
Abstract
Background
Cardiovascular disease mortality remains high in Europe and many patients have elevated risk factors, despite evidence-based targets and treatment guidelines. This survey examined barriers to implementing cardiovascular risk reduction guidelines.
Design
We conducted a semi-structured market research survey of physicians.
Methods
The survey was conducted in six European countries among cardiologists and primary care physicians. In total, 67 questions were used: 35 had multiple choice answers (prompted) and 32 allowed any answer (unprompted). Respondents were working full-time in patient care (≥ 3 years experience) and were in a position to initiate cardiovascular drug treatment.
Results
Of the 220 respondents (155 primary care physicians, 65 cardiologists), most (85%) based assessment of cardiovascular risk on all risk factors, reflecting a global approach to risk, rather than considering risk factors individually. A majority (62%) used subjective assessments for establishing global risk rather than guidelines or risk calculators. The most common unprompted barrier to guideline implementation was patient compliance (36%) and a lack of time (23%), and when prompted, the most important was government health policy (40%). The most common unprompted suggestion for improving implementation were financial opportunities (24%) and clear and easy to use guidelines (23%), while when prompted the most important change required was the development of simpler guidelines (46%).
Conclusions
Although a majority of physicians are aware of the need to look at a combination of cardiovascular disease risk factors, less than half use guidelines or risk calculators to determine total risk. It is recommended that guidelines need to be simpler and easier to use and supplemented with (patient friendly) risk calculators.
Keywords
Introduction
Cardiovascular disease (CVD) is the most common cause of death in developed countries; in 2000, 41% (1.5 million) of all deaths in Europe were attributable to CVD [1]. A large proportion of cardiovascular risk is attributable to modifiable risk factors such as smoking, elevated blood cholesterol, hypertension, obesity, diabetes and the pre-diabetic state [2–4]. In 1997, results from the EUROASPIRE (European Action on Secondary Prevention through Intervention to Reduce Events) I study demonstrated a high prevalence of these risk factors among European patients with coronary heart disease (CHD). Among 4863 such patients, 19% smoked, 25% were obese, 53% had raised blood pressure, 44% had raised plasma cholesterol levels and 18% had diabetes [5].
Reducing levels of modifiable cardiovascular risk factors is a key goal in CVD prevention, and management guidelines are the prime means by which medical societies, institutions, regulatory bodies and national committees aim to achieve this goal. Indeed, guidelines were published in 1998 and 2003 by a consortium of European societies, which aimed to instigate more intensive cardiovascular risk reduction strategies, by emphasizing the effect of global cardiovascular risk over consideration of individual risk factors [4, 6]. The results from the EUROASPIRE II audit, published in 2001, showed that this objective had not been achieved. Although the proportion of patients with elevated cholesterol levels had been reduced (from 86.2 to 58.8%), no other risk factors in these CHD patients had improved since EUROASPIRE I (1997) [7]. The proportion of patients smoking or with hypertension remained unchanged, while the proportion of patients with obesity had substantially increased (25.2 to 32.8%) [7]. Clearly, therefore, the European cardiovascular risk reduction guidelines (and others) had not been fully implemented among the EUROASPIRE countries: Belgium, the Czech Republic, Finland, France, Germany, Greece, Hungary, Ireland, Italy, The Netherlands, Poland, Slovenia, Spain and the UK.
The European Society of Cardiology (ESC) has identified a need to determine the reasons for the generally poor implementation of cardiovascular risk reduction guidelines, and accordingly, through its Cardiovascular Round Table Task Force on Prevention, instigated an international market research survey among European cardiologists and primary care physicians (PCPs). The survey reported here examined which guidelines physicians are using and the manner in which these are being implemented. It also assessed the barriers to guideline implementation, and the practical steps that could be taken to remove these barriers, so as to reduce CVD mortality.
Methods
Survey
The survey was conducted among cardiologists and PCPs; this latter group included general practitioners (GPs) and family doctors. Cardiologists included in this survey were general cardiologists, non-invasive cardiologists and internists specializing in cardiology. The survey was conducted in six European countries (Germany, France, Italy, Spain, the UK and Poland) and consisted of face-to-face in-depth interviews. Prior to the survey, four pilot interviews were conducted in Germany to test the comprehensibility of the master questionnaire. These pilot interviews also assessed the comprehensibility of interviewer instructions as well as the length of the questionnaire, and the suitability of the questions and multiple-choice answers.
A total of 67 questions were used in the in-depth interviews: 35 had defined multiple choice answers (prompted), and 32 allowed the physicians to provide any answer they wished (unprompted). Some of the prompted questions were designed such that respondents had to rate each one of a number of answers on a scale of 1 to 10 (1 being low and 10 being high).
