
Abstract
Background and purpose
Previous studies have suggested that blood pressure is a particularly important risk factor for stroke in Chinese, and that the magnitude of the effect may be greater than in Caucasians. We performed a meta-analysis in order to define the magnitude of the risk of stroke associated with hypertension among Chinese, and to compare the magnitude of this risk with Caucasians.
Methods
We searched Medline from 1966 to 2004, plus Chinese Medical Literature databases from 1977 to 2003 for Caucasian and Chinese studies. Results were pooled using the random effects model, and heterogeneity and publication bias were checked.
Results
For a 10 mmHg increase in systolic blood pressure, the pooled risk ratio was 1.44 [95% confidence interval (CI)] 1.39–1.51 for ischaemic stroke, and 1.5 (95% CI 1.45–1.57) for haemorrhagic stroke in Chinese, versus 1.19 (95% CI 1.15–1.23) for total stroke in Caucasians. The pooled odds ratio for hypertension measured dichotomously (defined as >160/95 mmHg) was 5.8 (95% CI 4.7–7.2) among Chinese versus 1.93 (95% CI 1.7–2.2) among Caucasians for ischaemic stroke; and 7.2 (95% CI 5.3–9.7) in Chinese versus 3.1 (95% CI 2.5–3.9) in Caucasians for haemorrhagic stroke.
Conclusion
The risk of stroke associated with hypertension is consistently and significantly greater in Chinese than Caucasians. This may help genetic epidemiologists to dissect the cause of stroke, and emphasizes the particular importance of hypertension control in the Chinese population. Eur J Cardiovasc Prev Rehabil 13:429–437 © 2006 The European Society of Cardiology
Keywords
Introduction
It is increasingly apparent that the spectrum of cardiovascular disease (CVD) among Chinese is very different than in Caucasians. Whereas coronary heart disease (CHD) predominates in Caucasians, stroke predominates in Chinese. Intracerebral haemorrhage occurs between two and three times more frequently in Chinese than in Caucasians. Only 6–18% of strokes in European populations are reported as intracerebral haemorrhages compared with 23–52% haemorrhagic strokes in Chinese [1, 2].
The mortality from stroke is commensurately high. Among the Chinese population, the mortality rate for stroke is three times higher than that for coronary heart disease [3], and haemorrhagic strokes also have a higher case-fatality rate than ischaemic strokes [3].
The reasons for this ethnic difference are slowly being teased out. A population-based incident case-control study found that the prevalence, odds ratio (OR), and population attributable risk (PAR) for stroke risk factors varied between ethnic groups [4]. Our previous work also observed that there were differences in the prevalence of hypertension, the magnitude of stroke risk associated with hypertension, and the PAR for hypertension between Chinese and Caucasians [5]. Other studies also confirm that the PAR of stroke associated with hypertension is higher in Chinese [6], and in East Chinese [7] than in Caucasians. Diet might explain at least part of this difference. For example, the International Study on Macronutrients and Blood Pressure (INTERMAP) found that macronutrient intakes were much higher in Western diets for total fat, saturated and trans fatty acids, key dietary lipid scores and sugars, but lower in total carbohydrate and starch. Dietary sodium was higher, but potassium lower, hence the sodium/potassium ratio was higher in the Asian diet. Higher salt intake may be part of the mechanism for hypertension among Chinese [8].
A comprehensive and quantitative summary of this data can be obtained by performing a meta-analysis. Indeed, a meta-analysis of the literature up to 1994 supported the view that hypertension had a more severe effect on stroke in Chinese than in Caucasians, although this was heterogeneous [6]. In the present study, we update this meta-analysis with two aims: first, to define the magnitude of the risk of ischaemic and haemorrhagic stroke separately associated with hypertension among Chinese; and second, to compare the magnitude of this risk with Caucasians.
Methods
Data collection
Selection of studies for review
For Chinese studies, firstly, we searched Medline from 1966 to April 2004 with the following strategy: stroke (MeSH) or ischaemic stroke (MeSH) or haemorrhagic stroke (MeSH) AND risk factors (MeSH) AND hypertension (MeSH) or blood pressure (key words); limited to Chinese. Secondly, we updated the previous meta-analysis of Chinese studies [6] by searching the Chinese Medical Literature database to 2003 (strategy available from authors on request).
For Caucasian studies we searched Medline data from 1966 to 2004 with the following strategy: stroke (MeSH) or ischaemic stroke (MeSH) or haemorrhagic stroke (MeSH) AND risk factors (MeSH) AND hypertension (MeSH) or blood pressure (key word) AND cohort or prospective study (MeSH) AND incidence (MeSH); limited to human and English. For case-control studies, the strategy was similar except that the term case-control was used instead of cohort. The searches were supplemented by personal files and expert knowledge.
