
Abstract
Background
The observation that exercise training reduces cardiovascular mortality is robust and consistent, but the amount and intensity of exercise that is required for risk reduction is not yet resolved.
Methods
We studied the association between the amount and intensity of exercise and cardiovascular mortality in 27 143 men and 28 929 women who were free from known cardiovascular disease at the beginning of follow-up between 1984 and 1986. The relative risk of death was calculated as the rate of death among participants within a given physical activity category compared with the rate of death in the reference category (no physical activity). We used Cox regression analysis to adjust for age and other potentially confounding factors.
Results
After 16 years (SD 4 years) of follow-up, 2946 men (10.8%) and 2486 women (8.6%) had died from ischaemic heart disease or stroke. A single weekly bout of exercise of high intensity reduced the risk of cardiovascular death, both in men [relative risk (RR) 0.61, 95% confidence interval (CI) 0.49–0.75], and women (RR 0.49, 95% CI 0.27–0.89), compared with those who reported no activity. There was no additional benefit from increasing the duration or the number of exercise sessions per week. The risk reduction related to exercise increased with increasing age in men, but not in women.
Conclusion
These results challenge the current recommendation that expenditure of at least 1000 kcal per week is required to achieve exercise-induced protection against premature cardiovascular mortality.
Introduction
The observation that exercise training reduces cardiovascular mortality is robust and consistent [1, 2], but the amount and intensity of exercise that is required for risk reduction is not yet resolved [3]. Current guidelines recommend at least 30 min of daily exercise of moderate intensity, or 20 min of vigorous exercise at least three times per week, but these recommendations appear to be hard to fulfill for most people [4]. A central question has been ‘how little can I get away with, and at what intensity’, and implicitly, achieve protection against premature cardiovascular death. Interestingly, Lee et al. [5] showed that apparently healthy elderly men who exercised one to two times per week (so-called weekend warriors), had a lower risk of all-cause mortality compared with sedentary, apparently healthy men [relative risk (RR) 0.41, 95% confidence interval (CI) 0.21–0.81].
Many studies suggest that moderate exercise intensity is sufficient to reduce the risk of cardiovascular disease in women and in older men [6, 7], but there are indications that middle-aged men need vigorous exercise to achieve protection [8–12]. Tanasescu et al. [13] showed that high exercise intensity was associated with reduced risk in a study of health professionals, independent of the duration of activity. Lee et al. [14] showed a greater reduction in the risk of coronary heart disease with increasing exercise intensity in older well-educated men, and the protective effect extended to men who did not fulfill current recommendations for physical activity. Also, Lee and Paffenbarger [11] reported an inverse association between exercise intensity and mortality in university-educated men.
Previous studies of exercise amount and intensity related to cardiovascular mortality have depended on data from selected populations that may limit the generalizability of the results. In this prospective study, we assessed exercise amount and intensity in relation to subsequent cardiovascular mortality in a large, unselected population of men and women in Norway (n = 56 072) who were free from known cardiovascular disease at the beginning of follow-up.
Material and methods
Study population
In Nord Trøndelag County in Norway, the total adult population aged 20 years and older was invited to participate in the HUNT Study in 1984–1986. Of 85 100 individuals who were eligible to participate, 75 058 (88.2%) accepted the invitation. They filled in the questionnaire that was included with the invitation, and attended a clinical examination between 1984 and 1986. At the clinical examination, the participants received a second questionnaire that was to be filled in and returned from home in a pre-stamped envelope. The study has been described in detail elsewhere [15]. Briefly, information was collected on a range of health-related subjects, and included past and present smoking, self-reported physical activity, and among other items, the clinical examination included standardized measurements of blood pressure, body height, and body weight.
Based on self-reports, we excluded 6719 participants who had a history of myocardial infarction or stroke, or known angina pectoris or diabetes mellitus from the mortality follow-up. In addition, 387 participants were excluded as a result of missing information on height or weight. Information on physical activity was collected from the second questionnaire that was handed out in conjunction with the clinical examination. Of the 67 740 participants who were followed up for cardiovascular mortality, 56 072 (28 929 women and 27 143 men) filled in and returned the second questionnaire that included physical activity, and they constitute the cohort of this study.
The mortality follow-up of the HUNT cohort was approved by the regional committee for ethics in medial research, and by the Norwegian Data Inspectorate.
Physical activity
In the questionnaire that included leisure-time physical activity, the participants were asked three specific questions with various response options: ‘how often do you exercise?’ (never, less than once per week, once per week, two to three times per week, and four times per week or more); ‘how hard do you exercise?’ (no sweat, sweat, and exhausted); and ‘for how long do you carry on each time?’ (less than 15 min, between 15 and 30 min, between 30 and 60 min, and more than 60 min).
The responses did not differentiate well between exercise intensity indicated by ‘sweat’ and ‘exhausted’, and we therefore divided exercise intensity into low (no sweat) or high intensity (sweat and exhausted). For clarity, we divided the duration of activity into less than 30 min or 30 min or more per exercise session.
The majority of the study participants did not meet the current recommendation of at least 30 min of physical activity each day, or at least 3 days of vigorous-intensity activity per week [16]. Approximately 24% of the cohort reported exercising more than two times per week.
