
Abstract
Background
Major risk factors do not entirely explain the worldwide variability of morbidity and mortality due to cardiovascular disease. Environmental exposures, including drinking water minerals may affect cardiovascular disease risks.
Method
We conducted a qualitative review of the epidemiological studies of cardiovascular disease and drinking water hardness and calcium and magnesium levels.
Results
Many but not all ecological studies found an inverse (i.e., protective) association between cardiovascular disease mortality and water hardness, calcium, or magnesium levels; but results are not consistent. Some case-control studies and one cohort study found either a reduced cardiovascular disease mortality risk with increased drinking water magnesium levels or an increased risk with low magnesium levels. However, the analytical studies provide little evidence that cardiovascular risks are associated with drinking water hardness or calcium levels.
Conclusion
Information from epidemiological and other studies supports the hypothesis that a low intake of magnesium may increase the risk of dying from, and possibly developing, cardiovascular disease or stroke. Thus, not removing magnesium from drinking water, or in certain situations increasing the magnesium intake from water, may be beneficial, especially for populations with an insufficient dietary intake of the mineral.
Introduction
Cardiovascular diseases (CVD) are among the leading causes of morbidity and mortality in industrialized countries. Hypertension, tobacco smoking, diabetes, dyslipidemia, obesity and physical inactivity are major risk factors for the disease [1–3], but they do not entirely explain the worldwide variability of CVD [4]. Environmental exposures including drinking water hardness or minerals that contribute to hardness may also affect CVD risks.
Interest in a ‘water factor’ can be traced to research in 1956 and 1957. Enterline and Stewart [5] called attention to the marked geographical variation in death rates from heart disease for the US during 1949–1951, and Kobayashi [6] associated mortality from apoplexy with the acidity of river water (i.e., the ratio of sulfates to carbonates) in Japan. Since then, investigators throughout the world have reported lower CVD mortality rates in hard water areas. The hypothesized beneficial effect may be due to high levels of calcium or magnesium in hard water; other constituents in some hard waters (e.g., selenium); reduced levels of toxics such as lead, which may be present in soft, low pH water [7–13].
Methods
This review focuses on epidemiological studies published since 1979, because studies published before that date have been reviewed extensively and are summarized briefly here [14–20]. Articles were identified from the Medline database. References in these articles were checked for other articles. We excluded articles written in languages other than English and articles that did not report a correlation coefficient (r) or quantitative measure for the association. No attempt was made to identify unpublished research, but abstracts in recent epidemiological meeting reports were searched.
A meta-analysis was not performed because of the heterogeneity of the measures of effect and exposure. Information from physiological, pathophysiological, and experimental studies was reviewed to help interpret the results of the epidemiological studies.
Drinking water hardness, defined as the sum of all polyvalent cations, is expressed in several ways [21]. We reported or computed hardness as CaCO3 equivalent levels in milligrams per litre. The principal hardness-causing cations are calcium and magnesium.
Results
Epidemiological studies published through 1978
More than 50 ecological (geographical correlation) studies were published from 1957 to 1978. Studies were conducted in the US, England and Wales, Canada, Sweden, the Irish Republic and Northern Ireland, The Netherlands, Finland, Italy, Romania, Bohemia and Moravia, Scotland, Germany, Japan, Australia, and Hungary. Populations in 21 cities around the world were also studied. Comstock [18, 19] reviewed these studies based on size of geographical areas (national or international; province or state; county, borough, or city).
Most studies reported associations between drinking water hardness and mortality from all CVD, arteriosclerotic and degenerative heart disease, hypertensive disease, and stroke [18, 19]. Associations were reported for both men and women but were often statistically significant for one sex only. A beneficial effect of hardness was found in most studies involving large geographical areas, but findings of studies in smaller areas tended to be inconclusive or non-beneficial [14]. For example, when all of Canada was considered, decreased CVD mortality was associated with increased municipal drinking water hardness, but when the same data were analyzed for individual provinces, this association was only found in Quebec and Ontario provinces [16–19, 22].
Most studies considered r, which provides no indication of the strength of the association [18, 19]. In fact, r is a measure of the scatter of the data points around an underlying linear trend; the greater the spread of the points, the lower the correlation [23]. Comstock estimated the relative risk (RR) associated with soft water in several studies (0 mg/l hardness) compared with hard water (200 mg/l hardness) [18, 19, 22, 24–26]. A 19–25% higher risk of death from all CVD was associated with soft water (0 mg/l compared to 200 mg/l hardness) in England and Wales (RR = 1.19) and the US (RR = 1.25), respectively. For deaths from arteriosclerotic heart disease (AHD) and stroke in Canada, the RR was 1.07 and 1.15; RRs in Colorado ranged from 1.01 to 1.19 depending on altitude and river basin.
Sharrett and Voors [20, 27] evaluated other water constituents including chromium, copper, zinc, cadmium, selenium, silicon and lead. Both concluded that the evidence was inconsistent and inconclusive in regard to an association (either protective or detrimental) with CVD.
Comstock discovered errors in six of seven studies where investigators evaluated changes in mortality following changes in hardness either due to softening or replacing a soft surface water source with a hard groundwater source. After a reanalysis of five studies, Comstock [18, 19] found that the mortality either remained high or did not decrease among populations when a soft water source was replaced with a hard water source. The most convincing study was conducted in 83 towns in the United Kingdom; after standardizing for socio-economic status, investigators found that, in nine of 11 towns where water hardness changed, mortality changes were consistent with the hypothesis that hard water is beneficial [28, 29].
