
Abstract
Objective
Our aim was to evaluate whether vitamin E (500IU) slowed the progression of carotid atherosclerosis in a population of chronic smokers over 4 years as measured by ultrasound determination of carotid intima-media thickness (IMT) and systemic arterial compliance (SAC).
Methods
The Melbourne Atherosclerosis Vitamin E Trial (MAVET) was a randomized, double-blind, placebo-controlled trial in which 409 male and female smokers aged 55 years and over were randomized to receive 500IU per day of natural vitamin E or placebo. The primary endpoint was progression of carotid atherosclerosis determined by intima-media thickness of the right common carotid artery. Secondary outcomes were change in systemic arterial compliance and low-density lipoprotein (LDL) oxidative susceptibility over time.
Results
The mean increase in intima-media thickness over time in the vitamin E group was 0.0041 mm/year faster than placebo (95% confidence interval −0.0021 to 0.0102 mm/year, P=0.20). Similarly, a non-significant difference between vitamin E and placebo was found for rate of change in systemic arterial compliance (P=0.11). Vitamin E supplementation did, however, significantly reduce LDL oxidative susceptibility (P>0.001).
Conclusion
Vitamin E supplementation is ineffective in reducing the progression of carotid atherosclerosis as measured by intima-media thickness in chronic smokers. This finding extends our knowledge of lack of effectiveness of vitamin E supplementation in populations with high oxidant stress. Eur J Cardiovasc Prev Rehabil 13:341-347 © 2006 The European Society of Cardiology
Introduction
A large body of experimental and epidemiological evidence suggests that antioxidant compounds inhibit atherosclerosis by reducing the formation of oxidized low-density lipoprotein (LDL) [1, 2]. The majority of trials of antioxidant compounds (mainly vitamin E) in unselected populations using intima-media thickness (IMT) as a measure of atheroma progression [3–7] and cardiovascular disease (CVD) endpoints have, however, been negative [8–10].
Evidence of enhanced oxidative stress has been found in smokers [11], diabetic [12] and dialysed patients [13]. It has been speculated that antioxidants might be more effective in these settings [14]. This theory has received support from recent studies of vitamin E conducted with patients with high oxidant stress which have reported a slowing of atheroma development [15] or a reduction in cardiovascular endpoints [16–18]. There are limited data on the impact of high doses of vitamin E in the most common state of enhanced oxidation, namely chronic cigarette smoking.
This study was conducted to reappraise the effect of high dose antioxidant supplementation for the progression of atheroma, as measured by carotid IMT and large vessel compliance, in the setting of chronic cigarette smoking.
Methods
The Melbourne Atherosclerosis Vitamin E Trial (MA-VET) trial was a randomized, double-blind, placebo-controlled study examining the effect of vitamin E (500IU/day) in cigarette smokers over a 4-year period of follow-up. The primary outcome measure was the rate of progression of carotid IMT. Changes in systemic arterial compliance (SAC) were also determined. The protocol was approved by the Standing Committee on Ethics in Research Involving Humans at Monash University.
Subjects
The study was conducted in a Caucasian population drawn from metropolitan Melbourne, Australia. Recruitment took place from November 1994 to November 1995. Follow-up was completed in November 1999.
Participants were recruited from the general community following an advertising campaign in the local media. For inclusion into the study, participants had to be 55 years of age or over and regularly smoke over five cigarettes per day. Exclusion criteria included life-threatening illness, previous carotid artery surgery or existing carotid stenosis warranting surgery, known sensitivity or intolerance to vitamin E, treatment with anticoagulant drugs, myocardial infarction (MI) or stroke within the previous 6 months or uncontrolled hypertension.
Study protocol
Participants who met initial telephone-screening criteria were invited to attend the study centre where an initial carotid ultrasound examination was performed and eligibility to participate confirmed. After providing written informed consent, each subject completed a questionnaire providing information on medical history, intake of drugs, diet and smoking history. Baseline clinical measurements included sitting blood pressure, pulse rate, weight and height, and a blood sample was taken.
Vitamin E was administered as capsules containing 500 IU of natural vitamin E (d-α tocopherol) in a soybean oil suspension, encapsulated in gelatine (Henkel Australia, New South Wales, Pty Ltd Australia). Placebo capsules also contained soybean oil and were of identical appearance. The randomization schedule, which was kept at a remote site, used an allocation scheme with a random permuted block size of eight. Neither study staff, nor participants were aware of treatment allocation.
