
Abstract
Background
The cardiovascular effects on fibrinolytic activity by urban air pollution are still unknown.
Methods
Paired fasting blood samples during high and low air pollution days in Taipei were taken from a panel of 49 patients with coronary heart disease or multiple risk factors to study their fibrinolytic and inflammatory response to urban air pollution. Paired t-tests and mixed-effects models were used to determine the air pollution effects.
Results
Patients' plasma plasminogen activator inhibitor-1 levels were significantly increased when hourly concentrations of particulate matter with diameters less than 10 μm (PM10) were greater than 100 μg/m3 during the period 0800 to 1800 h.
Conclusion
Urban air pollution has an adverse effect on plasma fibrinolytic function in a susceptible population.
Keywords
Introduction
Several epidemiologic and clinical observational studies on air pollution have shown that elevated concentrations of particulate matter with diameters less than 10 μm (PM10) and less than 2.5 μm (PM2.5) are associated with increased coronary heart disease (CHD) morbidity and mortality [1, 2]. Understanding of the biological mechanisms that associate particulate matter pollution with CHD, however, remains limited [3–5]. Previous studies have reported that high particulate air pollution can increase high sensitivity-C-reactive protein (hs-CRP) in healthy adults [6, 7]. It has also been reported that penetrated particles may exert adverse cardiovascular effects by increasing patients' fibrinogen levels [8, 9].
Two fibrinolytic parameters, plasma tissue-type plasminogen activator (tPA) and plasminogen activator inhibitor-1 (PAI-1), are also important risk factors for CHD [10, 11]. High plasma PAI-1 concentrations predicted the incidence of myocardial infarction in patients with stable angina pectoris [12]. Thus, high plasma PAI-1 can be considered a good marker of impaired fibrinolytic function and as a surrogate marker for a subsequent increase in CHD.
Except for fibrinogen, however, the effects of particulate matter exposure on fibrinolytic parameters in patients with CHD have rarely been investigated. In this study, we hypothesized that exposures to high air pollution episodes could induce changes in fibrinolytic function and inflammatory markers in a susceptible population in Taipei.
Materials and methods
Participants
This panel study was conducted from February to April 2002. There were two groups among our 49 non-smoking subjects: 23 CHD patients and another 26 patients with multiple CHD risk factors (non-CHD patients). All of these study subjects were recruited from cardiology clinics of the Department of Internal Medicine, National Taiwan University Hospital and lived in Taipei metropolitan area. CHD patients were defined as patients who had a history of angina pectoris or acute myocardial infarction, and had received cardiac catheterization and percutaneous trans-luminal coronary angioplasty. Patients with multiple CHD risk factors were defined as those who were not diagnosed as having CHD but had at least two of the following CHD risk factors: hypertension, diabetes mellitus and dyslipidemia. CHD patients with low-density lipoprotein (LDL) cholesterol levels of 3.317 mmol/l or higher, non-CHD patients with LDL cholesterol levels of 4.137 mmol/l or greater, those with triglyceride levels of 2.258 mmol/l or higher, those with high-density lipoprotein (HDL) cholesterol below 1.034 mmol/l, or those on lipid-lowering agents were defined as having dyslipidemia. The ethics committee of the National Taiwan University Hospital approved this study, and informed consent was obtained from each study participant.
Air pollution levels
A Taiwan Environmental Protection Agency (TEPA)-operated air-monitoring station, the Particulate Matter Supersite, which is located in the center of the Taipei metropolitan area, has measured hourly air pollution levels of particulate matter with size less than 10 μm (PM10) and 2.5 μm (PM2.5), sulfate (SO−2 4), nitrate (NO− 3), organic carbon, elemental carbon, temperature and humidity continuously since 2002. Hourly levels of ozone were measured by 12 TEPA-operated fixed site monitoring stations, which are located around the Taipei metropolitan area.
