
Abstract
Background
Post-traumatic stress disorder (PTSD) may develop in the aftermath of an acute myocardial infarction (MI). Whether PTSD is a risk factor for cardiovascular disease (CVD) is elusive. The biological mechanisms linking PTSD with atherosclerosis are unclear.
Design
A critical review of 31 studies in the English language pursuing three aims: (i) to estimate the prevalence of PTSD in post-MI patients; (ii) to investigate the association of PTSD with cardiovascular endpoints; and (iii) to search for low-grade systemic inflammatory changes in PTSD pertinent to atherosclerosis.
Methods
We located studies by PubMed electronic library search and through checking the bibliographies of these sources.
Results
The weighted prevalence of PTSD after MI was 14.7% (range 0–25%; a total of 13 studies and 827 post-MI patients). Two studies reported a prospective association between PTSD and an increased risk of cardiovascular readmission in post-MI patients and of cardiovascular mortality in combat veterans, respectively. In a total of 11 studies, patients with PTSD had increased rates of physician-rated and self-reported cardiovascular diseases. Various cytokines and C-reactive protein were investigated in a total of seven studies suggesting that PTSD confers a pro-inflammatory state.
Conclusions
Increasing evidence suggests that PTSD specifically related to MI develops considerably frequently in post-MI patients. More research is needed in larger cohorts applying a population design to substantiate findings suggesting PTSD is an atherogenic risk factor and to understand better the suspected behavioural and biological mechanisms involved.
Keywords
Introduction
Psychosocial factors, traumatic stress, and coronary artery disease
Psychosocial factors are now widely acknowledged as risk factors for cardiovascular diseases (CVD) in particular coronary artery disease (CAD) [1, 2]. In the INTER-HEART case—control study [3], the population attributable risk of myocardial infarction (MI) explained by a composite index of psychosocial factors was 32.5%, suggesting that psychosocial stress may account for much of the hitherto unexplained variance in coronary risk by traditional cardiovascular risk factors. One line of research in behavioural cardiology highlights the cardiovascular risk inflicted by the exposure of humans to traumatic events [4, 5]. Adverse short-term effects of natural or man-made disasters on the heart encompass life-threatening arrhythmias and sudden cardiac death [6–8]. There is, however, little research on more chronic cardiovascular sequelae of a trauma, contrasting with the clinical observation that some patients continue to perceive a heart attack as traumatic long after it occurs. Cardiologists are aware that an individual may experience an infarction as an unheralded and life-threatening event (i.e. ‘out of the blue'), leaving patients with intense fear and feelings of helplessness [9]. If patients repeatedly recall this cardiac trauma, develop avoidance towards cues related to the heart attack, and end up with sustained arousal for a period of more than 1 month post-MI, they may be suffering from full-blown post-traumatic stress disorder (PTSD).
Post-traumatic stress disorder, definition and epidemiology
According to the fourth edition of the Diagnostic and Statistical Manual of Mental Diseases (DSM) [10], the diagnosis of PTSD requires several clinical identification criteria (A–F): Criterion A1 refers to the experience of an event involving injury or threat to one's physical integrity and accompanied by intense fear or helplessness (criterion A2). Criterion B comprises frequent re-experience of the traumatic event by thought intrusions, flashbacks, nightmares, and sensory triggers, leading to intrusive recollections resulting in physiological reactivity and persistent avoidance of stimuli associated with the trauma (criterion C). Criterion D constitutes increased arousal shown as hypervigilance, sleep disturbances, and irritability. All defining criteria must persist for more than 1 month (criterion E), and must lead to clinically significant impairment in daily functioning (criterion F).
The life-time prevalence of PTSD is approximately 8%, with sexual violence in women and combat experience in men being most often associated with PTSD and with one-third of patients not recovering from PTSD many years after the trauma [11]. Only recently has PTSD developing in the aftermath of a heart attack attracted attention as a promising clinical entity to help understand better the compromised quality of life, poor adherence to cardiac therapy, and perhaps increased cardiac risk in post-MI patients [5, 12].