Epidemiological studies published after 1978: ecological studies
Eighteen ecological studies were reviewed (Table 1) [30–47]. Some studies took into account potential confounders such as age, gender, socio-economic status, income or climate [31, 38, 40–42, 45, 46].
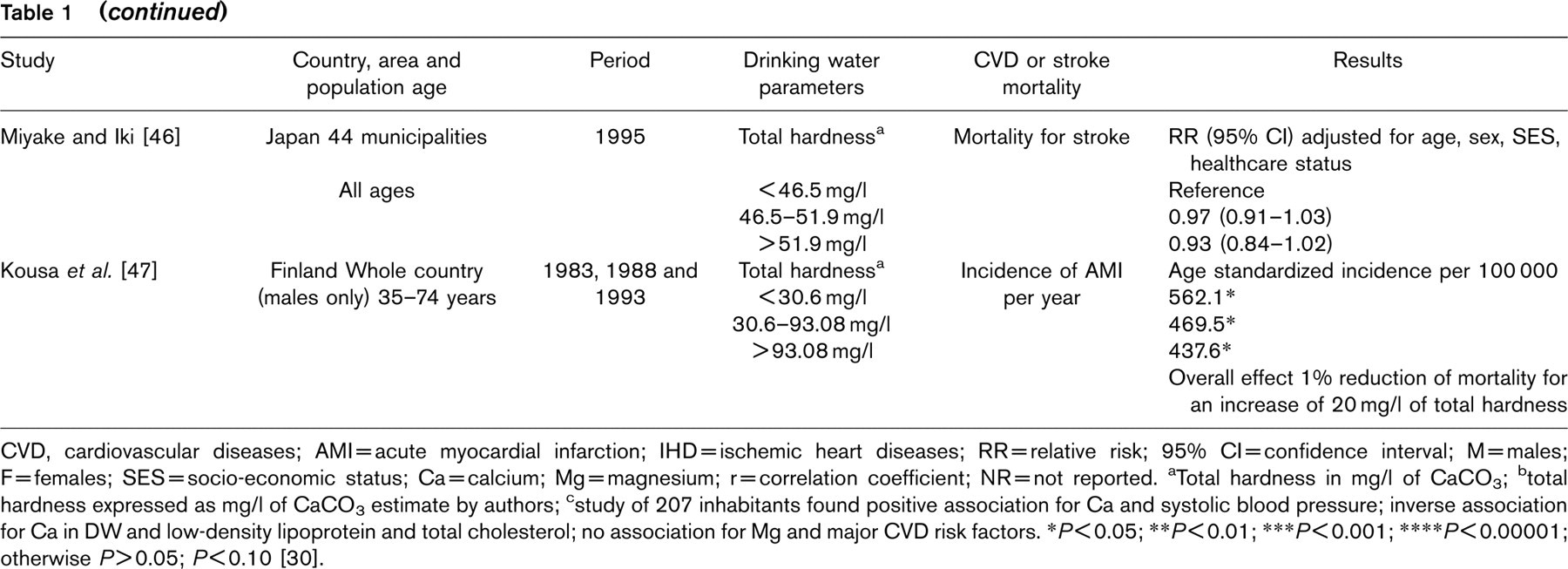
Eleven studies reported a statistically significant inverse (i.e., protective) association between CVD mortality and either drinking water hardness, magnesium, or calcium [30, 33–35, 37, 40, 41, 43–45, 47]. Six studies found no statistically significant association [31, 32, 36, 38, 42, 46]. In Norway [39] a positive association was reported between drinking water magnesium and mortality due to IHD and stroke, but these findings are questionable because virtually all municipalities in the study had soft water and magnesium was quite low. Three of these studies estimated the effect of drinking water hardness. A 7.5% reduction of CVD mortality in men for 100 mg/l increased water hardness was reported in England and Wales [34]. In Finland [47], the risk of acute myocardial infarction (AMI) decreased 0.56% for each 10 mg/l increase in water hardness. A 10% increase in the risk of ischemic heart disease (IHD) mortality was reported in Taiwan municipalities [41] with under 75 mg/l water hardness compared with those with over 150 mg/l hardness.
