
Abstract
Background
The role of exercise in preventing cardiovascular disease (CVD) has been well documented. To determine whether this benefit could be related to effects on vascular endothelial function and vessel wall elasticity, thereby preserving arterial compliance, we examined the relationship between habitual exercise and arterial compliance as measured by pulse wave analysis.
Design
A cross-sectional study of healthy volunteers and patients with type 1 diabetes.
Methods
Non-diabetic individuals not taking cholesterol or blood pressure-lowering medication (n = 176) and patients with type 1 diabetes (n = 105), aged 17–70 years, were recruited. Small and large artery compliance and other haemodynamic variables were measured using the PulseWave CR-2000 cardiovascular profiling system. A questionnaire was completed to assess the frequency of physical activity.
Results
In multivariate analysis, undertaking three or more episodes of vigorous activity per week was associated with having a 1 unit greater small artery compliance, independent of age, sex, height, diabetes status and blood pressure. The effect was especially marked in non-diabetic women.
Conclusions
The results support other findings that regular physical activity protects against CVD, through the preservation of vascular compliance.
Introduction
The role of exercise in preventing cardiovascular disease (CVD) has been well documented [1–3]. Exercise training has been found to improve vascular function, partly by upregulating nitric oxide synthesis and release [4], and in patients with coronary heart disease, exercise has been shown to improve endothelium-dependent vasodilation in coronary and resistance vessels [5]. Increased physical activity may slow the atherosclerotic process by improving traditional CVD risk factors such as obesity, hypertension and dyslipidaemia. In cross-sectional studies, other risk factors for atherosclerosis such as inflammatory markers [6] and advanced glycation end-products [7] have also been shown to be inversely associated with physical activity. Current recommendations suggest 30 min of moderate intensity exercise on most or all days of the week, to provide protection from CVD and type 2 diabetes [8, 9].
In addition to the benefit gained from reducing traditional CVD risk factors, exercise in patients with diabetes favourably influences blood glucose concentrations and insulin action [10–12]. Acute exercise enhances GLUT4 uptake of glucose into muscle, lowering blood glucose, and has also been shown to improve insulin sensitivity [13]. At present there is insufficient evidence regarding the effectiveness of exercise for long-term risk reduction and cardiovascular morbidity and mortality in patients with type 1 diabetes.
Vascular endothelial dysfunction and the loss of blood vessel compliance precede overt atherosclerotic disease and provide early markers of CVD risk [14, 15]. Pulse-wave analysis (PWA) is a clinically applicable, US Food and Drug Administration approved, non-invasive measure of arterial compliance [16], with impaired small artery compliance associated with diabetes, hypertension [17], hypercholesterolaemia [18], renal disease [19] and inflammation in rheumatoid arthritis [20]. Arterial compliance of both large and small blood vessels also decreases with age [15], and there is evidence that physical activity modulates at least some measures of this effect [21]. The aim of this study was to evaluate the association between arterial compliance and other haemodynamic variables, as measured by PWA, and self-reported exercise in a healthy population and individuals with type 1 diabetes mellitus.
Methods
This study was approved by the St Vincent's Hospital Melbourne Ethics Committee and written informed consent was obtained. The study involved non-diabetic, healthy participants aged 18–70 years recruited in order to define reference ranges for arterial compliance and other novel CVD risk markers. Also included in the study were patients with type 1 diabetes aged 18–70 years. Participants recruited included hospital patients, hospital staff, and the wider community.
For the non-diabetic group, participants with a self-reported history of coronary heart disease, renal disease or stroke were excluded. Participants on cholesterol-lowering or antihypertensive medications were also excluded because of their known effects on vascular compliance. Fasting glucose, glycated haemoglobin, and microalbuminuria were measured to screen for undiagnosed diabetes and renal disease, and participants were excluded if biochemical evidence of diabetes or renal disease was detected. The population studied was therefore one free of apparent chronic disease. The final sample size for this analysis was 176 participants.
