
Abstract
Background
Dairy consumption may be associated with a small but worthwhile reduction in cardiovascular disease risk, but results from epidemiological studies are inconsistent. The aim of the present study was to evaluate the association between dairy consumption and the prevalence of a first, non-fatal event of an acute coronary syndrome, in a Greek sample. Design Seven hundred male and 148 female patients with first event of an acute coronary syndrome and 1078 population-based controls, age and sex matched, were randomly selected.
Methods
Detailed information regarding their medical records, alcohol intake, physical activity and smoking habits was recorded. Nutritional habits were evaluated with a semi-quantitative food-frequency questionnaire. Multiple logistic regression analysis estimated the odds ratio of having acute coronary syndrome by level of dairy intake, after taking into account the effect of several confounders.
Results
An inverse relationship was observed between dairy products consumption and odds of having acute coronary syndrome. One portion increase in weekly dairy products intake was associated with 12% lower likelihood of having acute coronary syndrome, after controlling for various potential confounders (P<0.001). Cut-off analysis showed that 7.4 portions per week are the optimal consumption that benefits people from having acute coronary syndrome.
Conclusions
Dairy consumption seems to offer significant protection against coronary heart disease, irrespective of various clinical, lifestyle and other characteristics of the participants.
Introduction
Dairy products and especially milk have been associated as potential promoters of cardiovascular disease (CVD) because they are sources of cholesterol and saturated fatty acids [1, 2]. A considerable part of the saturated fatty acids, especially in milk fat, however, is short-chain fatty acids and the long-chain stearic acid, which do not adversely affect cholesterol levels [3]. Milk intake is probably positively related to blood lipid levels [4, 5], but the effect shown in many studies is either trivial or absent [6]. In fact, in some studies a milk supplement led to a decrease in blood lipids [7, 8], suggesting that milk and milk products may contain antiatherogenic bioactive substances to negate the effects of saturated fatty acids and cholesterol.
According to a systematic search and overview of 10 prospective cohort studies and two retrospective case–control studies, in which incident vascular disease events were related to estimates of milk intake at baseline, there is no convincing evidence that milk is harmful and it suggests that milk drinking may be associated with a small but worthwhile reduction in heart disease and stroke risk [9]. Additionally, Al-Delaimy et al. [10] found no appreciable association between dietary or supplemental calcium intake and risk of ischemic heart disease in men, but Umesawa et al. [11] showed lower mortality risks from total stroke with increased intake of dietary calcium in Japanese men and women.
Moreover, several epidemiological studies also linked dairy consumption or dietary calcium intake with reduced body weight [12–14], lower blood pressure and reduced risk of hypertension [15–17], type 2 diabetes [18] and prevalence of the metabolic syndrome [19], as well as with reduced coagulopathy [20], all factors that favour the promotion of CVD.
Hence, although there are several mechanisms which suggest a beneficial effect of dairy products on CVD risk, results from epidemiological studies are inconsistent. The aim of the present study was to evaluate the association between dairy consumption and the prevalence of a first, non-fatal event of an acute coronary syndrome (ACS) [myocardial infarction (MI) or unstable angina], in a Greek sample.
Methods
Patients and controls
The CARDIO2000 is a multicentre case–control study that explores the association between several socio-demographic, nutritional, lifestyle and clinical factors with the risk of developing non-fatal ACS. We stratified our sampling into all 10 Greek regions (Athens area, Sterea Hellas, Thessalia, Macedonia, Thrace, Epirus, Ionian Islands, Aegean Islands, Peloponnesus and Crete) according to the population distribution provided by the National Statistical Services. From every region we randomly selected a specific number of patients from the prefectorial or the major private hospitals. Thus, from January 2000 to August 2001, 848 out of 956 patients (89% response rate) who had been randomly pre-selected from the hospitals with a first symptom of coronary heart disease (CHD) (stable angina was excluded from the analysis) in their life, agreed to participate in the study (cases). Approximately half of the clinics in Athens and Thessalonica (the two major urban cities in Greece, covering about 55% of the total population) and almost all the clinics of the other counties were represented in the study. The number of participants was determined through power analysis, in order to evaluate a minimum difference of 7% in odds ratios per one unit increase in the explanatory variables with statistical power of 0.80 and P-value below 0.05.