Ecological (geographic correlation) studies on the relationship etween cardiovascular diseases or stroke and hardness or calcium/magnesium concentration of drinking water
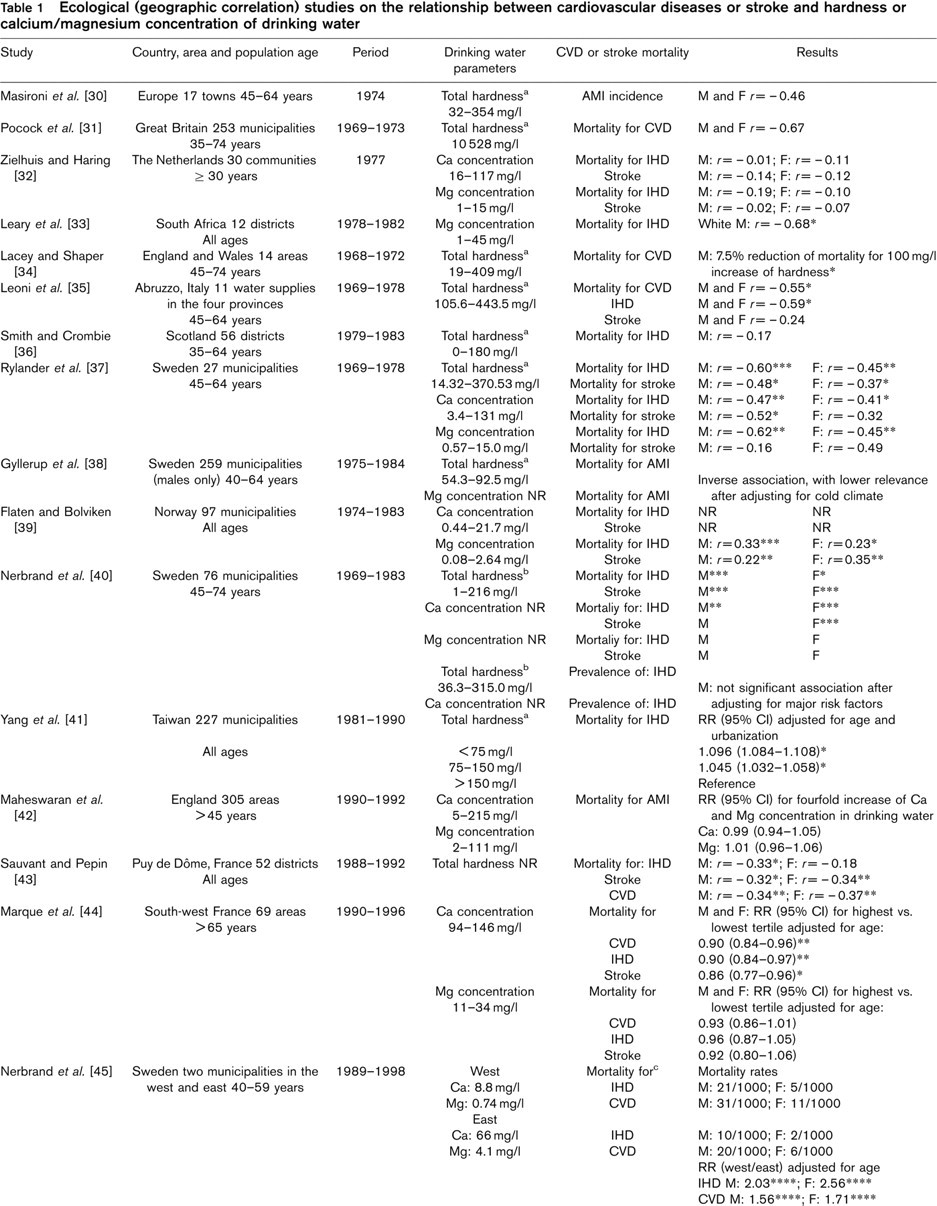
CVD, cardiovascular diseases; AMI = acute myocardial infarction; IHD = ischemic heart diseases; RR=relative risk; 95% CI = confidence interval; M = males; F = females; SES = socio-economic status; Ca = calcium; Mg = magnesium; r = correlation coefficient; NR = not reported. aTotal hardness in mg/l of CaCO3; btotal hardness expressed as mg/l of CaCO3 estimate by authors; cstudy of 207 inhabitants found positive association for Ca and systolic blood pressure; inverse association for Cain DWand low-density lipoprotein and total cholesterol; no association for Mg and major CVD risk factors. ∗P<0.05; ∗∗P <0.01; ∗∗∗P<0.001; ∗∗∗∗P<0.00001; otherwise P>0.05; P<0.10 [30].
Nine studies [32, 33, 37–40, 42, 44, 45] considered drinking water magnesium or calcium, but one [40] did not report the concentrations. Three studies reported a relative risk (RR) for calcium and magnesium [42, 44, 45], and two studies reported a RR for total hardness [41, 46]. Marque et al. [44] found a statistically significant protective effect for cardiovascular mortality at calcium levels of 94–146 mg/l (RR: 0.90) and at magnesium levels of 4–11 mg/l (RR: 0.90). Maheswaran et al. [42] failed to find an association between AMI mortality in England and drinking water calcium and magnesium levels of 5–215 and 2–111 mg/l, respectively. In Taiwan, a significant increase of RR for IHD mortality was associated with drinking water hardness of less than 150 mg/l [41]. In Japan, no statistically significant decrease in the RR for stroke mortality was observed with water hardness higher than 51.9 mg/l [46].
Nerbrand et al. [40, 45] conducted two studies in Sweden. In a study of 76 communities in mid-Sweden, IHD and stroke mortality decreased with increased drinking water hardness and calcium [40]. No association was found between drinking water hardness and non-fatal IHD among 14 675 subjects randomly selected from these communities [40]; investigations took into account information about potential confounders including smoking habits, preference for fatty foods, use of antihypertensive drugs, physical activity, and a measure for stress.
In two rural communities in Sweden where CVD and IHD mortality was significantly greater in the soft water community, Nerbrand et al. [45] also conducted a cross-sectional study of the prevalence of CVD risk factors. Tap water samples, clinical specimens, and dietary information were collected from 207 randomly selected subjects. Median levels of calcium and magnesium in the household drinking water of subjects was 12.5 and 3.3 mg/l in the soft water community and 58 and 5.4 mg/l in the other community, respectively. Significant associations were found between major CVD risk factors and drinking water calcium levels but not for drinking water magnesium or calcium and magnesium in the diet. The investigators concluded that drinking water calcium might be a factor in the complexity of relationships of CVD risk factors. Household water accounted for small amounts of the daily intake for calcium and magnesium in both communities. Paradoxically, total calcium and magnesium intakes were higher in subjects living in the softer water community due to a higher intake of food rich in these minerals. There was no difference between the two populations in mean serum or urine levels of calcium, and magnesium, and no association was found between drinking water calcium or magnesium levels and calcium or magnesium levels in serum or urine.
