
Abstract
Background
This study was performed to determine the blood pressure (BP) percentile curves by height, as well as to assess the prevalence of high BP and its influencing factors among children in the first national survey in this field in Iran.
Design
A multicentre national cross-sectional survey.
Methods
This study was performed in 23 provinces among a representative sample of 21111 students aged 6–18 years.
Results
Age and sex-specific percentile curves of systolic and diastolic BP were obtained by height. A comparison of the values obtained corresponding to the 90th percentiles with the Second Task Force cut-offs showed that the BP values and trends were relatively similar in both studies. The overall prevalence of systolic, diastolic as well as systolic or diastolic hypertension according to the Second Task Force study 95th percentile cut-off points were 4.2, 5.4 and 7.7%, respectively, without a significant sex difference. A history of low birthweight, overweight, taller height, the consumption of solid hydrogenated fat, as well as the frequency of fast food consumption increased the risk of both systolic and diastolic hypertension. Male sex, large waist, and low education of the mother were the risks for systolic hypertension, whereas the risk of diastolic hypertension rose with living in an urban area, attending public school, low physical activity level, having a housewife mother, and a positive family history of obesity, especially in the parents.
Conclusion
Considering the effect of modifiable environmental factors on the childrens' BP, encouraging breast feeding and a healthy lifestyle may have an important effect on public health.
Introduction
Non-communicable diseases are predicted to account for approximately three-quarters of all deaths in the developing world by the year 2020 [1]. In the general population, more than 70% of premature morbidity is estimated to be attributable to tobacco use, obesity, and the undertreatment of hypertension. Although these often preventable diseases emerge during adulthood, their origins could be traced back to early life [2], and by reducing related high-risk behaviours from childhood their incidence may decrease simultaneously [3]. As the treatment and control of hypertension in adulthood does not usually reduce the risk of cardiovascular disease [4], primary prevention efforts should be emphasized; such efforts may have a small, but important, effect on public health.
Ample evidence now supports the concept that the roots of essential hypertension extend back to childhood [5, 6]. A family history that relates to both genetic and environmental factors is also considered important in the development of hypertension [5, 7].
Considering ethnic differences, reference standards and nomograms of blood pressure (BP) for children have been defined in many countries [8–11]. However, similar to many other Asian countries, only a few local studies have been conducted in Iran [12, 13]. Consequently, for the first time in Iran, and to our knowledge in the eastern Mediterranean region (EMR), we performed the present project at national level as the baseline survey of a surveillance system. The system is designed for non-communicable disease-related risk behaviours and risk factors in children and adolescents, and is entitled: Childhood and Adolescence Surveillance and Prevention of Adult Non-communicable Disease, the CASPIAN Study (‘Caspian’ is the name of the world's largest lake, located in northern Iran).
One of the objectives of this project was to determine BP values by age and sex-specific height-adjusted BP percentile curves and elevated BP cut-points, as well as to assess the prevalence of high BP.
Methods
The baseline study was performed in 2003–2004 as a joint collaboration based on a World Health Organization (WHO)/Eastern Mediterranean Region Organization grant and support of the National Ministry of Health and Ministry of Education. This multicentric study was performed in 21 111 school students (96% participation rate), aged 6–18 years, living in urban and rural areas of 23 (out of 28) provinces in Iran. The samples were selected as a representative sample of nearly 16 000 000 Iranian school students (from near 67 000 000 total population of the country) with different ethnicities (Persian 51%, Azeri 24%, Gilaki and Mazandarani 8%, Kurd 7%, Arab 3%, Lur 2%, Baloch 2%, Turkmen 2%, other 1%).
Ethics committees and other relevant national regulatory organizations approved the study. Our team obtained written informed consent from parents and oral assent from students after full explanation of the procedure involved. The project team selected students by multistage random cluster sampling. They stratified schools according to location (urban/rural), and the socio-economic character of the uptake area, taking into consideration the proportion of the different types of schools (public/private) to avoid socio-economic bias.
We prepared our questionnaires in the Farsi language based on the questionnaires of the WHO STEPwise approach to non-communicable diseases (tools version 9.5) and the WHO global school-based student health survey. The validity of their content was affirmed on the basis of observations by a panel of experts, item analysis, and reliability measures were assessed on the basis of a pilot study.
The physical activity pattern was assessed by a scaled questionnaire organized in nine different metabolic equivalent (MET) levels ranging from sleep/rest (0.9 MET) to high-intensity physical activities (> 6 MET) by Aaddahl and Jorgensen [14] for adults. We have previously modified and validated it in Iranian youth; the questionnaire had high test-retest reliability (r = 0.87), and was significantly associated with the International Physical Activity Questionnaire [15] and a 7-day physical activity diary among Iranian youth [16]. For each activity level, the MET value was multiplied by the time spent on that particular level. The MET time from each level was added to the total 24-h MET time, representing the physical activity level on an average weekday. Energy expenditure was estimated by multiplying the total 24-h MET time by the body weight. In the current study, we categorized the physical activity level according to the tertiles computed in the population studied, and scored it from 1 to 3 according to the first to the third tertile.
