<0.04). None of the children were found to have diabetes; however, 58 of the high-risk versus 13 of the low-risk children had IFG (P < 0.001).
Thirty-four per cent of overweight/obese children in the high-risk and 12% of the overweight/obese offspring in the low-risk group had IFG (P < 0.001).
Means of anthropometric and blood pressure values of children and parents in high and low coronary heart disease risk families
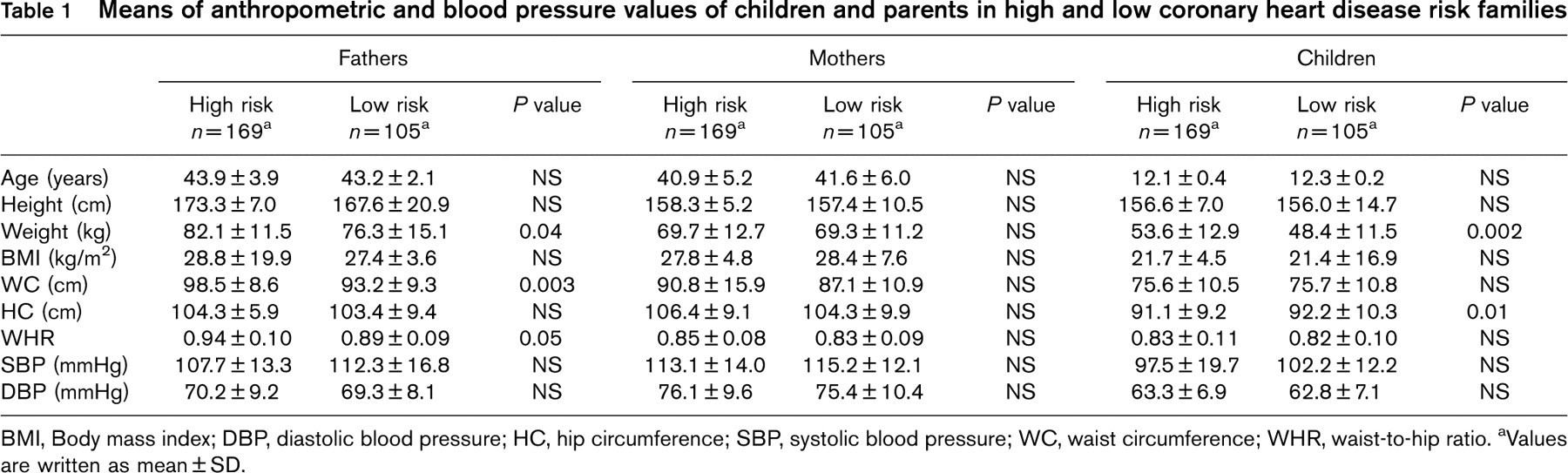
BMI, Body mass index; DBP, diastolic blood pressure; HC, hip circumference; SBP, systolic blood pressure; WC, waist circumference; WHR, waist-to-hip ratio. aValues are written as mean ± SD.
Means of metabolic parameters of parents and children in high and low coronary heart disease risk families
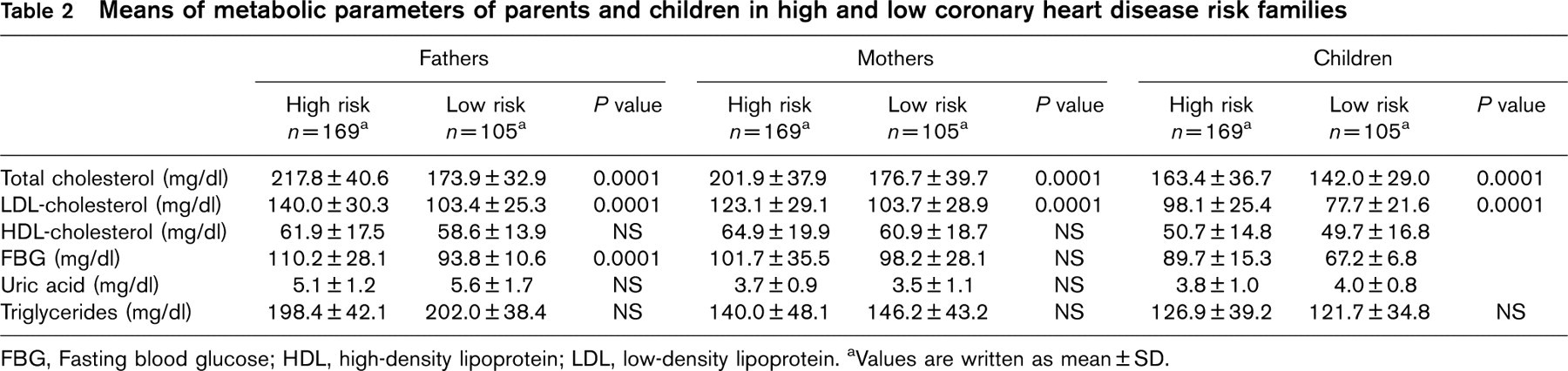
FBG, Fasting blood glucose; HDL, high-density lipoprotein; LDL, low-density lipoprotein. aValues are written as mean ± SD.