The survey was blinded in two ways: respondents were not made aware of the sponsor, and each completed questionnaire was coded to ensure anonymity. The sequence of questions was designed so that, as far as possible, respondents would be unaware of the precise focus of the study when answering critical questions. A large number of interviewers were used (on average, one interviewer for every 10 respondents) to minimize the impact of any bias that might have been inadvertently introduced by any individual interviewer. All of the interviewers were experienced both medically, and in conducting this type of survey. The questionnaire was translated into local languages to optimize data collection. Completed questionnaires were re-translated into English prior to analysis. All data were collated and analysed centrally by a market research company. Completed questionnaires were reviewed for completeness, relevance and comprehensibility immediately after each interview, and then re-reviewed centrally.z
Selection of participants
Major metropolitan areas within the target countries were selected. Potential respondents were identified from local sources listing medical practitioners (e.g. telephone directories and medical associations). Respondents initially deemed suitable were asked to answer a screening questionnaire to ensure that they met the necessary criteria. Specifically, respondents were required to be under 60 years of age, working full-time in patient care (at least 6 h per day) and to have at least 3 years of professional experience. In addition, they were required to be in a position of responsibility for initiating cardiovascular drug treatment, but could not be employed as a cardiovascular consultant for the pharmaceutical industry, or be participating in any cardiovascular clinical trials. PCPs were required to be seeing and treating patients in different disease areas covering at least four different therapeutic indications. Only respondents meeting these criteria took part in the survey. Data on physicians not qualifying for inclusion in the survey were not recorded.
Results
Survey size
A total of 220 respondents (155 PCPs, 65 cardiologists) were identified as being suitable from the screening questionnaire, and in-depth interviews were conducted accordingly (Table 1).
Respondents characteristics
The length of medical experience was similar between respondents from different countries (Table 1). Differences in healthcare systems between countries were evident, with the place of work of the respondents varying considerably (Table 1).
Respondents were asked to indicate the number of CHD patients they see or treat per week, and the number of patients seen or treated per week at risk of a cardiovascular event (Table 1). On average a PCP saw 23 patients with CHD and 38 patients at risk of a cardiac event per week, whereas a cardiologist saw 52 CHD patients and 62 at risk patients a week.
Assessment of cardiovascular risk
The respondents identified patients at risk of CHD by examining the following risk factors: hypertension (mentioned by 52%), smoking, patient history, diabetes, dislipidaemia (around 40% each), followed by obesity, and family history (30% each). The majority of respondents (85%) based their assessment on a combination of a number of the risk factors mentioned above rather than on single individual risk factor, with the overall percentage being similar among cardiologists and PCPs. Notable exceptions were Germany and Spain, where fewer cardiologists, 44 and 67%, respectively, based their assessment on all the risk factors (compared with 100% of cardiologists in Poland, France and the UK).
The methodology that respondents used to assess total individual cardiovascular risk was examined as well (Fig. 1). A subjective (focusing on combining the synergistic effects of individual risk factors based on personal experience) assessment of risk factors was the most common method used (overall mean 62% of respondents). In contrast were Spain and the UK, in which the majority of respondents stated that they used specific guidelines/risk calculators when assessing total risk. Cardiologists were more likely than PCPs to use a subjective assessment of CV risk: 72 versus 58%, respectively (data not shown).
Guideline usage and interpretation
Usage of the different types of guideline among respondents from the different countries is shown in Table 2: respondents were able to indicate that they used more than one type or set of guidelines. Across all countries apart from Spain, the most commonly used guidelines were national cardiology guidelines. The use of scoring systems/scales (e.g. the Framingham Scale) varied widely, as did the use of national metabolic disorder guidelines (e.g. those produced by the British Hyperlipidemia Society). Some of the least used guidelines were those from the World Health Organization (WHO) and ESC (Table 2), which may reflect the fact that many national guidelines are derived from the ESC and WHO recommendations. A large proportion of respondents from some countries used no guidelines at all, in fact, 40% of those questioned from Germany and France, gave this response. In general, there was a positive correlation between guideline awareness and usage (data not shown).
The respondents were asked to recall the key findings or suggestions for each set of guidelines that they were aware of. The most common answers for national cardiology guidelines were classification of patients/risk evaluation (42%), control of dyslipidaemia (34%), blood sugar control (18%) and control of blood pressure (16%). For management or scoring systems that were recalled, the most common answers were control of blood pressure (51%), control of dyslipidaemia (26%), classification of patients/risk evaluation (20%) and stop/reduce smoking (15%). Cardiologists generally recalled the key findings/suggestions of national cardiology guidelines more often than PCPs; for example 52 versus 36%, respectively, recalled classification of patients/risk evaluation as a key finding/suggestion (data not shown).