The inclusion criteria for the 848 cardiac patients were as follows: first event of acute MI diagnosed by two or more features such as typical electrocardiographic changes, compatible clinical symptoms and specific diagnostic enzyme elevations; or first diagnosed unstable angina corresponding to class III of the Braunwald classification [21].
Following selection of the cardiac patients, we randomly selected 1078 subjects (830 males, 58.8 ± 10 years old and 248 females, 64.8 ± 10 years old) without any clinical symptoms or suspicion of cardiovascular disease, in their medical history (controls), matched to the patients by age (± 3 years), sex, and region. Controls were mainly subjects who visited the outpatients department of the same hospital and at the same period as the coronary patients, for routine examinations or minor surgical operations. In a few cases (in county hospitals), where the available number of hospitalized controls was not sufficient for the matching procedure, we enrolled into the study friends or colleagues of the coronary patients. We used this type of controls in order to have more accurate medical information, to eliminate the potential adverse effect of unknown confounders, and to increase the likelihood that cases and controls shared the demographics. The information regarding the investigated medical factors was obtained from the subjects' medical records.
Exposure parameters
The information regarding the investigated medical factors was retrieved from the subjects' medical records, and the information regarding the lifestyle characteristics through a confidential, detailed, questionnaire during a specific interview by a physician, after the second day of hospitalization, for the cases and at entry for the controls. The investigators of the CARDIO2000 study retrieved all the collected information. The evaluation of the nutritional habits was with a semi-quantitative food-frequency questionnaire based on the guidelines from the Department of Nutrition of the National School of Public Health [22]. The consumption of several food items, as an average per week during the past year, was measured and the frequency of consumption was quantified approximately, in terms of the number of times a month this food was consumed, respectively. Thus, weekly consumption was multiplied by four and a value of 0 was assigned to food items rarely or never consumed. Particularly, for dairy consumption, the quantity (i.e. portions per week; one portion equals one cup which equals 240 ml of milk, 150 g of yoghurt and 30 g of cheese) and type (no, low or full fat) of milk, cheese and yoghurt, were recorded. Additionally, the use of butter in daily cooking or meals was evaluated, but because its nutrient content is completely different from other dairy products and practically belongs to fats, it was not included in the multifactorial analyses as a dairy product. Alcohol consumption was measured by daily ethanol intake, in wineglasses (100 ml and 12% ethanol concentration) [23].
Current smokers were defined as those who smoked at least one cigarette per day. Quantification of smoking status was based on the calculation of pack–years adjusted for nicotine content equal to 0.8 mg per cigarette. Physical activity was defined as any type of non-occupational physical exercise, at least once per week during the past year, and was graded in qualitative terms such as light (expended calories < 4 kcal/min, i.e. walking slowly, stationary cycling, light stretching), moderate (expended calories 4–7 kcal/min, i.e. walking briskly, swimming with moderate effort) and vigorous (expended calories > 7 kcal/min, i.e. walking briskly uphill, long distance running, cycling fast or racing) [24]. The rest of the subjects were defined as physically inactive. The partcipants' social status was investigated through educational level, which was measured in years of school.
Detailed medical records were retrieved in all participants. Hypertension was defined as systolic/diastolic blood pressure > 140/90 mmHg or use of special treatment; hypercholesterolemia was defined as elevated total serum cholesterol levels (> 200 mg/dl) or use of lipid-lowering agents and diabetes as fasting blood glucose levels > 125 mg/dl or use of anti-diabetic medication. Presence of premature CHD among first-degree relatives (< 55 years for male relatives and < 65 years for female relatives) was also recorded. Finally, height and weight were measured and the body mass index (weight/height2) was calculated.
The CARDIO2000 study was approved by the Ethics Committee of the Department of Cardiology, Athens Medical School. Further details regarding the aims, design and methodology of the CARDIO2000 study have been previously presented [25].