Separate validation study
We recruited a group of 53 men and 33 women who were self-selected and free from known cardiovascular disease to a separate validation study. The objective was to link the exercise intensities of no-sweat, sweat, and exhausted, as registered from the study questionnaire, to intensities measured by oxygen uptake and heart rate. We tested their maximal oxygen uptake and maximal heart rate as previously described [17], and they performed several exercise sessions of varying duration (20–30 min, 45–60 min, 75–90 min) and intensity (increasing from 40 to 100% of maximal oxygen uptake) within the next 30 days after initial testing. The subjects had a median age of 46 years (range 20–88), a median body mass index of 26.3 kg/m2 (range 18–36), a median maximal oxygen uptake of 44 ml/kg per min (range 14–79), and a median maximal heart rate of 180 beats/min (range 134–224). Thirteen of them were smokers.
Endpoints
The mandatory reporting of deaths by physicians and public health officers to the National Cause of Death Registry in Norway constitutes the basis for the coding of the underlying cause of death. Mortality follow-up to the Cause of Death Registry is virtually complete [18]. In this study, the primary endpoint was death caused by cardiovascular disease [International Classification of Disease (ICD) 9: 390–459; ICD 10: I 00–I 99]. Specific emphasis was given to deaths from ischaemic heart disease (ICD 9: 410–414; ICD 10: I 20–I 25) and stroke (ICD 9: 430–438; ICD 10: I 60–I 69).
Statistical analysis
Person-years were calculated from the date of attendance to the clinical examination during the period of data collection (1984–1986) until the date of death, or until the end of follow-up, 31 December 2002, whichever came first. The relative risk of death was calculated as the rate of death among participants within a given physical activity category compared with the rate of death in the reference category (no physical activity). We used Cox regression analysis to adjust for age (5-year categories) and other potentially confounding factors, including body mass index (< 18.5, 18.5–24.9, 25.0–29.9, ≥ 30.0 kg/m2), smoking status (never, former, current), systolic and diastolic blood pressure (in quintiles), use of blood pressure medication, use of alcohol (frequency last 2 weeks), marital status, and level of education (three levels). To test the equality of relative risks of cardiovascular mortality between different categories of physical activity we performed a Wald post-hoc test.
Characteristics of the study population
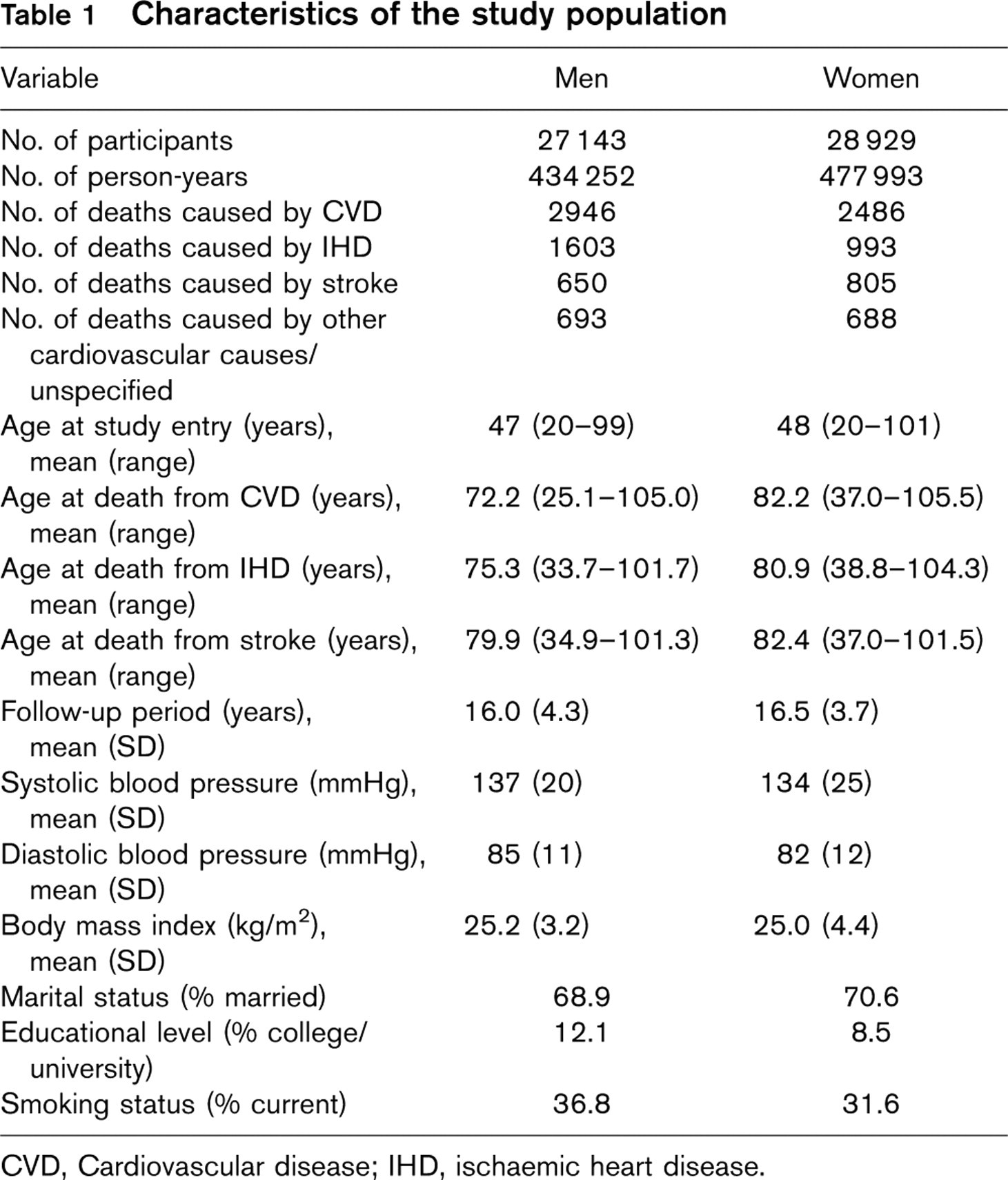
CVD, Cardiovascular disease; IHD, ischaemic heart disease.