Inclusion/exclusion criteria
The inclusion criteria were cohort or case-control design; outcome was reported for ischaemic or haemorrhagic stroke separately; multiple regression analysis was used and coefficients or odds ratios reported. Duplicate studies, or studies lacking any adjustment for confounders were excluded.
Statistical methods
Results were weighted and pooled using the inverse variance method [6]. Heterogeneity was assessed using a Q-test with a significance level of 0.1. Publication bias was assessed using funnel plots and the Egger test. Risk ratios (RR) or ORs and 95% confidence intervals (CIs) are presented after antilogarithmic transformation. We calculated the pooled measure of effect for hypertension measured in two ways: continuously, per 10mmHg increase in systolic blood pressure (SBP) or dichotomously using a threshold of SBP >160 mmHg or DBP >95 mmHg. Ischaemic or haemorrhagic stroke were analysed separately. If the study reported the coefficient and standard error for a 1 mmHg increase in SBP this was converted to estimate the effect of a 10 mmHg increase by multiplying the initial estimate and standard error by 10. Pooled ORs were obtained for Chinese and Caucasians separately. If heterogeneity was present, a meta-regression model including age, cholesterol, diabetes, smoking and follow-up years (where available) was used to try to ascertain the reasons for this. If the source of the heterogeneity could not be identified, data were pooled using a random effects model. STATA statistical software 7.0 (STATA, College Station, Texas, USA) was used.
Results
Only one of the 67 articles on Medline was potentially eligible [9], but it only reported the association of total fatal stroke with hypertension defined dichotomously (160/95 mmHg), and was therefore excluded [9]. From a previous meta-analysis for stroke [6], 12 studies were identified; six of these were excluded for the following reasons: reporting only fatal stroke (n = 2) [10, 11]; not reporting 95% CI (n = 3) [12–14]; different cut-off for hypertension (n = 1) [15]. This search was updated using the Chinese Medical Literature database: 223 references were identified, of which 12 were new, potentially eligible studies [16–27]. Six studies were excluded because of the following reasons: they did not adjust for other co-variables (n = 4) [17, 20, 23, 27]; they used a different cutoff for hypertension (n = 1) [24]; they reported total stroke only (n = 1) [19], leaving six eligible studies. Hence, the six studies identified from the Chinese Medical Literature database [16, 18, 21, 22, 25, 26] and the six studies identified from the previous meta-analysis [6], plus our own previous study [5], led to 13 studies being included in this meta-analysis.
Characteristics of Chinese studies treating hypertension as a continuous variable