Statistical analysis
Continuous variables are presented as mean ± standard deviation, while qualitative variables as absolute and relative frequencies (%). Contingency tables with calculation of χ2 test evaluated associations between the categorical variables, while using the Student's t-test we evaluated the associations between groups of study and continuous variables. The estimates of the odds ratios of having ACS were performed by calculating odds ratios and their corresponding 95% confidence intervals through conditional logistic regression analysis. First we evaluated all the interactions between the exposure variables and the main factor of interest (dairy consumption). Afterwards, we explored the potential confounding effect of the other exposure variables (by adding and removing each one from the model). Both elimination procedures were based on the Wald's statistic. Significant confounders, as well as interactions were retained in the model. Deviance residuals were calculated in order to evaluate the model's goodness-of-fit. Cut-off point analysis was used in order to determine the optimal value of the weekly dairy products intake that differentiates patients from controls. In particular, the crucial point defined by the largest distance from the diagonal line of the receiver operating characteristic curve (ROC) (sensitivity × (1 – specificity)). All reported P-values are two-sided and compared to a significant level of 5%. STATA 6 software was used for the calculations (STATA Corp., College Station, Texas, USA).
Results
Almost all (i.e. 98%) participants reported that they consume at least one portion of dairy products on a weekly basis, while 3.3% of patients and 1.3% of controls reported no consumption. Controls consumed more quantities of dairy products than cardiac patients (6.0 ± 1.7 versus 5.1 ± 1.4 portions per week, P < 0.001). Moreover, 72% of patients and 70% of controls consumed milk (P = 0.4), 40% of patients and 55% of controls consumed yogurt (P = 0.02), 38% of patients and 46% of controls consumed cheese (P < 0.001) and 23% of patients and 33% of controls consumed low fat dairy products (P < 0.001). Finally, 19.8% of patients and 14.9% of controls used butter in daily cooking or meals (P < 0.001).
Demographic and clinical characteristics of the participants by groups of dairy intake
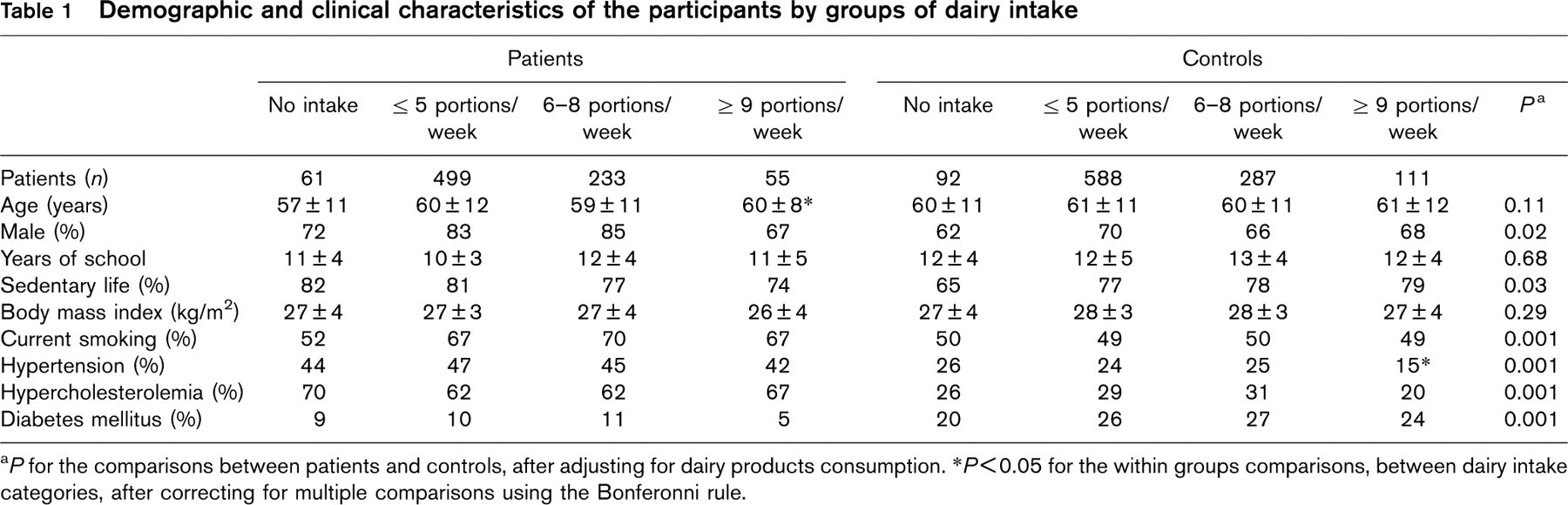
a P for the comparisons between patients and controls, after adjusting for dairy products consumption.
∗P<0.05 for the within groups comparisons, between dairy intake categories, after correcting for multiple comparisons using the Bonferonni rule.