Epidemiological studies published after 1978: case-control studies
Associations between CVD mortality and calcium or magnesium in drinking water were investigated in Finland, Taiwan, and Sweden (Table 2) [48–54]. Five of the seven studies found a statistically significant inverse association between magnesium levels in drinking water and mortality risks for AMI, stroke, or hypertension; one study found a significant inverse association between AMI and both calcium and magnesium levels [52]. Investigators considered major CVD risk factors in two studies [53, 54]; these were the only studies that found no significant association with either mineral.
In a small study in Finland, Luoma et al. [48] found that the risk of AMI mortality among 58 men increased as drinking water magnesium decreased. Both hospital and population control series were included. A statistically significant greater than fourfold increased risk was found among men at the lowest drinking water magnesium levels (<1.2 mg/l) as compared with those at the highest magnesium levels (> 3.0 mg/l) only using population controls. The risk estimates may have been underestimated, as the study included subjects with prolonged chest pain without definitive evidence of AMI. Tap water samples were collected and analyzed for individual exposure estimates; 60–70% of participants had used the same water for more than 10 years.
Case-control studies on the relationship between cardiovascular diseases and hardness or calcium/magnesium concentrations of drinking water
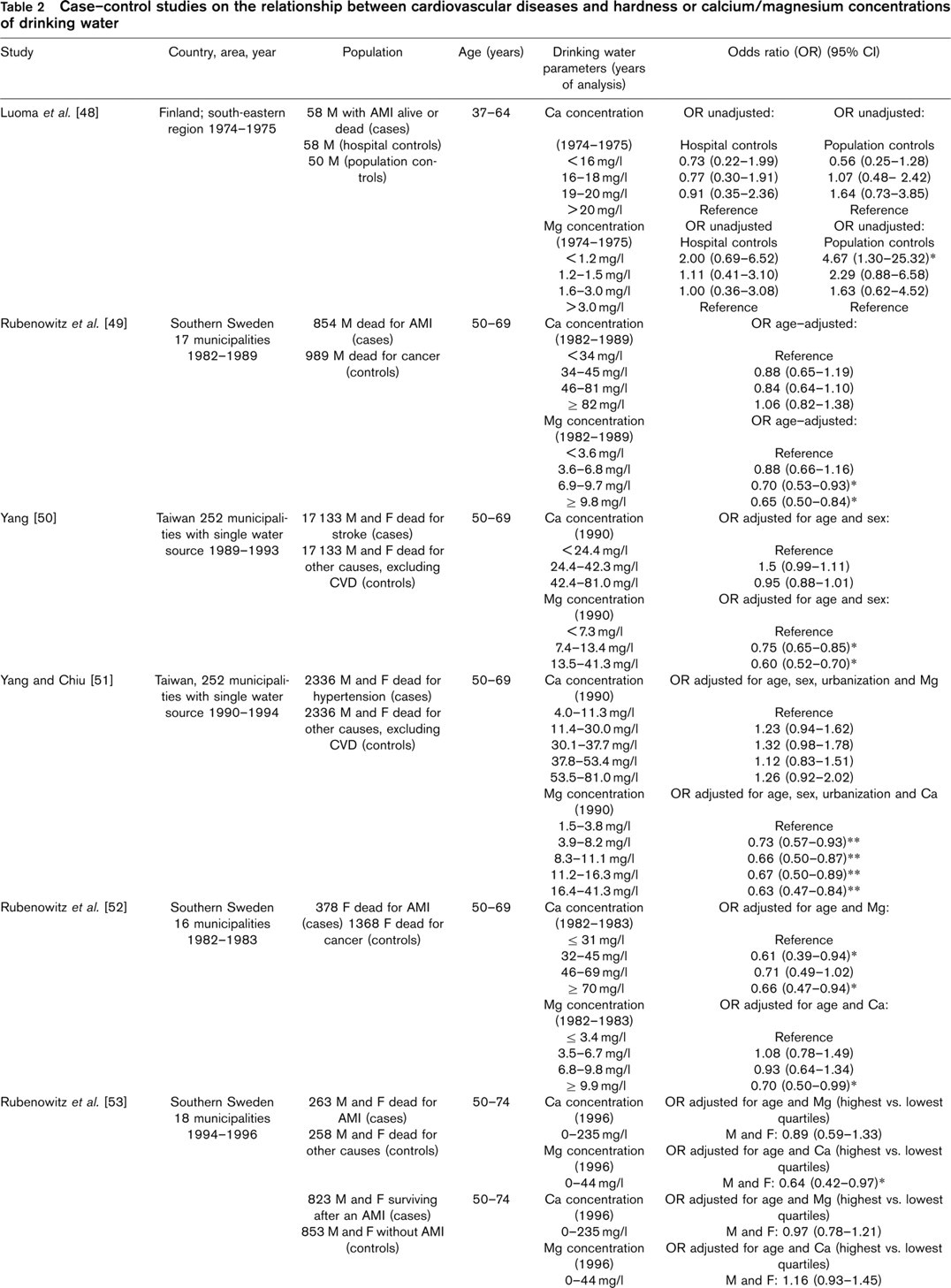
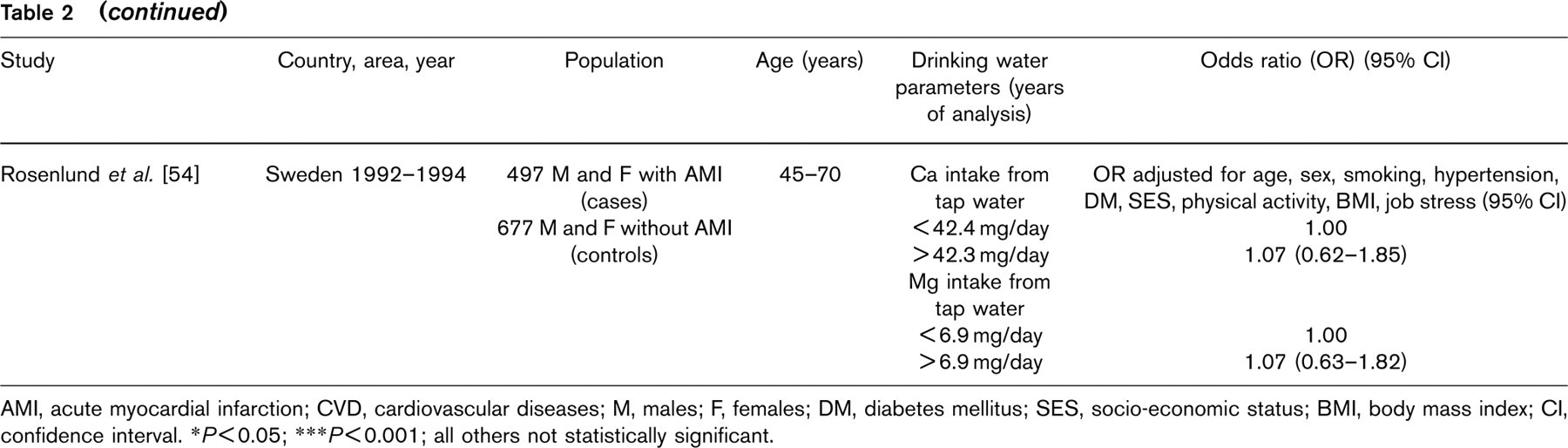
AMI, acute myocardial infarction; CVD, cardiovascular diseases; M, males; F, females; DM, diabetes mellitus; SES, socio-economic status; BMI, body mass index; CI, confidence interval. ∗P<0.05; ∗∗∗P<0.001; all others not statistically significant.
In Taiwan [50, 51], a statistically significant decreased risk of stroke and hypertension mortality among men and women was associated with increased drinking water magnesium. For stroke, a decreased risk (OR range 0.75–0.60) was associated with drinking water magnesium levels over 7.4 mg/l. An exposure-response relationship was found for drinking water magnesium levels and hypertension mortality risks (P <0.001); a decreased risk (OR range 0.73–0.63) was associated with magnesium levels over 3.8 mg/l. Exposure assessment in both studies was ecological. Using the most recent water quality analyses for municipal water systems, calcium and magnesium exposures were estimated for each person based on their residence. Historically, calcium, and magnesium levels were reasonably stable over time and season for these water systems.
