
Abstract
Background
Plasma lipids are associated with cardiovascular diseases. Population-based data on plasma lipids are scarce in Bangladesh.
Methods
We investigated plasma lipid levels in a rural population of Bangladesh in 2001. Fasting blood was collected in 447 adults (157 men and 290 women) aged 20–79 years (mean ± standard deviation 40 ± 11 years in men, and 39 ± 10 in women).
Results
The mean total cholesterol, high-density lipoprotein (HDL) cholesterol, low-density lipoprotein (LDL) cholesterol, triglycerides and total cholesterol/HDL cholesterol ratio levels were 182 ± 56, 39 ± 10, 115 ± 53, 139 ± 72 mg/dl and 4.8 ± 1.8, respectively. The prevalence of abnormal lipid levels were as follows: hypercholesterolemia (total cholesterol >240 mg/dl) 16.1%, high LDL cholesterol (>160 mg/dl) 20.4%, low HDL cholesterol (>40mg/dl) 66.4%, hypertriglyceridemia (>200mg/dl) 15.0% and total cholesterol/HDL cholesterol ratio (>5.5) 32.7%.
Conclusions
The prevalence of dyslipidemias, especially in the case of low HDL cholesterol, appears to be high even in this rural population of Bangladesh. Eur J Cardiovasc Prev Rehabil 13:444–448 © 2006 The European Society of Cardiology
Introduction
The World Health Report 2002 indicates that cholesterol is the 10th leading risk factor in high mortality developing countries, sixth in low mortality developing countries and fourth in developed countries [1]. Although plasma lipids are essential for physiological functions of the body, abnormal levels lead to morbidity and mortality from some major killer diseases such as ischemic heart diseases, stroke, and some cancers [2]. Cholesterol abnormalities include high levels of total cholesterol (TC), low-density lipoprotein (LDL) cholesterol and triglycerides, and low levels of high-density lipoprotein (HDL) cholesterol. There are ways to control levels of lipids both at individual and population levels, popularly known as high-risk and population approaches [3]. Periodic surveys are necessary to know the plasma levels of lipids in the population for preventing and controlling premature occurrences of deaths due to these diseases.
Data on plasma lipids are almost lacking in the Bangladeshi population. In one study conducted in 1996, we reported obesity, smoking and blood pressure along with blood cholesterol and glucose in a relatively comprehensive way for a sample population located near the capital city of Dhaka [4]. Its sample size for biochemical variables, however, was small. In other studies we described non-biochemical risk factors for cardiovascular diseases in a clinic-based [5] and general population [6] of Bangladesh. The current distribution of plasma lipids in the rural population of Bangladesh is not known. Clinical experience indicates that our people may have greater problems of low HDL cholesterol and high triglycerides rather than high TC [7]. Studies in Bangladeshi emigrants to the UK also indicate similar features [8]. We need to know the distribution of plasma lipids in the rural population because about 80% of the people of Bangladesh live in rural areas. The aim of this study was to determine the distribution of plasma lipids in a rural population of Bangladesh.
Methods
Study area and its people
This study was done in 2001 in Ekhlaspur village of the Matlab North upazila (sub-district) of the Chandpur district. It is located about 60 km south-east of Dhaka city. It is an agricultural area located on the bank of the river Meghna. Some of the families supplement their main agricultural income by small business and employment of male members residing in towns. Electricity has just been introduced in this village. River transportation is the only convenient means of travel to and from urban areas. It takes about 2–3 h by motor launch to reach nearby small towns. Extended joint families are still popular here. Most people endure hard physical work but most of them eat rice three times a day. Fish and vegetables are eaten at least once a day. Although this Muslim society contains the vestiges of Buddhist and Hindu cultural roots, alcohol is prohibited and unacceptable to the society and family. Women do not smoke (due to cultural reasons) but many chew tobacco leaf with betel quid (pan). All these are features of a traditional rural Bangladesh [5].
