
Abstract
Background
Cardiac troponins I and T and brain natriuretic peptide are the accepted standards to serologically identify myocardial necrosis and elevated wall stress. In addition, they allow risk stratification in cardiovascular patients. The clinical significance of increases in cardiac markers after strenuous endurance exercise in obviously healthy athletes is unclear.
Design
We therefore examined the reproducibility and clinical significance of exercise-induced increases in cardiac troponins I and T and N-terminal pro brain natriuretic peptide after two standardized endurance exercise trials in healthy endurance athletes with prior competition-induced elevations of cardiac troponins (I, 0.08–1.93 μg/l; T, 0.01–0.56 μg/l).
Methods
Twenty male athletes (36 ± 7 years; V O2max : 60 ± 5 ml/min per kg) completed a 1-h and a 3-h exercise study (exercise intensities 100 and 75%, respectively, of the individual anaerobic threshold) on two different days in randomized order to determine cardiac markers before, 30 min and 3h after exercise. In addition to pre- and post-exercise echocardiography including tissue Doppler imaging, delayed enhancement magnetic-resonance-imaging was performed after a 3-h exercise study to detect myocardial necrosis.
Results
A marginal increase in cardiac troponin I was documented after both exercise trials (from 0.02 to 0.03 μg/l; P>0.001). Cardiac troponin T remained without significant changes. N-terminal pro brain natriuretic peptide increased by 9 and 30 ng/l after 1-h and 3-h exercise studies, respectively (P>0.001). In contrast to cardiac troponins, increases in N-terminal pro brain natriuretic peptide after competition correlated with those after 1-h exercise study (ρ = 0.88) and 3-h exercise-study (ρ = 0.82). No pathologies were demonstrated by echocardiography or delayed-enhancement magnetic resonance imaging.
Conclusions
Due to the missing reproducibilty and evidence of myocardial damage, exercise-induced increases in cardiac troponins may represent a physiologic reaction under special conditions and seem to be without pathological significance in healthy athletes. Eur J Cardiovasc Prev Rehabil 13:388–397 © 2006 The European Society of Cardiology
Keywords
Introduction
Cardiac troponin T (cTnT) and cardiac troponin I (cTnI) are the accepted gold standards to diagnose myocardial injury serologically. In addition, elevated levels of brain natriuretic peptide (BNP) and its cleaved fragment N-terminal pro BNP (NT-proBNP) indicate myocardial dysfunction [1]. In the clinical setting, the use of these markers has been proven to hold advantages as superior diagnostic tools to other markers as well as excellent tools for risk stratification [2, 3]. Exercise-induced elevations of cardiac troponins and NT-proBNP reported after strenuous exercise in obviously healthy athletes, however, are still a matter of debate. At present, two theories of the exercise-induced release of cardiac troponins are discussed: irreversible injury (necrosis) and reversible injury of cardiomyocytes [4]. Because many studies documented elevations of cardiac troponins above upper reference limits (URLs) after prolonged and strenuous exercise, an exercise-induced myocardial damage was assumed [5–9]. Nevertheless, there is increasing evidence that exercise-induced elevations of cardiac markers do not necessarily represent myocardial damage in healthy athletes [4, 10–13].
As we have previously reported, in 105 endurance athletes the URL of NT-proBNP was exceeded in 77%, and the URLs of cTnI and cTnT in 74 and 47%, respectively, after prolonged strenuous exercise [14], but the non-invasive cardiological follow-up of 21 athletes with the highest elevations in cTnI and cTnT revealed no signs of myocardial damage or heart disease except in one athlete with prior unknown coronary artery disease [13]. The applied non-invasive methods could, however, have been not sensitive enough to detect sub-clinical myocardial damage, coronary artery or heart disease in these athletes. Therefore, we conducted the present study to examine in a standardized fashion, if exercise-induced elevations in cTnT and cTnI as well as NT-proBNP after competition are reproducible and are associated with clinical consequences. In addition, the impact of intensity and duration of exercise on elevations of cardiac markers should be examined. To achieve this information, sensitive diagnostic testing was utilized including pre-exercise and post-exercise echocardiography with tissue Doppler imaging (TDI) analysis, as well as delayed enhancement magnetic resonance imaging (DE-MRI) to detect myocardial necrosis by hyperenhancement. The presence of an increase in NT-proBNP, in association with reduced cardiac function at echocardiography or myocardial hyperenhancement in DE-MRI would be considered of pathological significance.