Rubenowitz et al. [49, 52, 53] studied AMI mortality and morbidity in southern Sweden. A significantly decreased risk of AMI mortality among both men and women was associated with increased drinking water magnesium [49]. Water calcium was not associated with fatal AMI in men, but a significant reduced mortality in women was associated with increased drinking water calcium levels [49, 52]. An exposure-response relationship was observed between magnesium, but not calcium, levels in drinking water and risk of death [49, 52]. For men, a decreased risk (OR range 0.70–0.65) was associated with magnesium levels above 6.8 mg/l; for women, a decreased risk (OR = 0.70) was associated with magnesium levels above 9.8 mg/l [52]. Exposure measures were based on water quality data obtained from the appropriate municipal water systems for calcium and magnesium, and study participants were grouped into exposure quartiles based on the median levels during the studied time period.
Rubenowitz et al. [53] conducted a separate study of persons dying from AMI and AMI survivors. Information was collected about major CVD risk factors, and household water levels of calcium and magnesium were measured. A statistically significant, reduced risk of death for AMI (OR = 0.64) was found for the highest (> 8.3 mg/l) with respect to the lowest (<3.6 mg/l) quartile of drinking water magnesium concentration. No association was found between calcium levels in drinking water and death for AMI. For surviving cases, however, neither magnesium nor calcium levels in drinking water were associated with AMI after adjusting for the major risk factors for CVD. Investigators concluded that magnesium prevents AMI deaths rather than incidence.
Rosenlund et al. [54] studied the association between AMI risk and the average daily intake of drinking water constituents in a subset of individuals from a large Swedish population-based case-control study. After adjusting for major risk factors, no association was found. The authors noted some limitations to their study particularly the relatively low levels of calcium and magnesium in drinking water; two-thirds of study participants received a drinking water with mean values of 4.4 and 24.5 mg/l of magnesium and calcium, respectively.