All statistical analyses were conducted using SPSS for Windows, version 13.0 (SPSS Inc., Chicago, Illinois, USA), and all reported P values are two-sided.
Results
Baseline characteristics of the study population are presented in Table 1. During 16 years of follow-up, 2946 men (10.8%) and 2486 women (8.6%) had died from cardiovascular disease. In women, 993 deaths (39.9%) were caused by ischaemic heart disease, and 805 (32.4%) were caused by stroke. Among men, 1603 (54.4%) died from ischaemic heart disease and 650 (22.1%) from stroke.
Exercise and cardiovascular deaths
Table 2 shows the relative risk of dying from cardiovascular causes associated with various levels of exercise in men and women. After adjustment for potentially confounding factors, there was a significant risk reduction of 20% (RR 0.80, 95% CI 0.71–0.90) in men associated with exercising less frequently than once a week, compared with men who reported no activity. In women, there was a corresponding 6% risk reduction associated with exercising less than once a week (RR 0.94, 95% CI 0.82–1.05).
Relative risk with 95% confidence interval of death caused by cardiovascular disease among Norwegian men and women in combined categories of frequency, duration and intensity of physical activity
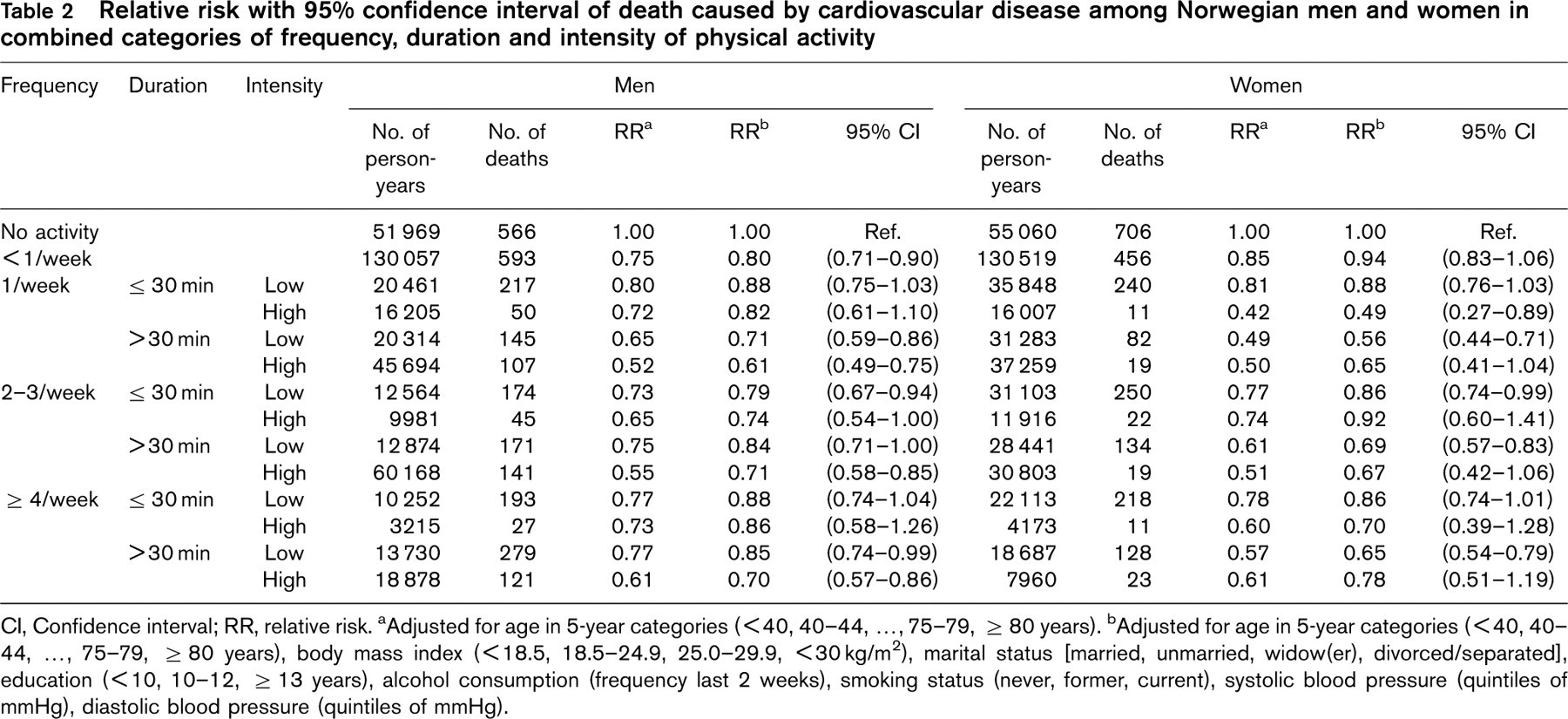
CI, Confidence interval; RR, relative risk.
aAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years).
cAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years), body mass index (< 18.5, 18.5–24.9, 25.0–29.9, < 30 kg/m2), marital status [married, unmarried, widow(er), divorced/separated], education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency last 2 weeks), smoking status (never, former, current), systolic blood pressure (quintiles of mmHg), diastolic blood pressure (quintiles of mmHg).