Coronary heart disease risk factors of parents in high and low coronary heart disease risk families
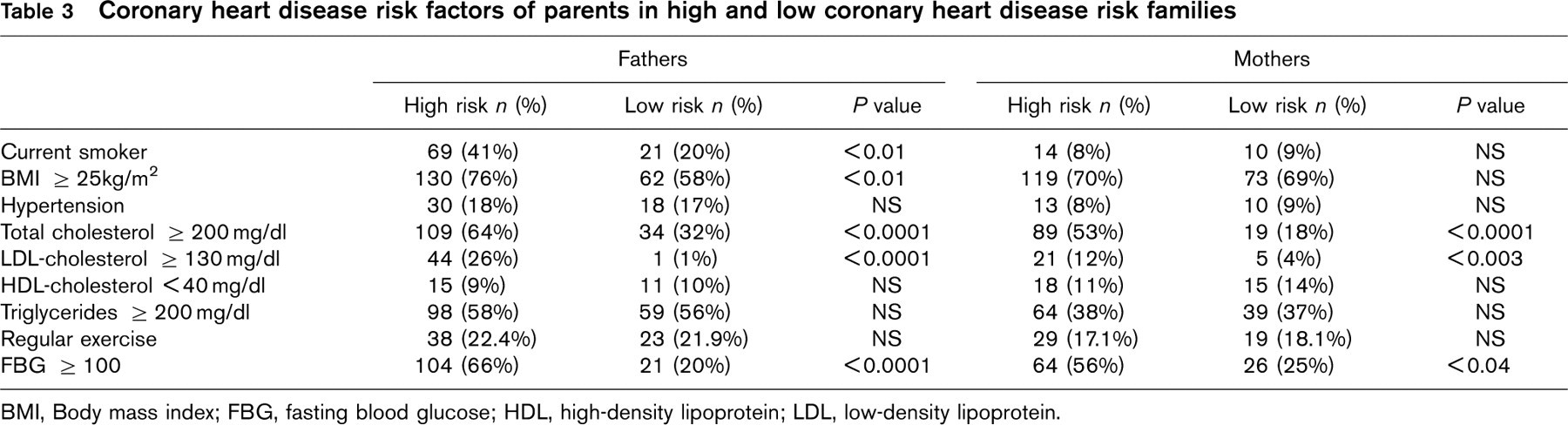
BMI, Body mass index; FBG, fasting blood glucose; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Coronary heart disease risk factors of children in high and low coronary heart disease risk families.
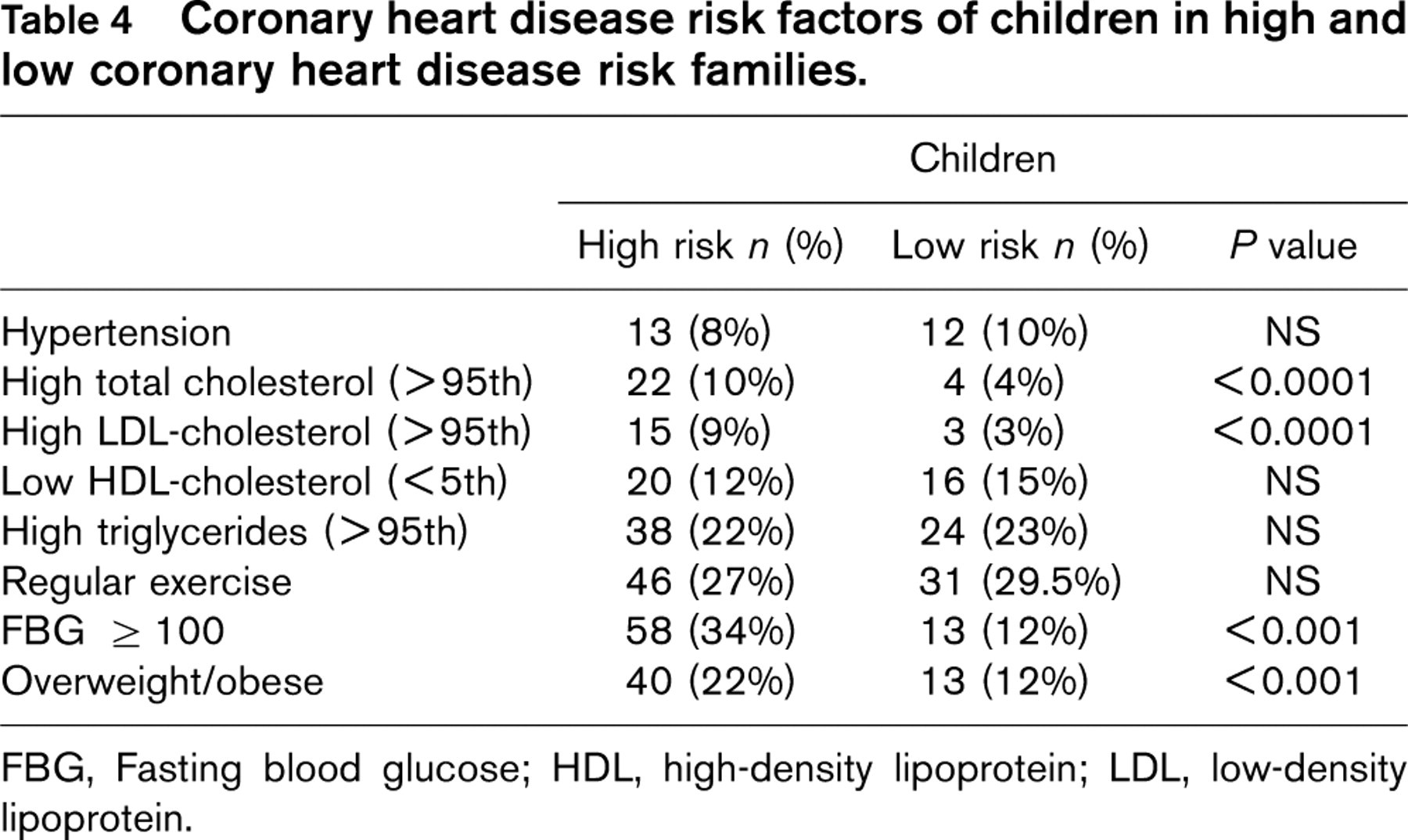
FBG, Fasting blood glucose; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Less than 30% of parents and offspring in both the high and low-risk families were doing regular exercise.
We calculated the risk score of the children by assigning a unit number to each of the classic risk factors, namely a positive family history of premature CVD, hypertension, hyper-LDL, hypertriglyceridemia, hypo-HDL, glucose intolerance and overweight/obesity in the offspring and adding the number of risk factors they had. High-risk children were those who had at least two of these risk factors.
Binomial logistic regression analysis revealed that only age-adjusted maternal obesity, diabetes mellitus, hypertension and dyslipidemia had a significant relationship with being a high-risk child [odds ratio 4.17, 95% confidence interval (CI) 1.92–9.06]. No correlation was found between paternal factors such as obesity, hypertension, diabetes and dyslipidemia, and being high risk in children. The adjusted odds ratio for obesity of fathers and high-risk children was 0.77 (95% CI 0.27–2.21). No obvious relationship was detected between being a high-risk child with the presence of premature death caused by CVD in the grandparents.
Discussion