Age–sex-adjusted odds ratios (95% confidence interval) for non-fatal acute coronary syndromes (acute myocardial infarction and unstable angina) associated with dairy consumption among men and women of the study sample
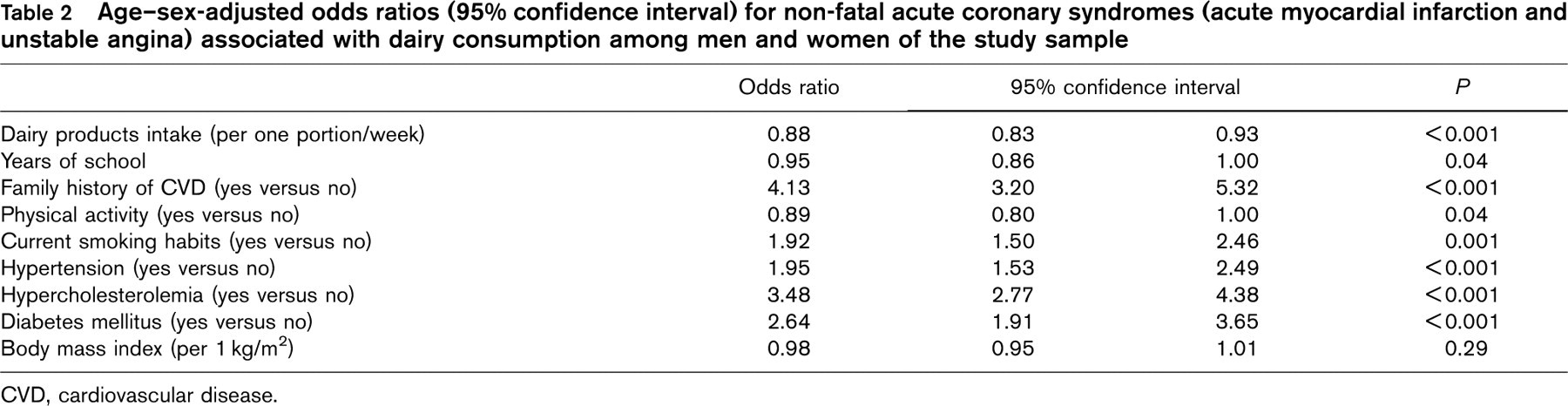
CVD, cardiovascular disease.
Table 1 presents various characteristics of the patients and controls, by tertiles of dairy intake. As we can see, compared to controls, patients were more likely to have hypertension, hypercholesterolemia, diabetes, be smokers, and physically inactive, even after adjusting for dairy products intake. Moreover, within group comparisons revealed that high dairy consumption was associated with increased age in cardiac patients and reduced prevalence of hypertension among control participants. No other significant associations were observed between dairy products intake and socio-demographic and clinical characteristics of the patients and the controls.
The age and sex-adjusted odds ratio of having ACS based on dairy products consumption was 0.86 (95% confidence interval 0.82–0.90), which means that one portion increase in consumption was associated with 14% lower likelihood of having an event. When dairy consumption was categorized into four groups (never or five or fewer portions/week, six to eight portions/week and nine or more portions/week) we observed that compared to low intake, only the highest group was associated with a significant decrease in the likelihood of having ACS (odds ratio = 0.16, 95% confidence interval 0.1–0.29), while moderate intake did not show any significant relationship (P = 0.18).
Food-specific analysis showed that compared to no intake, yellow and white cheese consumption was associated with 23 and 53% lower odds of ACS, respectively (odds ratio = 0.77, P < 0.001 and odds ratio = 0.47, P < 0.001); yoghurt intake was associated with 39% lower odds of ACS (odds ratio = 0.61, P < 0.001); and low fat dairy products seem to confer more protection: 59% lower likelihood of having cardiac events (odds ratio = 0.41, P < 0.001), after adjusting for age and sex of the participants. On the other hand, milk intake was not associated with the likelihood of having ACS, when other characteristics of the participants were taken into account (odds ratio = 1.16, P = 0.12). It should be mentioned, however, that patients and controls that consumed milk were older than those who did not consume (62 ± 12 versus 57 ± 11, P < 0.001) and were more likely to have diabetes (P = 0.022) and hypercholesterolemia (P = 0.008). Finally, use of butter in daily cooking or meals was associated with 2.7-times higher odds of having ACS, after adjusting for age and sex (odds ratio = 2.7, P < 0.001). No associations were observed between cheese or low fat dairy intake and age, sex or other clinical characteristics of the participants.