For the type 1 diabetes group, participants with documented diabetes were recruited from endocrinology clinics at St Vincent's Hospital, Melbourne. The medication use of the type 1 diabetic participants was recorded, and they were permitted to take their usual medications on the day of the study, and only those participants with documented coronary artery disease were excluded. Insulin injections were taken after PWA given the known acute vasodilatory effects of pharmacological doses of insulin. The final sample size of the type 1 diabetes group for this analysis was 105 participants.
Measurements
Blood pressure, heart rate, systemic vascular resistance and small and large artery compliance were measured by PWA using the HDI/PulseWave CR-2000 Research Cardiovascular Profiling System (Hypertension Diagnostics Inc., Eagan, Minnesota, USA). This technique analyses the diastolic decay curve of the radial artery pressure waveform, detected using a non-invasive direct contact acoustic transducer. A modified Windkessel model is used to estimate small and large artery compliance [16]. Participants were studied between 0800 and 1000 h, having fasted and not smoked since at least midnight the previous night. Height and weight were measured for calculation of body mass index (BMI). Participants rested in the supine position for at least 5 min, before having three PWA measurements taken, with the average of these measurements used for statistical analyses. Measurements obtained from this system included: supine systolic blood pressure (SBP) and diastolic blood pressure (DBP), pulse pressure (PP), resting pulse rate, large artery compliance (presented as ml/mmHg × 10), small artery compliance (ml/mmHg × 100) and systemic vascular resistance (SVR; dyne/s per cm5). Inter and intra-run coefficients of variation of the two PWA operators were less than 10%.
Physical activity
The frequency of ‘vigorous’ exercise was assessed by administration of the question ‘In the last week, did you do any exercise which made you breathe hard or puff and pant (such as basketball, football, swimming, other sport, heavy gardening or other heavy work) for at least 20 minutes at a time?'. Three response options to these questions were available: No; Yes – less than three times; or Yes – three or more times. This question was based on similar questionnaires used previously [22, 23]. However, as for the National Heart Foundation Risk Factor Prevalence Study [24], the wording of the intensity of the exercise was changed from exercise that induced sweating to that described above, as appropriate for warmer climates.
Statistical analysis
Analysis of variance (ANOVA) or the chi-squared test was used to test for variation in potential confounding variables across exercise categories. Variations in haemodynamic variables across categories of exercise were tested by ANOVA and tests for linear trend, with adjustment for sex. Linear regression was used to model compliance as a function of clinical and behavioural variables. A P value of less than 0.05 was considered to indicate statistical significance. All analyses were conducted using SPSS version 11.0 (SPSS Inc., Chicago, Illinois, USA).
Results
Non-diabetic and type 1 diabetic groups did not differ significantly with respect to age, sex or smoking prevalence (Table 1). Diabetic participants had higher mean BMI and were less likely to have completed post-secondary education than non-diabetic participants. Forty-three per cent of type 1 diabetic participants were taking antihypertensive or lipid-lowering medication. Despite this, diabetic participants had significantly higher SBP and DBP, PP and pulse rate, and significantly lower small and large artery compliance (Table 1).
Table 2 shows participant characteristics stratified by levels of vigorous activity and diabetes status. There was no significant variation across levels of vigorous activity with respect to age or BMI for either group (data not shown). For non-diabetic participants, smoking prevalence decreased in a linear manner with increasing exercise frequency (13, 10 and 2% across exercise categories; P = 0.04). Men were more likely to perform vigorous activity than were women. More active individuals tended to be taller (data not shown) but this was largely the result of sex differences between groups. Therefore ANOVA in haemodynamic variables across activity strata were adjusted for sex.