Epidemiological studies published after 1978: cohort studies
Neither of the two cohort studies [55, 56] considered major CVD risk factors (Table 3). Punsar and Karvonen [55] conducted a 15-year follow-up of 1711 resident men in two rural areas of Finland; all used private well water. Mortality due to CHD was almost twice (14.7 versus 8.7%) as high in the area with lower drinking water magnesium. Among 1126 men who submitted a household water sample for analysis, those who died of CHD had significantly lower mean levels of drinking water magnesium than those alive at the end of the study.
Cohort studies of the relationship between cardiovascular diseases and drinking water hardness or magnesium levels
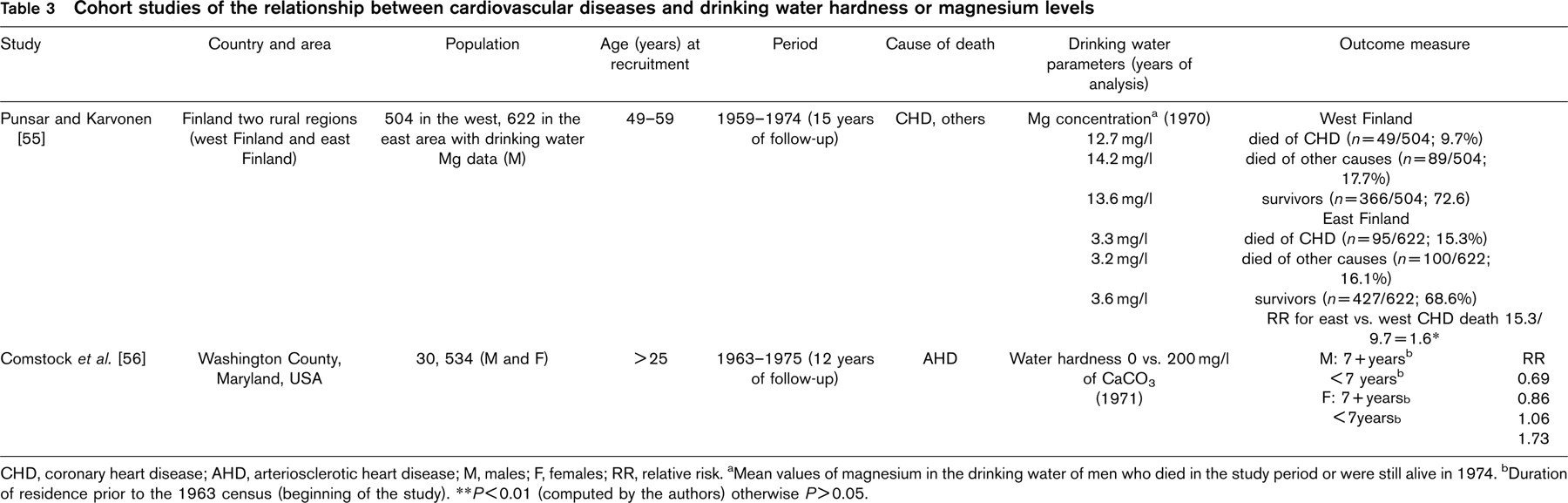
CHD, coronary heart disease; AHD, arteriosclerotic heart disease; M, males; F, females; RR, relative risk. aMean values of magnesium in the drinking water of men who died in the study period or were still alive in 1974. bDuration of residence prior to the 1963 census (beginning of the study). ∗∗P <0.01 (computed by the authors) otherwise P>0.05.
In Washington County, Maryland, Comstock et al. [56] found no consistent association between water hardness and CVD mortality. Water samples from 1569 households were analyzed for total hardness. An analysis that accounted for socio-economic characteristics and cigarette smokers showed no significant trend of CVD mortality with water hardness [21]. A reduced risk of mortality for AHD was found in men but not women.
Discussion
Because calcium is the primary constituent that contributes to water hardness, investigators who only measured hardness have tended to attribute associations to calcium. The ratio of magnesium to calcium in hard water, however, often differs depending upon geography, and the inconsistent results from the early studies that considered only hardness may be due to the different levels of magnesium in drinking water. Furthermore, calcium and magnesium act differently in human cells and may play different roles in CVD development and evolution. Thus, calcium and magnesium require separate evaluations when attempting to interpret these associations.
Total water hardness and cardiovascular disease
Eight of the 18 recent ecological studies reported that CVD mortality significantly decreased with increased drinking water hardness. In the three studies that estimated the risk, CVD mortality risk was decreased by 6–10% in areas with higher hardness depending on the specific outcome. In the two ecological studies that considered major CVD risk factors [40, 45], no significant association was found between drinking water hardness and CVD mortality or non fatal IHD.
Calcium concentrations and cardiovascular disease
Of the seven case-control studies that considered drinking water calcium, only one [52] found a protective association; there was no evidence for an exposure-response relationship. Recent cohort studies of dietary calcium intake and CVD have reported contrasting results. For instance, one study [57] found no protective effect of dietary calcium intake on the risk of developing either fatal or non-fatal IHD among men, whereas another one [58] found a protective effect for IHD mortality among postmenopausal women.
In evaluating possible biological plausibility for a calcium association, there is evidence [59] that calcium may play a role in the development and control of primary ‘essential’ hypertension in humans. Although current evidence supports recommendations of an adequate dietary intake of calcium to prevent or treat hypertension, a recent meta-analysis of 42 randomized controlled trials found only a small, clinically modest, reduction in both systolic (mean reduction of 1.44 mmHg) and diastolic (mean reduction of 0.84 mmHg) blood pressure by dietary and non-dietary calcium supplementation [60, 61]. Alternatively, the drinking water calcium association may be indirect. Soft waters dissolve lead and other contaminants from water pipes, storage tanks, and plumbing materials. The presence of lead, even at low blood levels, has been associated with hypertension and also with stroke [11, 12]. Water with high calcium levels has an anticorrosive effect that can prevent leaching of toxic metals from pipes and tanks [62].