The results of this study suggest that it is essential to screen for cardiovascular risk factors from childhood in high-risk families, because childhood and adolescence are crucial periods for the development of risk-related behaviours. On the other hand, young unaffected members of high-risk families have a greatly increased risk of early-onset CHD. We found that many of the traditional CHD risk factors were more prevalent in parents and children of the high-risk families compared with those from low-risk families.
The most consistent findings in our study were the higher total cholesterol and LDL-cholesterol levels in high-risk parents and children compared with the low-risk families, which are similar to the findings of Barth et al. [26] that showed significantly higher total cholesterol and LDL-cholesterol values in children with a positive family history of premature CHD. In addition, this difference in total cholesterol and LDL-cholesterol levels was also present between the parents of the high and low-risk groups in our study. However, we found no significant difference in HDL-cholesterol and triglyceride levels between the high and low-risk groups. In a recent study of atherosclerosis risk factors in Iranian children [27], it was found that total cholesterol, LDL-cholesterol, triglycerides and apolipoprotein B100 were significantly higher, whereas apolipoprotein A1 and HDL-cholesterol were significantly lower in the offspring of families with a history of premature CHD. In contrast to these findings, no significant differences were found in the concentrations of lipids and lipoproteins between the offspring of the high and low-risk families by other investigators [28].