Respondent characteristics
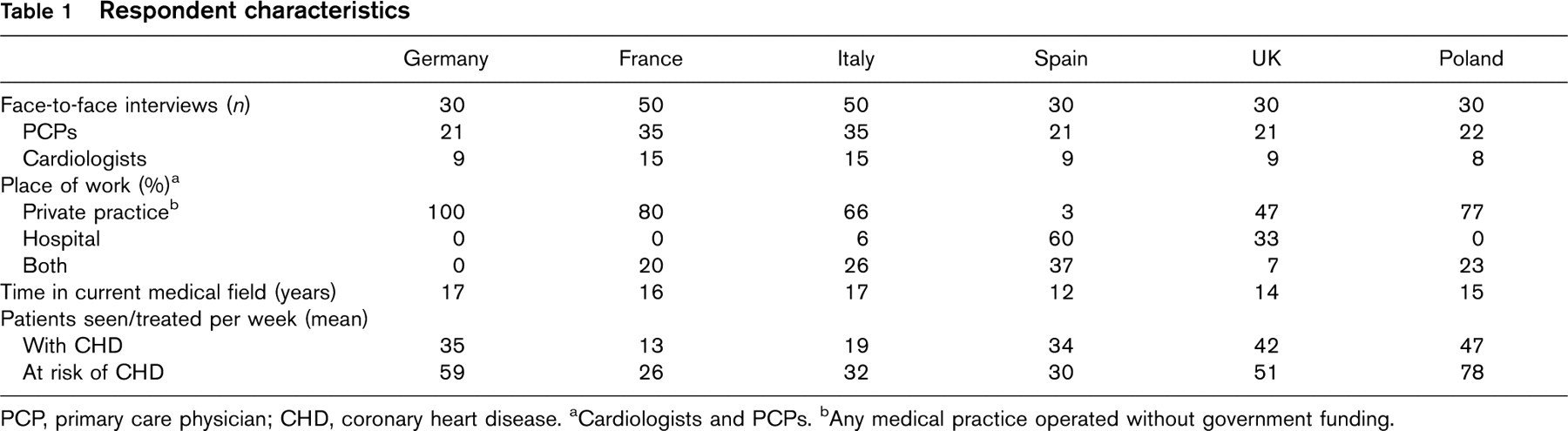
PCP, primary care physician; CHD, coronary heart disease.
aCardiologists and PCPs.
bAny medical practice operated without government funding.
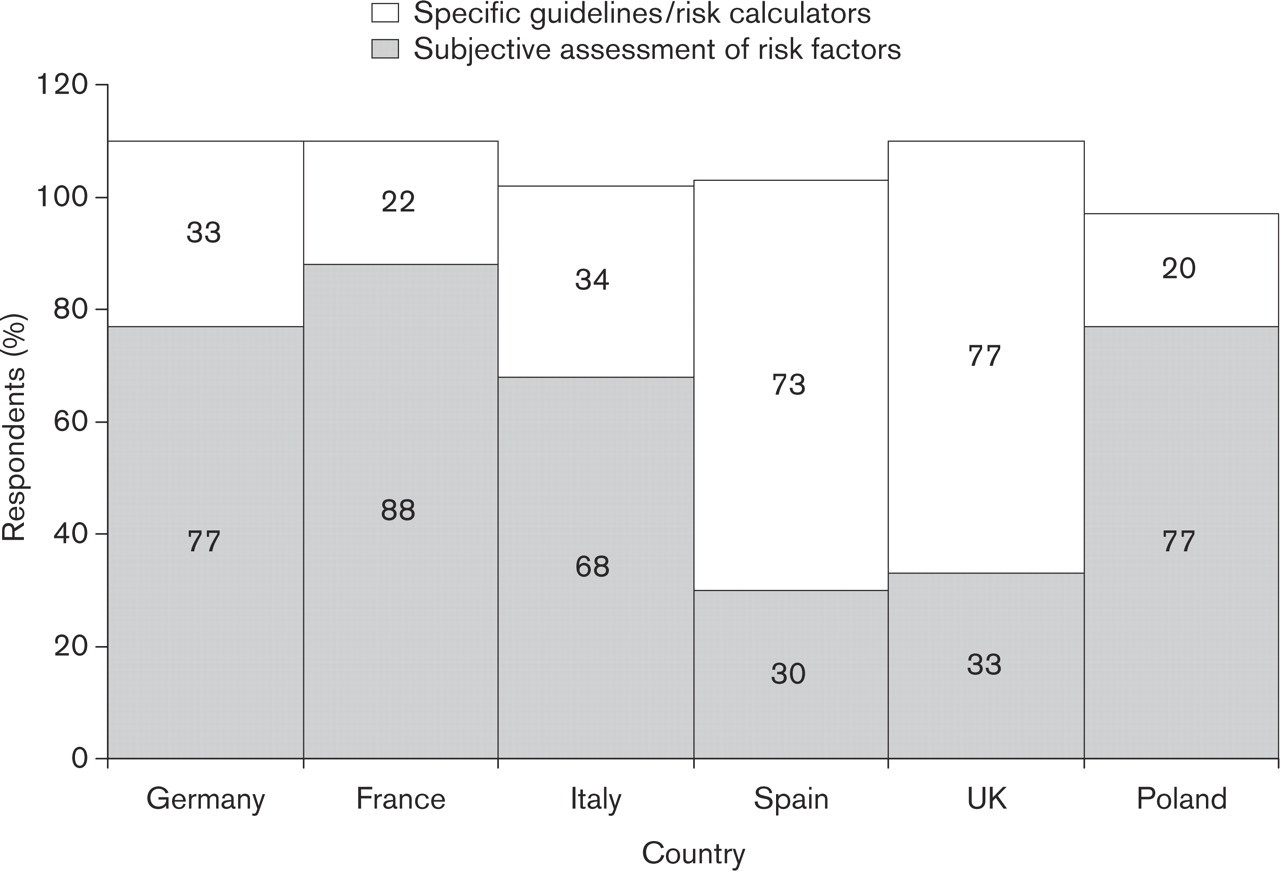
The preferred method for total cardiovascular risk assessment among respondents. Respondents could choose more than one response.
The types of guidelines used by respondents from different countries
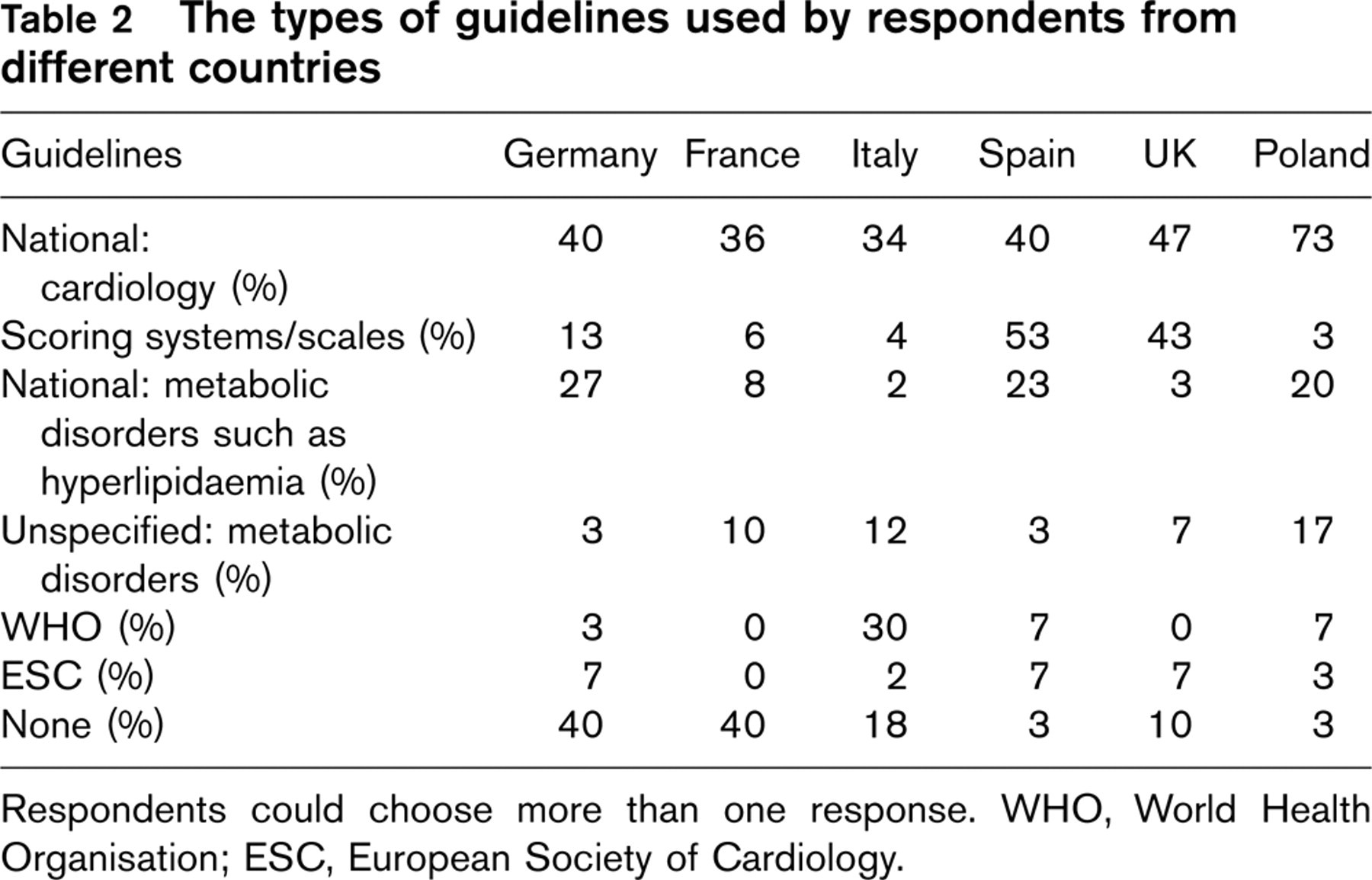
Respondents could choose more than one response. WHO, World Health Organisation; ESC, European Society of Cardiology.
The manner in which respondents apply guidelines was also determined (Table 3). The use of guidelines as specified was a relatively uncommon practice among the different countries, although Spain was a notable exception, with 43% of physicians stating that they used guidelines as specified. The use of guidelines combined with personal experience was a common practice in some countries (guideline usage tempered with respect to personal experience), although the variation in responses was great, ranging from 10% of those from Germany, to 70% of those from Italy. A significant proportion of respondents employed a set of guidelines but with pre-specified modifications, ranging from 10% in Italy to 33% in Germany.
