
Abstract
Background
Patients' beliefs about the causes of their heart disease (causal attributions) are important to effective medical communication, psychological adaptation, and adherence to advice. We assessed the extent to which causal attributions relate to risk factors, sex and socio-economic status in men and women diagnosed with acute coronary syndrome.
Design
We conducted an interview and questionnaire study of 171 acute coronary syndrome patients assessed within 5 days of admission to three hospitals in the London area.
Method
Patients rated beliefs in the role of 16 factors in causing their heart disease. Associations between attributions and risk factors were assessed, and differences in beliefs by sex and socio-economic status (defined by educational attainment) analysed.
Results
The most common attributions were to stress, smoking, high blood pressure, chance or bad luck, and heredity. Attributions were strongly associated with risk factors: 90% of smokers attributed heart disease to smoking, compared with 0% never smokers; 90.4% of hypertensives attributed heart disease to high blood pressure, 72.2% of patients with a positive family history to heredity, 85% of obese patients to being overweight, and 49% of sedentary patients to lack of exercise. Attributions to stress were related both to current mood and reports of recent life stress. There were few sex differences, but higher socio-economic status patients were more likely to attribute heart disease to heredity and genetic factors.
Conclusions
Causal beliefs about heart disease are strongly associated with risk factors. Effective communication about modifiable risk factors may influence causal beliefs and stimulate lifestyle change, thereby promoting secondary prevention.
Keywords
Introduction
Patients' beliefs about the causes of their heart disease (causal attributions) are part of the overall mental representation of the illness [1]. They may be partly based on lay beliefs [2], but will also be influenced by the medical knowledge of the patient and information provided by medical staff.
There are variations between studies of patients with coronary heart disease (CHD) in the relative importance of different causes. Stress has been ranked as the commonest cause in many studies [3–7], while in others family history is most frequently cited [8, 9]. Smoking is ranked high in some studies [3, 6], but relatively low in others [7, 8]. Understanding the source of these variations is important for patient care. One plausible explanation is that they relate to risk factor awareness. The associations between risk factors and causal attributions, however, have been inconsistent [4, 9–11]. In the present study, we related causal attributions of smoking, high blood pressure, hereditary, sedentary lifestyle, body weight, tiredness, and other medical problems, to information about the occurrence of associated risk factors, in order to test the strength of associations in a sample of newly admitted patients with acute coronary syndrome (ACS). We also related stress attributions to recent stressful life experience and current mood states.
There is some evidence that socio-demographic factors, such as sex and socio-economic status (SES), are related to causal attributions, although results have again been inconsistent [11–13]. Such variations may be significant clinically, since they influence effective communication with different types of patient. We therefore carried out analyses comparing causal attributions in male and female ACS patients, and in patients varying by SES as defined by educational attainment.
Method
Participants
Participants were 171 patients admitted with an ACS to one of three hospitals in the London area. ACS was diagnosed by the presence of chest pain plus verification by electrocardiographic and biochemical (troponin or creatine kinase) measures [14]. Patients were eligible if they could recall a specific time of onset of symptoms, and did not have co-morbid conditions that might influence either symptom presentation or mood, including severe psychiatric illness, ongoing infection, inflammatory conditions, or conditions that might cause false troponin positivity [15]. Patients were excluded if they could not complete measures in English, and were aged under 18 or over 90 years. These criteria were in place for recruitment of participants for other aspects of the study not described here [16]. A total of 217 patients were eligible for the study, of whom 27 were discharged or transferred to another hospital before being interviewed, and 19 (8.8%) refused to participate.