In addition to the questions about family dietary habits, all subjects completed a food frequency questionnaire that was previously validated among Iranian youth [17]. Food items were grouped into the following categories: carbohydrates (rice, bread, pasta, potato); vegetables (potato and French fries not included); fruits (fresh, dried, juice); dairy products (milk, cheese, yogurt); proteins including both animal type (red meat, poultry, fish, egg) and plant type (beans, soy, nuts); fast foods (pizza, hamburgers, sausages, etc.); and snacks (salty/fat/sweet).
A team consisting of expert healthcare professionals carried out the field examinations by standardized and calibrated instruments. The participants filled out the questionnaires under the supervision of trained nurses. The nurses recorded age and birth date, and measured height and weight twice to ± 0.2cm and to ± 0.2kg, respectively, with subjects being barefoot and lightly dressed; the averages were recorded. Body mass index (BMI) was computed as weight in kilograms divided by the square of height in meters. Waist circumference and hip circumference were measured to the nearest half centimetre, according to the WHO protocol [18].
The nurses measured BP in a calm situation using mercury sphygmomanometers after at least 5 min of rest in the sitting position. The subjects were seated with the heart, cuff, and zero indicator on the manometer at the observer's eye level. All readings were taken in duplicate in the right arm. Appropriate size cuffs were used with a cuff width 40% of the mid-arm circumference, and cuff bladders covering 80–100% of the arm circumference and approximately two-thirds of the length of the upper arm without overlapping. The procedure was explained to the students and the cuff inflated and deflated once, the first BP measured was not used in the analysis of this study. The reading at the first and the fifth Korotkoff phase were taken as the systolic blood pressure (SBP) and diastolic blood pressure (DBP), respectively. The average of the two time measurements was recorded and included in the analysis. Elevated BP was defined as the mean SBP or DBP above the 95th percentile for that age and sex after adjusting for weight and height [9].
The Data and Safety Monitoring Board of the project closely supervised the quality control and quality assurance of the survey at the national level.
The data entry staff entered data for all forms and questionnaires twice and checked for completeness and inconsistencies. The data checking process was conducted at the district and national level for preventing outliers and rechecking of a fraction of entered questionnaires for each operator.
Statistical analysis
After editing, the data were analysed and transferred by the SPSS v13/win software package (SPSS, Inc., Chicago, Illinois, USA). Reference standard curves (smoothed percentiles) were constructed by modelling data in SPSS v13 using a fractional polynomial trend line to smooth the percentile curves.
Prevalence data are expressed as percentages and are compared by using the chi-squared test. The linear regression analysis was performed between SBP and DBP as the dependent variables and other factors were assessed as independent variables. Odds ratios from logistic regression models were employed to evaluate the associations of high SBP and DBP with other factors. The significance level was set at P < 0.05.
Results
The participants were 10858 girls (51.4%) and 10253 boys (48.6%) living in 23 provinces in Iran. The mean (± SD) age of students was 12.2 ± 3.3 years, 84.6% of them were from urban and 15.4% from rural areas, and 90% were from public and 10% from private schools.
Most of the students' fathers worked in the private sector (34.9%) or were employees (31.5%), and most of their mothers (88.9%) were housewives. Most of students' parents were literate. Respectively, 14.7 and 10.1% of students had a history of low (< 2500g) and high (> 4000g) birthweight. Most of the subjects studied were breast fed (71.4%) without using any other kind of milk during the first year of life and their weaning food was homemade (65.9%).
The mean BMI of the subjects studied was 18.53 ± 3.84 kg/m2, without a sex-specific difference. Based on the cut-points of the US Centers for Disease Control and Prevention [19], the prevalence of under-weight, normal weight, at risk of overweight, and over-weight was 13.9, 72.7, 8.82, and 4.5%, respectively.
The most frequent type (73.8%) of fat consumed for food preparation in the students' home was hydrogenated solid fat. Most students (58.4%) consumed breads prepared by white wheat flour, and 19.7% of students declared they never added salt to the table food. Of the subjects studied, respectively, 34.4, 38.9 and 25.1% were included in the first, second and third physical activity tertiles.