Following randomization, participants were telephoned 3-monthly to encourage compliance and to report adverse events. Carotid ultrasound, SAC assessment, capsule compliance and measurement of the clinical and lipid parameters were repeated at 6, 12, 24, 36 and 48 months after entry into the study.
Carotid intima-media thickness
Carotid IMT was measured using a high-resolution ultrasound instrument (Diasonics DRF-400; Diasonics, Santa Clara, California, USA) with a 7.5 MHz mechanical sector transducer (7.5-SPC) as previously described [19]. In brief, three images of each B-mode, taken from anterior, anterolateral, and lateral angles were recorded from a region 1 cm proximal to the origin of the bulb of the right and left common carotid arteries (only the IMT measurements of the right common carotid artery were used for the analysis). Images were analysed using the customized House of Windows software program at completion of the study by a single assistant blinded to both the treatment allocation and visit number, as previously described [19, 20]. The mean IMT represented the mean of 60 successive measurements. Repeatability of the measurements was assessed by repeating the analysis of IMT from 365 subjects within MAVET. The coefficient of variation was 17.3%; the mean difference ± SD was 0.014 ± 0.029 mm; the coefficient of repeatability was 0.0034; and the correlation coefficient was 0.974 [95% confidence interval (CI) 0.969 to 0.979].
Systemic arterial compliance
Systemic arterial compliance was estimated using the area method. The methods are described in detail elsewhere [19, 21, 22]. SAC measurements in our laboratory have also been shown to have good repeatability [23]. Since SAC estimation became available after the study had commenced, only a subset of participants was assessed.
Brachial blood pressure was measured at 5-min intervals throughout the entire clinic visit using a Dinamap recorder (Critikon 1846 SX; Critikon Inc., Tampa, Florida, USA). Central blood pressure was measured using applanation tonometry applied to the right common carotid artery with a non-invasive pressure transducer (Millar Mikro-tip; Millar Instruments Inc., Houston, Texas, USA). Carotid artery pressure waveforms were obtained simultaneously with the brachial artery pressure recordings.
Laboratory measurements
Plasma was measured for blood glucose (random) and lipid profile [total cholesterol, triglyceride and high-density lipoprotein (HDL)] by a commercial assay using an Abbott auto-analyser. LDL oxidative susceptibility was measured on plasma samples from a randomly selected subset of 60 patients on three occasions by determining the length of time before the onset of conjugated diene accumulation (lag phase), as previously described [24].
Statistical analysis
The sample size for the study was based on assuming our placebo group would follow a study of natural progression of IMT [25] which showed an increase of 0.12 ± 0.2 mm in IMT over 2 years. For 80% power to detect a 30% difference between placebo and treatment groups in the rate of change of IMT over 4 years, a total of 250 participants were required (two-sided significance level of 0.05). Allowing for a combined drop out and mortality rate totalling approximately 44%, 360 participants were required, 180 in each arm.
IMT was compared between groups using all IMT data from participants to their last follow-up visit. We fitted a linear regression model with an interaction between study groups and time (assuming a linear change in IMT over time) using generalized estimating equations with an exchangeable working correlation matrix for repeated IMT measurements within a person over time [26]. The sensitivity of these results to missing data was explored by firstly fitting a logistic regression model to a binary indicator of whether a participant missed more than one IMT measurement over the six visits with covariates of sex, age, study group, hypertension, diabetes, baseline IMT, cholesterol and systolic blood pressure. The linear regression model of IMT was then expanded to include adjustment for variables that were predictive of participants’ propensity to have missing data, and a random patient intercept and slope [27]. Secondly a pattern-mixture model [28] was fitted to the IMT measurements in which the study groups were compared at each visit using only the patients that dropped out before the subsequent visit and the comparisons were averaged using weights related to the proportion of dropouts.
The analysis of SAC was restricted to the initial 2 years of the study because of increasing rates of missing data at later visits and because it was hypothesized that any treatment effect should have manifested itself in this period. The analysis proceeded as for IMT with the additional testing of an indicator variable for the baseline visit to account for an observed rise in mean SAC for both study groups between baseline and the second visit. Baseline, 1 and 4-year HDL was analysed as per IMT but with adjustment for sex (which was related to propensity for missing HDL measurements and strongly related to mean HDL). All analyses were performed on an intention to treat basis using Stata version 7 (Stata Corp., College Station, Texas, USA).