Procedure
Patients were interviewed in hospital an average of 2.56 ± 1.5 days after admission, and the circumstances surrounding the cardiac admission were assessed. Patients' beliefs about the causes of their heart problem were measured within 10 days of admission using a questionnaire containing 16 possible causes, based on the major categories described by French et al. [17] and Gudmundsdottir et al. [6]. Patients rated their belief in the extent to which each factor contributed to their heart problem by endorsing one of three response options: yes, maybe, and no. The list of items is given in Table 1. At the same time, participants completed the Beck Depression Inventory (BDI), and the anxiety subscale from the Hospital Anxiety and Depression (HAD) scale within 10 days of admission. Patients' beliefs about causes might be influenced by negative affectivity biases [18]. We therefore measured negative affect using the subscale from the Type D questionnaire for inclusion as a covariate in analyses [19].
Causal attributions for heart disease
During the interview, patients were also asked about stresses in their lives, and whether they had experienced stress over the past 4 weeks due to problems related to their partner, family, work, or other illnesses. Subsequently, these responses were divided into positive and negative categories. They were also asked if they had experienced unusual fatigue over the past 4 weeks.
Other measures
Information about clinical factors during admission, management, risk factors, cardiovascular and psychiatric history, and other current medical problems was collected from medical notes. Admission electrocardiograms and biochemical data were reviewed by a cardiologist, and were classified for presentation as ST elevation myocardial infarction (STEMI), non-STEMI, or unstable angina. Composite 6-month risk scores were computed on the basis of the algorithm developed in the Global Registry of the Acute Coronary Events (GRACE) study [20]. This uses nine measures to define the risk of 6-month post-discharge death. Smoking and habitual physical activity were assessed using standard measures [21], and body weight was measured. Educational attainment was categorized into no qualifications, primary qualifications, and secondary or higher. Body mass index (BMI) was computed, and patients were classified into normal weight (BMI < 25), overweight (BMI 25–29.9) and obese (BMI ≥ 30).
Statistical analysis
Six of the patients provided ratings of fewer than 10 of the causal attribution items, so they were excluded from the final analysis, leaving 165 patients. These six individuals did not differ on demographic or clinical characteristics from the remainder. Analysis of causal attributions was carried out by computing the proportion of patients answering ‘yes’ to each item, and the proportion giving any positive attribution (yes or maybe). Results were comparable with the two methods, so the findings presented here are based on the proportion giving any positive attribution.
Associations between causal attributions and related risk factors were analysed using logistic regression, and odds ratios adjusted for age and sex [with 95% confidence intervals (CI)] are presented. The analyses of causes other than stress included negative affect as an additional covariate to take account of dysphoric reporting biases. Associations between causal attributions, sex, and SES were also assessed.
Results
The participants in this study were predominantly white, relatively poorly educated men admitted with a STEMI (Table 2). A substantial number were former or current smokers, and more than 50% had a history of heart disease within their immediate family. Scores on the BDI indicated moderate depression levels on average, and 35.7% had ratings of 10 or over. Women were an average 2 years older than men (P < 0.001), and had significantly higher anxiety scores in hospital (P = 0.013), while men were more likely to be current or former smokers (P= 0.022).