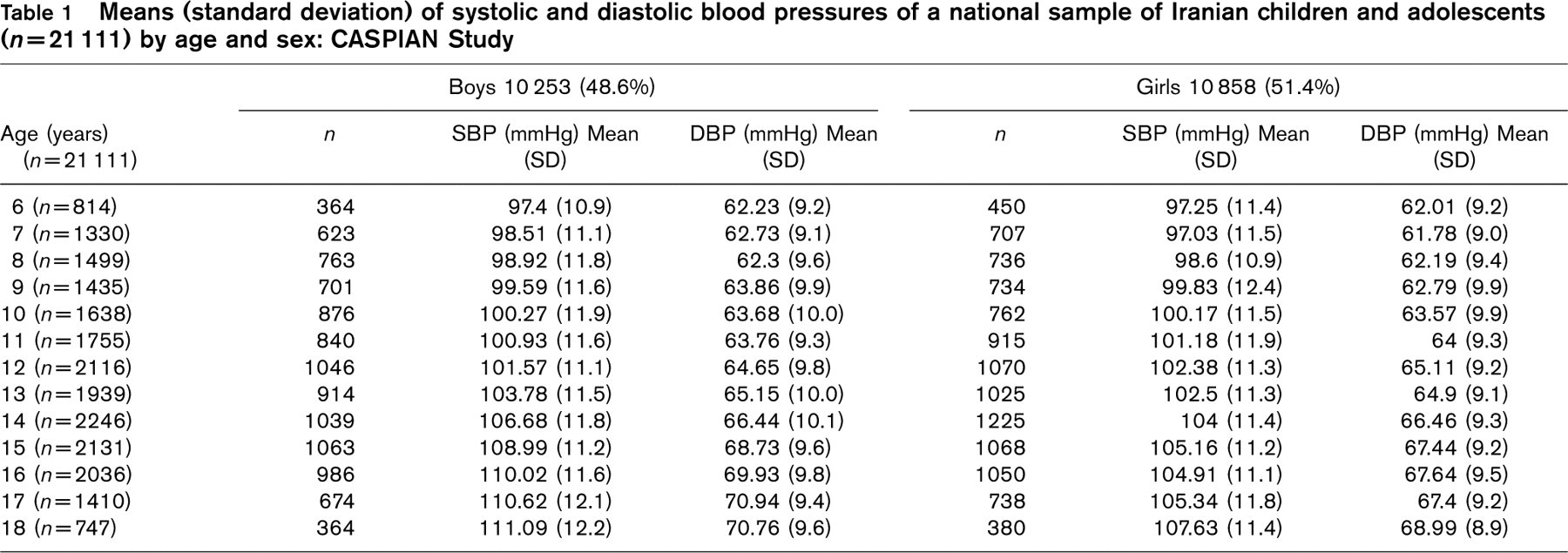
The SBP and DBP means and standard deviations by age and sex are given in Table 1. The age-specific and height-specific percentiles of SBP and DBP for both sexes are presented in Table 2. These figures were used to delineate the smoothed percentile nomogram curves shown in Fig. 1. These curves reveal that BP measurements in both sexes are similar in appearance and trends. SBP and DBP increased gradually and steadily with age in both sexes. The rate of increase in SBP and DBP values accelerated from approximately 12 to 14 years of age in both sexes. The age-specific 90th percentile of SBP and DBP values, which are conventionally considered as cut-off points for elevated BP [2, 9], were compared with corresponding figures mentioned in the Second Task Force study [9], and presented in Fig. 2. Taken as a whole, BP values and trends were relatively similar in these studies.
By the linear regression method, significant associations were observed for SBP with BMI, height, school type, waist circumference, physical activity, and dietary habits, for example, the habit of adding salt to table food and the frequency of consumption of sweets/candies had a direct relationship with SBP, whereas with regard to the frequency of dairy consumption, this association was inversely present. There were also correlations in DBP with the sex, weight, waist circumference, school type, low birthweight, a positive family history of hypertension, as well as current dietary habits, for example, the frequency of consumption of sweets/candies had a direct relationship with DBP, whereas the history of breast feeding during infancy, the consumption of whole-grain bread, and the frequency of vegetable consumption, as well as hip circumference and the mother's education level had an inverse association with DBP (Table 3).
Means (standard deviation) of systolic and diastolic blood pressures of a national sample of Iranian children and adolescents (n = 21111) by age and sex: CASPIAN Study
The age-specific percentiles of systolic and diastolic blood pressures according to sex in a national sample of Iranian children and adolescents (n = 21111): CASPIAN Study

DBP, Diastolic blood pressure; SBP, systolic blood pressure.
Logistic regression analysis revealed that a history of low birthweight, overweight, taller height, the consumption of solid hydrogenated fat, as well as the frequency of fast food consumption can increase the risk of both high SBP and DBP. However, male sex, a large waist, and low education of the mother were the risks for high SBP, whereas the risk of high DBP rose with living in an urban area, attending public school, a low physical activity level, having a housewife mother, and a positive family history of obesity, especially in the parents (Tables 4 and 5).