Magnesium concentrations and cardiovascular disease
Epidemiological studies provide some evidence that drinking water that is high in magnesium protects against CVD and stroke mortality. Ecological studies reported contrasting results. Five of seven case-control studies, however, found a statistically significant protective association between magnesium in drinking water and mortality risks for AMI, stoke, or hypertension. Two of these analytic studies measured drinking water magnesium at the individual level and took into account major risk factors for CVD [53, 54]. One of them [53] found a significant protective effect of drinking water magnesium level on CVD mortality, with evidence for a linear exposure-response trend, whereas the other one [54] found no association between magnesium concentration and AMI.
Magnesium exerts many different biological functions [63], including structural roles by complexing negatively charged groups (i.e. phosphates in nucleic acids, catalytic roles in enzyme activation or inhibition), regulatory roles by modulating cell proliferation, and cell cycle progression and differentiation. Magnesium is needed to maintain the normal gradient of potassium and calcium over the cell membranes [53]. Magnesium deficiency accelerates the development of atherosclerosis and the induction of thrombocyte aggregation and has been described as a risk factor for AMI and cerebrovascular disease [64, 65]. Magnesium is also known to protect against soft tissue calcification, particularly for myocytes, and its role in AMI has been documented [8, 66].
Studies in experimental animals provide support for a causal association between magnesium intake and IHD. Experimentally-induced magnesium deficiency changes the blood lipid composition in a more atherogenic direction [67, 68]. Magnesium-fortified water reduced atherogenesis in low-density lipoprotein (LDL) receptor-deficient mice compared with those receiving distilled water, with and without a high-cholesterol diet [69–71]. Magnesium supplementation in drinking water also significantly inhibited atherogenesis in female but not male apolipoprotein-E-deficient mice not receiving a high-fat diet [72].
Findings by Rubenowitz et al. [53] suggest that magnesium may reduce the fatalities among those who develop CVD (secondary prevention) rather than prevent the onset of disease (primary prevention). In addition, a cohort study found that increased serum magnesium levels were associated with decreased CHD mortality but not with incidence, and clinical studies found that magnesium is useful in treating patients with AMI and other acute CVD [73, 74]. Furthermore, oral magnesium therapy in CHD patients has been shown to have beneficial effects [75, 76].
A diet rich in vegetables, fruit and whole grains not only provides more magnesium than the common diet in industrialized countries but also significantly reduces blood pressure and CVD incidence [77–80]. Many observational studies have reported a protective role of magnesium in reducing the incidence of hypertension [81]. A recent prospective study [82] found a lower risk of hypertension in subjects with high magnesium serum levels among people free of the diseases at baseline. Magnesium may also be involved in CVD development by other ways [83]. For instance, a recent in-vitro experimental study demonstrated a direct role of low magnesium in promoting endothelial dysfunction by generating a pro-inflammatory, pro-thrombotic and pro-atherogenic environment [84].
Recent dietary cohort studies reported a protective effect of magnesium intake on CVD risk, both fatal and non-fatal [85, 86]. Cross-sectional, case-control, and cohort studies found that, subjects with low magnesium serum levels have an increased risk of CHD compared with people with high levels when all major risk factors were considered [73, 87–90]. A recent study [91] of postmenopausal women maintained in a metabolic unit for 81 days found that an adequate, ordinary diet low in magnesium (160 mg/day) disrupted magnesium homeostasis and increased myocardial irritability. A recent study of participants in a nationally representative survey found that those who consumed less than the current recommended daily allowance (RDA) of magnesium were more likely to have elevated C-reactive protein (CRP), a marker of vascular inflammation that is associated with increased risk of CVD [92]. Adults who consumed under 50% the RDA were almost twice as likely to have an elevated CRP than those who consumed at the RDA (OR = 1.75; 95% CI 1.08–2.87).
Drinking water magnesium can be important in areas where magnesium intake is low. The daily intake of magnesium in industrialized countries does not reach the RDA in many people, and marginal magnesium deficiencies are common. A national survey among US adults found that 68% consume less than the RDA [92] and about 23% have magnesium serum concentrations under 0.80 mmol/l (19.44 mg/l), levels considered as hypomagnesemia [73]. Two liters of water rich in magnesium (40 mg/l) would provide about 25% of an adult's total requirement, and magnesium may be more bioavailable in drinking water than food [40].
Interpreting the epidemiological evidence
Epidemiologists evaluate the causality of observed associations by considering Hill's criteria [93]. Current studies satisfy temporality concerns and provide reasonable evidence of biological plausibility, consistency, and specificity especially for drinking water magnesium. There is also limited evidence of a magnesium exposure-response relationship. The strength of the association is, however, relatively weak. Recent studies suggest that less than15% of CVD mortality may be attributed to drinking water hardness and that at least 80% of major CHD events in middle-aged men can be attributed to the most common risk factors: serum total cholesterol, cigarette smoking, diabetes, blood pressure, obesity and sedentary lifestyle [1–3, 94]. Morris et al. [95] reported that a large part of the geographical variation observed in CHD incidence in British towns was reduced after adjustment for the main risk factors. It follows that the contribution of any drinking water constituent to CHD incidence or mortality is modest. The benefit can be considerable, however, because of large populations affected.