Participants
All people of Ekhlaspur village were enumerated (5476) by program assistants of Ekhlaspur Center of Health (ECOH) in 1999. Among them, 2854 participants were aged between 20 and 79 years (1504 men and 1350 women). This study was a part of a general health checkup of the residents of Ekhlaspur done by ECOH. We identified 700 of them (equal number of men and women) using simple random sampling. We intended to have at least 50 people in each decade of age. Thus in six such decades for two sexes the expected number was 600. Anticipating a low response rate, however, we targeted another 100 subjects. Of the 700 people targeted, 447 (64%) responded [157 men (45%) and 290 women (83%)].
An awareness meeting for people in general from Ekhlaspur was held at which most of the opinion leaders were present. The importance of a health check-up and assessment of cardiovascular risk factors was explained. Village people agreed that they will have at least one such examination every 5 years depending on availability of resources. Subsequently, at the time of individual examination, verbal informed consent was obtained from every participant.
Data collection
Assessment of cardiovascular disease risk factors by a trained health assistant comprised administration of a questionnaire on age, sex, education, meat and fish consumption, smoking including chewing tobacco, current drug treatment for chronic diseases, and measurements of weight and height (without heavy clothing and shoes) and blood pressure.
Measurement of lipids
All potential participants were requested not to eat anything after 2000 h and to attend the clinic at ECOH between 0800 and 1000 h on the following day. Fasting status was ensured by interview. Venous blood samples (5 ml) were drawn into ethylenediaminetetra-acetic acid containing vacuum tubes with minimum stasis. Aliquots of plasma were immediately frozen and transported to Dhaka in an icebox. All measurements were done in the laboratory of the National Center for Control of Rheumatic Fever and Heart Diseases (Dhaka) with appropriate internal quality control procedures. Plasma TC was measured by an autoanalyser by enzymatic method. Plasma triglycerides were measured after enzymatic hydrolysis with lipases. HDL cholesterol was measured from supernatant after quantitative precipitation of LDL cholesterol and chylomicron fractions by the addition of phosphotungstic acid in the presence of magnesium ions. LDL cholesterol was calculated by the Friedewald equation, given that none had triglycerides level above 400 mg/dl [9].
Statistical analyses
Participants were categorized into two age groups, dividing at 50 years because most of heart attacks occur after this age. Descriptive statistics of selected variables for all participants and age and sex-specific descriptive statistics of plasma lipids were obtained. Categorization of the plasma lipid levels was done according to the third report of the US National Cholesterol Education Program (Adult Treatment Panel III) [10]. Prevalence of dyslipidemia with 95% confidence intervals in each group was calculated. All analyses were done using the SAS statistical package (SAS Institute Inc, Cary, North Carolina, USA).
Results
Out of 700 selected subjects 447 participated in the study. Table 1 shows the sociodemographic background of the target population of Ekhlaspur and the survey participants. Non-participants were similar to the participants in terms of age and education status. The participants were mainly fish eaters with a median intake of fish four times in the last 3 days. Although the meat, milk and egg intake was very low, tobacco consumption was very high for both smoking (19%) and smokeless forms (36%). None were alcohol consumers. The mean body mass index was 19 indicating that many participants were lean.
Overall and age and sex-specific distributions of TC, HDL cholesterol, LDL cholesterol and triglycerides are shown in Table 2. Average plasma lipid levels were approximately similar in men and women. Plasma lipid levels were higher in the older age groups (≥50 years). The ratio of TC to HDL cholesterol was also related to age.
Men and women had approximately similar prevalence of dyslipidemias (Table 3). Prevalence of hypercholesterolemia (>240 mg/dl), high LDL cholesterol (>160 mg/dl), low HDL cholesterol (>40mg/dl) and high triglycerides (>200 mg/dl) were 16.1, 20.4, 66.4, 15.0%, respectively. These prevalences were directly related to age (Fig. 1).