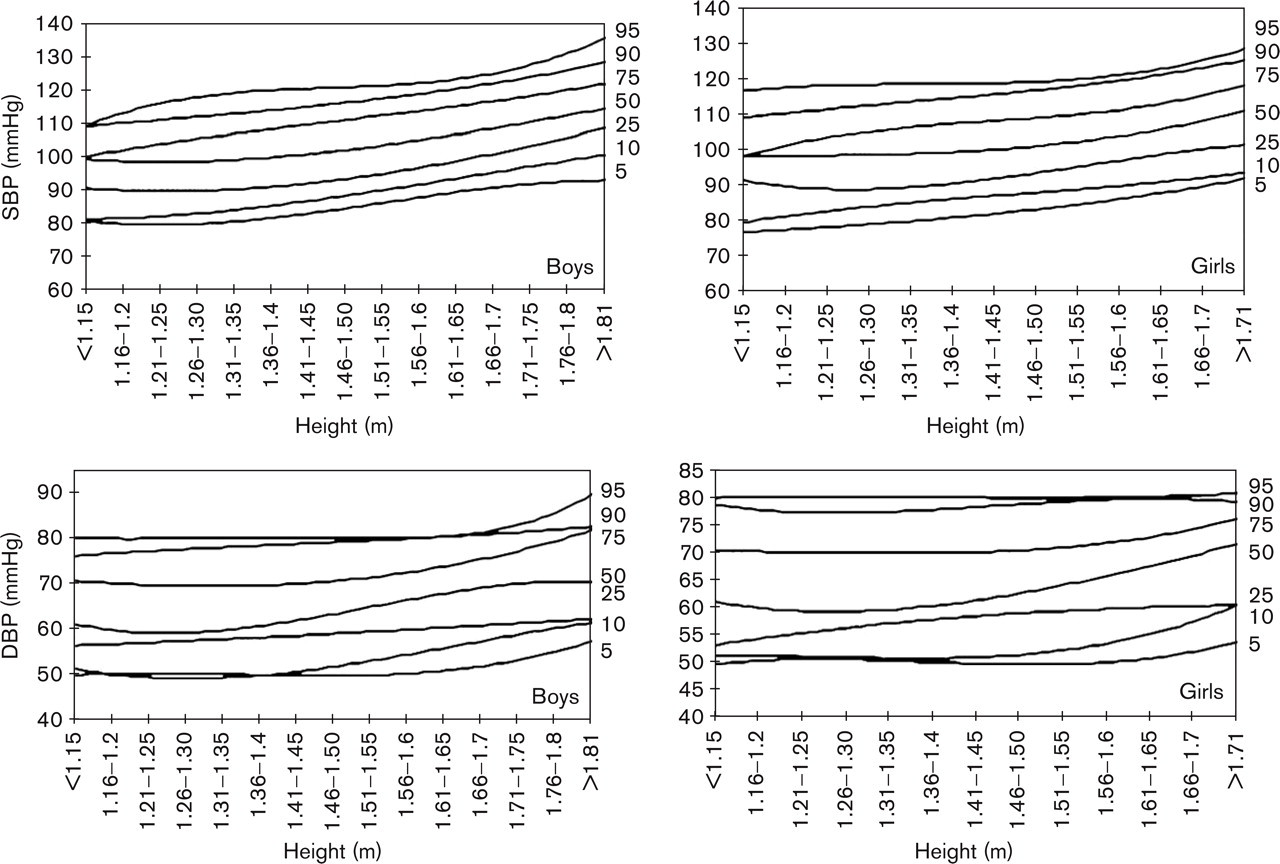
Smoothed percentile nomogram curves of height-specific diastolic blood pressure according to sex in a national sample of Iranian children and adolescents (n = 21111): CASPIAN Study. DBP, Diastolic blood pressure; SBP, systolic blood pressure.
The overall prevalence of high SBP, DBP and SBP or DBP [9] was 4.2, 5.4 and 7.7%, respectively, without a significant sex difference.
Discussion
The findings of the present national study provided for the first time in Iran, and to our knowledge in the EMR, the age and height-specific BP percentile of a large number of representative samples of children and adolescents. Our obtained cut-points for the 90th SBP and DBP were closely similar to that of the Task Force Report on High Blood Pressure in Children and Adolescents [9]. We documented significant influences of environmental factors, including birthweight, a history of breast feeding, a family history of chronic diseases, as well as the current dietary and physical activity habits on BP.
As BP is not distributed similarly in different communities, many countries have already achieved their normal values and cut-off points [8–11], however in Iran, and to our knowledge in Asian countries, only a few similar studies have been conducted.
In the current study, although there was no sex difference in the prevalence of high BP, male sex increased the risk of high SBP. This finding is consistent with studies that have suggested a relationship between male sex and high BP [8, 20], whereas some others did not confirm such a correlation [11, 21].
Height and weight are reported to be correlated with BP [11, 13, 20, 21]. We observed a significant correlation between height and weight with SBP as well as between weight and DBP, for example, taller individuals had a greater likelihood of developing high BP. The more important role of height than weight has also been emphasized in some other studies [9, 20].
In our study, waist circumference correlated with both SBP and DBP, and a large waist size was a risk for high SBP, and hip circumference had a significant inverse correlation with DBP. This finding is in line with some previous studies [22], and indicates that the health hazards of abdominal obesity are not limited to adult life. Consistent with previous works [20, 23], in our study, overweight increased the risk of both high SBP and DBP. An obese family member was the other risk factor for high DBP in our study; this has occasionally been confirmed [24].