Clinical and haemodynamic characteristics
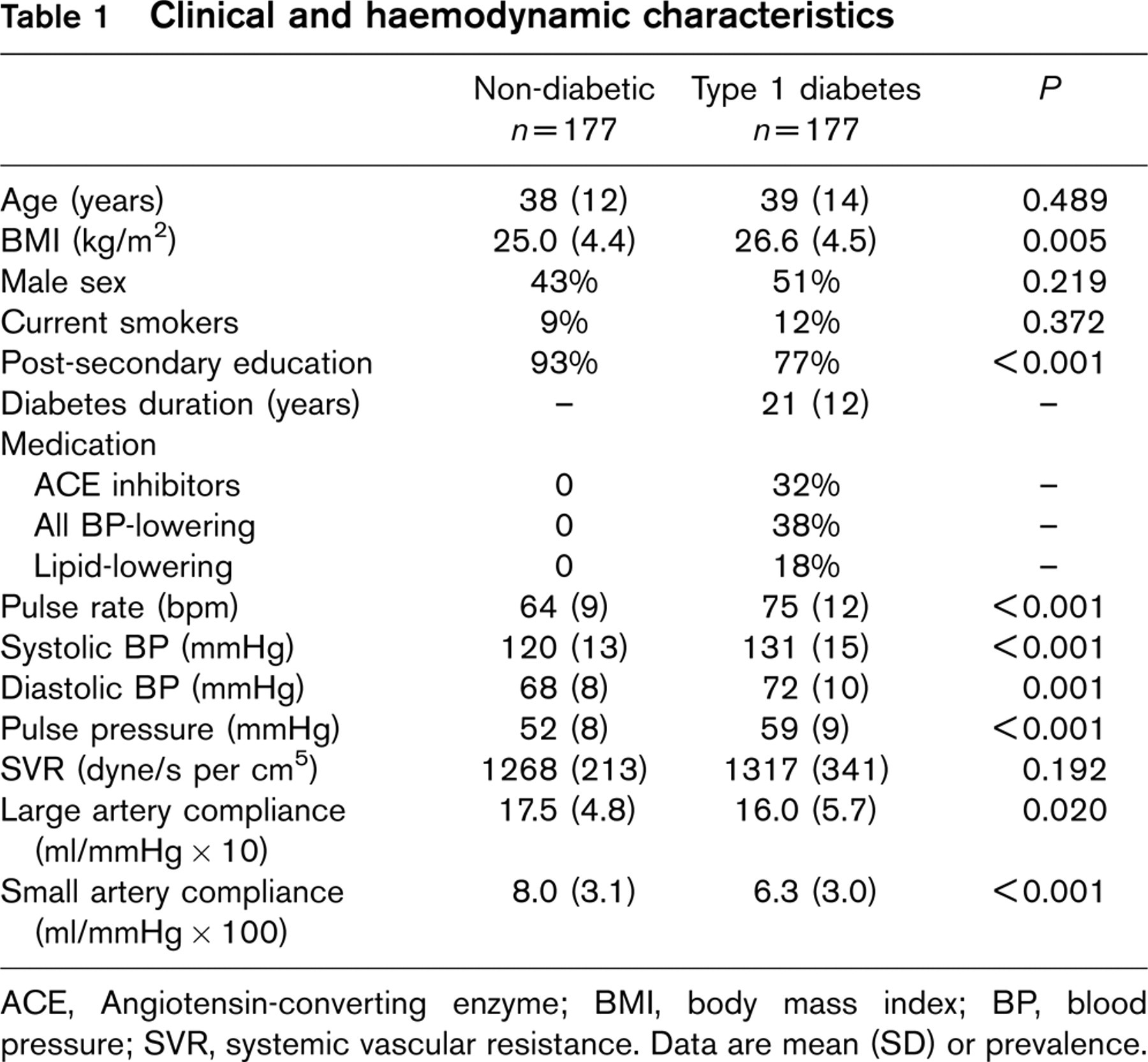
ACE, Angiotensin-converting enzyme; BMI, body mass index; BP, blood pressure; SVR, systemic vascular resistance. Data are mean (SD) or prevalence.