Adjusted Cox proportional model hazard ratio (95% confidence interval) of stroke associated with a 10 mmHg increase in systolic blood pressure. RR, risk ratio.
Characteristics of Chinese studies treating hypertension as a dichotomous variable
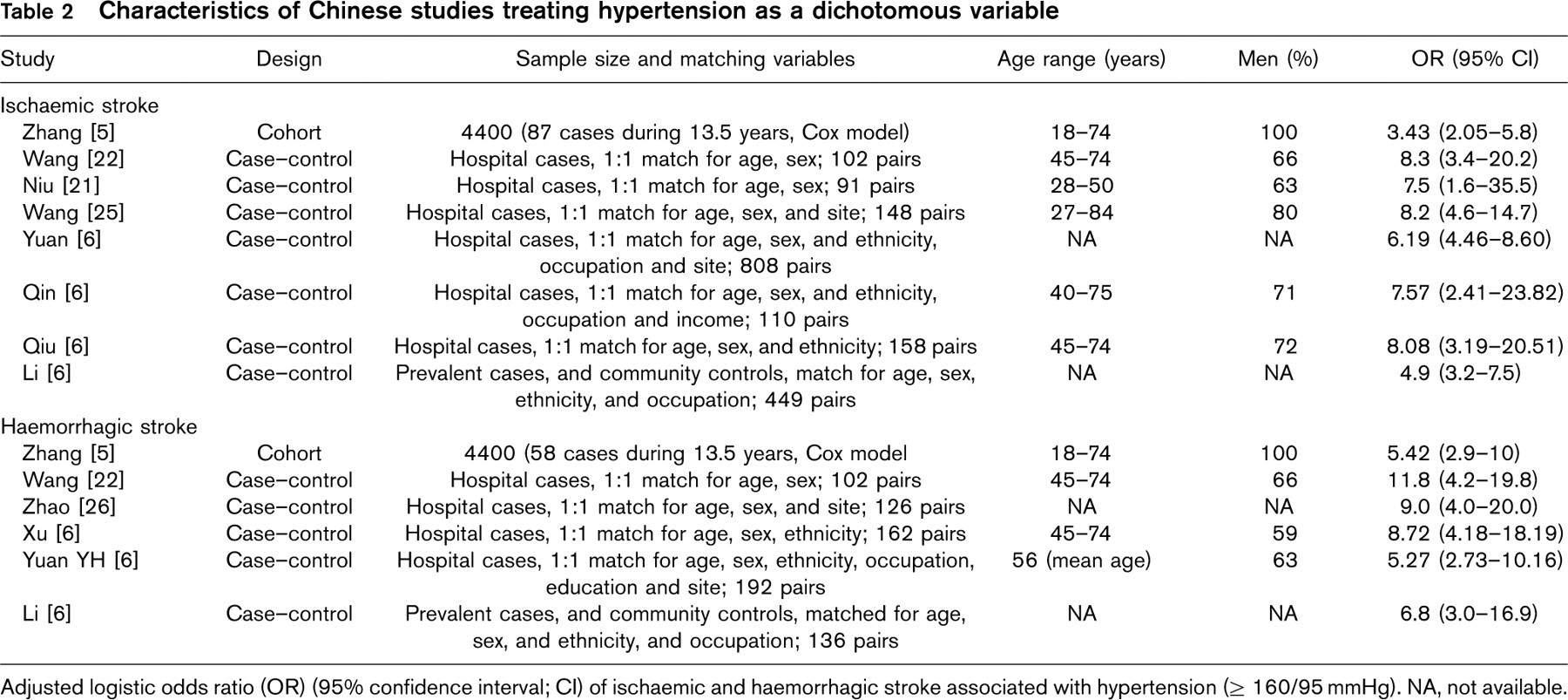
Adjusted logistic odds ratio (OR) (95% confidence interval; CI) of ischaemic and haemorrhagic stroke associated with hypertension (>160/95 mmHg). NA, not available.
Eleven cohort studies [28–38] were potentially eligible from 771 references identified for hypertension treated as a continuous variable. Among these, four studies reported only fatal stroke [29, 31, 34, 35] leaving seven cohort studies for inclusion in this meta-analysis.
Out of 280 references, 20 studies [39–55] reporting hypertension as a dichotomous variable (>160/95 mmHg) were potentially eligible. Eight of these did not identify the type of stroke [29, 36, 48–50, 52–54] leaving 12 studies for inclusion. One previous meta-analysis [56] identified a further three studies meeting inclusion criteria [57–59]. Thus, in total, seven cohorts and 15 case-controls were included.
Chinese studies
Tables 1 and 2 present the details of the studies on mainland China. The three cohorts and 10 case-control studies report 3160 stroke events in total.
Hypertension as a continuous variable
Ischaemic stroke Figure 1 shows the Peto plot for the three Asian cohort studies assessing the association between a 10mmHg increase in SBP and ischaemic stroke. There was no heterogeneity (P=0.256) and no publication bias (P = 0.12) among these three individual studies. The pooled coefficient indicated a risk of 1.44 (95% CI 1.39–1.51) for each 10mmHg rise in SBP.
Haemorrhagic stroke Figure 1 also shows the Peto plot for the three Asian cohort studies assessing the association between a 10mmHg increase in SBP and haemorrhagic stroke. There was no heterogeneity (P = 0.454) but there was evidence of publication bias (P = 0.019), although with only three studies this significance is questionable. The pooled coefficient indicated a risk of 1.51 (95% CI 1.45–1.57) for each 10mmHg rise in SBP.
Hypertension as a dichotomous variable
Ischaemic stroke Figure 2 shows the Peto plot for eight studies assessing hypertension (as a dichotomous variable) and the OR of ischaemic stroke. There was no heterogeneity (P = 0.381), and no publication bias (P = 0.41). The pooled OR of ischaemic stroke associated with hypertension was 5.8 (95% CI 4.7–7.2).
Haemorrhagic stroke Figure 3 shows the Peto plot for six studies assessing hypertension as a dichotomous variable and odds ratio of haemorrhagic stroke. Again, there was no heterogeneity (P = 0.579) and no publication bias (P=0.157). The pooled OR of haemorrhagic stroke associated with hypertension was 7.2 (95% CI 5.3–9.7).