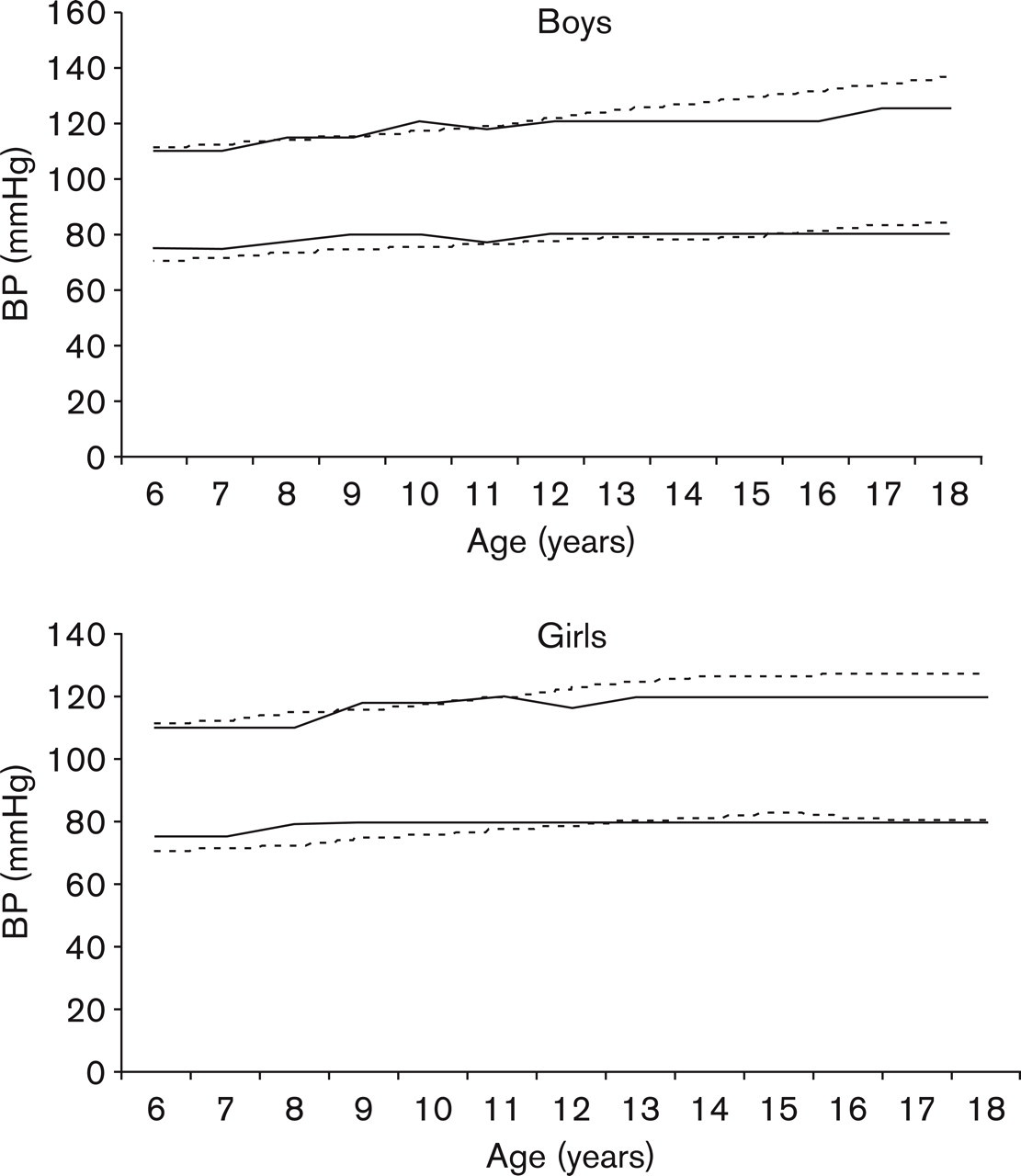
Comparison between age and sex-specific 90th percentile systolic and diastolic blood pressures of Task Force on Blood Pressure and Iranian children and adolescents: CASPIAN Study. — Iranian; — Task Force.
Evidence is growing that factors operating early in life influence BP in childhood and young adulthood [25, 26]. The influence of breastfeeding on BP later in life is controversial; however, our findings were in line with a recent meta-analysis that confirmed the protective role of breast feeding on BP later in life [27].
Consistent with many other studies [28, 29], our findings revealed that a history of low birthweight increased the risk of high BP. However, some other studies did not support such an association [30]. A long-term cohort study should examine the significance of such correlations.
Dietary habits had correlations with BP in our study. Whereas the frequency of the intake of sweets correlated with both SBP and DBP, adding salt to food had a direct correlation, and the frequency of the consumption of dairy products had an inverse correlation with SBP. The frequency of vegetable consumption and the use of whole-grain bread had an inverse correlation with DBP. Furthermore, the use of hydrogenated solid fat and the frequency of fast food consumption raised the probability of high BP. We have previously documented the role of such dietary behaviours, especially the consumption of solid fats rich in saturated and trans fatty acids on dyslipidemia in youth in our community [31]. Fortunately, in addition to increasing the population knowledge about healthy nutrition, many efforts are currently being made by the Ministry of Health to improve the quality of fat produced in the country.