The manner in which guidelines were applied by respondents from different countries
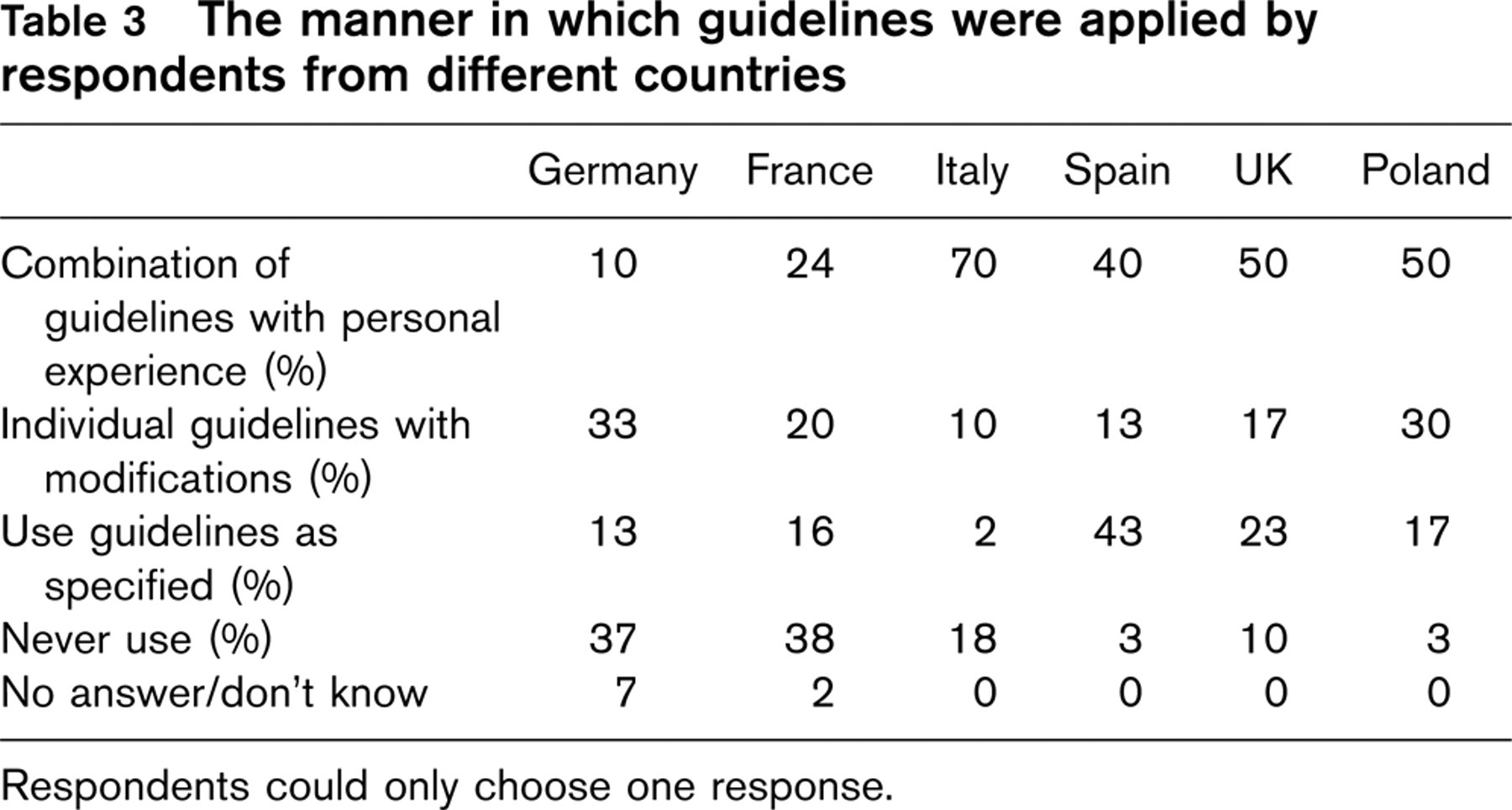
Respondents could only choose one response.
The barriers to guideline implementation
When asked open-ended questions as to the greatest barrier to the implementation of cardiovascular guidelines (Fig. 2a), 36% cited a lack of patient compliance, and this barrier was greatest among PCPs from the UK and Poland (67 and 59% respectively). Other barriers commonly cited were time (23% of respondents), the fact that guidelines are too theoretical and individual treatment is required (21% of respondents; 44% UK cardiologists), financial aspects (20%; 44% German cardiologists; 67% Poland) and overcomplicated guidelines were cited by 15% of respondents (44% UK cardiologists).
Respondents were asked to rate a series of barriers on their importance (on a scale of 1 for unimportant to 10 for very important) in reducing guideline implementation (Fig. 2b). The fact that government health strategy does not help in prevention was rated as an important barrier (rated 8–10) by 40% of the respondents (ranging from 77% in Poland, to 16% in France). Little or no financial reward for prevention was also an important barrier (36% of respondents; 93% Poland), budget constraints were rated as