Results
Of the 919 telephone-prescreened individuals, 421 were invited for a clinic-screening visit and 409 were randomized (204 placebo and 205 vitamin E; Fig. 1). The mean age of the participants was 64 years and 56.6% were women. All were regular smokers, with a mean self-reported intake of 20 cigarettes daily (range 5-80 cigarettes/day).
Overall, a comparison of baseline variables between the two groups showed there was close similarity in most characteristics (Table 1). The vitamin E group, however, had greater body mass index (BMI) and were more likely to use calcium channel blockers while the placebo group were more likely to use angiotensin-converting enzyme (ACE) inhibitors. The mean pack-years of smoking was similar in the two groups.
Compliance was determined by counting capsules in the returned medication bottles. Overall 75.0 and 73.6% of the vitamin E and placebo groups, respectively, consumed 80% or more of their capsules. After 4 years of follow-up, 83.4% of the vitamin E group and 79.4% of the placebo group remained on their assigned medication. There were more deaths in the placebo group than with vitamin E (Fig. 1) but the difference was not statistically significant (X 2 test, P = 0.10).
Intima-media thickness assessment
Of the 409 subjects recruited for the study, 317 (78%) had IMT measurements at all six visits. The IMT analysis (Table 2, Fig. 2) includes these individuals and a further 14 (3%) patients for whom IMT was measured on five visits inclusive of the 4-year visit.
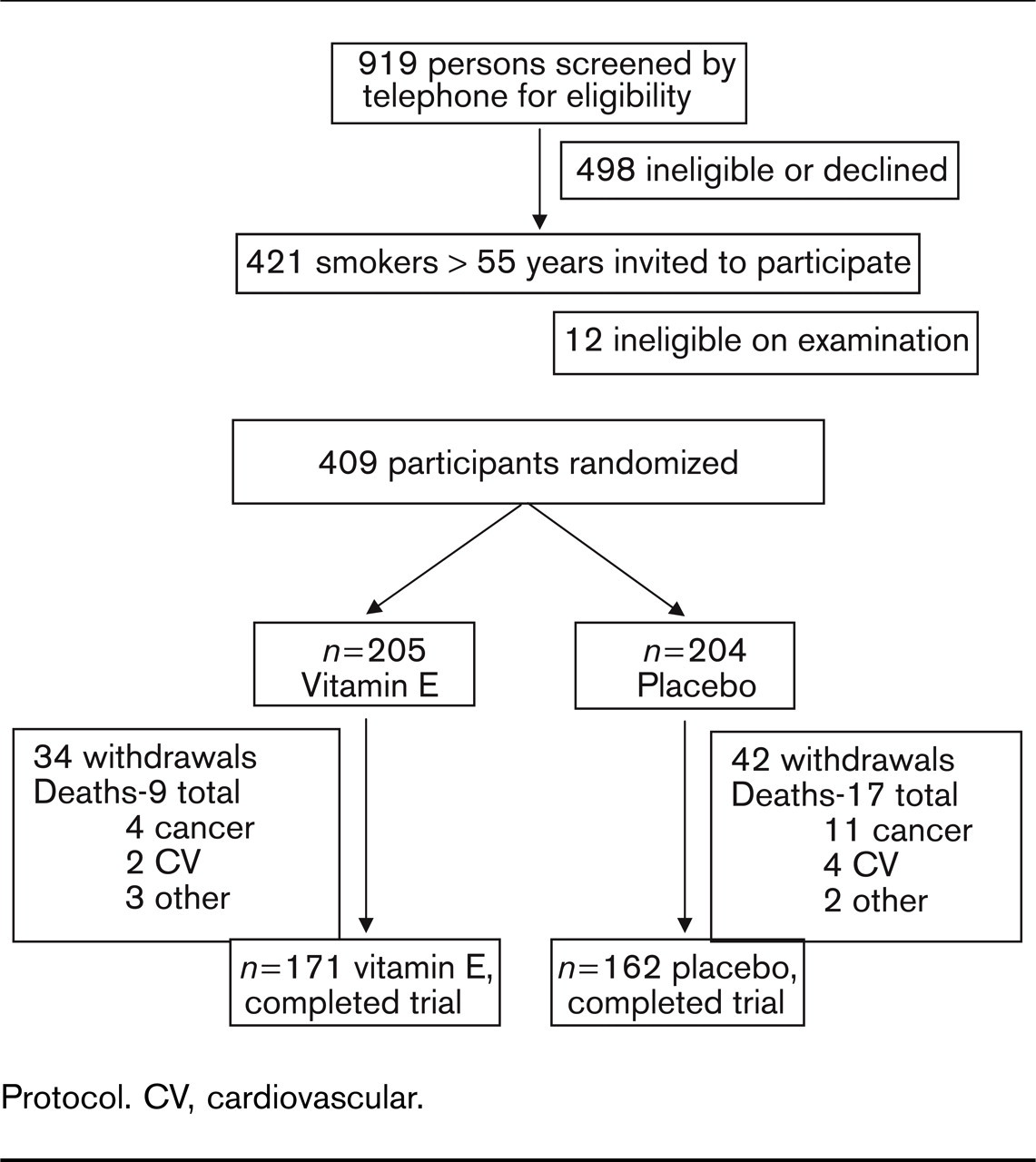
Protocol. CV, cardiovascular.