Linear regression analysis of environmental factors a with systolic and diastolic blood pressure of a national sample of Iranian children and adolescents aged 6–18 years (n = 21111): CASPIAN Study
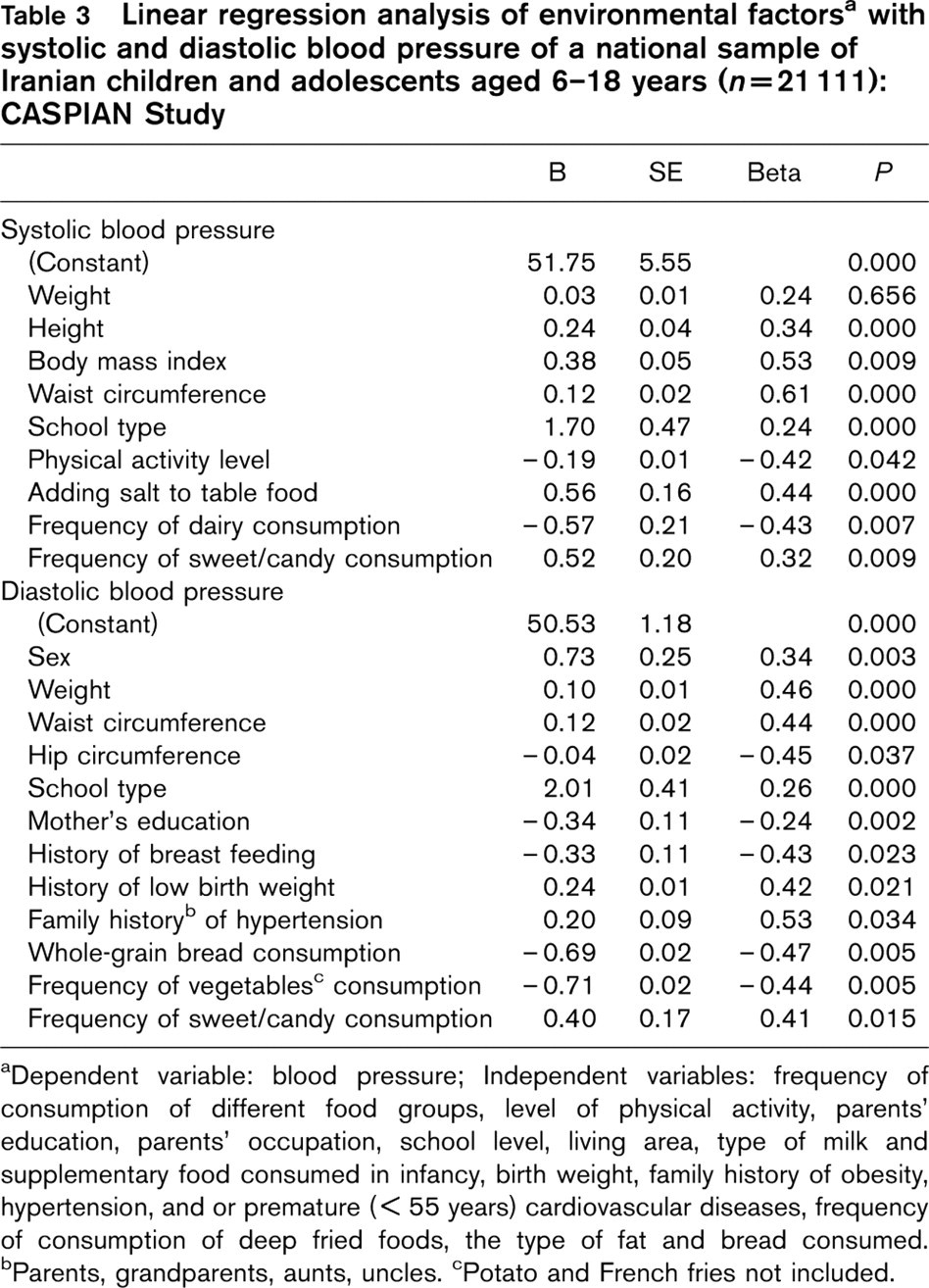
aDependent variable: blood pressure; Independent variables: frequency of consumption of different food groups, level of physical activity, parents' education, parents' occupation, school level, living area, type of milk and supplementary food consumed in infancy, birth weight, family history of obesity, hypertension, and or premature (< 55 years) cardiovascular diseases, frequency of consumption of deep fried foods, the type of fat and bread consumed.
bParents, grandparents, aunts, uncles.
cPotato and French fries not included.