Description of the sample
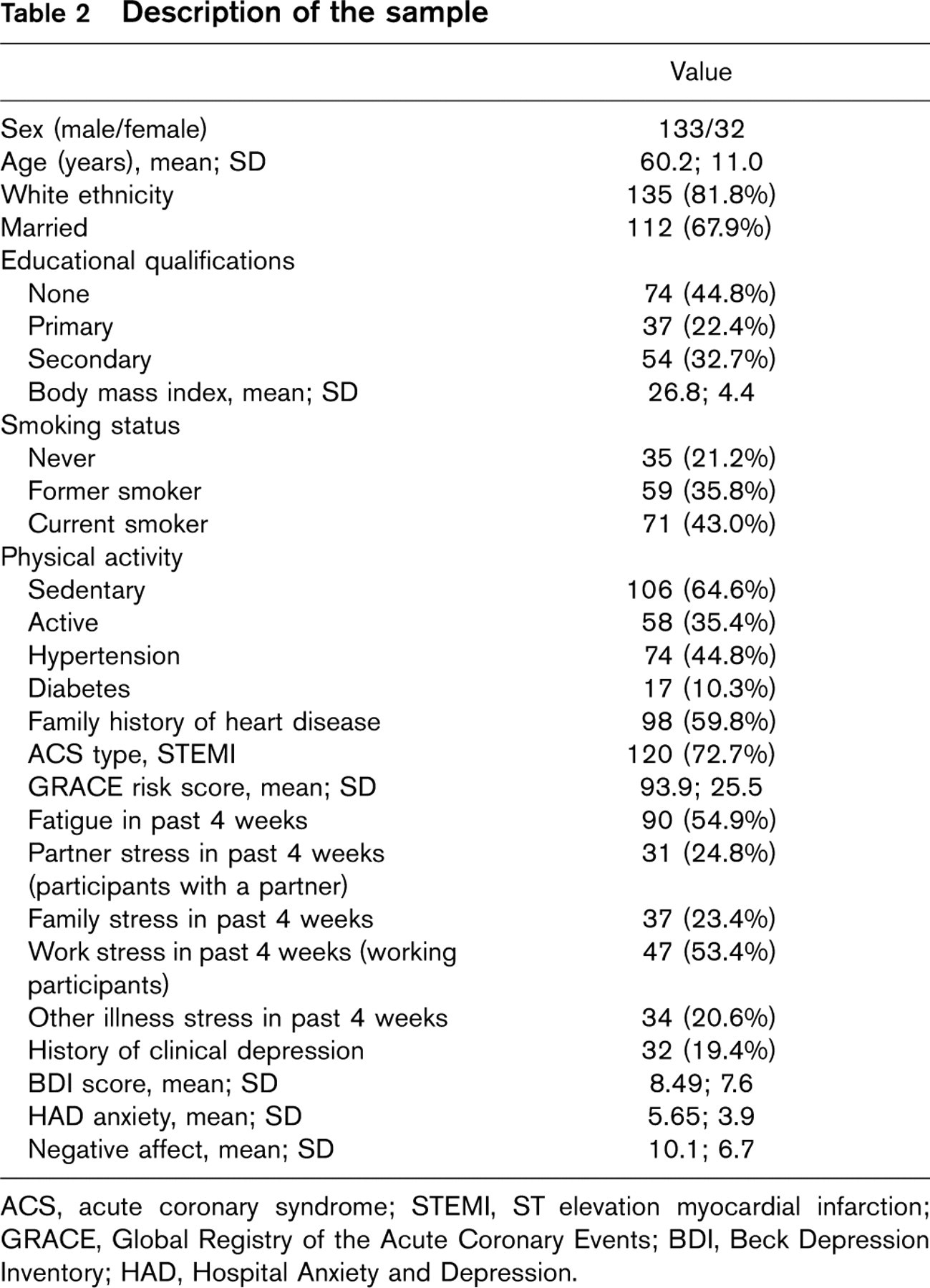
ACS, acute coronary syndrome; STEMI, ST elevation myocardial infarction; GRACE, Global Registry of the Acute Coronary Events; BDI, Beck Depression Inventory; HAD, Hospital Anxiety and Depression.