Contrasting post-traumatic stress disorder with depression in cardiac patients
Post-MI, approximately 20% of patients have major depression and 20% have minor depression [13]. Depression prospectively increases the risk of first-time MI and recurrent MI in apparently healthy individuals and post-MI patients, respectively. Convincing evidence suggests that adverse health habits (e.g. smoking, poor diet) and direct pathophysiological changes (e.g. increased inflammation, platelet hyperactivity) both contribute to the link between depression and CAD [13]. Before encouraging cardiologists to adopt PTSD as a construct similarly important to cardiovascular health as depression, several questions should be addressed guiding us in defining the three aims of this review.
Aims of this review
First, PTSD as a specific sequel of MI should be frequent. Therefore, our first aim was to estimate the prevalence of PTSD in post-MI patients. Second, in prospective rather than cross-sectional studies, PTSD should demonstrate its cardiovascular risk factor status in individuals initially free of CVD and in those who have already experienced an infarction. Therefore, our second aim was to review studies reporting a relationship between PTSD and self-reported as well as physician-diagnosed cardiovascular endpoints.
Third, if PTSD confers an atherogenic risk, behavioural factors (e.g. smoking, non-adherence to medication), biological mechanisms (e.g. inflammation, dyslipidaemia), and stress-mediating systems (e.g. sympathetic overactivity) are probably all involved [1]. However, teasing apart the unique contributions of these intertwined domains to differences in cardiovascular biology between PTSD patients and controls is difficult. Cardiovascular risk factors tend to cluster with psycho-social risk factors, which, in turn, also cluster among each other [1]. Accordingly, PTSD has been associated with depression [14] and virtually all traditional cardiovascular risk factors, some of which are vastly behavioural. More precisely, PTSD has been associated with elevated blood pressure [15], obesity [16], atherogenic dyslipidaemia [17], increased prevalence of diabetes [18], heavy smoking [19], and low physical activity [20]. Bearing these complex interactions in mind, our third aim was to review a growing literature on circulating molecules of low-grade systemic inflammation in PTSD. Atherosclerosis is mainly an inflammatory disease and circulating C-reactive protein (CRP), tumour necrosis factor-α, and interleukin (IL)-6 were all shown independently to predict coronary risk in different populations [21]. We hypothesized that PTSD would confer a pro-inflammatory state providing one psychobiological mechanism linking PTSD with atherosclerosis. It was beyond our scope to review alterations in the hypothalamic—pituitary—adrenal (HPA) axis and autonomic nervous system function in PTSD [22]. We refer to this literature if it provides an explanation for observed inflammatory changes in PTSD patients compared with non-PTSD controls.
Methods
Candidate studies in English performed in adults and published between 1980 (i.e. when the American Psychiatric Association added PTSD to the DSM-III nosological classification scheme) and November 2005 were identified by PubMed/Medline electronic library search using the following key words in alphabetical order: atherosclerosis, cardiovascular disease, cytokines, coronary artery disease, inflammation, myocardial infarction, post-traumatic stress disorder. Reference lists of tracked studies were scrutinized for additional studies of potential interest for the topic of this review. To estimate the prevalence of PTSD in post-MI patients, the percentage value of patients having PTSD in each study was weighted with the sample size of that study. Symptom severity and the frequency of a PTSD diagnosis in traumatized samples wane over time [11, 23]. We therefore computed the Pearson correlation coefficient between the prevalence of PTSD after MI and the average time since MI when PTSD was diagnosed, hypothesizing an inverse relationship between the two variables. To estimate the effect sizes of differences in biological marker between PTSD patients and controls, we computed Cohen's d by means of dividing the difference between the two means by the pooled standard deviations (SD), namely the square root of the average of the squared SD [24].
To be included, a study had to provide a diagnosis of PTSD based on a structured clinical interview or by meeting a cut-off on an established symptom questionnaire. In particular, we did not include a case series study as it would inflate a prevalence of PTSD in post-MI patients of 100% by nature of its design [25]. Other studies were excluded because their subjects were either cardiac arrest patients in whom tachyarrhythmia was not necessarily a consequence of an acute MI [26] or stable CAD patients who had not all experienced an acute MI [27]. A study reporting more symptoms of PTSD in 21 post-MI patients than in 20 non-MI controls was excluded because it did not provide the prevalence of PTSD in patients [28]. Studies reporting relatively more health problems in PTSD patients were excluded if not providing a distinct analysis in terms of CVD [29]. To clarify whether there was data overlap between studies we contacted the first authors of the respective studies. If the same group reported prevalence rates of PTSD after MI from the same study sample in different papers [30–34], the paper most apparently addressing the issue of PTSD prevalence after MI was considered [30, 33].