Confounding, however, may still exist. Thus, we have also adjusted for body mass index, smoking and dietary habits, physical activity level, educational status, as well as the presence of family history of CHD, hypertension, hypercholesterolemia, diabetes and any special medication used by the participants. Using multiple logistic regression analysis revealed that one portion increase in weekly dairy products intake was associated with 0.88 times (or 12%) lower likelihood of having ACS (from 7 to 17%) after controlling for various potential confounders (Table 2). Cut-off analysis showed that at least 7.4 portions per week are the minimum consumption that benefits people from having ACS. Among the other investigated factors physical activity was protective, while presence of hypertension, hypercholesterolemia and diabetes were associated with higher odds of having ACS.
Further stratified analysis showed that dairy intake was still protective among obese (odds ratio = 0.89, P = 0.05), overweight (odds ratio = 0.87, P = 0.001) and normal weight (odds ratio = 0.84, P = 0.001) participants. Similarly, when we stratified our analysis by hypercholesterolemia status we did not find any significant alterations. Specifically, dairy intake was associated with 9% reduced odds of having ACS in hypercholesterolemic (odds ratio = 0.91, P = 0.04) and 15% lower odds in normal participants (odds ratio = 0.85, P < 0.001). The benefits were still highly significant among normotensive (odds ratio = 0.85, P < 0.001) and hypertensive subjects (odds ratio = 0.91, P = 0.04). A significant interaction was observed between presence of diabetes and dairy products consumption. In particular, the benefits from dairy intake were still highly significant among non-diabetic people (odds ratio = 0.87, P < 0.001). No significant associations were observed between ACS and dairy products intake into diabetic patients (odds ratio = 1.02, P = 0.27).
Finally, no significant interactions were observed between dairy products intake and various food items consumed or alcohol intake, on the odds of having ACS (data not presented in text or tables).
Discussion
The present study revealed that the consumption of dairy products is significantly associated with lower odds of having acute coronary events, even after controlling for several potential confounding risk factors. In particular, those in the highest tertile of consumption (nine or more servings per week) had 84% lower relative odds for ACS, compared with those who did not consume dairy products, whereas the risk of ACS was 59% lower in those who consumed low fat dairy products. Furthermore, we observed that more than seven portions per week (or about one portion per day, i.e. 240 ml of milk, 150 g of yoghurt and 30 g of cheese) seem to be the minimum intake of dairy products that benefits CHD risk.
Although Greece may have several particularities regarding the culture of dietary habits, our study sample reported the intake of a wide range of dairy products, milk, yoghurt, white cheese (e.g. Greek Feta) and yellow cheese (e.g. Edam, Gouda) and hence our results can be compared with those from other countries of central or northern Europe. In the literature there are several approaches concerning the relation between diet and CVD risk, exploring the role of nutrients alone, others exploring the role of food groups and others exploring food patterns. Previous studies that examined the potential effect of total calcium intake [10, 26] on CVD risk, have conflicting results, as well as those exploring the effect of dairy products on CVD risk [27, 28]. Data from the prospective study of Bostick et al. [27] showed a 6% reduction in CHD risk by consumption of dairy products, but this was not statistically significant. On the other hand, Tavani et al. [28] showed that consumption of seven or more cups of milk, seven or more portions of yoghurt or 350 g or more cheese per week had a protective effect against MI. Most of the studies examined the effect on CVD of milk alone and were reviewed by Elwood et al. [9]. The pooled estimate of the relative odds for ischemic heart disease in the subjects with the highest milk intakes, compared to those with the lowest, was 0.87 [9]. On the contrary, results from the Seven Countries Study positively associated milk intake with CHD [29]. In our study, we failed to show a significant association between milk intake and the likelihood of having ACS, after adjusting for various potential confounders, as previous studies did and this could be attributed to the increased age and higher burden of other co-morbidities observed among milk consumers.