important by 30% (60% Germany, 8% France, 10% Spain, 67% Poland) and a lack of time for patients by 27% (70% Poland). The fact that hospital policies do not help, and a lack of patient motivation were the most important barriers among 23 and 20%, respectively.
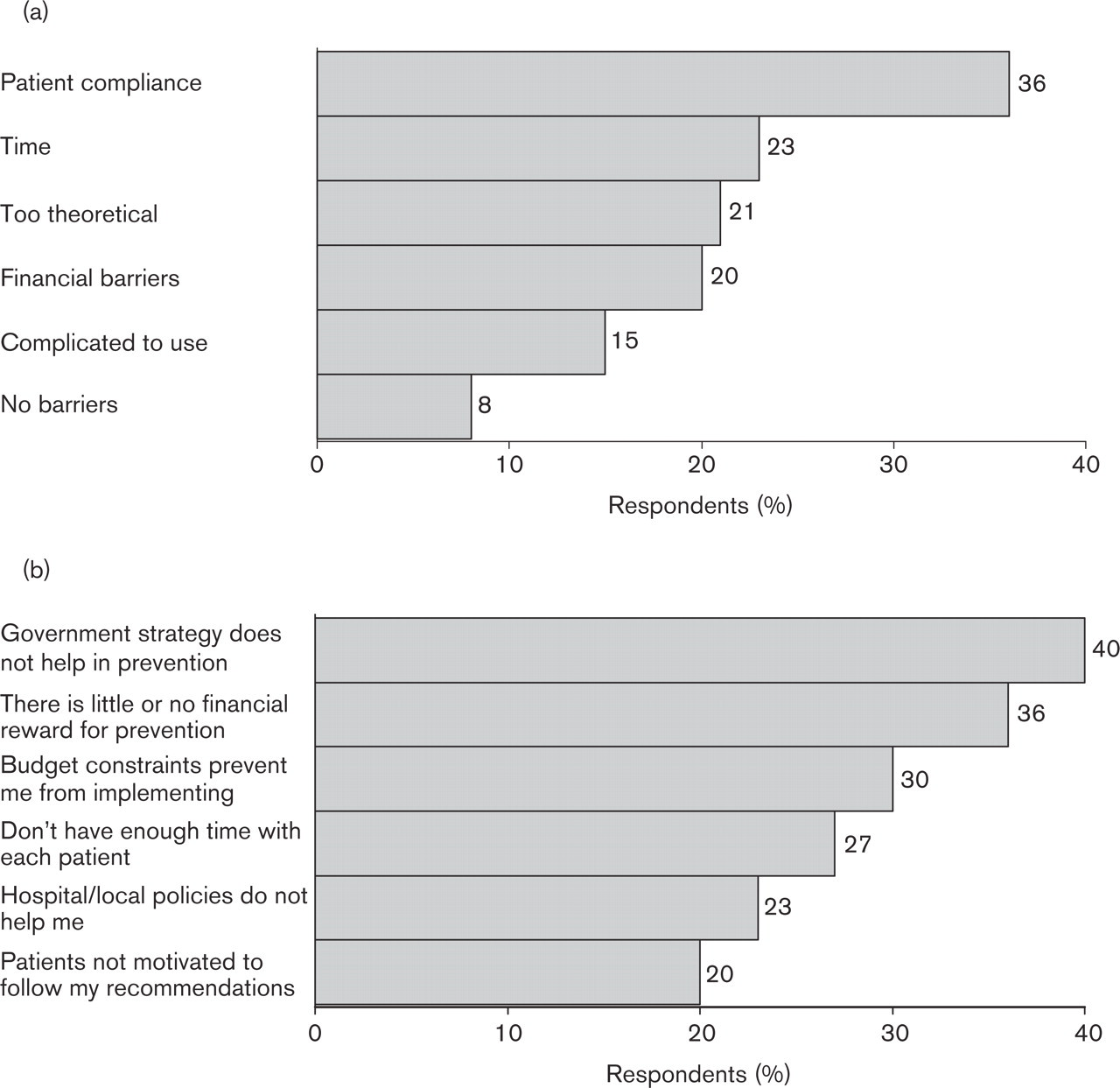
(a) Barriers suggested by respondents as preventing the implementation of cardiovascular risk reduction guidelines. (b) Barriers rated by respondents as being important in preventing implementation.
Practical means of improving guideline implementation
Respondents were asked to provide suggestions (unprompted) for practical means by which guideline implementation could be made easier. The top four suggestions were financial opportunities (24%), clear and easy to use guidelines (23%), more time for every patient (22%) and patient information (22%). Other suggestions were more attention to lifestyle, greater awareness/written information on guidelines, better co-operation between healthcare professionals and easier access to guidelines (approximately 10% of respondents for each response).
Respondents were also asked to rate practical suggestions according to how much of an impact they would have in making prevention easier (on a scale of 1, would not make it easier at all, to 10, would make it a lot easier). The