Results
Prevalence of post-traumatic stress disorder in the aftermath of an acute myocardial infarction
Table 1 lists 13 studies fulfilling the inclusion criteria [30, 33, 35–45]. The weighted prevalence of PTSD in post-MI patients was approximately 15% (the prevalence was 14.1% if three studies, for which data overlap could not be excluded [39–41], were weighted and counted as one study). Whereas three studies applied a clinical interview for DSM diagnosis of PTSD [35–37], 10 studies applied established self-report symptom scales to define PTSD [30, 33, 38–45]. As opposed to the post-traumatic diagnostic scale [46] and the PTSD Inventory [47], the impact of event scale [48] considers intrusive and avoidance symptoms but does not assess hyperarousal. However, above threshold intrusion and avoidance symptoms appearing in the same patient on the impact of event scale are very likely to correlate with a clinical diagnosis of full PTSD [43]. Interestingly, lower perceived control was associated with higher PTSD symptom scores in one study [37]. Later assessment of PTSD after MI showed an insignificant association with a lower prevalence of PTSD (r = –0.24, one-tailed P = 0.22). The association between MI and PTSD became insignificant with adjustment for depression in one study investigating this issue [30].
Estimated prevalence of post-traumatic stress disorder in relation to acute myocardial infarction
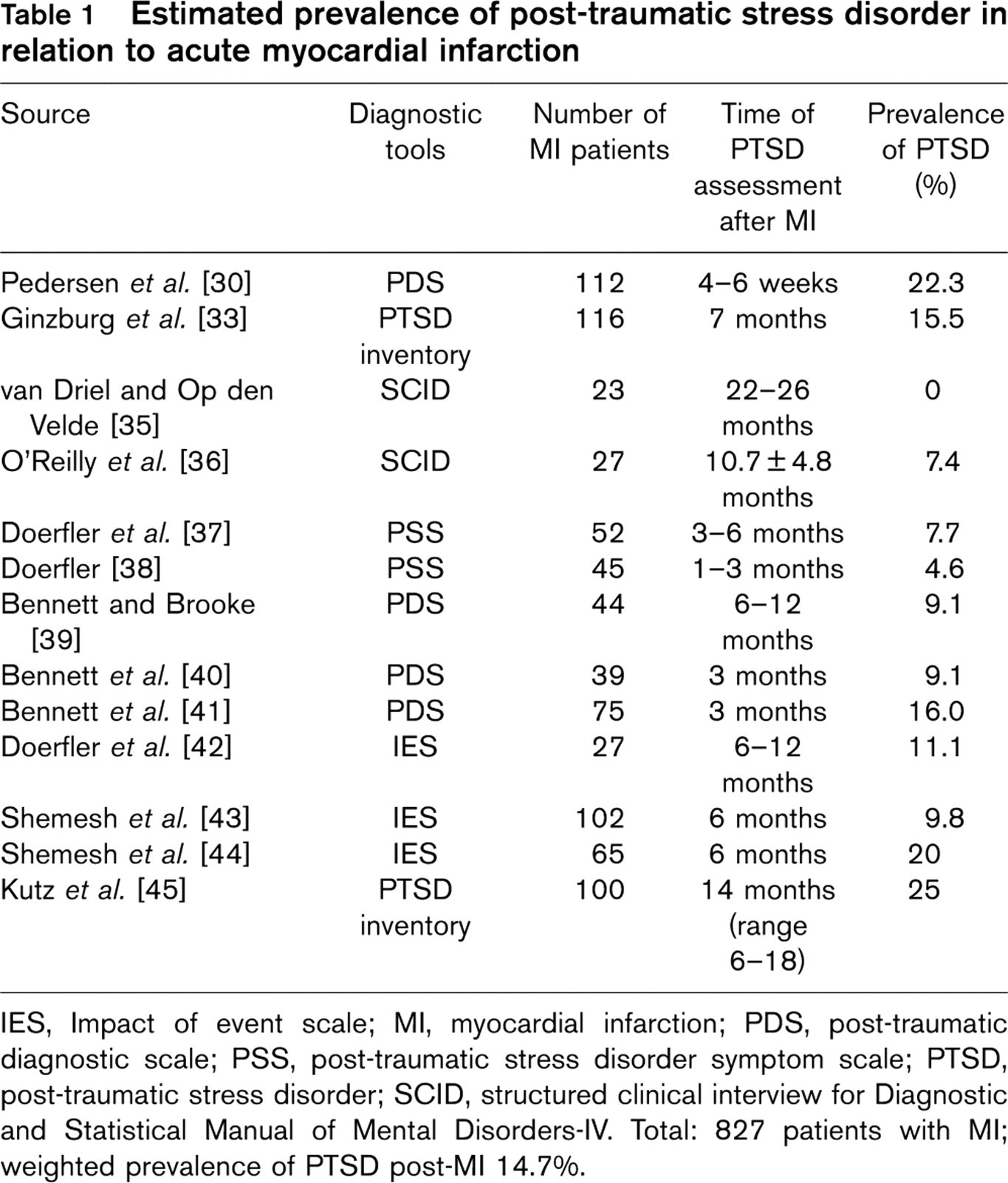
IES, Impact of event scale; MI, myocardial infarction; PDS, post-traumatic diagnostic scale; PSS, post-traumatic stress disorder symptom scale; PTSD, post-traumatic stress disorder; SCID, structured clinical interview for Diagnostic and Statistical Manual of Mental Disorders-IV. Total: 827 patients with MI; weighted prevalence of PTSD post-MI 14.7%.