The rates of progression of IMT in the two groups are shown in Table 2. The average rate of change in placebo was −0.0005 mm/year while that in the vitamin E group was 0.0035 mm/year; that is the rate of progression was 0.0041 mm/year less in the placebo group (Table 2). The findings were similar when all subjects were included and the analysis was adjusted for sex and presence of diabetes or hypertension, which were associated with increasing likelihood of missing data (estimate of difference between groups in IMT change over time 0.0042 mm/ year; 95% CI −0.0102 to 0.0017 mm/year; P=0.16). The conclusion was unchanged when analysing the data using the pattern-mixture approach and when both sexes were considered separately.
Comparison of baseline characteristics between two groups of participants
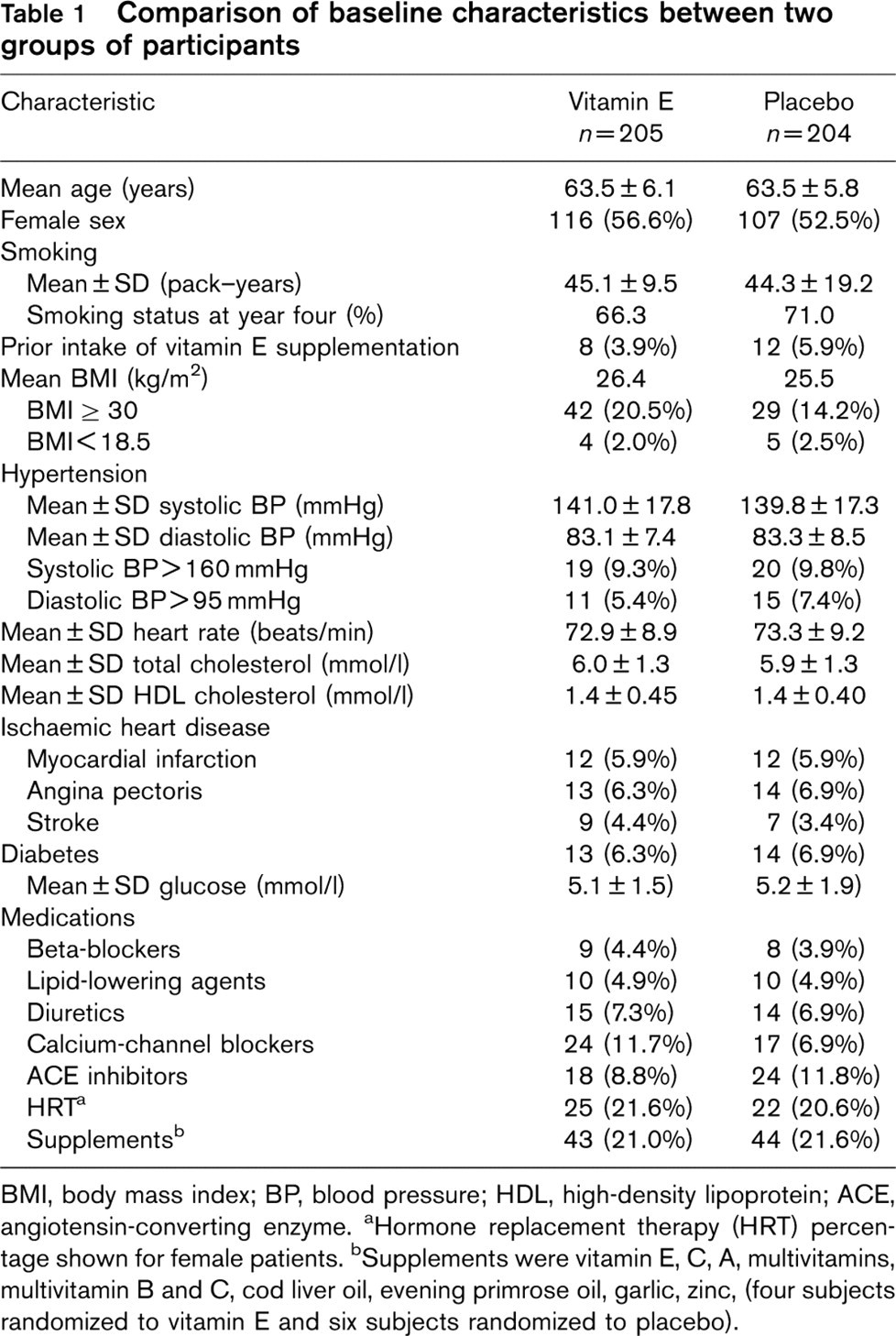
BMI, body mass index; BP, blood pressure; HDL, high-density lipoprotein; ACE, angiotensin-converting enzyme. aHormone replacement therapy (HRT) percentage shown for female patients. bSupplements were vitamin E, C, A, multivitamins, multivitamin B and C, cod liver oil, evening primrose oil, garlic, zinc, (four subjects randomized to vitamin E and six subjects randomized to placebo).