For non-diabetic participants, after adjustment for sex, there was no significant variation across categories of vigorous exercise in pulse rate, SBP, DBP, PP, SVR or small artery compliance, nor was there evidence of a linear trend across categories of exercise frequency (Table 2). Large artery compliance varied significantly across categories of vigorous exercise and mean large artery compliance was greatest for the group reporting one to two episodes of vigorous activity per week. There was a statistically significant interaction of sex with exercise frequency for small artery compliance (P = 0.029); there was a strong linear relationship between small artery compliance and exercise frequency for women (P = 0.001) but not for men (P = 0.528; Fig. 1).
For diabetic participants, after adjustment for sex, there was no significant variation across categories of vigorous exercise in SBP, PP or small artery compliance (Table 2). Linear trends approached significance for large artery compliance and SVR. Pulse rate decreased significantly with increasing exercise frequency. There was no significant interaction of sex with exercise frequency for small artery compliance (Fig. 1) or other haemodynamic variables.
Sex and haemodynamic variables by vigorous activity strata
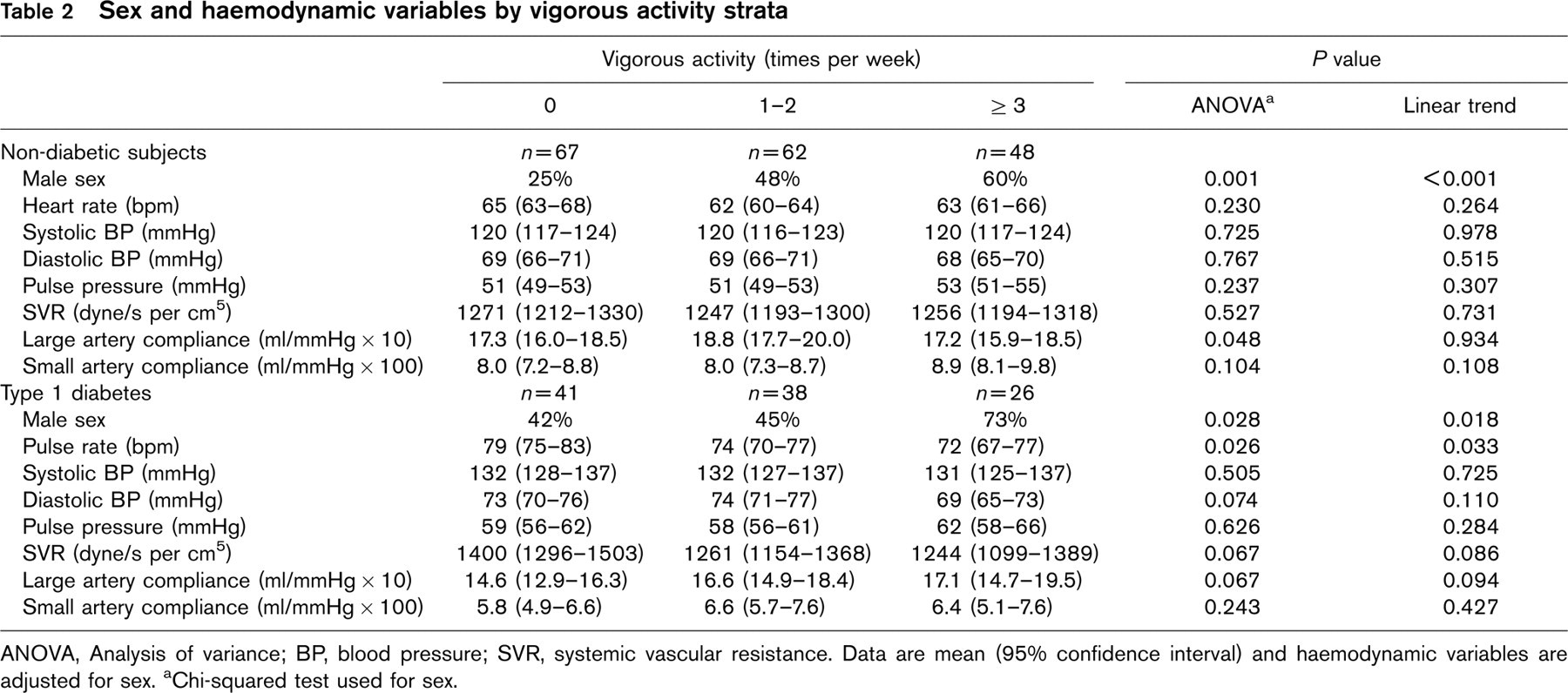
ANOVA, Analysis of variance; BP, blood pressure; SVR, systemic vascular resistance. Data are mean (95% confidence interval) and haemodynamic variables are adjusted for sex. aChi-squared test used for sex.