Discussion
This is the first population-based study to describe a range of lipid variables in a rural population of Bangladesh. In this predominantly agricultural rural population with traditional lifestyle and dietary habit, the mean total cholesterol was 182 mg/dl while the prevalence of hypercholesterolemia was 16.1%. The mean cholesterol level for this population was higher than our previous report [4] (159 mg/dl) done in another rural population in 1996. In that study, however, younger participants were included, the sample size was small and cholesterol was measured on capillary blood. The plasma total cholesterol level in our participants was lower than that in Bangladeshi emigrants to the UK (214 and 208 mg/dl in men and women) [11], and other Asian (e.g. the Japanese, 180 and 201 mg/dl in men and women) [12] and Western (e.g. British 224 mg/dl) [13] populations. In a rural adult population of India, the mean cholesterol level was about 170 mg/dl, which is similar to our findings [14]. In that study the prevalence of hypercholesterolemia, defined as TC of 200 mg/dl or higher, was 22%, which is also similar to our findings. There were, however, methodological differences among those studies and comparison of the results may not be valid and should be interpreted cautiously. It is difficult to compare the prevalence of hypercholesterolemia with other reports as studies use different cut off values to define hypercholesterolemia.
Sociodemographic background of target population (ages 20–79 years) of Ekhlaspur and the survey participants
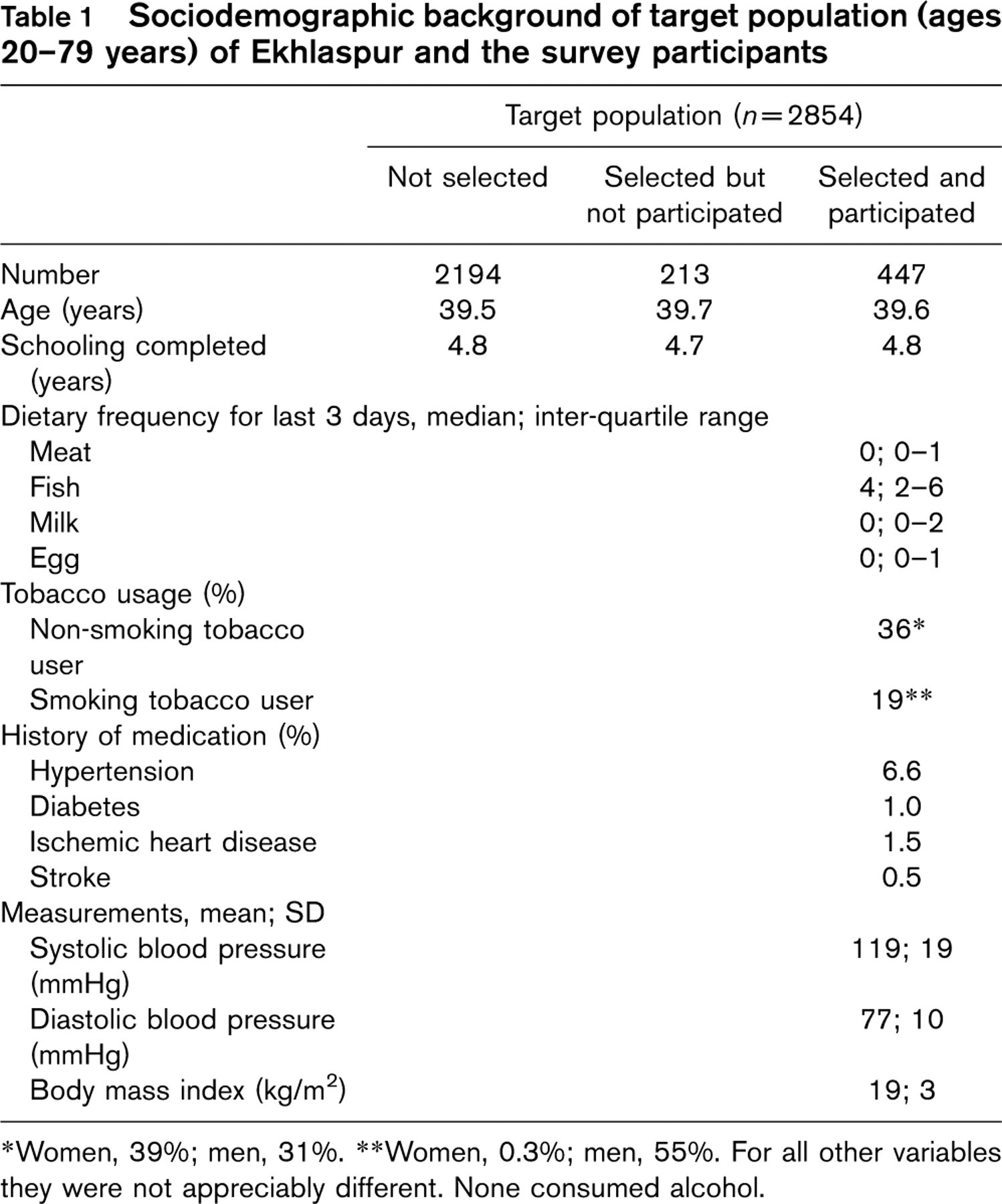
∗Women, 39%; men, 31%. ∗∗Women, 0.3%; men, 55%. For all other variables they were not appreciably different. None consumed alcohol.