Relative risk with 95% confidence interval of death from ischaemic heart disease among Norwegian men and women in combined categories of frequency, duration and intensity of physical activity
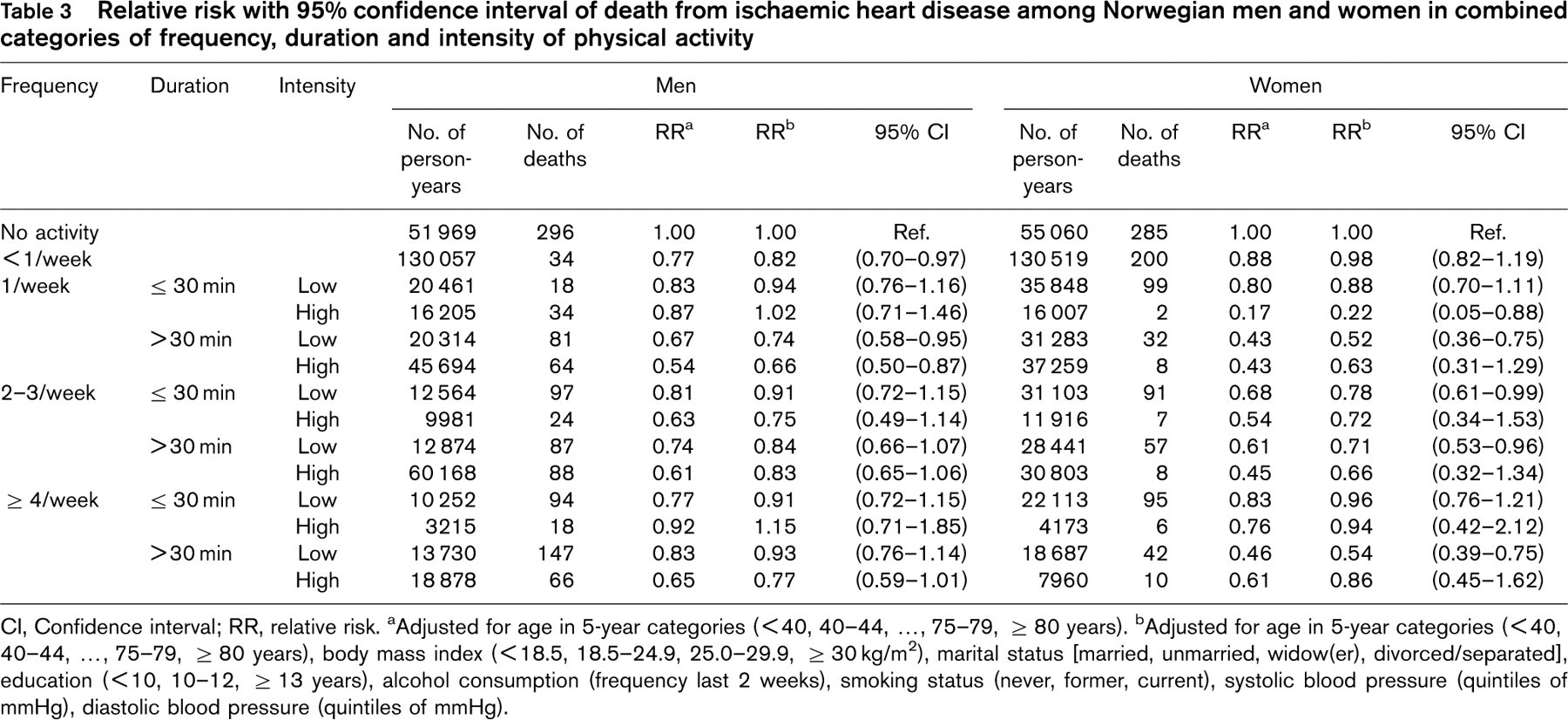
CI, Confidence interval; RR, relative risk.
aAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years).
bAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years), body mass index (< 18.5, 18.5–24.9, 25.0–29.9, ≥ 30 kg/m2), marital status [married, unmarried, widow(er), divorced/separated], education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency last 2 weeks), smoking status (never, former, current), systolic blood pressure (quintiles of mmHg), diastolic blood pressure (quintiles of mmHg).