Association of post-traumatic stress disorder with cardiovascular endpoints
Table 2 summarizes 11 studies in which PTSD correlated with either physician-diagnosed [44, 49–52] or self-reported cardiovascular endpoints [16, 52–57]. Notably, PTSD symptom severity correlated with an earlier onset of physician-diagnosed arterial disease but showed no association with CAD [50]. War veterans with PTSD reported significantly more angina pectoris but a similar rate of previous MI than veterans without PTSD; this study did, however, not control for a higher rate of smokers in the PTSD group [53]. Few studies controlled for demographic factors and lifestyle variables bearing the potential to increase cardiovascular risk on their own. Also, the traditional risk factors diabetes, hypertension, and exercise were not accounted for in any study. All but one study [50] addressed psychiatric co-morbidity, most often depression or substance abuse. Two recent studies applied a longitudinal design [44, 49]. The first and smaller study found a prospective relationship between PTSD and an increased risk of cardiovascular readmission at one-year follow-up in post-MI patients; this relationship was independent of depression [44]. The second study showed that PTSD predicted cardiovascular mortality in a large population of combat veterans 16 years down the line [49].
Association of post-traumatic stress disorder symptoms and diagnosis with cardiovascular endpoints
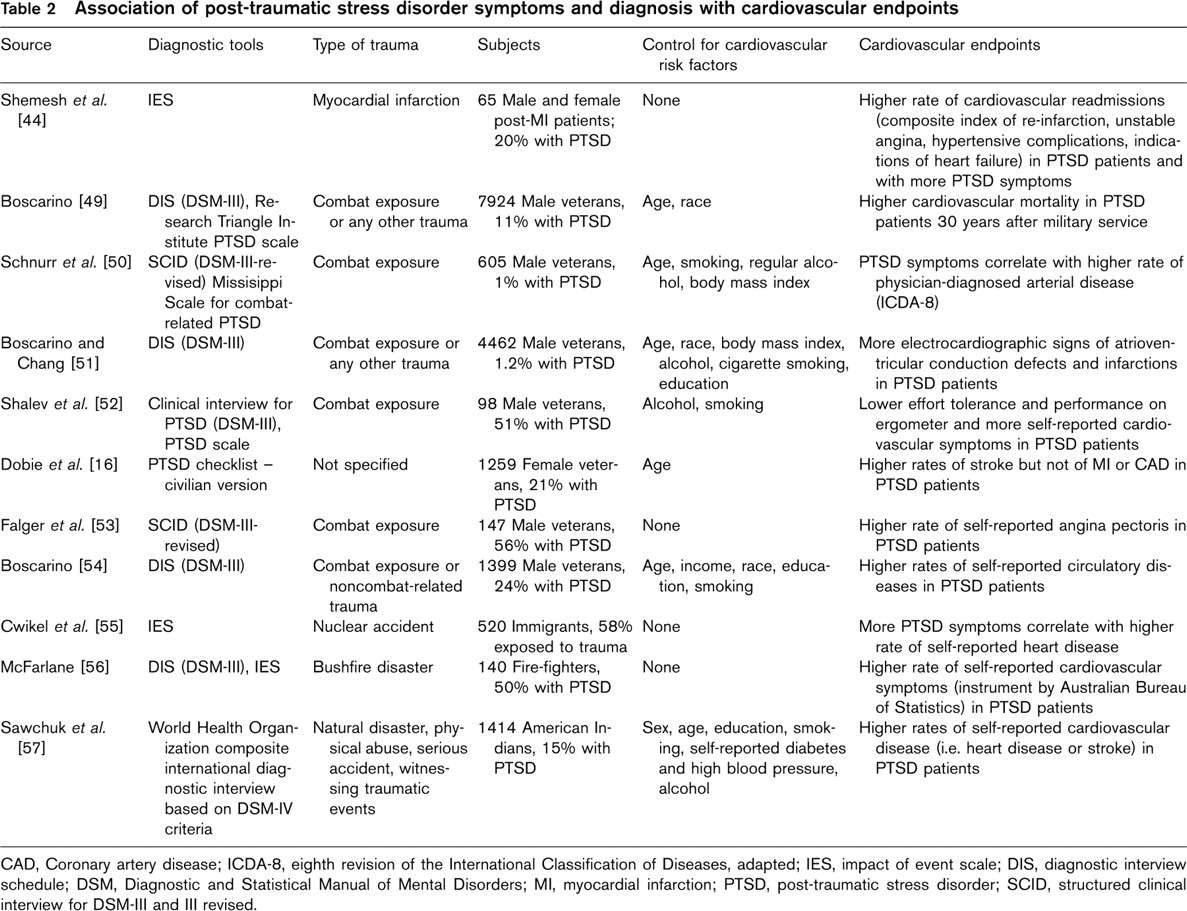
CAD, Coronary artery disease; ICDA-8, eighth revision of the International Classification of Diseases, adapted; IES, impact of event scale; DIS, diagnostic interview schedule; DSM, Diagnostic and Statistical Manual of Mental Disorders; MI, myocardial infarction; PTSD, post-traumatic stress disorder; SCID, structured clinical interview for DSM-III and III revised.