Systemic arterial compliance assessment
One hundred and fifty-three participants had SAC measured at baseline. Of these, 107 (70%) had SAC measured at each of the initial four visits and these participants were more likely than the other 46 (30%) to have been women, of younger age and not have had hypertension. There is no evidence of difference in SAC measurement between the vitamin E group and the placebo (after adjustment for sex, age and presence of hypertension) with the observed rate of change of SAC being marginally greater for placebo than for vitamin E (Table 3). The comparison between groups of change in SAC over time was unaffected by the inclusion of a factor to account for the upwards shift in SAC from baseline to visit two, although this factor was in itself of borderline significance (mean shift = 0.042 units/mmHg; 95% CI, −0.008 to 0.092 units/mmHg; P=0.10). The findings were similar when analysing only those participants with SAC measured at all four visits (estimate of difference between groups in SAC change over time=0.026 units/mmHg per year; 95% CI −0.007 to 0.059 units/mmHg per year; P = 0.12).
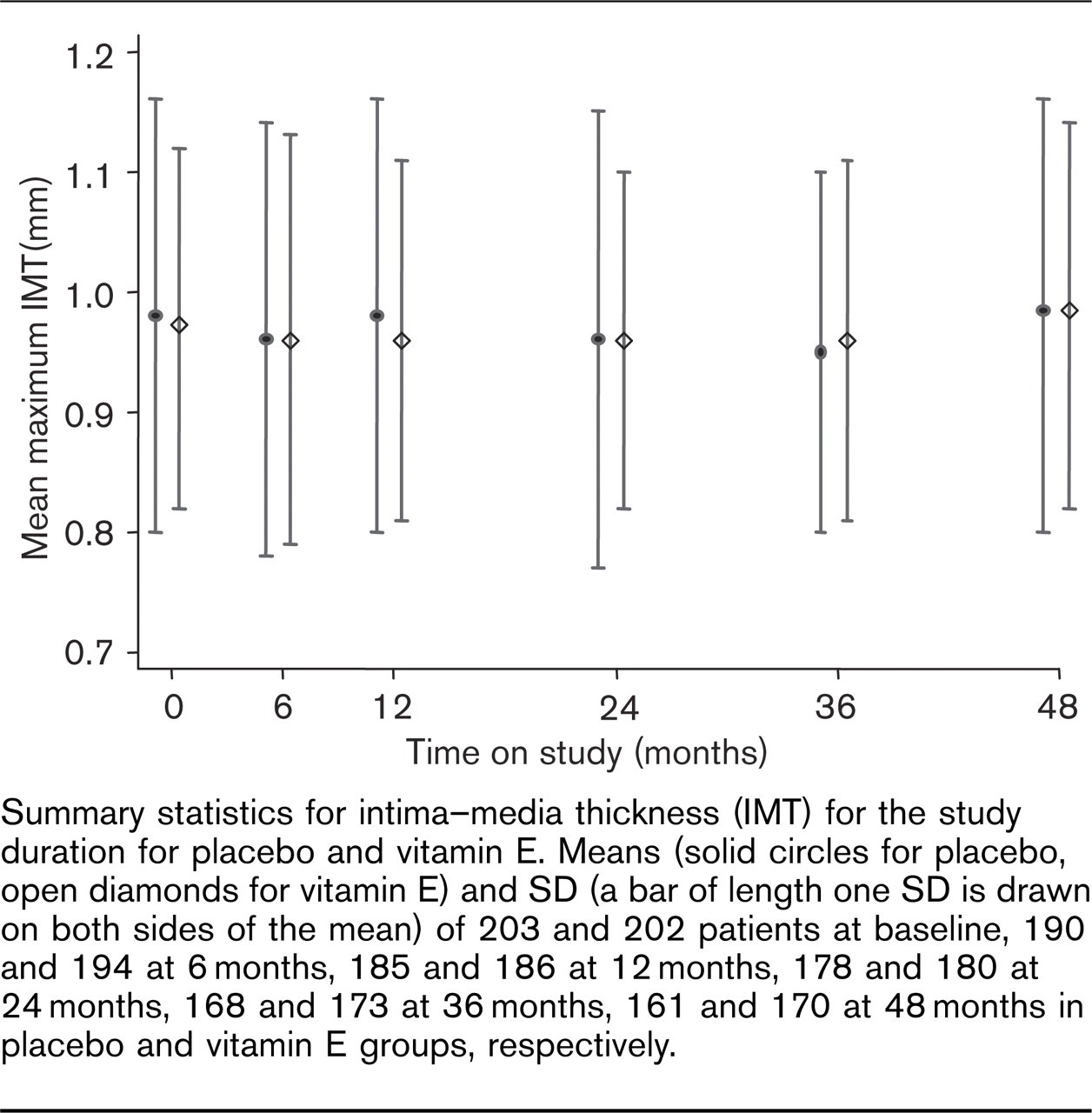
Summary statistics for intima-media thickness (IMT) for the study duration for placebo and vitamin E. Means (solid circles for placebo, open diamonds for vitamin E) and SD (a bar of length one SD is drawn on both sides of the mean) of 203 and 202 patients at baseline, 190 and 194 at 6 months, 185 and 186 at 12 months, 178 and 180 at 24 months, 168 and 173 at 36 months, 161 and 170 at 48 months in placebo and vitamin E groups, respectively.
Analysis of change in intima-media thickness over 4 years after randomization to either vitamin E or placebo
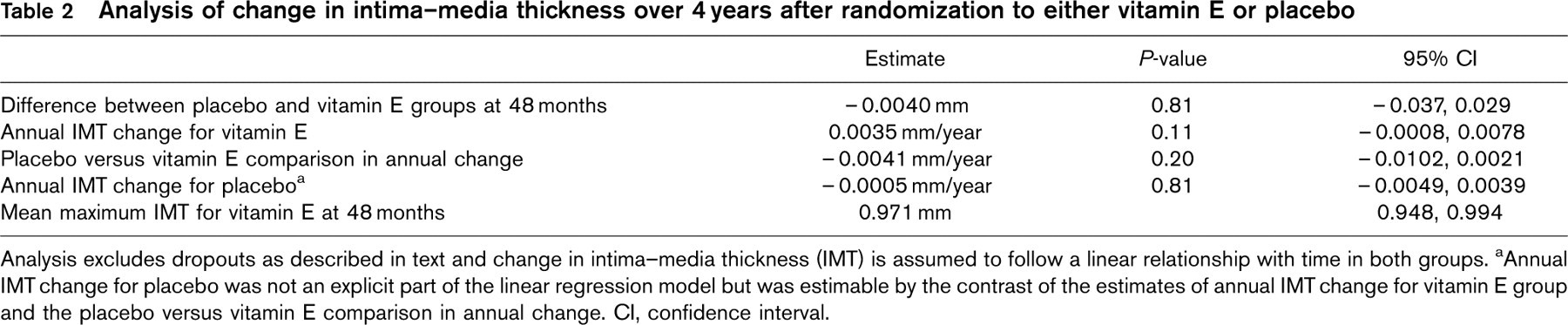
Analysis excludes dropouts as described in text and change in intima-media thickness (IMT) is assumed to follow a linear relationship with time in both groups. aAnnual IMT change for placebo was not an explicit part of the linear regression model but was estimable by the contrast of the estimates of annual IMT change for vitamin E group and the placebo versus vitamin E comparison in annual change. CI, confidence interval.