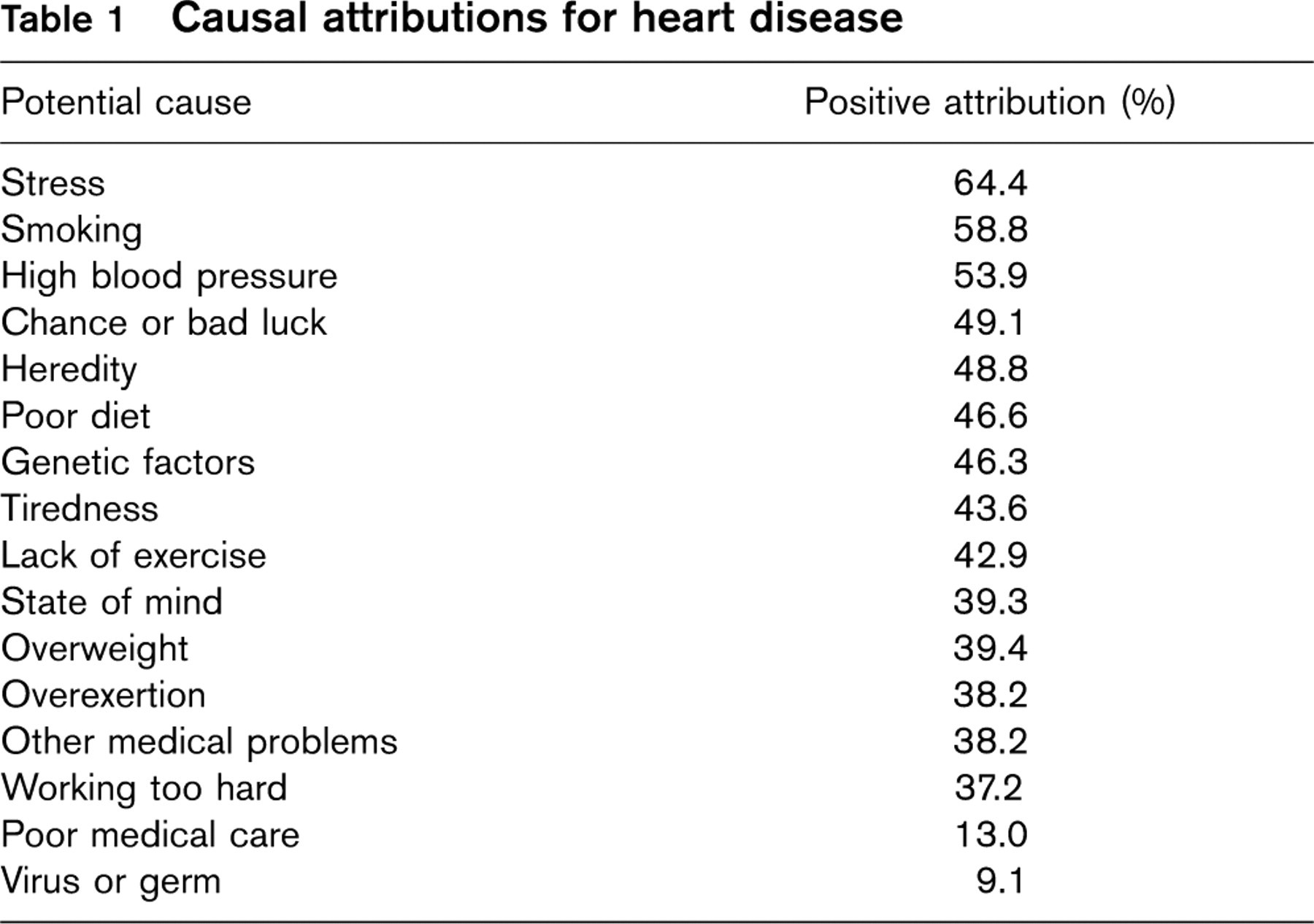
Patients' causal attributions for heart disease are ranked in Table 1. Stress was the most frequently rated cause, followed by smoking, high blood pressure, chance or bad luck, and heredity. Fewer than 20% of patients attributed their heart disease to poor medical care in the past, or to a virus or germs. There were no associations between causal attributions and clinical presentation of ACS or cardiological risk as defined by GRACE risk scores.