Mean and standard deviation of plasma lipids
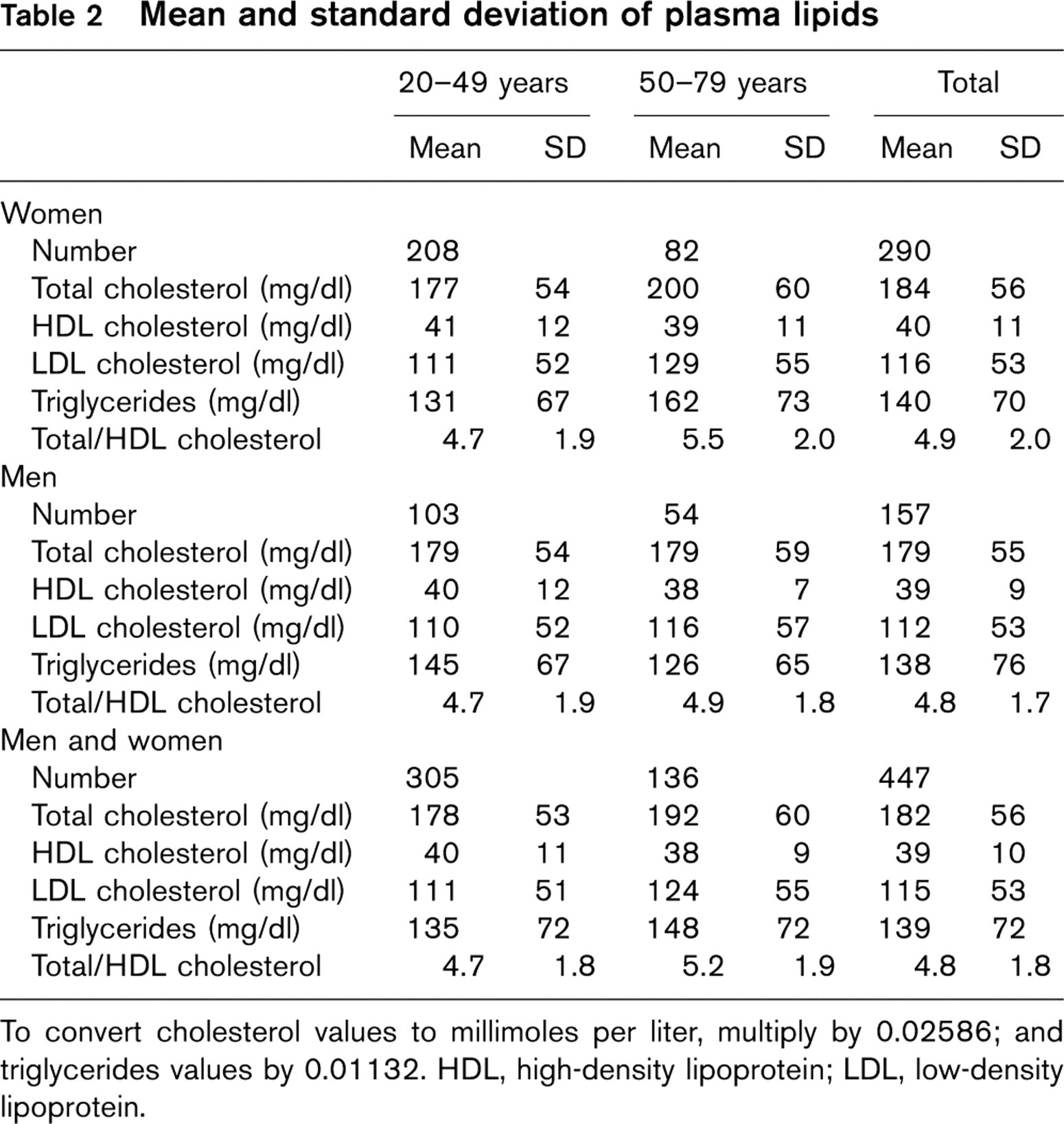
To convert cholesterol values to millimoles per liter, multiply by 0.02586; and triglycerides values by 0.01132. HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Prevalence and 95% confidence intervals of dyslipidemias

HDL, high-density lipoprotein; LDL, low-density lipoprotein.