We stratified the exercise according to frequency, duration, and intensity, and found that among men, a single weekly bout of high intensity, lasting more than 30 min, was associated with a 39% reduction (RR 0.61, 95% CI 0.49–0.75) in cardiovascular death, compared with men who reported no activity. Among men who reported a similar amount of exercise with low intensity, the reduction in risk was 29% (RR 0.71, 95% CI 0.59–0.86). Among men who reported four or more weekly bouts of high-intensity exercise, each lasting more than 30 min, there was no additional benefit (Wald P value 0.3) in relation to cardiovascular mortality (RR 0.70, 95% CI 0.57–0.86). The relative risk associated with four times of exercise of low intensity per week was 0.85 (95% CI 0.74–0.99), compared with men who reported no activity.
Among women who reported one weekly bout of high-intensity exercise for less than 30 min, the risk of cardiovascular death was 51% lower (RR 0.49, 95% CI 0.27–0.89) than for women who reported no activity.
There was no additional benefit of increasing the frequency of exercise (Wald P value 0.6). For women who reported four or more weekly bouts of high-intensity exercise, each lasting more than 30 min, the risk of cardiovascular death was 22% lower (RR 0.78, 95% CI 0.51–1.19). The same frequency of exercise, but with low intensity, was associated with a 35% risk reduction (RR 0.65, 95% CI 0.54–0.79), compared with women who reported no activity.
Exercise and death from ischaemic heart disease
The results related to physical exercise and death from ischaemic heart disease were quite similar to the results for cardiovascular mortality overall (Table 3). Therefore, among men who reported exercising once a week for more than 30 min of high intensity, the relative risk was 0.66 (95% CI 0.50–0.87), compared with men who reported no activity. The same frequency of exercise, but with low intensity, was associated with a relative risk of 0.74 (95% CI 0.58–0.95).
In women who exercised once a week, the reduction in risk was particularly apparent for exercise of high intensity (RR 0.22, 95% CI 0.05–0.88), compared with women who reported no exercise. For exercise of low intensity, there was no clear association with the risk of dying from ischaemic heart disease (RR 0.88, 95% CI 0.70–1.11).
Exercise and death from stroke
The relative risk of dying from stroke for men who exercised once a week for at least 30 min at high intensity was 0.51 (95% CI 0.31–0.86), compared with men who reported no activity. The relative risk associated with a similar frequency of exercise, but with low intensity, was 0.62 (95% CI 0.40–0.95; Table 4).
In women, the relative risk of dying from stroke associated with a single weekly bout of exercise of at least 30 min at low intensity was 0.63 (95% CI 0.42–0.94), compared with women who reported no activity, and there was no additional benefit of increasing the number of exercise sessions per week (Table 4).
Relative risk with 95% confidence interval of death from stroke among Norwegian men and women in combined categories of frequency, duration and intensity of physical activity
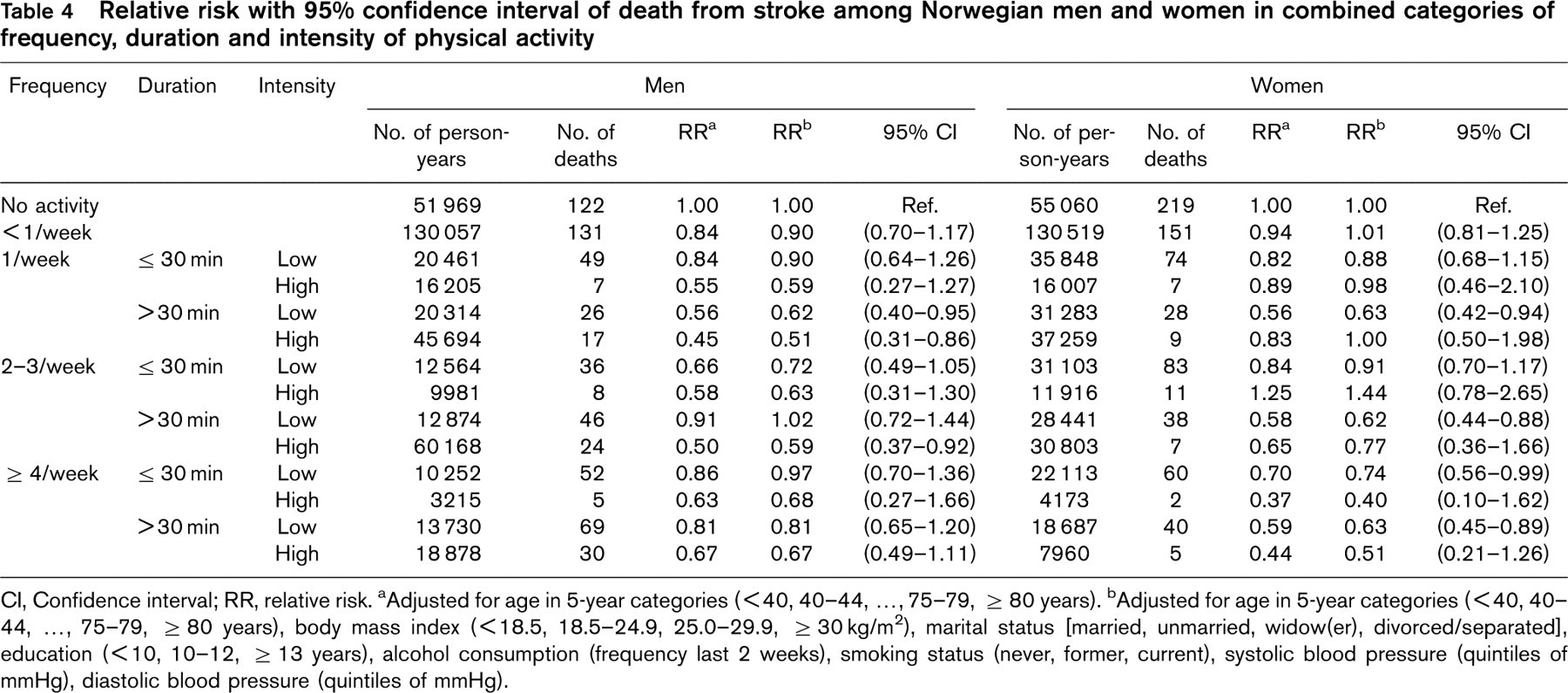
CI, Confidence interval; RR, relative risk.
aAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years).
bAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years), body mass index (< 18.5, 18.5–24.9, 25.0–29.9, ≥ 30 kg/m2), marital status [married, unmarried, widow(er), divorced/separated], education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency last 2 weeks), smoking status (never, former, current), systolic blood pressure (quintiles of mmHg), diastolic blood pressure (quintiles of mmHg).
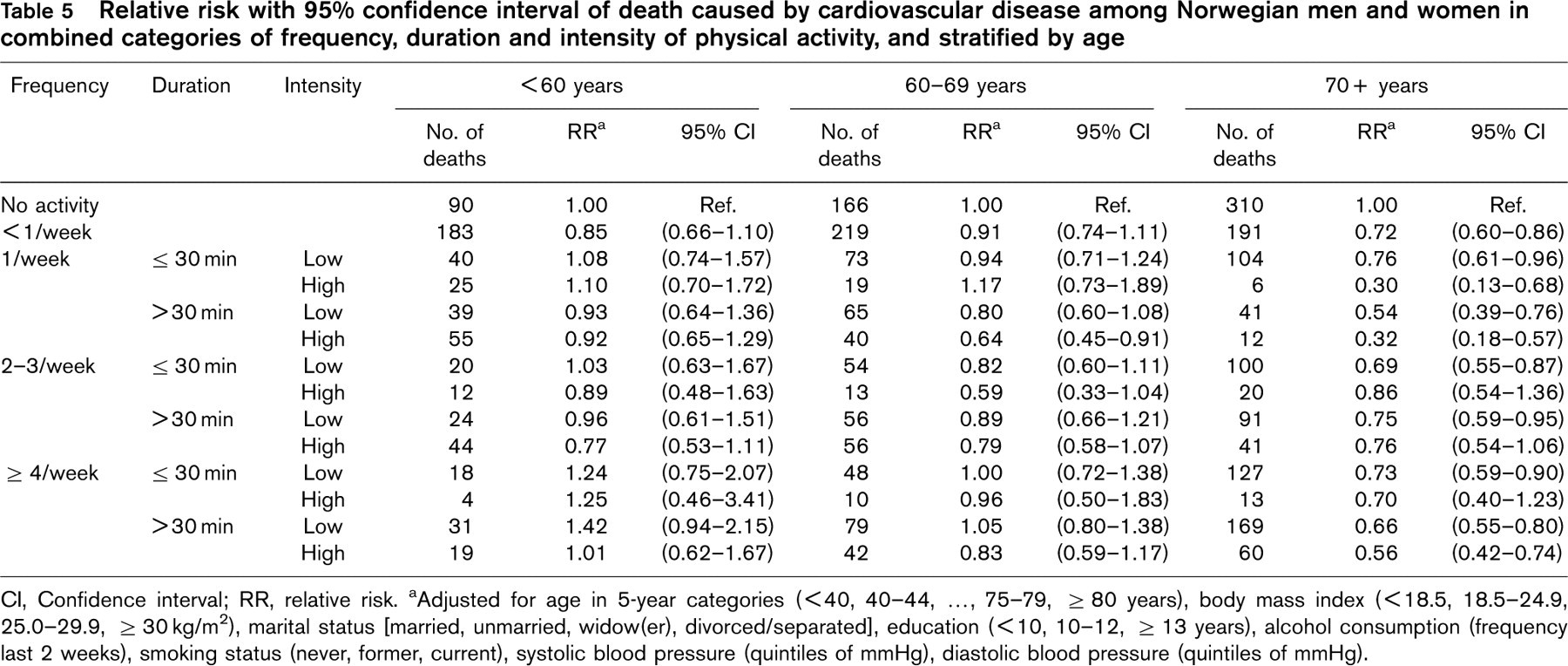
Relative risk with 95% confidence interval of death caused by cardiovascular disease among Norwegian men and women in combined categories of frequency, duration and intensity of physical activity, and stratified by age
CI, Confidence interval; RR, relative risk.
aAdjusted for age in 5-year categories (< 40, 40–44, …, 75–79, ≥ 80 years), body mass index (< 18.5, 18.5–24.9, 25.0–29.9, ≥ 30 kg/m2), marital status [married, unmarried, widow(er), divorced/separated], education (< 10, 10–12, ≥ 13 years), alcohol consumption (frequency last 2 weeks), smoking status (never, former, current), systolic blood pressure (quintiles of mmHg), diastolic blood pressure (quintiles of mmHg).