practical suggestions rated as being the most important in making prevention easier (rated 8–10) revolved around providing simpler (rated by 46% of respondents), shorter (45%) guidelines, and increasing the number of nursing (46%) or medical (46%) staff trained in prevention. The implementation of shared care programmes between GPs and consultants (44%) and the use of regular updates and workshops were rated as most important by 44 and 41% of respondents, respectively. Physicians also placed importance on the wider availability of paper-based risk charts and guidelines (37%), the use of different forms of risk calculators (37%) and computer-based risk charts, either with (29%) or without (32%) interactive features.
Discussion
This survey shows that most physicians (85%) base their assessment of cardiovascular risk on all the well established risk factors. A majority of interviewed participants used subjective ways (62%) of assessing combined effects of risk factors and 48% used specific guidelines or risk calculators. The most commonly stated barrier to the implementation of cardiovascular risk reduction guidelines was patient compliance (36%), and the barrier rated as being important by most respondents was government health policy (40%). The most common suggestion for improving implementation was financial opportunities (24%), and the most important way to make prevention easier was simpler guidelines (46%).
Survey limitations
A number of measures were used to reduce bias in the respondents' answers: the respondents were not made aware of the study's sponsor and the sequence of questions designed to reduce respondent intuition as to the precise purpose of the survey. A large number of interviewers were used to reduce any interviewer bias in recording responses. In conducting this survey, the master questionnaire was translated from English into the local language and the responses translated back into English for data analysis. While every effort was made to ensure the comprehension of questions, and the fidelity of data, there exists the possibility that some variation in the interpretation of questions by respondents could have occurred. There could also have been a loss of data fidelity during the translation of answers into English.
As with similar studies, the qualitative nature of much of the data means that it is not amenable to detailed statistical analysis. The sample comprised a large experienced group of physicians, however, and therefore the results bear some considerable weight when deciding upon future tactics to improve implementation of cardiovascular risk reduction guidelines.