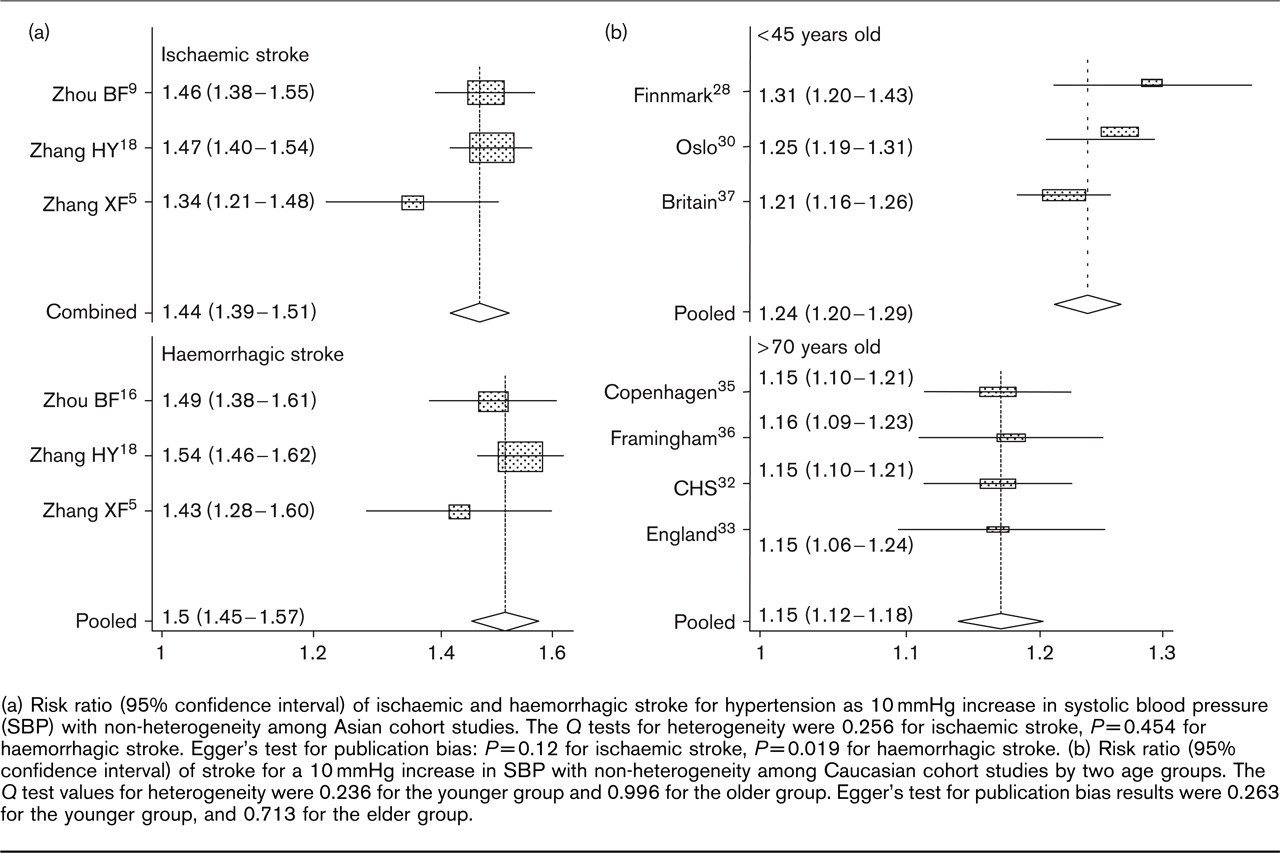
(a) Risk ratio (95% confidence interval) of ischaemic and haemorrhagic stroke for hypertension as 10 mmHg increase in systolic blood pressure (SBP) with non-heterogeneity among Asian cohort studies. The Q tests for heterogeneity were 0.256 for ischaemic stroke, P = 0.454 for haemorrhagic stroke. Egger's test for publication bias: P = 0.12 for ischaemic stroke, P =0.019 for haemorrhagic stroke. (b) Risk ratio (95% confidence interval) of stroke for a 10mmHg increase in SBP with non-heterogeneity among Caucasian cohort studies by two age groups. The Q test values for heterogeneity were 0.236 for the younger group and 0.996 for the older group. Egger's test for publication bias results were 0.263 for the younger group, and 0.713 for the elder group.
Caucasian studies
Tables 3 and 4 present the details of Caucasian studies. The seven cohorts and 15 case-control studies report over 7000 stroke events in total.
Hypertension as a continuous variable
Seven cohort studies assessed hypertension (as a continuous variable) and risk of total stroke. This estimate showed heterogeneity (P = 0.024) but no evidence of publication bias (P = 0.751). The pooled OR was 1.19 (95% CI 1.15–1.23) for each 10mmHg increase in SBP. It was not possible to sub-divide this into ischaemic or haemorrhagic strokes because no studies reported these data separately. It is well established, however, that in Caucasians the majority of these (>80%) would be ischaemic stroke [1].