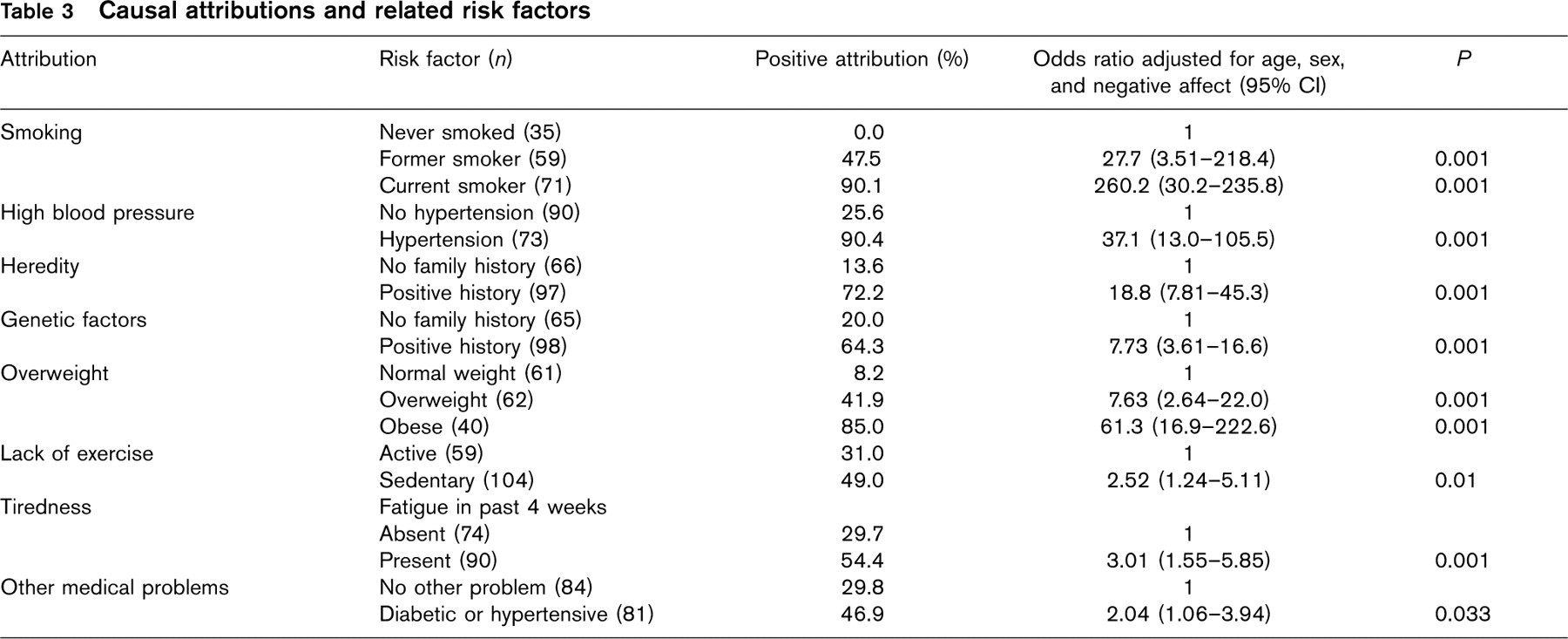
Associations between causal attributions and risk factors are summarized in Table 3. Some 90% of current smokers believed that smoking was a causal factor in heart disease, compared with 47.5% of former smokers, and none of the never smokers. The odds adjusted for age, sex and negative affect of a current smoker attributing heart disease to smoking were 260.2 compared with never smokers. In the same way, patients with hypertension were 37 times more likely to attribute heart disease to high blood pressure (P < 0.001), and those with a family history of CHD were 18 times more likely to believe that heredity contributed to their illness, and were also more likely to endorse genetic factors (P < 0.001). Of obese patients, 85% attributed heart disease to being overweight, compared with 8.2% of those with a BMI under 25, and adjusted odds ratio of 61.3 (P < 0.001). Sedentary individuals were more likely to believe that lack of exercise was a cause (P < 0.01), while the belief that tiredness was a cause was positively associated with reports of fatigue over the previous 4 weeks (P < 0.001). The belief that other medical problems contributed was related to the presence of diabetes or hypertension (P= 0.033).