We used daytime (0800 to 1800 h) hourly PM10 concentrations of 100 μg/m3 reported by the Supersite as a criterion to define days of high or low air pollution in Taipei in this study. We then calculated 24-h averages (midnight to midnight) of air pollution and temperature measurements from the Supersite to represent daily air quality and weather condition that our study participants experienced during the low and high air pollution days. Therefore, two sets of daily environmental data were used for each study participant.
Inflammatory markers and fibrinolytic factors
Paired fasting (10–14 h) blood samples were taken during high and low air pollution periods for each participant. After we noticed that daytime hourly PM10 concentrations were greater than 100 μg/m3 we informed our participants that night to come to receive blood drawing the next morning. We repeated the same blood sampling for the low pollution days for each individual. Our participants were blinded to air pollution conditions on the monitoring days. A retrospective diary was also used to document each participant's activities during his or her high or low air pollution days.
Serum total cholesterol, HDL cholesterol, and triglyceride levels were measured by enzymatic methods. The LDL cholesterol level was then calculated using Friedewald's formula. Serum hs-CRP, interleukin (IL)-6, and tumor necrotic factor-α (TNF-α) were measured with commercial kits. Antigens of tPA and PAI-1 were measured by the enzyme-linked immunosorbent assay method (IMUBIND tPA ELISA and IMUBIND PAI-1 ELISA; American Diagnostica, Stamford, Connecticut, USA). Fibrinogen was measured by the clotting method of Clauss (Diagnostica Stago, Asnières sur Seine, France).
Statistical analysis
We used paired t-tests to evaluate the self-comparisons of differences for each participant in air pollution levels, fibrinolytic factors, and inflammatory markers between high air pollution days and low air pollution days. We further applied linear mixed-effects models to examine the association between air pollution levels and fibrinolytic factors and inflammatory markers with sex, age, temperature and humidity being adjusted. Test results were considered statistically significant or marginally significant when P-values were below 0.05 or 0.10.
Results
There were 31 male and 18 female subjects in our study. Their ages were 62.7 ± 9.5 (40–75) years. The average body mass index was 25.6 (± 3.5) kg/m2 and mean systolic/diastolic blood pressure was 130.5 (± 10.8)/79.8 (± 7.0) mmHg. The medical histories showed that 18 had diabetes (37%), 23 had hypertension (63%) and 45 were dyslipidemic (92%). There were 34 dyslipidemic participants taking statins (69%) and another six taking fibrates (12%). The documented records showed that all study subjects' medication and physical activities did not change during the entire study period.
The self-comparisons of air pollution exposures, inflammatory markers, and fibrinolytic factors during high and low pollution days in 49 study subjects are list in Table 1. By comparing particulate matter measurements in high air pollution days with those in low air pollution days, we found PM10 increased by 53.7 μg/m3, PM2.5 increased by 37.9 μg/m3 and ozone increased by 20.8 ppb. The concentrations of particulate matter's chemical components during high air pollution days were also significantly higher than those in low air pollution days. On average, they were 3.6 μg/m3 higher in organic carbon, 2.5 μg/m3 higher in elemental carbon, 4.8 μg/m3 higher in sulfate, and 3.5 μg/m3 higher in nitrate during the high air pollution days compared with low air pollution days. The temperature in Taipei during the high air pollution days was not significantly different from that in the low air pollution days. For the air pollution data at 2-day to 4-day averages before blood samples were taken, we observed similar difference between high and low pollution days as 1-day averages (data not shown).