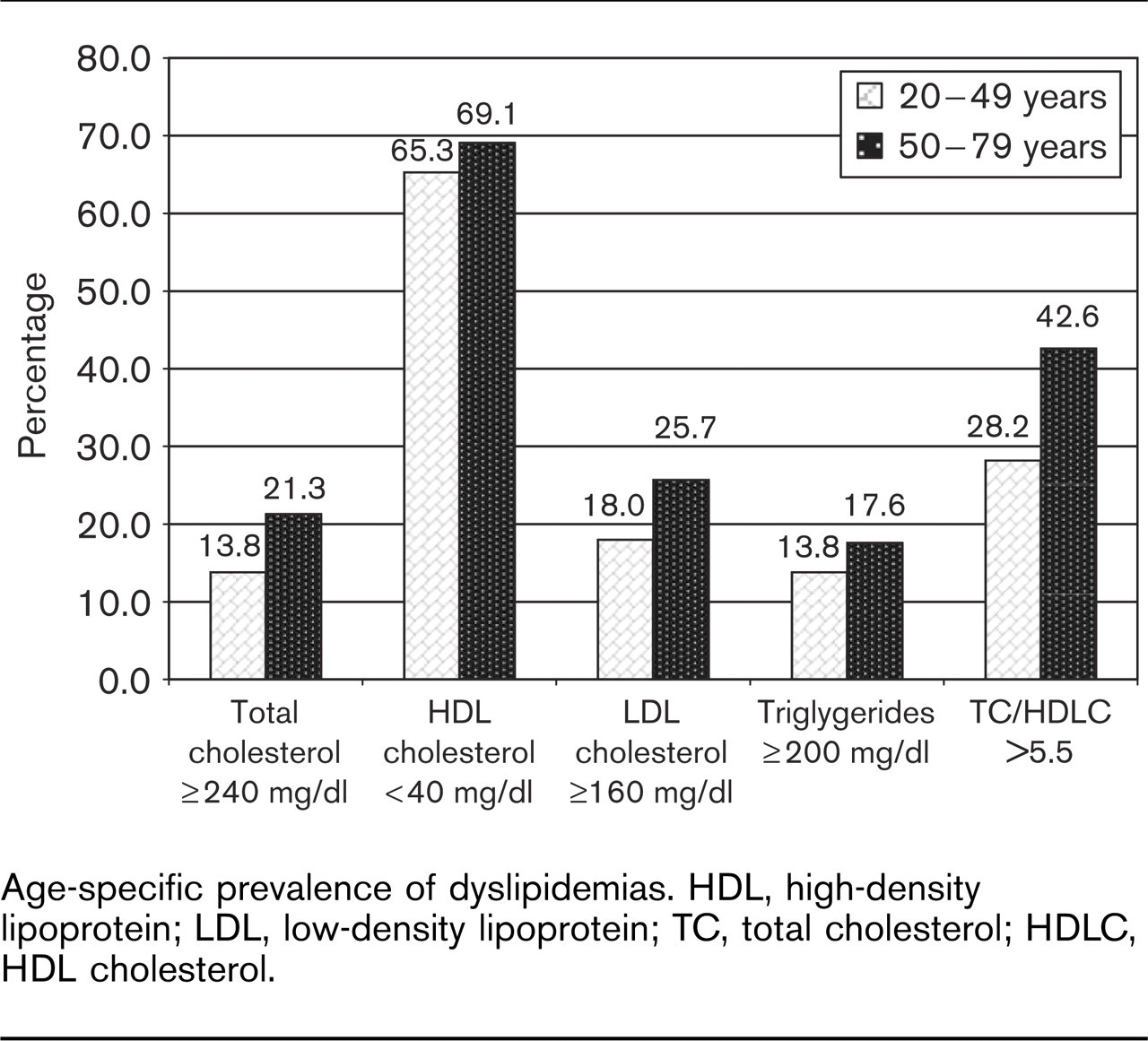
Age-specific prevalence of dyslipidemias. HDL, high-density lipoprotein; LDL, low-density lipoprotein; TC, total cholesterol; HDLC, HDL cholesterol.