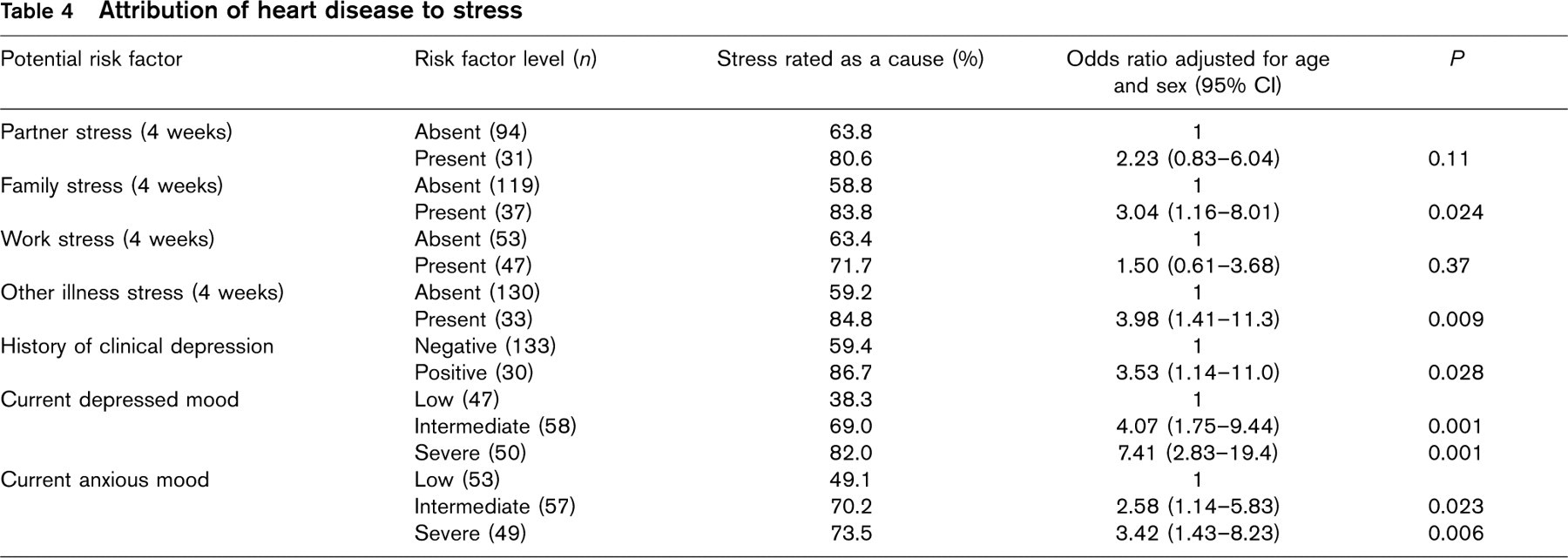
We assessed associations between belief in stress as a cause and both recent life stress and mood disturbance. Patients who reported family stress (P = 0.024), or stress due to other illness (P = 0.009) over the past 4 weeks were more likely than others to believe that stress contributed to their heart disease (Table 4). Associations with a history of depressive illness and with anxiety and depression in hospital were also observed (P = 0.028–0.001). For example, 82% of patients with BDI scores in the upper tertile believed stress was a cause, compared with 38.3% in the lower tertile, with an odds ratio of 7.41 after adjustment for age and sex. Ratings of recent life stress might be affected by current mood. Consequently, we entered both current depression and the life stress measures in the same regression models. When this was done, the association between causal attributions to stress and depressed mood was retained (P < 0.001), while the associations with family and other illness stress were no longer significant.
Men were more likely than women to attribute heart disease to smoking (60.2 versus 37.5%, P= 0.029), poor diet (53.0 versus 19.4%, P < 0.001), and working too hard (41.4 versus 19.4%, P= 0.024), while more women than men believed that chance or bad luck was responsible (43.6 versus 71.9%, P= 0.005). After adjustment for age and negative affect, the sex differences remained significant for poor diet (P = 0.001), and for chance or bad luck (P = 0.034), but not for the other attributions.