Association of post-traumatic stress disorder with intermediate endpoint measures of atherosclerosis
Table 3 summarizes seven studies on differences in biological markers of atherosclerosis in PTSD patients compared with controls, all performed in non-CVD samples [58–64]. All studies investigated inflammatory changes in serum or plasma previously shown to predict atherosclerotic diseases, namely CRP and IL-6 [21]. The magnitude of effect sizes indicates that differences in pro-inflammatory markers (e.g. CRP, IL-1β, IL-6) and in the anti-inflammatory cytokine IL-4 between PTSD patients and controls are substantial.
Most studies found evidence for a pro-inflammatory state in PTSD although findings are not uniform. For example, CRP correlated with intrusive symptoms in one study [58], but was lower in PTSD patients than in controls in another [59]. Most consistency emerged from two studies showing higher IL-1β in subjects with PTSD compared with controls [59, 60], rendering a weighted effect size of d = 3.8. In one of these studies, IL-1β showed a direct correlation with duration of PTSD [60]. Elevated IL-6 was found in two of three studies [58, 62, 63]. In one of these studies [63], IL-6 became different between groups only after controlling for age, highlighting the notion that this type of analysis should adjust for common covariates (e.g. age) of inflammatory markers. Only one additional study controlled for age, sex, body mass index, and smoking status [59]. However, age, sex, and smoking status were matching criteria in several other studies [61–64]. One study excluded subjects with current alcohol or substance abuse, but maintained those with a current inflammatory condition and taking anti-inflammatory drugs [60].