Logistic regression of environmental factors and high systolic blood pressure (≥ 95th percentile) in a national sample of Iranian children and adolescents aged 6–18 years: CASPIAN Study
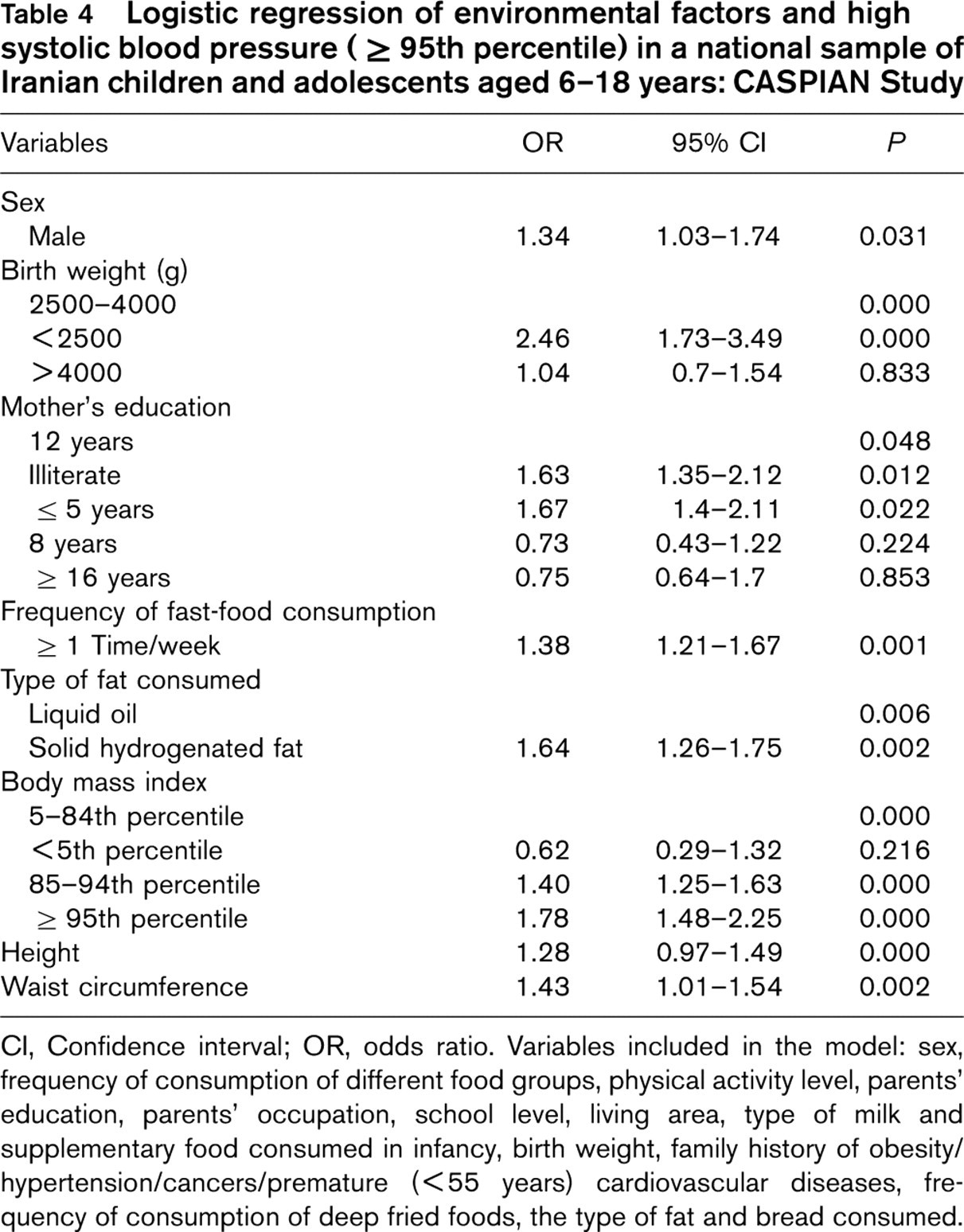
CI, Confidence interval; OR, odds ratio. Variables included in the model: sex, frequency of consumption of different food groups, physical activity level, parents' education, parents' occupation, school level, living area, type of milk and supplementary food consumed in infancy, birth weight, family history of obesity/hypertension/cancers/premature (< 55 years) cardiovascular diseases, frequency of consumption of deep fried foods, the type of fat and bread consumed.