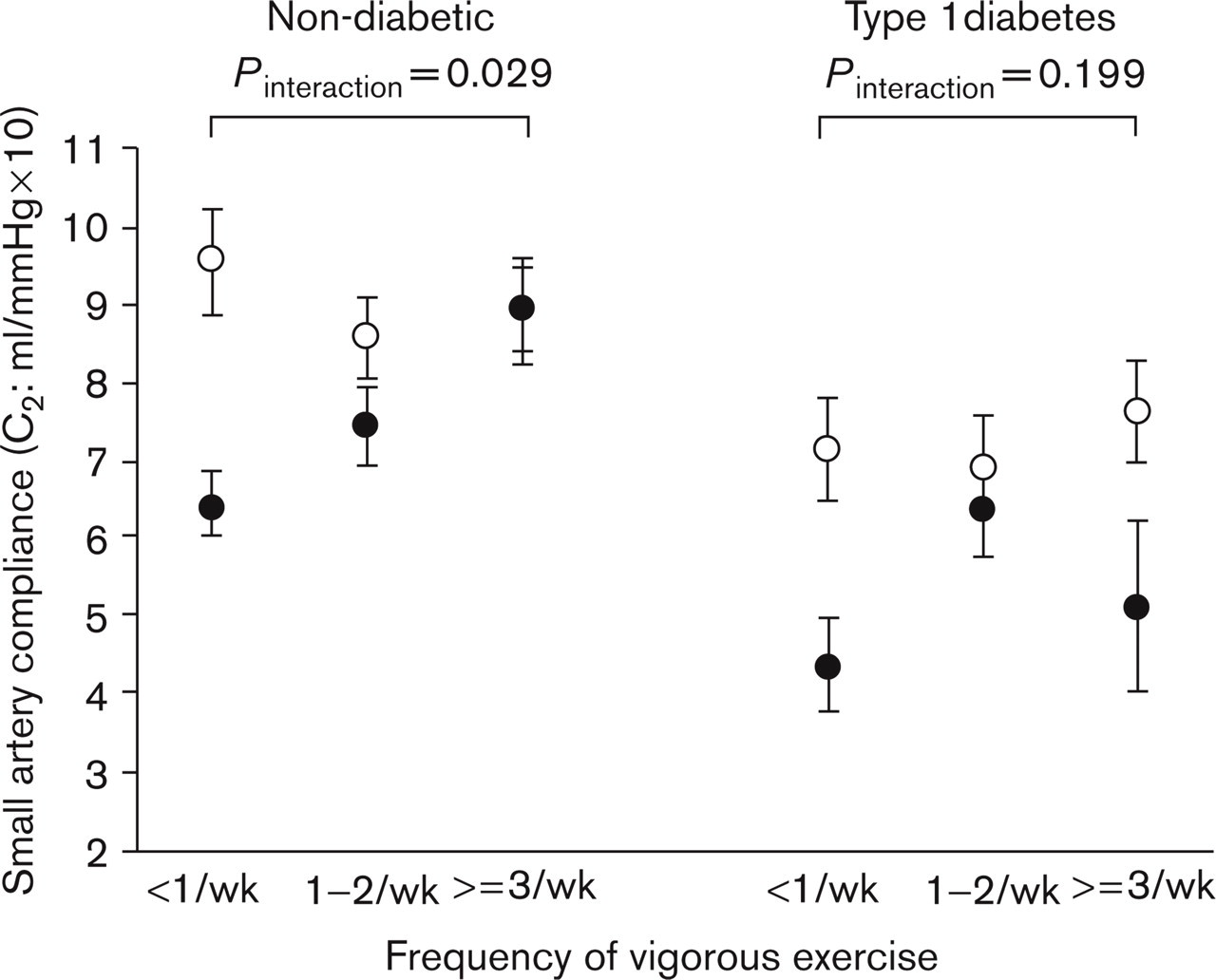
Small artery compliance according to frequency of vigorous activity, for men (open circles) and women (black circles). Data are mean (S.E.M.).