Methods
General design
Out of 105 endurance athletes studied on exercise-induced elevations of cTnT, cTnI and NT-proBNP after competition [14], athletes with the highest cTnI or cTnT values were invited for the study, which was approved by the review board of the German National Institute of Sports Science. To exclude acute or chronic diseases, an initial medical examination including the determination of routine blood parameters, blood pressure, electrocardiography (ECG) and Doppler echocardiography at rest, an exercise ECG with additional determination of the individual anaerobic threshold (IAT) by the method of Stegmann et al. [15], as well as an exercise echocardiography were performed in all athletes. On two separate days, athletes had to perform in randomized order either 1 h of endurance exercise with an intensity of 95–100% IAT (1 h exercise study) or 3 h of endurance exercise with an intensity of 75% IAT (3 h exercise study) (intensities correspond to approximately 75 and 60% V O2max , respectively) in their major discipline (running or mountain biking) on a 400 m track. Intensities were prescribed by heart rates and supervised by heart rate monitors (Polar, Kempele, Finland). Intensities of 75% IAT and 95–100% IAT were chosen as they represent the maximal sustainable intensities for the chosen durations of endurance exercise, and therefore guarantee a sufficient stress for the cardiopulmonary system. Venous blood samples were taken before, 30 min and 3 h after exercise. To avoid prior exercise-induced changes on blood markers, athletes were told to refrain from intensive or prolonged training sessions in the days before the studies. The tests took place between March and December, and weather conditions between the two exercise studies (1-h and 3-h) were comparable on an intra-individual basis without differences in mean temperature or humidity.
Study population
Twenty male athletes [15 mountain bike marathon cyclists and five marathon runners; age 36 ± 7 years; height 183 ± 8 cm; weight 79 ± 7 kg; calculated V O2max (method of Swain et al. [16]) 60 ± 5 ml/min per kg] gave their written informed consent to take part in the study. The median period of time between the competition race and the present study was 7.5 months; the median period of time between the 1-h and the 3-h exercise studies was 3 weeks. Athletes had a training history in endurance exercise of 7 ± 3 years and trained 9 ± 4 h per week. Athletes reported no changes in their training habits in the time between the competition race and the present study, and were told to refrain from intensive or prolonged training sessions the days before the exercise studies.
Diagnoses of athletes’ initial medical examination are reported in Table 1. Standard echocardiographic parameters determined at the athletes’ initial medical examination were as follows: left and right ventricular end-diastolic diameters, 54 ± 5 and 25 ± 5 mm; interventricular septum thickness, 11 ± 1 mm; posterior wall thickness, 10 ± 1 mm; fractional shortening, 38 ± 8%; E/A ratio, 1.4 ± 0.3; heart volume (method of Dickhuth [17]), 12.2 ± 1.4 ml/kg.
Athletes’ discipline and competition exercise times, age, maximal concentrations of cardiac troponins I and T and N-terminal pro brain natriuretic peptide after competition, the 1-h exercise study and the 3-h exercise study, and the echocardiographically determined ejection fractions examined 1 h before and 1 h after both exercise studies