Self-comparison of air pollutants, inflammatory makers and fibrinolytic factors between high pollution and low pollution days in coronary heart disease patients and patients with multiple coronary heart disease risk factors
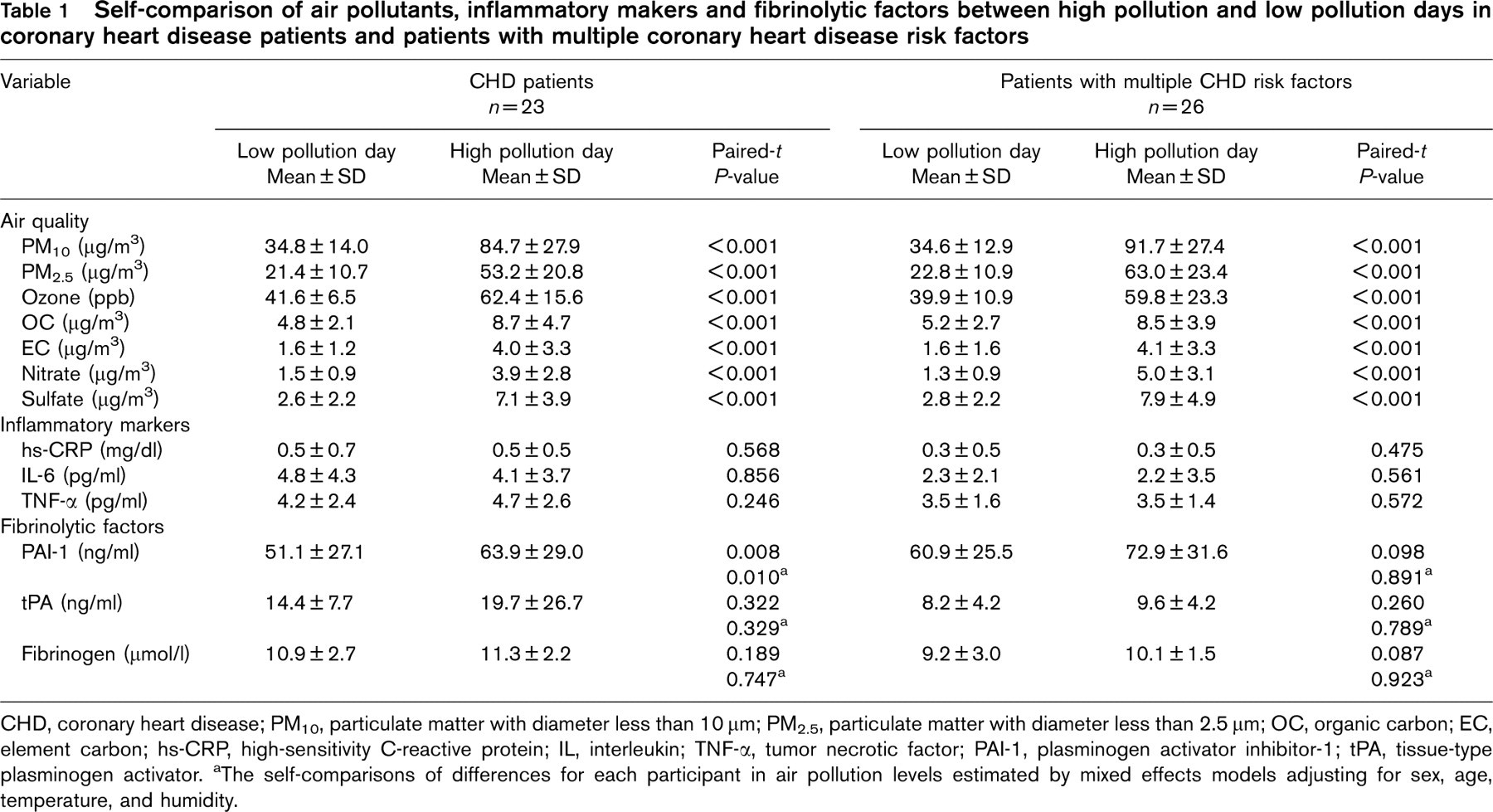
CHD, coronary heart disease; PM10, particulate matter with diameter less than 10 μm; PM2.5, particulate matter with diameter less than 2.5 μm; OC, organic carbon; EC, element carbon; hs-CRP, high-sensitivity C-reactive protein; IL, interleukin; TNF-α, tumor necrotic factor; PAI-1, plasminogen activator inhibitor-1; tPA, tissue-type plasminogen activator.
aThe self-comparisons of differences for each participant in air pollution levels estimated by mixed effects models adjusting for sex, age, temperature, and humidity.