Independent correlates of arterial compliance were examined in multiple linear regression analysis. Models tested included age (categorized as < 30, 31–40, 41–50, 51–60, 61–70 years), sex (coded as male 1, female 0), height, blood pressure, smoking, diabetes status (coded as diabetic 1, non-diabetic 0) all known to be associated with small artery compliance [15, 25–27], and reporting three or more episodes of vigorous activity per week. Interaction terms between physical activity, sex and diabetes status were also tested. Variables (other than age, sex, diabetes status and physical activity) were excluded from the final model if P > 0.2. Independent predictors of small artery compliance were age (0.8 unit decrease for each 10 year increase in age), sex (1 unit greater in men), blood pressure (1 unit lower per 10mmHg increase in mean arterial pressure), height (positively) and being physically active (almost 1 unit greater for participants reporting three or more episodes of vigorous activity per week compared with less than three; Table 3). Type 1 diabetes was not a significant predictor of small artery compliance independent of blood pressure. The interaction terms of sex and diabetes with physical activity were not statistically significant. Smoking status did not approach significance (P > 0.2) and was not included in the final model, nor was the three-way interaction term of sex, diabetes and physical activity. The final regression model explained approximately half of the variance in small artery compliance. Independent predictors of large artery compliance were age (0.6 units lower per 10-year increase in age), blood pressure (1.7 units lower per 10mmHg increase in mean arterial pressure) and height (positively). Physical activity, diabetes status, sex and smoking were not independently associated with large artery compliance. The final regression model explained approximately one-third of the variance in large artery compliance (Table 3).
Linear regression analysis of small and large artery compliance
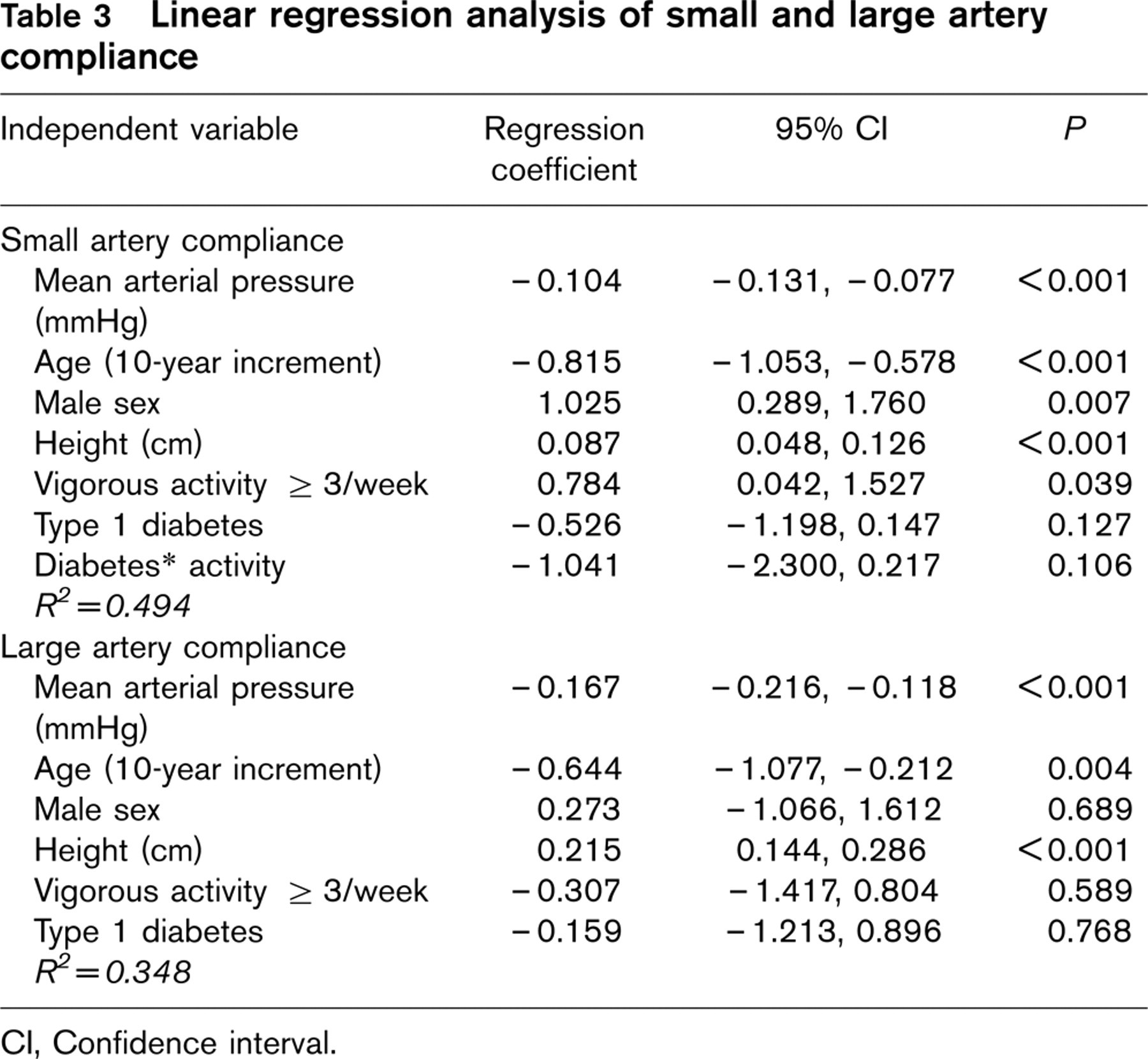
Cl, Confidence interval.
When pulse rate was included in the regression models of small artery compliance, it tended to weaken its (already modest) relationship with diabetes status, without pulse rate being a significant determinant itself and without affecting the observed relationship of small artery compliance with physical activity (data not shown). Pulse rate was a significant determinant of large artery compliance in regression analysis, but its inclusion in the model had little effect on the relationship of large artery compliance with other independent predictors, nor did it greatly improve the variance of large artery compliance explained by the model (not shown).