The strong correlation between the lipid levels of the parents and their offspring in this study is similar to the findings from previous studies [29, 30].
It is necessary to lower the average blood cholesterol level in all of the parents and offspring with hypercholesterolemia, as children and adolescents with high cholesterol levels are more prone to have high plasma cholesterol levels when they are adults [31–33].
Our finding of an increased prevalence of overweight/obesity in the fathers and children of the high-risk compared with the low-risk group is compatible with those of Glowinska et al. [34], in which children with a family history of CVD had a higher BMI. They concluded that in these children BMI was a great risk factor. Obesity in boys would be significantly related to coronary artery calcification 15–20 years later [35]. Overweight and hypercholesterolemic children would also have more relatives dying from CVD [36].
An important finding in this study was the increased prevalence of diabetes in high-risk fathers and the increased rate of IFG in high-risk children compared with the low-risk group. A higher prevalence of hyperglycemia, obesity and elevated cholesterol were also previously shown in young adults with a positive family history of CHD [37]. IFG predicts adverse cardiovascular events whether or not this is manifested as overt diabetes [38]. This is usually accompanied by hyperinsulinemia and a clustering of risk factors such as obesity, dyslipidemia and hypertension in the childhood metabolic syndrome [39]. Obese and diabetic children often originate from the families with CVD [34]. Offspring of diabetic parents were previously shown to be significantly overweight, with higher rates of the development of hyper-LDL and hyperinsulinemia over time [40].
Although we did not find any significant difference in the prevalence of hypertension between the two groups, some other studies have indicated that hypertension alone may be a strong risk factor for premature CVD. For example, Masana et al. [41] found a high prevalence of hypertension in young adults with a familial incidence of myocardial infarction before the age of 55 years. In another study, a high frequency of hypertension was found in siblings of those with premature CHD [42].
We found a generally low level of physical activity in both high and low-risk parents and children. A sedentary lifestyle is known to increase the relative risk of CHD death to 1.6-fold [38], so regular physical activity should be encouraged in all family members, especially in the children of high-risk families to forestall CVD endpoints in their adulthood.
The findings of this study set forth special consideration for a household approach based on obtaining a complete family history to identify high-risk families and to implement preventative measures for CVD from childhood. In general, a significant family history of CVD is an important risk factor for recurrence in offspring [43]. A family-based approach towards screening for CVD would serve as a surrogate for both genetic and environmental components. By this method, we can also identify at-risk individuals within high-risk families, who can be targeted for educational and lifestyle intervention.
Although a parental history of CVD is a useful marker for screening, it will underestimate the number of at-risk individuals, especially the children with hyperlipidemia. On the other hand, many parents were still too young to manifest coronary artery disease at the time of screening [44–47]. Therefore we tried to expand the domain of screening by including households containing any family member with at least two risk factors.
Schools provide an excellent setting for introducing comprehensive health education and promotion. This study demonstrated that it is feasible to involve pupils to convey cardiovascular health messages into the household environment and to motivate participation of the members of high-risk families in the screening programme. Health campaigns have also shown that children could actively influence their parents’ habits [48]. In addition, school-based programmes that get the high-risk parents involved with their children in learning about CHD and its risk factors can improve the ability of the parents to instill healthy behaviours in their children [49].
Despite the great burden of CHD in urban communities of Iran, screening for cardiovascular risk factors is not performed in a systematic manner. This lack of attention, despite its being critically important for the prevention of CVD, may be running worldwide. The survey of families with a history of premature CHD in Europe also showed that screening of family members for the risk factors is rarely performed, and 80% of patients with a positive family history remain undiagnosed [50]. However, regarding the familial nature of CHD and the fact that CHD expression is clustered in subpopulations with a positive family history, the screening of high-risk families can identify in a cost-effective way most of the individuals eligible for preventative measures, because a relatively small subgroup of families in the population may carry the vast majority of the CVD burden in the community [51]. A major task for health professionals in our community is thus to demarcate high-risk families that comprise the majority of the target population requiring CVD prevention.
Footnotes
Acknowledgements
The authors appreciate the contributions of Ms Yalda Rezayeekhah, Mr Peyman Shooshtarizadeh, and all of the families who participated in this study. They also thank Dr Mohsin Raza for critically reviewing the manuscript.