Age, sex and exercise-induced protection against cardiovascular mortality
In men, the reduction in cardiovascular mortality related to exercise increased with increasing age (Table 5), but in women, a similar age-related pattern could not be found (data not shown). There was no clear reduction in risk associated with physical exercise in men younger than 60 years of age, but in the age group 60–69 years, a single weekly bout of high-intensity exercise for at least 30 min was associated with a 36% reduction (RR 0.64, 95% CI 0.45–0.91) in cardiovascular mortality. In this age group, there was no reduction in risk associated with low exercise intensity, regardless of the duration and frequency of the exercise. In men 70 years or older, a single weekly bout of high-intensity exercise for less than 30 min was associated with a 70% reduction in the risk of cardiovascular death (RR 0.30, 95% CI 0.13–0.68). A similar frequency of low-intensity exercise was associated with a 24% lower risk (RR 0.76, 95% CI 0.61–0.96). There was no additional benefit of increasing either the frequency or duration of exercise among men 70 years and older.
Validation study
In our separate validation study (Table 6) there were no differences by age and sex in reporting exercise intensity (no sweat, sweat, and exhausted), or in observed exercise intensity according to maximal oxygen uptake. No sweat corresponded to an intensity of approximately 55% of maximal oxygen uptake, regardless of the duration of the exercise up to 90 min. Sweat and exhausted corresponded to an exercise intensity of 71–75 and 76–90% of maximal oxygen uptake, with decreased relative intensity with increasing duration of exercise (Table 6).
Average exercise intensity in relation to maximal oxygen uptake and maximal heart rate
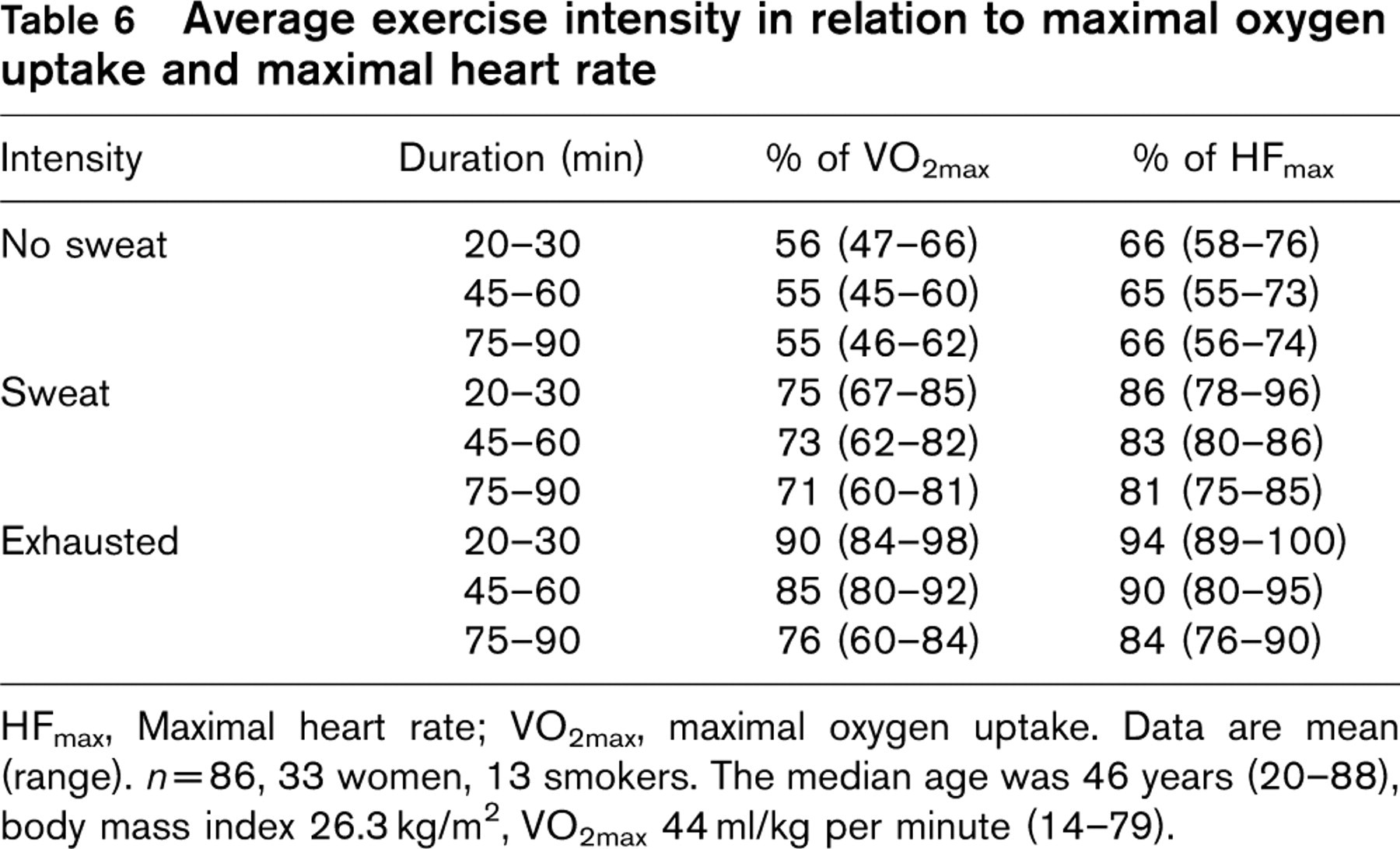
HFmax, Maximal heart rate; VO2max, maximal oxygen uptake. Data are mean (range). n=86, 33 women, 13 smokers. The median age was 46 years (20–88), body mass index 26.3 kg/m2, VO2max 44 ml/kg per minute (14–79).