Meta-regression did not demonstrate reasons for heterogeneity but we suspected age, and hence divided studies into two age groups: average age ≤45 and ≥70 years old. A test for heterogeneity was not significant (P = 0.236), and there was no indication of publication bias (P = 0.263) among the three younger cohort studies; the pooled OR was 1.24 (95% CI 1.20–1.29) for each 10 mmHg increase in SBP (Fig. 1). For the four older Caucasian cohort studies, there was no indication of heterogeneity (P = 0.996), or publication bias (P = 0.713) (Fig. 1) and the pooled OR was 1.15 (95% CI 1.12–1.18) for each 10mmHg increase in SBP.
Hypertension as a dichotomous variable
Ischaemic stroke Figure 2 shows the Peto plot for 10 studies assessing hypertension (as a dichotomous variable) and risk of ischaemic stroke. There was no heterogeneity (P = 0.12), and no publication bias (P = 0.31). The pooled OR for ischaemic stroke risk was 1.96 (95% CI 1.66–2.30).
Haemorrhagic stroke Figure 3 shows the Peto plot for seven studies assessing hypertension as a dichotomous variable and risk of haemorrhagic stroke. There was no heterogeneity (P = 0.11), and no publication bias (P=0.56). The pooled OR for haemorrhagic stroke was 3.11 (95% CI 2.39–4.05).
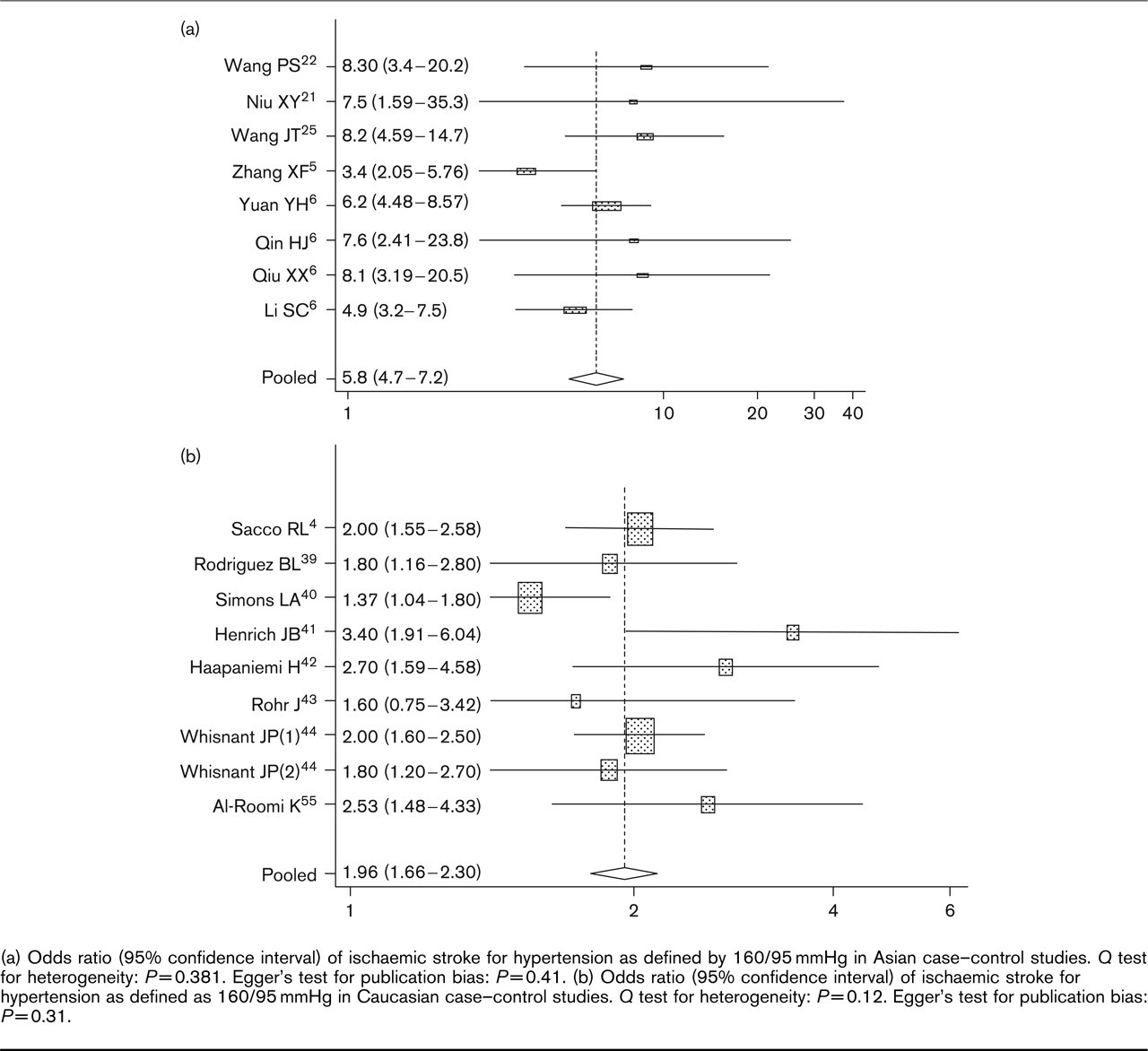
(a) Odds ratio (95% confidence interval) of ischaemic stroke for hypertension as defined by 160/95mmHg in Asian case-control studies. Q test for heterogeneity: P = 0.381. Egger's test for publication bias: P = 0.41. (b) Odds ratio (95% confidence interval) of ischaemic stroke for hypertension as defined as 160/95 mmHg in Caucasian case-control studies. Q test for heterogeneity: P = 0.12. Egger's test for publication bias: P = 0.31.