Causal attributions and related risk factors
Attribution of heart disease to stress
Two causal attributions were associated with SES as defined by education. A significantly greater proportion of patients in the highest education category attributed heart disease to heredity (63.0%) than those with intermediate (48.6%) or low (38.4%) education (P = 0.006). The same pattern was present for beliefs that genetic factors were responsible (61.1 versus 44.4 versus 36.5%, P= 0.006). These effects remained significant in logistic regression after adjustment for age, sex and negative affect. Theoretically, such patterns could be due to greater prevalence of heart disease among relatives of the more educated group, since family history of heart disease is associated with beliefs in heredity and genetic factors (Table 3). When analyses were limited to patients with a positive family history, however, differences persisted. The odds of attributing heart disease to heredity in the most compared with the least educated groups were 3.36 (95% CI 1.01–11.2, P= 0.048) adjusted for age, sex and negative affect, while the odds for genetic factors were 3.45 (95% CI 1.18–10.1, P= 0.024).
Discussion
This study was designed to assess acute cardiac patients' beliefs about the causes of their illness, and understand how these develop. Acute coronary syndromes are threatening and unwanted conditions, and most people try to make sense of their experience by developing views of what caused their problem [22]. Identifying causes may engender a sense of predictability and control over illness, and so help in the coping process [1]. From the clinical perspective, causal attributions are significant for several reasons. First, effective communication between patients and medical staff is impeded if patients have different models of cause from those held by clinicians; patients may lose confidence in the doctor's knowledge, and be less likely to follow advice. Second, beliefs about cause may stimulate efforts at secondary prevention [7]. Third, some causal attributions may be maladaptive and engender invalidism and poor psychological adjustment; in one study, attributions of heart attacks to stress were associated with long-term morbidity [3].
Causal attributions have been described as post-hoc interpretations or redefinitions of what caused the illness [1]. As such, they may be socially constructed, and the products of stereotypic lay beliefs. Stress, for example, is commonly reported as a cause not only of heart disease, but also of rheumatoid arthritis, diabetes and breast cancer [22]. Patients admitted to modern coronary care facilities, however, are provided with extensive information about their health status and risk factors, while medical information through the internet and mass media is increasingly accessible. This may lead to more veridical causal attributions concerning heart disease than in the past.
The overall ranking of causes in this study was comparable with several previous reports, with stress, smoking, and high blood pressure being the most frequently endorsed factors [5, 6, 9]. The proportion of patients endorsing these causes was higher than in some other studies. For example, 53.9% of patients attributed their heart disease to high blood pressure, compared with 15% or fewer in other studies [10, 11]. These differences may relate to the method of scoring attributions [19]. Some studies have used open-ended questions to assess causal attributions, and rates are typically lower than those generated with the checklist approach used here. We also aggregated possible and definite endorsements to generate the positive attribution scores, following the procedure used by Gudmundsdottir et al. [6]. This method is appropriate, since many patients may not be sufficiently confident about their views to state that a factor definitely caused their disease.
There were striking associations between risk factors and the frequency of endorsement of several causal attributions in this study. There was almost universal agreement among smokers, hypertensives, and obese patients that their heart disease was caused in part by smoking, high blood pressure, and overweight respectively (Table 3). The odds ratios for these effects were very high and were significant after adjusting for negative affect along with age and sex. Strong associations were also observed between beliefs in heredity and genetics and family history of CHD, sedentary lifestyle and lack of exercise, and the presence of diabetes or hypertension and belief that other medical problems were relevant.
These data suggest that the presence of risk factors is a strong determinant of patients' attributions about the causes of heart disease. Other studies have shown less concordance between risk factor presence and causal attributions [9–11]. For example, Astin and Jones [11] found in a sample of patients undergoing percutaneous coronary angioplasty that although hypertension was diagnosed in more than 50%, just 3% of male and 6% of female patients cited it as a cause of their CHD. Murphy et al. [9] reported that only 15% of obese patients attributed CHD to obesity. There are several explanations of this discrepancy from earlier literature. First, studies that have reported low concordance have frequently used open-ended rather than cued methods to elicit attributions. Open-ended approaches require patients to make a definite statement of belief, which they may feel reluctant to do. Second, the pattern will vary with the quality of communication in the hospital. If patients with ACS are advised by medical staff that smoking, body weight, physical activity, heredity and other factors are relevant, they will be more likely to make these attributions. Findings will therefore vary between hospitals, depending on the quality and intensity of communication. These results endorse the need to inform patients emphatically about the relevance of modifiable risk factors.