Scientific evidence has revealed that there are factors in milk and milk products which may actively protect from CVD, by improving many risk factors [30]. Several bioactive peptides and as yet unidentified components in whole milk may protect from hypertension; folic acid, vitamins B6 and B12 or other components may contribute to low homocysteine levels, whilst conjugated linoleic acid may have hypolipidemic and antioxidative and thus antiatherogenic properties [30]. It should, however, be mentioned that dairy products are potentially full of very different fatty acids and that the origin of the milk products is very important in that context, as Hauswirth et al. [31] recently reported in a review paper. Additionally, hypocholesterolemic or hypotensive properties have been attributed to fermented dairy products (e.g. yoghurt), although the existing data do not yet allow definitive conclusions [32].
Quantitative analysis showed that moderate dairy intake did not show any significant association with cardiac risk. Therefore, we have suggested that an intake of at least 7.4 portions/week should be provided in order to observe a significant reduction in ACS risk. This is important for public health and gives one more reason why dairy products should be ingested daily. Current dietary guidelines for adults [33] recommend the intake of three portions of dairy products per day to optimize bone health and therefore such a recommendation could also provide protection against cardiac risk.
We also observed that low fat dairy products seem to confer more protection on the likelihood of having cardiac events by lowering the risk by 59%. Results from cohort studies have not revealed such a protection probably because they had been set up at times when reduced fat milks were unavailable or scarce [9], whereas Tavani et al. [28] observed an identical benefit of high intake of both full-fat and semi-skimmed milk against MI.
Moreover, stratified analysis showed that the protection of dairy consumption against cardiac events is independent of the presence of overweight/obesity and hypercholesterolemia. This is an important message since a lot of overweight or hypercholesterolemic people try not to consume dairy products in order to control their body weight or serum cholesterol levels.
Furthermore, according to our results, high dairy consumption was associated with reduced prevalence of hypertension among control participants, whereas dairy benefit was also significant both in normotensive and hypertensive participants. Many studies link higher intakes of dairy products with lower blood pressure and reduced risk of hypertension [15–17]. Milk is a complex mixture of nutrients that can influence blood pressure, including minerals (calcium, sodium, potassium and magnesium), vitamins (D, B6, B12) and potentially lipids [34]. A number of peptides derived from casein have been suggested to act as hypotensive components by inhibiting angiotensin I-converting enzyme that is involved in the renin–angiotensin system [35]. Finally, the Dietary Approaches to Stop Hypertension (DASH) study showed that a diet rich in low-fat dairy products, fruits and vegetables and low in sodium is the best for the prevention and treatment of high blood pressure [36].
Limitations of the study
In case–control studies two main sources of systematic errors may exist: the selection and the recall bias. In order to eliminate selection bias we tried to set objective criteria, both for patients and controls. Insignificant misclassification may exist, however, since a small percentage of asymptomatic coronary patients may be wrongly assigned to controls, even though they were evaluated by a cardiologist. Concerning information bias we tried to avoid it through accurate and detailed data from subjects' medical records. Moreover, the coronary patients who died at entry or the day after were not included into the study. This bias could influence our results, but, since the proportion of deaths during the first 2 days was estimated at between 2 and 4%, by the physicians of the study, we believe, that the inability to include the fatal events did not significantly alter our findings. Furthermore, we tried to reduce the potential effect of uncontrolled, unknown confounders by using the same study base both for patients and controls.
Conclusion
According to our findings dairy consumption seems to offer significant protection against CHD. The optimal consumption that benefits people from acute cardiac events is about one portion per day and could be incorporated as an aim of CVD prevention programmes for the benefit of public health.
Footnotes
Acknowledgements
The authors would like to thank the physicians and the specialists that co-ordinated the data collection of this study: K. Tzioumis (Athens, Crete, Pelloponisos), J. Skoumas (Athens), N. Papaioannou (Athens, Thessalia), P. Stravopodis (Ionian Islands), L. Karra (Aegean Islands), D. Antoniades (Macedonia), G. Rembelos (Aegean Islands), D. Markou (Athens), A. Moraiti (Athens), D. Evagelou (Crete), S. Vellas (Attica, Hpeirous), G. Skoumbourdis (Sterea Hellas), B. Meidanis (Macedonia, Sterea Hellas, Thessalia), S. Loggos (Attica), Í. Elefsiniotis (Athens), N. Marinakis (Aegean Islands), G. Koutsimbanis (Thrace) and S. Zombolos (Peloponnese).