Discussion
A single weekly bout of exercise was associated with a reduced risk of cardiovascular death (ischaemic heart disease and stroke) in this mortality follow-up of a large unselected population of men and women who were free from known cardiovascular disease at baseline.
Ischaemic heart disease
Our results are in line with other studies [5, 19] in showing that physical activity may prevent cardiovascular disease. The large and unselected population combined with long-term mortality follow-up are strong features of our study. Our results suggest that men and women who exercise to a moderate degree, and spend less than the recommended energy (i.e. < 1000 kcal/week), are at lower risk of dying from ischaemic heart disease than those who never exercise. In contrast to studies of male college alumni, in which mortality from ischaemic heart disease was gradually reduced with increasing energy expenditure from 500 to 3500 kcal per week [19], we found no additional benefit associated with as many as four high-intensity sessions per week compared with a single weekly bout. Our results therefore challenge current recommendations that require caloric expenditure of at least 1000 kcal per week to achieve exercise-induced protection against premature cardiovascular death.
Assuming that the observed exercise intensities in our validation sample of 86 individuals (Table 6) is representative of the HUNT population, the usual weekly energy expenditure may be estimated. Using the exercise intensity from the validation study, an individual with maximal oxygen uptake of 3.51 per min may for example perform a single weekly exercise bout for 45 min at 80% of maximal oxygen uptake, or four bouts of 75 min each at 55% of maximal oxygen uptake. It is known that physical exertion that requires 11 oxygen uptake per min corresponds to 5 kcal in energy expenditure [20]. In our example, 80% of maximal oxygen uptake therefore requires 2.81 per min or 14 kcal per min. In other words, during a workout of 45 min energy expenditure will be 630 kcal. In comparison, exercising a total of 300 min per week at 55% of maximal oxygen uptake requires 1.941 per min or 9.71 kcal per min; yielding a total energy expenditure of 2913 kcal. It is reasonable to assume that exercise intensity during the 45 min is not likely to be much higher than 80% of maximal oxygen uptake, as previously reported [20]. If anything, this suggests that energy expenditure could be overestimated, and is not likely to be close to the 1000 kcal that is recommended in the current guidelines, and far below the energy expenditure of exercising four times per week with a total duration of 300 min. Therefore, substantially less exercise than is currently recommended [16] may be sufficient to reduce cardiovascular mortality.
On the other hand, sporadic physical activity appears to increase the risk of musculoskeletal injuries, and for weight control, a very modest level of activity is certainly not sufficient. However, there is evidence that overweight individuals who engage in regular physical exercise may achieve cardiovascular protection compared with individuals who report no physical activity [21].
Difference by age and sex
Another striking finding from this study was that exercise training became more important with increasing age in men, but not in women. Fleg et al. [22] recently showed that the rate of decline in aerobic fitness was higher than 20% per 10 years in the age group 70 years and older, and that the decline was stronger in men than in women. As the decline in aerobic fitness accelerates with age, and maybe more so in men than women, this may be one reason why exercise training becomes increasingly more important with increasing age, as we observed for men.
Possible mechanisms behind the protective effect of a single bout of exercise
It has previously been thought that the effects of physical activity are short lived, and that several weeks of exercise training are necessary to achieve beneficial effects on the cardiovascular system. However, it is now well known that a single bout of exercise induces changes that may last from minutes to days after the cessation of the exercise. A single bout may improve endothelial function, which is a strong and independent marker for long-term cardiovascular morbidity and mortality [23]. However, the decline in endothelial function after the cessation of exercise, or the effect of different exercise intensities, is not known.
Stroke
Stroke is the third leading cause of death and long-term disability in western countries. More than half a million US adults suffer from stroke each year [24], and approximately 25% of these strokes are fatal [25]. Effective treatment is limited, and survivors require lengthy rehabilitation and care. Primary prevention is therefore imperative to reduce the burden of stroke. However, whether physical activity reduces the risk of stroke remains controversial. One meta-analysis showed that a moderate to high level of physical activity was associated with reduced risk both for ischaemic and haemorrhagic stroke, compared with a low level of activity [26]. Our results show that both high and low-intensity exercise may be associated with a reduced risk of stroke in both men and women.
Limitations of the study
Physical activity and other predictors of mortality were assessed before follow-up, but assessment took place only once, and updated information throughout the follow-up period would be valuable. Individual changes in physical activity and other predictors of disease could thus not be taken into account in the analysis. Furthermore, we cannot exclude the possibility that the reported physical activity may be a marker of other health behaviour that we did not measure, and thus could not adjust for in the statistical analysis.
Conclusion
A single weekly bout of exercise training may prevent cardiovascular deaths among men and women without known cardiovascular disease, and in men, the importance of exercise appears to increase with age. Our results challenge current recommendations that require at least 1000 kcal of caloric expenditure per week to achieve exercise-induced protection against premature cardiovascular death.