Analysis of change in systemic arterial compliance over 2 years after randomization to either vitamin E or placebo
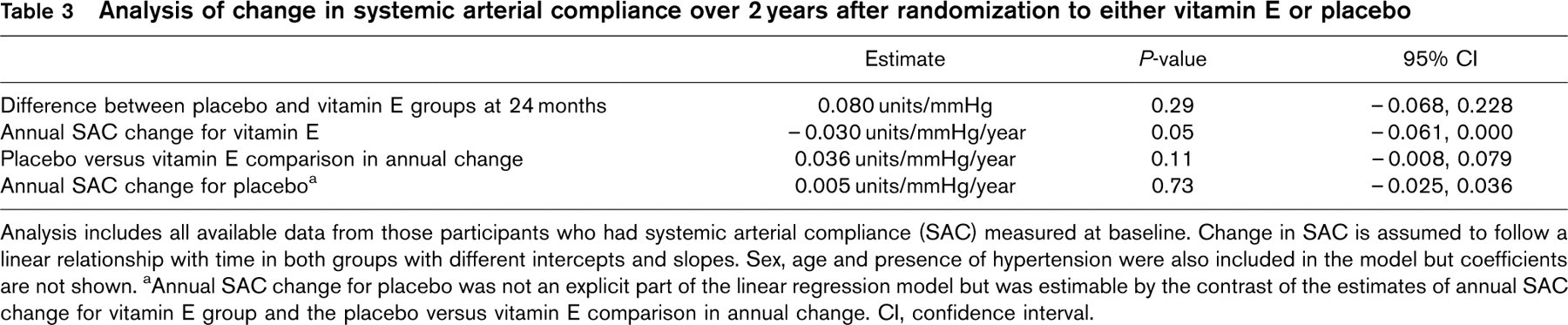
Analysis includes all available data from those participants who had systemic arterial compliance (SAC) measured at baseline. Change in SAC is assumed to follow a linear relationship with time in both groups with different intercepts and slopes. Sex, age and presence of hypertension were also included in the model but coefficients are not shown. aAnnual SAC change for placebo was not an explicit part of the linear regression model but was estimable by the contrast of the estimates of annual SAC change for vitamin E group and the placebo versus vitamin E comparison in annual change. CI, confidence interval.
Low-density lipoprotein oxidizability
LDL susceptibility to oxidation (lag time) was measured on 63 randomly chosen participants at baseline, 6 and 12 months. The vitamin E group had significantly longer lag times when compared with the placebo group. The estimated difference between groups in mean lag time change over time was 1.6 h (95% CI 1.1 to 2.2). As for the whole sample, however, there was no evidence of a difference in the rate of change of IMT change between vitamin E and placebo based on this subset of participants.
High-density lipoprotein
Mean HDL was 1.37 mmol/l in both groups at baseline (Table 1). There was a significant drop in mean HDL from baseline to 4 years in the vitamin E group (−0.08 mmol/l per year; 95% CI −0.12-0.04 mmol/l per year; P >0.001) that was similar to the drop seen in the placebo group (test of interaction, P = 0.54).
Discussion
In the MAVET cohort of continuing cigarette smokers, high dose vitamin E supplementation did not slow the progression of atherosclerosis, as measured by IMT, over a 4-year period. In fact, the rate of progression of IMT in the vitamin E-treated group was slightly greater than in the placebo group although the difference was not statistically significant. Similarly, the decline in vascular compliance was slightly greater in the vitamin E-treated group, but also did not reach statistical significant. Vitamin E supplementation did reduce LDL oxidative susceptibility as measured by lag time in a subset of participants. These results demonstrate that in a strongly pro-oxidant setting vitamin E did not slow the progress of artherosclerosis.
The study was powered to detect a 30% difference in the rate of IMT progression between the two groups, and the 95% CI for the difference in the rates of IMT progression (−0.0102 to 0.0021 mm/year) suggests that all but small effects (either protective or harmful respectively) of vitamin E can be excluded.
Although the baseline characteristics of patients in the two groups were very similar, there were minor differences in BMI, the use of calcium channel blockers and ACE inhibitor medication. As these differences were not large and did not favour either group, it is likely that they did not bias the results of this study. Also a difference in proportions of deaths in the two groups was observed but this finding was consistent with chance.