Logistic regression of environmental factors and high diastolic blood pressure (≥ 95th percentile) in a national sample of Iranian children and adolescents aged 6–18 years: CASPIAN Study
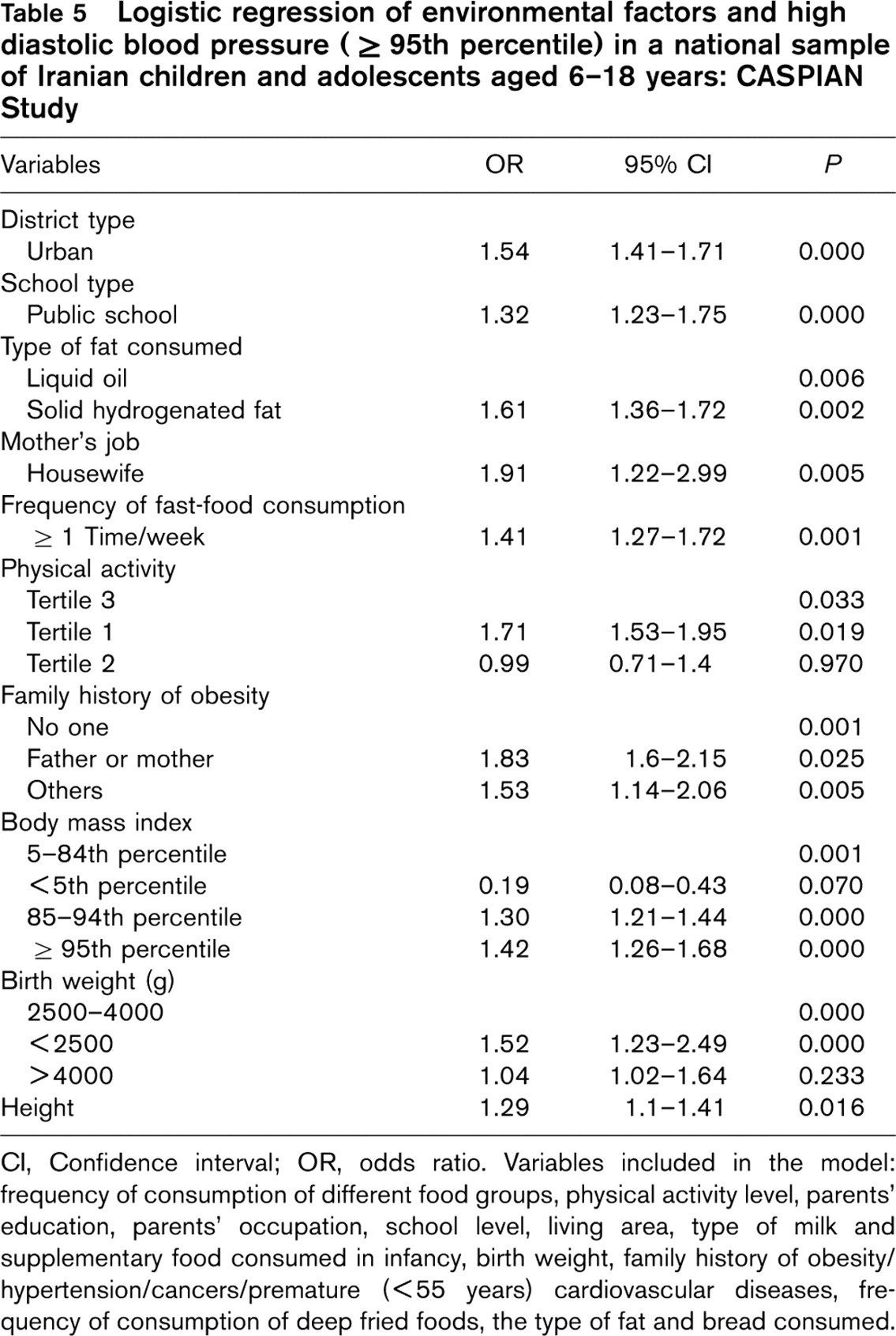
CI, Confidence interval; OR, odds ratio. Variables included in the model: frequency of consumption of different food groups, physical activity level, parents' education, parents' occupation, school level, living area, type of milk and supplementary food consumed in infancy, birth weight, family history of obesity/hypertension/cancers/premature (< 55 years) cardiovascular diseases, frequency of consumption of deep fried foods, the type of fat and bread consumed.
Socio-economic status has frequently been revealed to have a negative association with BP [32]. In our study, attending private school and living in urban areas increased the risk of high BP; such associations should be verified in the next steps of this longitudinal study.
In our study, physical activity correlated with SBP, and lower levels of physical activity increased the risk of high DBP. Other studies have usually shown a protective role for physical activity [33]. Efforts to reduce sedentary behaviours among youth, and encouraging them to increase their physical activity are warranted.
We also found that a positive family history of obesity, especially in parents, correlated with DBP, and a positive family history of hypertension increased the risk of high SBP.
Study limitations
We should acknowledge that certain factors might have influenced the findings of the present study, such as the presumptions on the few missing data and the recall bias for the process of recalling and recording the food intake and the physical activity habits, which requires attention and involves perception. It is therefore possible that some databases are unable to reflect the precise values. Considering the large number of subjects studied, only a quantitative food frequency questionnaire was used in the present survey, and such data cannot provide the precise nutrient and energy intake of the subjects studied. The findings of the analysis of factors associated with BP should be interpreted with caution given the cross-sectional nature of the associations.
Conclusion
Considering the effect of modifiable environmental factors on BP, encouraging breast feeding and healthy dietary habits, such as increasing fibre intake, reducing the consumption of junk foods and saturated fat, as well as increasing physical activity from childhood, may have an important effect on public health, especially in developing countries faced with an epidemic of chronic diseases in the near future.
Footnotes
Acknowledgements
The authors would like to forward their sincere thanks to all the large team working on this project.