Major findings
An important and encouraging observation from this survey is that the majority of physicians are aware of the need to follow a comprehensive or ‘global’ approach to cardiovascular risk assessment and management. Indeed, 85% of respondents stated that they considered all risk factors in making management decisions, and furthermore, many respondents stated that this was based on an appreciation of the cumulative, synergistic effect of cardiovascular risk factors, necessitating a global approach to cardiovascular risk reduction. Nevertheless, although they are aware of the need to follow this approach, in practice the majority of physicians (62%) revert to a subjective assessment of combined cardiovascular risk, rather than using the more objective risk assessment systems recommended by guidelines such as those of the Joint European Task Force [4]. Such a practice would most likely involve placing emphasis on individual cardiovascular risk factors rather than considering all of the risk factors in conjunction (total risk or global approach). Spain and the UK are unusual in this respect in that, compared with other countries, most physicians use specific guidelines/risk calculators in assessing total cardiovascular risk.
The guidelines used by respondents varied considerably, with most favouring their national cardiology guidelines, and most respondents saying that they used their chosen guidelines combined with personal experience. Few respondents stated that they used the WHO or ESC guidelines, which may reflect the fact that national guidelines are frequently derived from these sources. A significant proportion of respondents do not use any guidelines at all when assessing cardiovascular risk.
When physicians were asked what barriers they faced to the implementation of guidelines, the most common answer was a lack of patient compliance (36%). This is not surprising, as compliance is well known to be a major problem in cardiovascular prevention, for example where compliance with antihypertensive medication is concerned [8]. A lack of time, and the fact that guidelines are too theoretical to facilitate individual treatment, were also mentioned as barriers, along with financial constraints and the fact that guidelines are too complex. When physicians were asked to suggest practical means to improve guideline implementation and cardiovascular prevention, the availability of simpler shorter guidelines and the availability of risk calculators in different formats featured highly in their responses. It therefore appears that the most readily rectifiable barrier to implementation is the lack of simple, easy to use and practically viable guidelines.
The less readily rectifiable barriers to guideline implementation and cardiovascular risk prevention generally reflected a lack of resources, with many physicians stating financial aspects, time constraints, and a need for more nursing staff and medical colleagues trained in prevention. Political aspects also featured as barriers to guideline implementation, with the fact that government health strategy does not help in prevention being rated as the most important barrier.
Comparability with other surveys
The findings from the present survey relate to and amplify the results of other published surveys, including for example, the REACT (Reassessing European Attitudes about Cardiovascular Treatment) survey, which examined the attitudes to, and the implementation of CHD and lipid treatment guidelines among 754 European PCPs (France, Germany, Italy, Sweden, and the UK) [9]. In common with the results presented here, key barriers identified were a lack of time (38%), prescription costs (30%) and patient compliance (17%). Suggested means of improvement were better education for physician (29%) and patient (25%), promoting, publicizing, or increasing guideline availability (23%) and producing simpler (17%) and clearer (12%) guidelines. The results also reflected a lack of time to spend with each patient and the feeling that patients did not listen or understand anyway. In addition, a recent study in Italy investigated the approach of PCPs to the diagnosis of hypertension [10]. This study showed that the majority of PCPs managed hypertension according to a simple blood pressure-based approach, rather than considering a global approach incorporating all of the cardiovascular risk factors.
Future perspectives
Clearly, issues of resource finance or policy will depend upon the government health strategy of each individual country. Medical societies, however, have a role to play in improving guideline clarity, adaptability and ease of use. Indeed, the latest version of the ESC guidelines have been designed to be used as a framework to promote the development of national guidelines that reflect the political, economic, social and medical circumstances in different European countries [4, 11]. They should therefore complement the preference of physicians for using their national cardiology guidelines. At the centre of the most recent European guidelines is a new chart for assessing total cardiovascular risk based on the SCORE (Systematic Coronary Risk Evaluation) system [12], and incorporating data from a large data set of European studies. In its present form, SCORE predicts 10-year risk of CVD death; developments to allow prediction of total CVD events are anticipated. To improve ease of use, the SCORE risk chart is also available on the internet as an interactive version (HeartScore) [5].
The ESC has invested considerable resource in aiding the reduction of cardiovascular risk in Europe. Although current recommendations exist in full text, summary and pocket form, the present survey suggests that even simpler versions and more widespread dissemination would be helpful. Furthermore, the role of the cardiology profession in lobbying for more physician time for prevention, and appropriate reimbursement, has probably been underestimated.