Peripheral cortisol levels did not significantly correlate with CRP [59], IL-1β [60, 61], soluble IL-2R [60], and IL-6 [63] in all four studies investigating a relationship between the HPA axis activity and inflammation. An association between sympathetic nervous system activity and inflammation was investigated in one study showing a positive correlation between plasma levels of norepinephrine and IL-6 in PTSD patients [63]. Treatment for 10 weeks with either selective serotonin re-uptake inhibitors or placebo similarly lowered IL-1β levels and increased IL-2R levels [60].
Inflammation changes in post-traumatic stress disorder (PTSD) pertinent to atherosclerosis
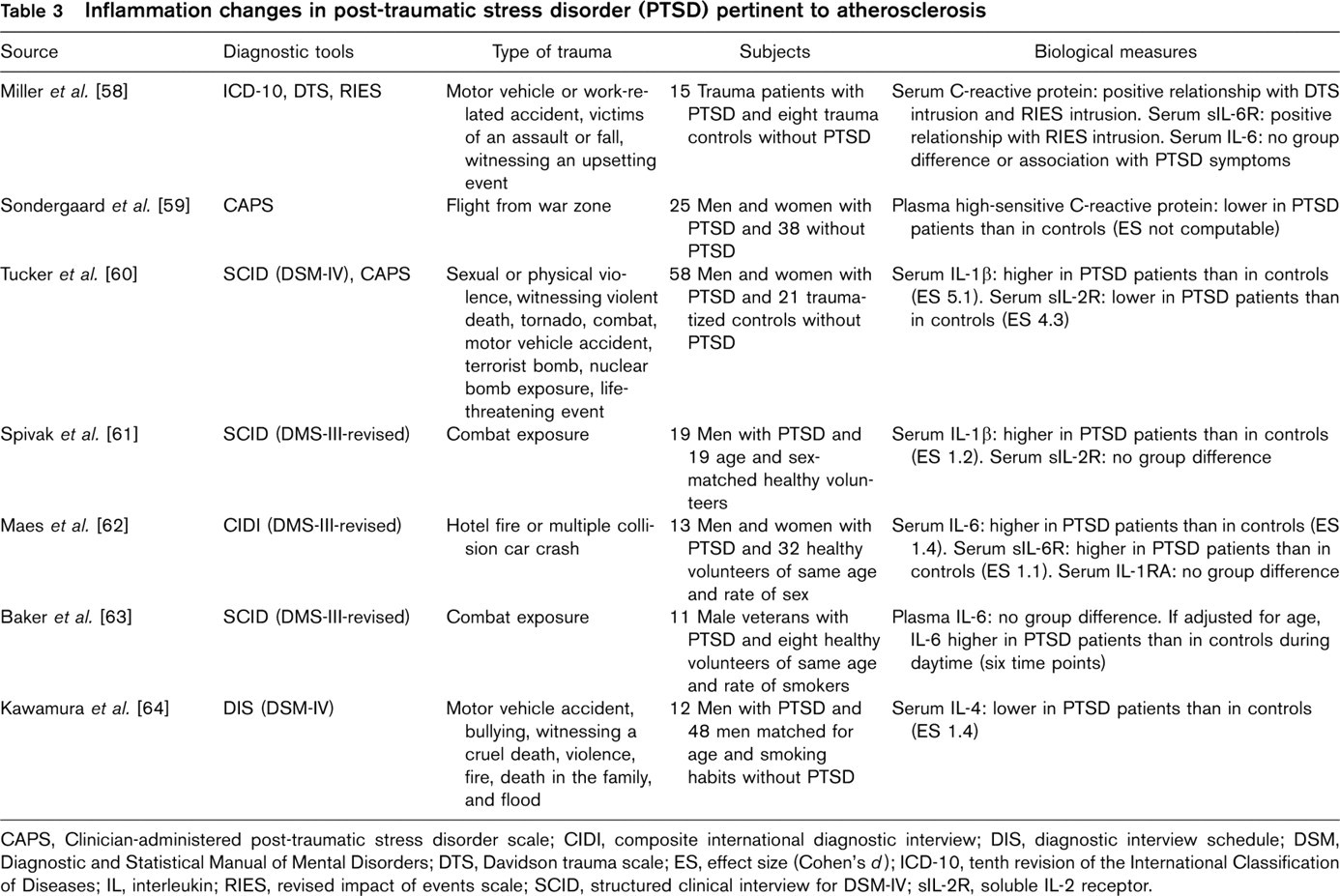
CAPS, Clinician-administered post-traumatic stress disorder scale; CIDI, composite international diagnostic interview; DIS, diagnostic interview schedule; DSM, Diagnostic and Statistical Manual of Mental Disorders; DTS, Davidson trauma scale; ES, effect size (Cohen's d); ICD-10, tenth revision of the International Classification of Diseases; IL, interleukin; RIES, revised impact of events scale; SCID, structured clinical interview for DSM-IV; sIL-2R, soluble IL-2 receptor.