Discussion
Our meta-analysis is the first to address both Caucasian and Asian populations, and the most significant finding is that the magnitude of the effect of hypertension, whether measured continuously or dichotomously, on the risk of ischaemic or haemorrhagic stroke is significantly higher in Chinese than in Caucasians. These results are consistent with other studies: for example, a meta-analysis in the Asia Pacific region indicated that a 10mmHg lower SBP was associated with 41% lower stroke risk in Asia and 30% lower stroke risk in Australia [60]. This has implications at the population level.
The population attributable risks for stroke associated with hypertension in Chinese are 31% for ischaemic and 42% for haemorrhagic [5] compared with 25 and 34%, respectively, in Caucasians [4, 46]. This highlights the need to target hypertension as a public health issue and preventive measure in China. Current evidence indicates that the rate of control of hypertension is lower than in Caucasians. For example, among hypertensive patients, only 45% were aware of their high blood pressure, 28% were taking antihypertensive medicine, and 8% achieved blood pressure control (140/90 mmHg) [61]. Decreasing the incidence of hypertension may entrain certain reductions in stroke beyond that expected from the PAR. For example, in China, the prevalence of smoking is much higher than in Western countries [3, 5], and the deleterious impact on stroke, particularly for ischaemic stroke, may be potentiated in combination with hypertension.
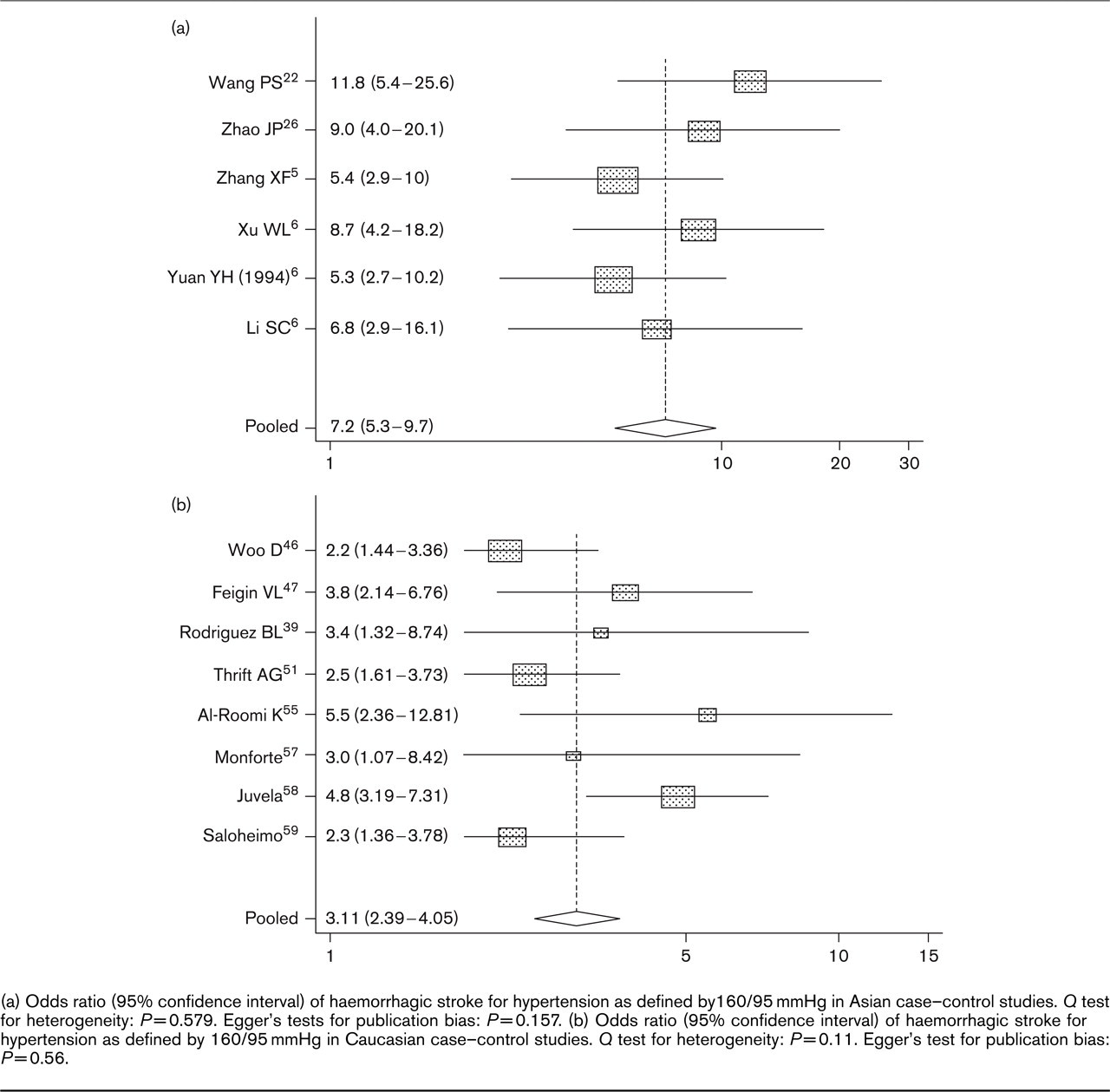