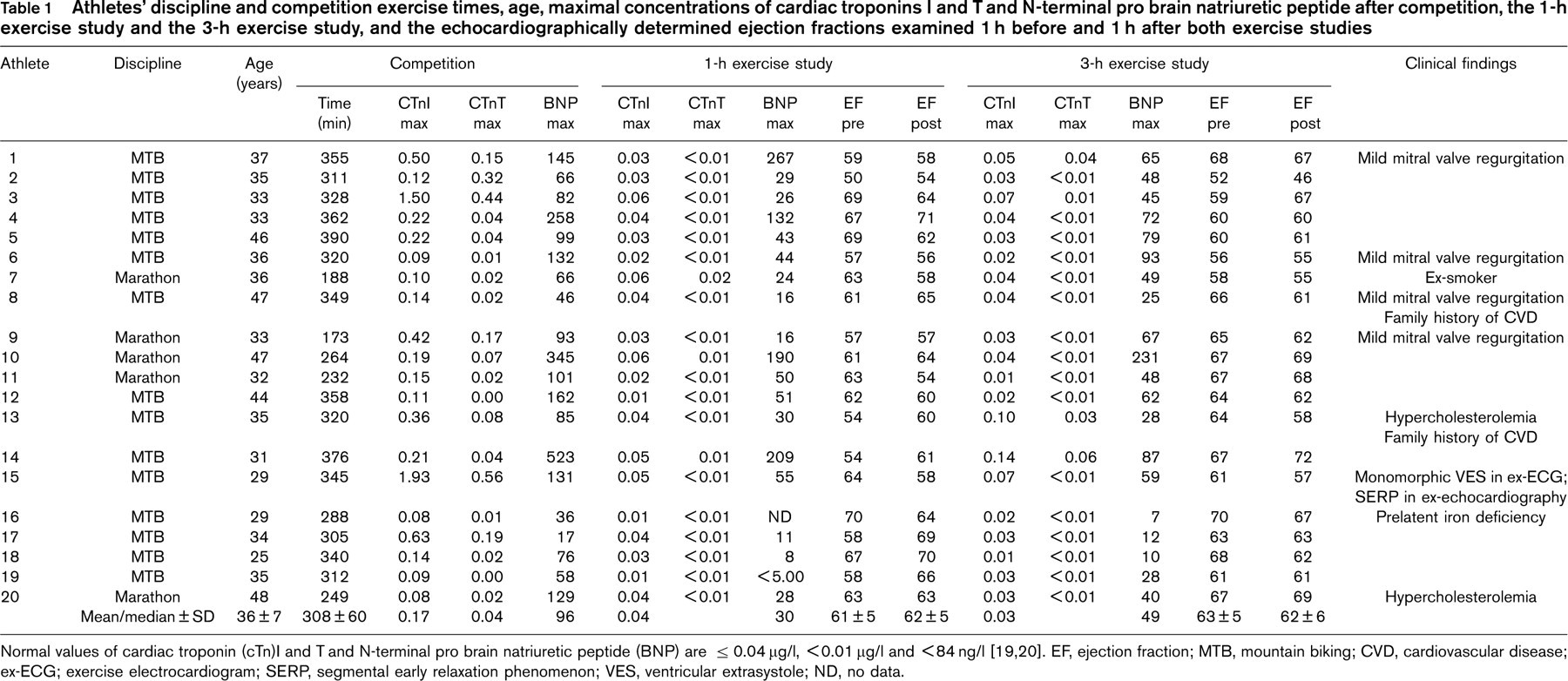
Normal values of cardiac troponin (cTn)I and T and N-terminal pro brain natriuretic peptide (BNP) are ρ 0.04 μg/l, >0.01 μg/l and < 84 ng/l [19, 20]. EF, ejection fraction; MTB, mountain biking; CVD, cardiovascular disease; ex-ECG; exercise electrocardiogram; SERP, segmental early relaxation phenomenon; VES, ventricular extrasystole; ND, no data.
Exercise ergometry
To determine the IAT, an incremental multi-stage cycle ergometry for cyclists and a treadmill ergometry for marathon runners was started at 100 W and 3 m/s, respectively, and increased by 50 W and 0.5 m/s, respectively, every 3 min until exhaustion. Capillary blood samples were taken from the hyperaemized earlobe at the end of each stage and 1, 3, 5, 7 and 10 min after cessation of exercise to determine lactate concentrations (Greiner Super GL, Flacht, Germany). In addition, a 12-lead ECG and the blood pressure were recorded.
Echocardiography
Doppler echocardiography was performed on a GE System FiVe (GE, Vingmed Ultrasound, Horten, Norway) with a 2.5 MHz-transducer in accordance with the guidelines of the American Society of Echocardiography on the day of the initial medical examination as well as on both exercise days 1 h before and 1 h after exercise. In addition to standard echocardiographic parameters determined in the parasternal and the apical view, the ejection fraction by use of the Simpson rule and the isovolumetric relaxation time were determined. Systolic and diastolic myocardial velocities were determined at the basis of the left ventricular septum by TDI.
Magnetic resonance imaging
Athletes were studied 6.5 ± 1.4 h after cessation of the 3-h exercise study in the supine position in a 1.5 T scanner (Sonata; Siemens, Berlin, Germany). Initially, ECG-gated cine images were acquired by use of a True-FISP sequence (TR/TE = 44/1.5 ms) with a breath-hold technique to analyse left ventricular function applying 10–14 short axis slices as described previously [18]. Contrast enhanced imaging was performed by applying 0.1 mmol gadolinium-based contrast agent (Gd-BOPTA; Multi-Hance, Bracco, Milano, Italy) per kilogram of bodyweight, administered intravenously through an antecubital vein. Contrast enhanced images for DE-MRI were acquired in long and short axis planes after a 15-min delay using a T1-inversion-recovery segmented gradient-echo sequence (TR/TE 650/4.0 ms). Typical voxel size was 2.1 × 1.6 × 8.0 mm.
Troponin I and T
CTnI and cTnT were measured by chemiluminescence immunoassays on automated analysers (AccuTnI, Access; Beckman Coulter, Krefeld, Germany; Troponin T Elecsys 3rd Generation, Elecsys 2010; Roche Diagnostics, Mannheim, Germany) detecting free cardiac troponin as well as binary and tertiary complexes. For cTnI, the cross reactivity with skeletal cTnI and human cTnT is 0.034 and 0.001%, respectively (functional sensitivity 0.03 μg/l with 20% imprecision, 10% imprecision at 0.06 μg/l, total imprecision at 0.57 μg/l 5.8%). For cTnT, the cross reactivity with skeletal troponin T and human cTnI is 0.001 and 0.002%, respectively (functional sensitivity 0.01 μg/l with 20% total imprecision, intra- and interassay imprecision at 0.48 μg/l 1.2 and 4.9%). The URLs defined as the 99th percentile in healthy subjects are <0.04 μg/l for cTnI and >0.01 μg/l for cTnT [19].