Discussion
In a group of non-diabetic, healthy participants from workplace and community-based populations, we found that the frequency of self-reported ‘vigorous’ exercise was significantly associated with greater arterial compliance: small artery compliance increased in a linear manner as the frequency of vigorous activity increased in women, and in multivariate analysis undertaking three or more episodes of vigorous activity per week was associated with significantly greater small artery compliance. The effect was clearly apparent for non-diabetic women, whereas evidence for a similar effect among men and in type 1 diabetes was inconsistent. Type 1 diabetic participants had lower small artery compliance than non-diabetic participants, consistent with a loss of compliance [25] and endothelial dysfunction [28] as previously reported. For diabetic participants, increasing exercise frequency was associated with a lower pulse rate, a well-established marker of cardiovascular fitness and associated with CVD risk [29]. The relationship of small artery compliance to exercise was independent of age and blood pressure, suggesting that exercise has beneficial effects on the vasculature preceding more overt changes in blood vessel structure and function. The results of linear regression analysis suggested that participating in three or more episodes of vigorous activity per week is associated with a small artery compliance value of approximately one unit greater compared with less active individuals. Other studies have shown that aerobic and anaerobic exercise training improves endothelium-dependent dilation in healthy participants [4, 30], consistent with the observed association of small artery compliance with exercise frequency. Physical exercise augments blood flow and shear stress, resulting in the upregulation of nitric oxide synthase activity [4]. Arterial compliance, especially small artery compliance, depends to some extent on endothelial regulation of vascular smooth muscle tone [31, 32]. We have previously demonstrated that flow-mediated dilation, a well characterized measure of endothelial function via nitric oxide synthesis, is strongly correlated with small artery compliance, as measured by PWA in both healthy participants and participants with type 2 diabetes [32]. The findings reported here thus support the hypothesis that the beneficial effects of exercise on small artery compliance are likely to be partly mediated through improvements in endothelial function and nitric oxide regulation.