(a) Odds ratio (95% confidence interval) of haemorrhagic stroke for hypertension as defined by 160/95 mmHg in Asian case-control studies. Q test for heterogeneity: P = 0.579. Egger's tests for publication bias: P = 0.157. (b) Odds ratio (95% confidence interval) of haemorrhagic stroke for hypertension as defined by 160/95 mmHg in Caucasian case-control studies. Q test for heterogeneity: P = 0.11. Egger's test for publication bias: P = 0.56.
The reasons for this difference between blood pressure and stroke risk among Chinese and Caucasians are uncertain. It could be partially confounded by other factors, such as a higher proportion of the study population on antihypertensive medications in Caucasians versus Chinese, or the differential effect and distribution of hypercholesterolaemia on ischaemic and haemorrhagic stroke. It could also indicate a difference in genetic make-up or environmental factors between ethnic groups. For example, Chinese in New York City had a greater proportion of deaths due to haemorrhagic stroke than did whites in New York although there were similar rates of total stroke for both New York Chinese and whites. Haemorrhagic stroke deaths among New York City Chinese were intermediate between Chinese in China (highest) and New York City Caucasians (lowest) [62].
Characteristics of Caucasian studies treating hypertension as a continuous variable
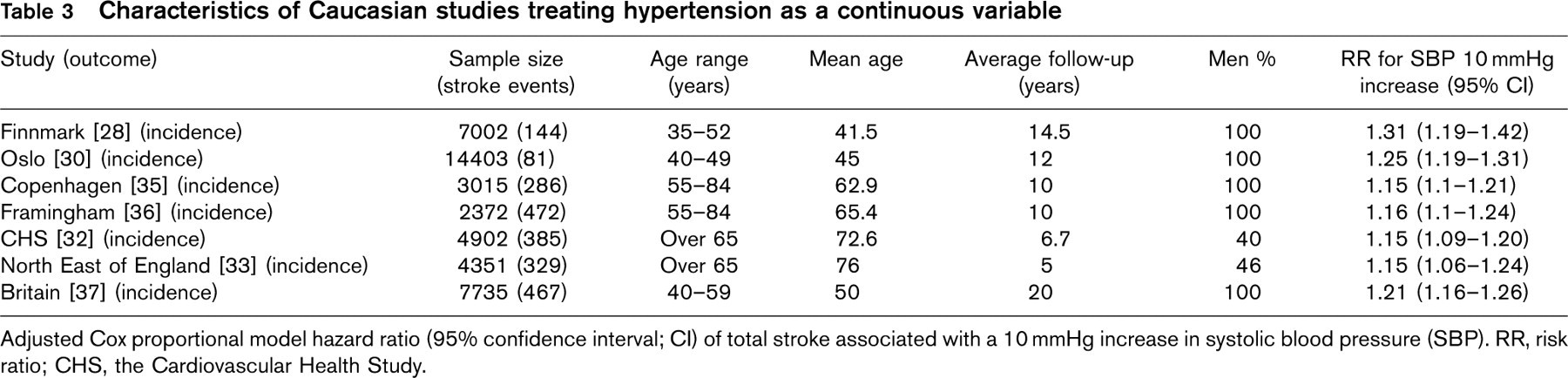
Adjusted Cox proportional model hazard ratio (95% confidence interval; CI) of total stroke associated with a 10 mmHg increase in systolic blood pressure (SBP). RR, risk ratio; CHS, the Cardiovascular Health Study.