All the studies conducted before 1979 and most conducted afterwards were ecological. Since health, exposure, and demographic statistics in ecological studies characterize population groups, some observed relationships in these studies may be merely coincidental [21]. Studies conducted by Nerbrand et al. [40, 45] provide an example of the ecological fallacy; no association was found between drinking water calcium or magnesium and CVD mortality at the individual level in spite of an apparent geographical correlation. Ecological studies can, however, provide valuable information about population-based risks and often provide the stimulus for more expensive case-control and cohort studies in which information is collected for individual exposures and disease risks.
In terms of study design, an important concern is exposure misclassification. Imprecision in assessing exposure usually causes non-differential misclassification, reducing the chance of detecting an association should it really exist or underestimating the magnitude of an effect. Various factors may contribute to mistakes in exposure measurement. First, retrospective studies usually relied on relatively current water hardness measures, and prospective studies usually had only one measure, at the beginning of the study. Unless water sources or treatment are changed, however, drinking water hardness is generally stable over time. Second, almost all of these studies classified exposure by the finished water quality at the treatment plant. Except for several analytical studies, little regard was given to tap water quality. Not considering the use of home softeners may be important in hard water areas, and this may be a reason for inconsistent results. For example, the market saturation for softeners in the US was 60–70% in 1970 [18, 19]. Third, not considering water consumption may also be important, as Gillies and Paulin [96] point out there can be a large variation (tenfold or greater) in the amount of water people drink daily. In addition, mineral levels in 24-h samples can vary markedly from those in water collected from the water system or household tap. Bottled water consumption may also cause misclassification, especially in areas where mineral waters have been available for many years. Some mineral-rich waters provide an important contribution to the total calcium and magnesium intake. Depending upon the brand, mineral water may contribute 25% of the total daily calcium intake and 6–17% of the magnesium intake [97]. It should also be recognized that soft water, when used for cooking, can cause substantial losses of these minerals [98].
Few drinking water CVD studies collected information about possible confounders. Major CVD risk factors may confound the relationship if they are also associated with drinking water hardness, calcium, or magnesium levels. There is, however, no a priori reason for such an association. In one study [45], several CVD risk factors were found to be associated with water hardness and calcium levels, but in another study [53] there was no change in the estimated risks of death for AMI when the major confounders were controlled for. It seems unlikely that confounding alone can completely explain the many associations found among different populations and at different times.
An important limitation of several studies is that they compared populations or individuals with little differences in drinking water hardness, calcium, and magnesium levels. This may help explain the inconsistent results, especially among the case-control studies. For example, the lack of an association observed by Rosenlund et al. [54] may be due to a low intake of drinking water magnesium; drinking water magnesium intake was under 3.5 mg per day for 70% of the participants. In comparison, Rubenowitz et al. [49, 52, 53] found a protective effect only when the daily intake of drinking water magnesium was over 13.8 mg (based on a daily consumption of two litres).
Conclusion
There is little evidence that supports an association between drinking water hardness, as such, and CVD mortality. There is limited evidence of an association between increased calcium levels in drinking water and a decreased risk of CVD mortality. The available information does, however, support the hypothesis that a low intake of magnesium from drinking water increases the risk of dying from, and possibly developing, CVD or stroke. Others have reached similar conclusions about the benefits of magnesium in drinking water [4, 64, 65, 99]. A recent intervention study showed that daily consumption of at least 1l of natural mineral water with a magnesium concentration of 84 mg/l reduced blood pressure significantly at 4 weeks [100].
Additional evidence supporting this conclusion about drinking water magnesium includes the following: Invitro studies show that low magnesium level in the media determines endothelial cell dysfunction, the initiating event leading to the formation of the atherosclerotic plaque. Animal studies show that a low-magnesium diet causes inflammation and high serum cholesterol levels, particularly LDL, favouring the development of atherosclerosis. High magnesium intake protects against the atherosclerotic effects of oxidative stress and hypercho-lesterolemia-inducing diets. In patients with CHD, magnesium in pharmacological doses can reduce endothelial lesions and is a useful anti-ischemic and anti-arrhythmic agent. Cohort studies show that people with low serum magnesium levels are at a higher risk of hypertension, CHD, and stroke. Dietary studies show that a diet rich in magnesium reduces the risk of CVD.
Results from the numerous epidemiological studies of drinking water hardness and CVD do not completely satisfy all of the suggested criteria for a causal association, and some scientists may argue that additional information is needed to establish causality. It should, however, be recognized that effective public health actions may be taken even with incomplete knowledge or certainty about causality. Increased magnesium intake from water used for drinking and cooking may be beneficial especially in populations with an insufficient dietary intake and would be a relatively easy way in which sufficiency can be maintained for the entire population. With the increased use of softening and other home water treatment devices, it is important that the public be aware that they may be reducing or removing minerals such as calcium and magnesium from drinking water. With that in mind, softening and demineralization units can be installed to provide untreated water for drinking and cooking while softened or treated water is delivered to the rest of the home. Research should be conducted to determine the feasibility of returning magnesium to demineralized or softened water, and health officials should consider epidemiological studies to assess changes in cardiovascular risks when municipalities soften public water supplies.