A recent study conducted in Dhaka city showed that mean lipid levels are relatively high. The values for TC, HDL cholesterol, LDL cholesterol and triglycerides were 207, 36, 132 and 199 mg/dl, respectively (unpublished data). All these values are higher than those we are reporting here. Therefore our findings are not surprising. The differences can be explained in terms of rapid lifestyle changes in the urban capital, Dhaka. The difference for triglycerides is more remarkable. This may mean that urbanization has greater impact on triglyceride levels. This is being observed in our tertiary level hospitals.
The most prevalent dyslipidemia in our sample is low HDL cholesterol, which is 66.4%. Previous studies have used different cutoff values to define low HDL cholesterol. One study in India reported prevalence of low HDL cholesterol as 30% [14] while another study reported only 7% in a rural population [15]. Recent Adult Treatment Panel III guidelines have defined low HDL cholesterol as under 40 mg/dl. Since in our sample mean HDL cholesterol was lower than that of Western and Japanese populations [13, 16], this new cutoff point categorized about two-thirds of the population as having low HDL cholesterol. The implication of this new cutoff point in this population in terms of treatment and prediction of cardiovascular disease needs to be addressed in the future. We believe that abstinence from alcohol and a high consumption of tobacco is responsible for the unfavorable HDL level in our sample.
About 20% of our subjects had LDL cholesterol of more than 160 mg/dl. Using 124 mg/dl as a cutoff value, one study in India reported about 22% of the subjects as having high LDL cholesterol. Compared with that study our sample has a relatively high prevalence of high LDL cholesterol. A few studies have reported the prevalence of hypertriglyceridemia in a South Asian population and it is thought to be an important risk factor for coronary heart disease in this population [8]. The prevalence of hypertriglyceridemia was 15% in our sample, which is higher than the prevalence in a rural Indian population (9.8%) [15]. There was, however, a difference in the cutoff level and therefore a direct comparison may not be appropriate. It is relevant to note here that emigrant studies on South Asians observed that Bangladeshi people are in a most disadvantageous position in terms of major cardiovascular risk factors [17]. This might also be the case in their native countries. Therefore, Bangladesh needs to pay due importance to control these risk factors because they lead to many killer diseases.
Limitations
This study was done only in one village using a small sample. The main problem of the study was a low response rate in men. The overall response rate (64%) was fairly acceptable to give a fair estimate of the lipids in the community. A lower response rate in men (45%) was due to the fact that they went to the field to work in the morning after breakfast. Participation in this study in fasting status could hamper their day's work (and earning) given that we could not compensate for the work loss. Therefore data presented here for men may be of marginal value. People with lower levels of risk factors are less likely to come forward for a blood test. The similarity of background between responders and non-responders is against this argument (Table 1). Although we have tried to maintain internal quality control for the laboratory for lipid measurement, our laboratory did not have an external quality control mechanism.
Conclusion
Although the strength of this study has been limited by a small sample size, our findings are important because such data have never been made available for our rural population. The prevalence of dyslipidemias, especially in the case of low HDL, appears to be high even in this rural population of Bangladesh. Further well-designed studies involving large numbers of representative subjects are needed to identify determinants of dyslipidemias (especially low HDL) in this population.
Acknowledgements
We convey our thanks to Dr's Mamun-or-Rashid, Turin Chowdhury and Sumon Islam for assistance in data collection. Our enumerators, Nargis Aktar and Nazrul Islam, deserve special thanks for their sincere contribution. We are indebted to the participants; without their help we could have achieved nothing.