For non-diabetic participants, we found no significant linear relationship of measures of large artery stiffness (PP and large artery compliance) with exercise frequency, although the linear association of large artery compliance with exercise frequency tended to be of significance in type 1 diabetes. The difference in large artery compliance between diabetic and non-diabetic groups was largely explained by differences in blood pressure. In contrast, previous studies in healthy participants reported associations between higher aerobic fitness levels and lower central arterial stiffness [33, 34]. The self-reported frequency of vigorous exercise (as opposed to aerobic fitness) is a less precise measure and a behavioural rather than an objective physiological variable, which may explain the different results observed here. Not all studies found beneficial associations between muscular strength training and large artery compliance [35].
The trend of increasing small artery compliance to increasing frequency of vigorous exercise in the healthy (female) population was less apparent in the type 1 diabetic participants. It is possible that the known effects certain medications have on vascular compliance [18, 36, 37] prevented any association from being observed. It is also possible that the adverse effects of diabetes on vascular structure and function outweigh the potential beneficial effects of exercise. Despite this, the trend of decreasing pulse rate to increasing episodes of vigorous exercise per week and the results of multiple regression analysis suggest the presence of the beneficial effects of exercise on cardiovascular function even in the presence of type 1 diabetes. In type 2 diabetes, 12 months of exercise training (endurance and muscle strength) resulted in improved maximum oxygen consumption and glycaemic control in the absence of haemodynamic changes [38].
This cross-sectional study has a number of limitations. PWA, although non-invasive, may lack sensitivity compared with ‘gold standard’ measures of vascular function, which have found significant effects of exercise on vascular function [4, 39, 40]. The present survey sample of ‘healthy’ participants was obtained largely through opportunistic sampling of workplace and community-based populations. The sample included a large proportion of individuals with post-secondary education and with a low prevalence of smoking, suggesting they represent a higher than average socio-economic status group. It is unlikely to be representative of the general Australian population, but the analysis of trends in cardiovascular variables across strata of exercise remain valid nonetheless. The effects of exercise in a higher CVD risk group may be even greater than observed here, given a lower baseline level of vascular health. Another aspect that needs consideration is that some participants may exercise more because they have an intrinsically higher cardiovascular capacity. It is likely that both factors, exercise levels and intrinsic cardiovascular capacity, play a role in determining vascular function. In keeping with this is the finding in heart failure patients that acute exercise capacity was limited with greater aortic stiffness (pulse wave velocity) [41]. However, the non-diabetic group includes only healthy participants, with no known cases of heart failure or less severe forms of overt CVD that could limit participation in physical activity. Finally, our measure of usual physical activity is likely to be somewhat imprecise, but this would tend to bias the results to the null.
In conclusion, we found that in an apparently healthy population, increasing episodes of vigorous activity per week were associated with greater small artery compliance. This result supports other findings that regular physical activity improves vascular health. In a type 1 diabetic population, small artery compliance was not associated with the frequency of vigorous exercise. This result does not undermine any role for exercise in the management of patients with type 1 diabetes, as the relationship between lower heart rate and the frequency of exercise implies an extent of cardiovascular benefit even in diabetes.
Footnotes
Acknowledgements
The authors would like to thank Connie Karschimkus and Craig Nelson for performing PWA measurements, and Drs Nelson, Wilson and O'Neal for assistance with participant recruitment and discussion.