Characteristics of Caucasian studies treating hypertension as a dichotomous variable
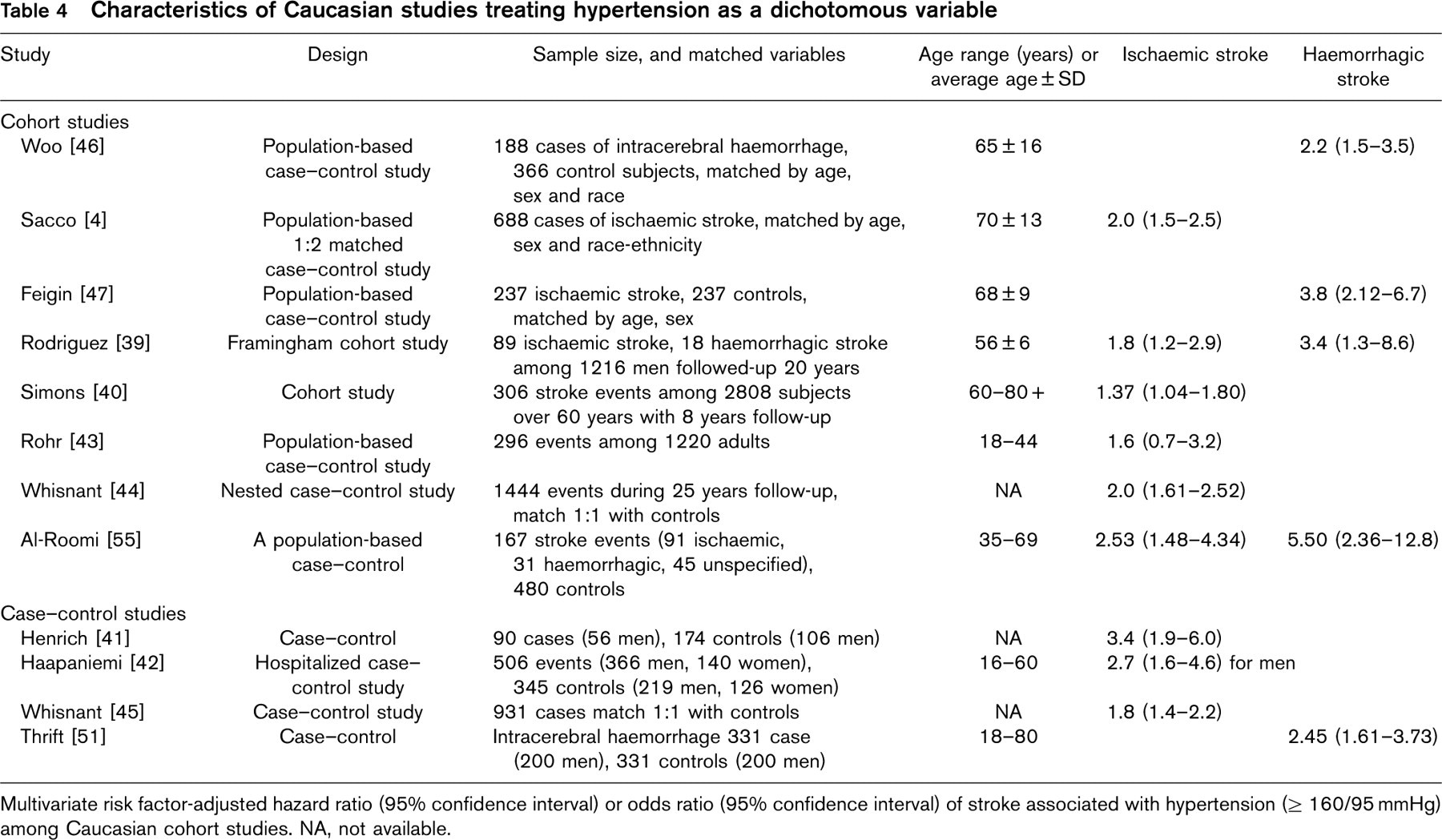
Multivariate risk factor-adjusted hazard ratio (95% confidence interval) or odds ratio (95% confidence interval) of stroke associated with hypertension (>160/95 mmHg) among Caucasian cohort studies. NA, not available.
Conclusion
This is first meta-analysis to compare the effect of hypertension on ischaemic and haemorrhagic stroke between Chinese and Caucasians, respectively. The ORs and RRs of both ischaemic and haemorrhagic stroke are consistently and significantly greater in Chinese than Caucasians. Such ethnic differences may assist genetic epidemiologists to dissect the causes of stroke, but also emphasizes that public health interventions targeting hypertension control among Chinese are critical in order to avoid the high morbidity and mortality of cardiovascular diseases.