Discussion
Prevalence of post-traumatic stress disorder in post-myocardial infarction patients
With an average prevalence of almost 15%, full-blown PTSD seems to be frequent in post-MI patients, reaching approximately double the prevalence of PTSD in the community [11]. Moreover, the magnitude of this prevalence is comparable with that found for major depression in post-MI patients [13]. The range of PTSD prevalence in post-MI patients was rather wide (i.e. 0–25%). This is not likely a consequence of PTSD definition because we included only studies diagnosing PTSD with instruments following DSM criteria [10]. One explanation for a comparably low prevalence in studies performing a clinical interview [35–37] could be that patients may avoid being interviewed about their heart attack in an attempt to avoid reminders of their traumatic experience [39]. Nevertheless, the derived prevalence of 15% should be interpreted with caution for two reasons. First, all studies were performed in selected clinical samples, and thus did not apply a population sampling framework. Second, all studies asked for PTSD specifically related to MI as the traumatic event, but did not provide information on patients who had PTSD for other reasons. Symptoms of hyperarousal could have emerged non-specifically from different traumas.
One previous study showed that the prevalence of PTSD dropped by 40% between 4–6 weeks and 9 months after MI [32]. We found no convincing evidence that PTSD diminishes over time in post-MI patients. Of note, a recent meta-analysis concluded that the effect of depression on cardiac mortality was significant only after 2 years but not within the first 6 months of mood assessment [65]. Similarly, it may be that PTSD lasting for a longer period or emerging after several months is particularly malignant in terms of cardiac prognosis, although this has yet to be established. With only one study addressing this issue [30], it remains unresolved whether the prevalence of PTSD post-MI is independent of depression.
Considering PTSD in post-MI patients may optimize their clinical management, as, for example, the diagnosis of PTSD correlated with non-adherence to the intake of cardiac medication after MI [43]. Compliance with usual cardiac therapy might be compromised in some patients who avoid cues reminding them of the traumatically perceived infarction. Routine screening for PTSD during cardiac outpatient treatment could thus prompt means to increase adherence with cardiac therapy, thereby perhaps resulting in better cardiovascular outcome. Although sound self-report scales are available for this purpose [46–48], behavioural scientists may want to develop an easy-to-administer screening tool with sufficient sensitivity to detect clinically evident PTSD in post-MI patients. To compare, two single-item questions asking about depressed mood and anhedonia can track major depression with a sensitivity of 90–99% [66]. Trauma-related psychotherapy and selective serotonin reuptake inhibitors are effective treatments for PTSD patients with different types of trauma [22] and might provide comparable benefit for post-MI patients with PTSD. Moreover, sertraline has been shown to be a safe drug in patients with CAD [67].
Association of post-traumatic stress disorder with cardiovascular endpoints
The issue of whether PTSD could be an aetiological factor for atherosclerosis, and therefore have implications for the prognosis of MI patients is of interest both theoretically and clinically. Accumulated findings from a surge of studies suggest that routinely addressing PTSD in cardiac care perhaps reduces cardiovascular morbidity. Some of this reasoning is based on traumatized subjects’ self-reporting of relatively more cardiovascular symptoms [52, 56] and diseases [53–55]. Subjective health complaints are usually less reliable than medical data objectively obtained by physicians. For example, cardiac patients with intrusive thoughts about the MI may interpret chest pain as angina pectoris rather than as a consequence of anxiety-induced atypical chest pain [68]. Nonetheless, PTSD was prospectively related to poor cardiovascular outcome in post-MI patients [44] and in a large population of Vietnam combat veterans [49]. PTSD also correlated with higher rates of physician-diagnosed peripheral arterial disease [50] and electrocardiographic signs of a previous infarction [51].