Attributions of heart disease to stress present a different problem. Psychosocial factors such as work stress, social isolation and depression have been identified as risk factors for CHD in prospective epidemiological studies [23]. It is therefore possible that attributions to stress are veridical, and reflect greater exposure to a chronic life stress in these individuals. Negative mood states, however, may also colour causal attributions. Day et al. [8] recently showed that patients who endorse stress and other negative emotional states as causes tend to have elevated anxiety and depression scores. In the present analysis, we found evidence both for recent stress exposure and for current mood being relevant to the belief that stress is a cause of CHD. When recent life stress and current mood were entered simultaneously into regression models, mood remained a significant determinant of stress attributions, while life stress did not. The causal links between stress attributions and negative mood states are unclear. One explanation may be that stress attributions are characteristic of people who experience post-ACS depression. Since depressive symptoms may predict greater morbidity following acute myocardial infarction (MI) and other forms of ACS [24], it could be that the negative impact of causal attributions to stress are relevant because they reflect depression in the days and weeks after admission. Interestingly, Affleck et al. [3] observed that attributing heart attacks to stress predicted greater morbidity over an 8-year period. Alternatively, stress attributions may be dysfunctional, stimulating greater depressive responses.
The differences between men and women in causal attributions were rather modest once age and negative affect had been taken into account. Martin et al. [13] found that men were more likely to attribute acute MI to dietary factors, lack of exercise and smoking than were women. A Finnish study showed that men more often thought that risk behaviours and ‘internal’ factors such as mental attitudes were responsible, while women believed more strongly in poor medical care and chance [12]. Sex differences are likely to vary markedly as a function of the effectiveness of risk factor identification, and secondary prevention may be pursued more vigorously in men [25], leading to more frequent causal attributions to lifestyle factors.
There was a consistent SES difference in causal attributions, with better educated patients being more likely to believe that heredity and genetic factors contributed to their heart disease. This was almost certainly an effect of the greater medical knowledge of higher SES patients, since the difference was not due to a stronger family history in more educated groups. SES, however, was not related to beliefs about the role of smoking, physical activity, diet and other lifestyle factors. Even when analyses were restricted to individuals with a particular risk factor (e.g. current smoking, sedentary lifestyle), no differences by SES in associated causal attributions were present. This indicates that education about lifestyle and secondary prevention should be pursued actively with patients whatever their educational background and SES.
Data were collected in this study within a few days of acute cardiac admission. It might be argued that the findings reflect short-term beliefs rather than more stable attributions concerning the causes of heart disease [26]. Causal attributions, however, evidently remain stable over at least 6 months after admission [4], suggesting that beliefs assessed soon after admission may be important in the longer term. The selection process for the larger study in which these data were collected led to a higher proportion of clinical presentations of ACS as STEMI compared with non-STEMI/unstable angina than has been described in recent surveys [27], and this may have influenced the pattern of causal attributions observed. The number of female patients was relatively small, and there were insufficient non-white admissions to carry out a systematic comparison of ethnic groups. Nevertheless, our results challenge the notion that causal attributions for CHD are stereotypic reinterpretations of a patient's experience. Rather, causal beliefs may be strongly influenced by knowledge of risk profiles and medical communication about causes. Such factors may be harnessed to stimulate more effective lifestyle change and secondary prevention in patients with acute CHD [28].
Footnotes
Acknowledgements
The authors are grateful to Dr Philip Strike and Dr Susan Edwards for their contributions to data collection.