We first analyzed our data by grouping both patient groups. Paired t-tests showed no significant changes in our subjects' hs-CRP, IL-6, TNF-α, and tPA between high and low air pollution days. PAI-1 and fibrinogen levels were significantly increased by an average of 11.3 ng/ml and 0.71 μmol/l during high air pollution days (data not shown). We also found that plasma PAI-1 levels significantly increased by an average of 12.8 ng/ml for the CHD patients during high air pollution days. Moreover, the results showed that plasma levels of PAI-1 were still significantly higher in high air pollution days after adjusting for temperature, humidity, sex, and age in CHD patients. PAI-1 and fibrinogen levels, however, became non-significant after adjusting covariates for the non-CHD group. By contrast, we found no significant difference between high and low pollution days for tPA, hs-CRP, IL-6, and TNF-α for both patient groups.
Discussion
This is the first report to show that impaired fibrinolytic factors (concurrently increased PAI-1 and fibrinogen levels) may be triggered independent of inflammation pathways in patients with CHD or patients at risk for developing CHD during high air pollution days. Significant increases in plasma fibrinogen levels coupled with significant elevation in plasma PAI-1 levels were possibly attributable to high mass concentrations of coarse and fine particulate matter as well as carbon, sulfates, and nitrates contained in particulate matter during the high air pollution days.
Our study agrees with Seaton's hypothesis [13], which was confirmed in later large population studies [8, 9], showing that fibrinogen levels increase in subjects exposed to air pollution. Further subgroup analysis in our study found that PAI-1 levels increased significantly during high air pollution periods in CHD patients, but did not increase in participants with multiple CHD risk factors. Increasing plasma PAI-1 has been considered as an acute reaction of vascular endothelial stimuli, especially in atheromatous arteries [14]. Our findings support that CHD patients' diseased arteries are vulnerable to adverse stimuli from environmental factors, such as exposure to high air pollution in our study. As patients with multiple CHD risk factors are reported to have atherosclerotic plaque in their diseased arteries [15], we believe this explains why there was also a marginal increase in fibrinogen and PAI-1 levels in 26 patients with multiple CHD risk factors in this study. Accordingly, our findings of increased plasma PAI-1 may indicate an early vascular response to air pollutants in study participants during high air pollution days. Studies have shown that fibrinolytic factors of PAI-1 [16] and fibrinogen [17] levels are higher in cold weather and lower in warm weather. In addition to pollution effects, our study also confirmed such temperature effects on PAI-1 and fibrinogen.
The absence of significant increases in inflammatory markers may be due to the wide use of lipid-lowering medications, the frequency of which was about 81% in our study participants. Statins are known to have anti-inflammatory effects [18]. The potential protective effects of medications, such as statins, on CHD patient's response to air pollution have been proposed as an important research issue in one recent consensus report [5]. The source of our participants in this study underscores the relatively difficult task of evaluating the effects of air pollution on such a susceptible population without medication's confounding effects.
Since we used air pollution levels from air monitoring stations to represent individuals' exposures, we could misclassify our study subjects' exposures to air pollutants in this panel study. It has been reported that such exposure misclassification can bias our outcomes toward either null or positive results when exposures are correlated [19, 20].
Regardless of such limitations, we conclude that urban air pollution in Taipei impairs fibrinolytic activity in patients with CHD and multiple CHD factors by concurrently elevating their PAI-1 and fibrinogen. We believe high concentrations of particulate matter and several chemical components contained in particulate matter are responsible for the pathogenesis on their cardiovascular systems. The mechanism responsible for fibrinogen and PAI-1 elevation remains to be elucidated. Therefore, more studies are recommended to investigate the role of air pollution in increasing the risk of thrombosis and its relation to the risk of cardiovascular events.