However, the bulk of studies is cross-sectional, and, moreover, did not co-vary for an acceptable range of known cardiovascular risk factors in analyses. Clearly, prospectively designed studies in larger cohorts need to examine the role of sociodemographic, lifestyle, and classic cardiovascular risk factors, medication, and psychiatric co-morbidity before PTSD can be viewed as an independent CAD risk factor similarly strong to depression [2]. These factors should not be treated as mere confounding variables in all cases, but rather as moderators or mediators of an increased atherosclerotic risk with PTSD. For example, smoking could be an important mechanism by which PTSD leads to poor cardiovascular outcome. All but one study [44] investigated cardiovascular endpoints in relation to a trauma other than MI. Future studies may want to account for the nature of the traumatic exposure because the type of trauma may specifically relate to cardiovascular outcome. For example, non-adherence to medication can be an avoidance cluster phenomenon only if the trauma is the MI itself. If PTSD is confirmed as a cardiovascular risk factor, intervention studies testing whether cardiovascular outcome can be improved in post-MI patients with PTSD seem warranted. Such studies are cumbersome and costly to perform [69], but could rely on effective treatment options [22].
Association between post-traumatic stress disorder and inflammatory changes
One mechanism by which PTSD could contribute to CVD and particularly CAD is by prompting poor health habits [1] such as excessive alcohol consumption and smoking [11, 19]. Another possibility for increased coronary risk with PTSD is a pattern of biological alterations pertinent to atherosclerosis initiation and progression [1]. Our review provides evidence for a pro-inflammatory state in PTSD, as evidenced by a respective change in the pattern of cytokines and CRP in traumatized patients. Perturbation in stress mediators, namely the HPA axis and the autonomic nervous system [70], may partly govern the interplay between post-traumatic stress and biological mediators of atherosclerosis. Patients with PTSD had lower peripheral cortisol levels [71] and higher plasma catecholamine levels both at rest and in response to trauma-specific and trauma-non-specific stimuli than controls [72–74]. Autonomic dysfunction as per sympathetic overactivity, vagal withdrawal, or both is further supported by studies showing reduced heart rate variability and respiratory sinus arrhythmia in PTSD [75, 76]. Importantly, a heart rate with great variability is thought to prevent fatal ventricular tachyarrhythmia [77] and atherosclerosis progression to manifest CAD [78]. Consequently, low heart rate variability has been associated with increased cardiovascular mortality in post-MI patients [79] and an incident risk of MI in the general population [78].
To protect the organism from an overshooting inflammatory stress response, IL-6 increase with stress-induced arousal, such as may occur in individuals re-experiencing a trauma, suppresses the HPA axis via a feedback mechanism [80, 81]. Therefore, lowered glucocorticoid suppression of cytokines could be one explanation for the low-grade systemic inflammation in PTSD. The reviewed literature does not confirm this assumption, given the lack of an association between basal peripheral cortisol levels and inflammatory markers in PTSD patients [59–61, 63]. However, differences in pro-inflammatory cytokines between PTSD patients and controls in relation to the HPA axis activity could unmask when patients engage in a mental stressor or are subject to experimental trauma re-experience.
Norepinephrine correlated positively with IL-6 in PTSD patients [63] compatible with a study demonstrating that catecholamines stimulate systemic IL-6 increase [82]. Also, reduced vagal tone in PTSD might result in increased inflammatory activity during the stress response [83]. Taken together, investigating whether attenuated cortisol activity, attenuated vagal activity and sympathetic overactivity alone or in combination elicit inflammation in PTSD seems one promising avenue of research to understand atherogenetic mechanisms in traumatized individuals better.
Conclusions
Although PTSD is considerably frequent in post-MI patients, its strength as an independent cardiovascular risk factor possibly affecting the outcome of MI patients needs to be established. More work corroborating pro-inflammatory activity and on other biological surrogate markers of atherosclerosis could eminently advance our understanding of biobehavioural pathways linking PTSD with an increased risk of CVD in general and of CAD in particular.
Footnotes
Acknowledgements
The authors wish to thank Lina Wiedemar for the helpful literature search.