Clinical trial data of vitamin E
Two previous trials of vitamin E or vitamin E containing combinations in unselected populations found that this agent does not reduce the progression of IMT [4, 5]. Similarly, the majority of large-scale trials with assessment of CVD endpoints found no evidence that vitamin E reduces the incidence of MI or stroke or prolongs survival. In the Heart Protection Study (HPS) [8], a trial of 20 536 men and women, vitamin E supplementation with a mixture of antioxidants did not significantly reduce all-cause mortality, or incidence of CVD. The Heart Outcomes Protection Evaluation (HOPE) trial [10] randomized 9541 men and women at high risk of future CVD events to receive vitamin E or ramipril using a 2 × 2 factorial design. After 4-5 years of treatment, there was no reduction in any CVD endpoints. Using a similar design, the Primary Prevention Project (PPP) [9] study evaluated the effects of aspirin and vitamin E for the prevention of CVD in 4495 men and women at high risk of CVD and reported no difference in CVD endpoints between vitamin E and placebo. In the Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto Miocardio (GISSI) study [29], supplementation with vitamin E and n-3 polyunsaturated fatty acids in the survivors of acute MI showed that while fish oil supplementation reduced cardiovascular risk, vitamin E produced no benefit. More recently, several meta-analyses of the effect of vitamin E on CVD concluded that vitamin E was neither protective nor beneficial for CVD [30–32].
Contrary to these findings, there is evidence from trials with clinical and surrogate endpoints to suggest that vitamin E may have patient-specific benefits. The Antioxidant Supplementation in Atherosclerosis Prevention study [3] showed that the progression of atherosclerosis in the common carotid artery by IMT over 6 years was reduced in the subgroup of hypercholesterolemic, male smokers who took vitamins C and E. The observed effect was paralleled by a reduction in lipid peroxidation in men. In another study of 42 men, supplementation with vitamin E and C retarded early progression of transplant-associated coronary arteriosclerosis [15]. In addition, several randomized controlled trials measuring CVD clinical endpoints have also reported some positive findings, two of which were in settings where oxidative stress may be increased. The Secondary Prevention with Antioxidant of Cardiovascular Disease in End-Stage Renal Disease study showed that supplementation with high doses of vitamin E reduced composite CVD endpoints in 196 haemodialysis patients with pre-existing CVD. The Alpha-Tocopherol, Beta-Carotene Cancer Prevention study [33, 34] was designed to examine the health effects of synthetic vitamin intake of vitamin E and β-carotene in the prevention of lung cancer in male smokers. In a subgroup analysis, it was found that among men with previous MI, low-dose vitamin E was associated with a reduction in subsequent risk of non-fatal MI and an increased risk of fatal MI.
The present study has examined the possibility that vitamin E may be efficacious in patients with enhanced lipid oxidation induced by chronic cigarette smoking [1, 2]. There are several reasons why vitamin E may have been ineffective, despite the favourable clinical setting and the demonstrated pharmacological effect. The ability of a substance to be an antioxidant is determined by its ability to reduce LDL oxidative susceptibility in vitro. The increase in lag time (reduction in LDL susceptibility) in vitamin E-supplemented individuals in this study suggests that vitamin E acted as an antioxidant in plasma. As other authors have suggested, it is possible that this action is confined to the plasma, and does not reflect an inhibition of oxidation in the vessel wall [4]. There is evidence to suggest that for vitamin E to have an antioxidant effect, it requires the presence of other reducing agents [6] such as vitamin C and glutathione, acting as co-antioxidants [4]. The concentration of the co-regulatory molecules may not be as abundant in the artery wall as they are in plasma. When these agents are not in great supply, as is commonly the case in smokers [35], vitamin E may act as a pro-oxidant. The mechanism by which this might happen is unclear, but it has been suggested that high doses of vitamin E may displace other antioxidants, by disrupting the balance of antioxidants, thereby increasing the susceptibility to oxidative damage. Supporting this theory, a recent meta-analysis showed that moderate doses of vitamin E (>150 IU/day) were associated with increased risk of all-cause mortality [36]. In our study, the vitamin E group had slightly faster progression of atherosclerosis than the placebo group, although the observed difference was not statistically significant.
The failure of vitamin E supplementation to reduce clinical and surrogate CVD outcomes in other studies has been attributed to a vitamin E-induced blunting of HDL [6]. It is unlikely, however, that this occurred in this study as vitamin E had no effect on HDL levels throughout the study.
Conclusion
Vitamin E had no effect on the progression of carotid atherosclerosis despite a high dose being used in a setting where oxidation is strongly enhanced. The absence of an effect in this environment, coupled with the lack of effect in a variety of other settings, suggests that this compound is ineffective in slowing the progression of carotid atherosclerosis in humans.
Footnotes
Acknowledgements
We would like to acknowledge Judy Snaddon for data collection and Emma Link for assistance with the literature search and statistical analysis.