N-terminal pro brain natriuretic peptide
NT-proBNP was measured by chemiluminescence on an automated analyser (Elecsys proBNP; Elecsys 2010; Roche Diagnostics, Germany). Since the precursor peptide proBNP (amino acids 1–108) is cleaved into fragments of NT-proBNP (amino acids 1–76) and BNP (amino acids 77–108) during its secretion into the extracellular space, NT-proBNP represents BNP in an aquimolar manner. The test uses two polyclonal antibodies, which bind to the NT-proBNP peptide and form a stable sandwich complex. The sensitivity of the test is 5 ng/l. Intra-assay and inter-assay coefficents of variance at 175 ng/l are 2.7 and 3.2%, respectively, without cross-reactivities with other hormones. The URL is 84 ng/l for men under 50 years, defined as the 99th percentile in healthy subjects [20].
Creatine kinase and creatine-kinase-MB, creatinine, haematocrit and haemoglobin
On an automated analyzer (Synchron CX5; Beckman Coulter); creatine kinase (CK) and CK-MB activity were measured enzymatically at 25°C, and creatinine by the method of Jaffé. Haematocrit and haemoglobin concentrations of venous blood samples were measured on an automated analyzer (Sysmex K-1000; Sysmex GmbH, Langenfeld, Germany).
Statistics
For statistical calculations the software package Statistica 6.1 (StatSoft Inc, Tulsa, Oklahoma, USA) was used. Gaussian distribution was tested with the Kolmogorov-Smirnov test. Gaussian-distributed values are expressed as mean ± standard deviation; changes in dependent variables were tested by analysis of variance and post hoc by the Scheffé test. Differences for independent variables were tested by the unpaired Student t-test. For non-Gaussian-distributed variables, values are given as medians. Changes in non-Gaussian-distributed dependent variables were tested with the Friedman-analysis of variance; medians were compared by the Wilcoxon test for paired samples. Independent samples were compared by the Mann-Whitney test. The Spearman correlation coefficient was calculated to test relationships between cardiac markers. An α-error below 0.05 was considered as statistically significant. CTnT concentrations below 0.01 μg/l were set as 0, NT-proBNP concentrations below 5 ng/l as 5 ng/l.
Results
Exercise intensities were prescribed by exercise heart rates, which could be kept by all athletes. Athletes finished both exercise studies without cardiovascular symptoms or other health problems. Mean heart rates, lactate concentrations and covered distances are given in Table 2.
Mean exercise heart rates, lactate concentrations and covered distances of the 1-h and the 3-h exercise studies of mountain bikers and marathon-runners

Data are given as mean ± SD. MTB, mountain biker.
Cardiac troponins I and T and N-terminal pro brain natriuretic peptide
Before exercise, all athletes presented normal resting values for cTnI, cTnT and NT-proBNP. Maximum individual cTnI, cTnT and NT-proBNP concentrations of the 1-h and 3-h exercise study as well as of the competition races are presented in Table 1. In the competition races, the URL of cTnI was exceeded in all athletes and that of cTnT was exceeded in 18 athletes. NT-pro BNP exceeded the URL in 12 athletes. In the 1-h exercise study, elevated concentrations for cTnI and cTnT were documented in five and three athletes, respectively. The URL of NT-proBNP was exceeded in four cases. In the 3-h exercise-trial, cTnI and cTnT were elevated in five and four athletes, respectively, and NT-proBNP was elevated in three. Taking both exercise studies together, cTnI exceeded the URL in seven and cTnT in six athletes. Elevations above the URL in both trials were documented in three athletes for cTnI and two athletes for cTnT.
The median concentrations of cTnI significantly increased in the 1-h exercise study from 0.02 μg/l before to 0.03 μg/l 3 h after exercise, and in the 3 h exercise study from 0.02 μg/l before to 0.03 μg/l 30 min and 3 h after exercise (all P <0.01). Median cTnT concentrations did not change in both exercise studies. Median concentrations of NT-proBNP significantly increased in the 1-h exercise study from 21 ng/l before to 30 ng/l 30 min after exercise, and decreased to 24 ng/l 3 h after exercise (P >0.001). In the 3-h exercise study, NT-proBNP significantly increased from 19 ng/l before to 49 ng/l 30 min after exercise, and decreased significantly to 38 ng/l 3h after exercise (P >0.001).
Increases in cTnI and cTnT of both exercise studies were not related to the increases in the competition races. On the other hand, maximal NT-proBNP concentrations of both, the 1-h and the 3-h exercise studies were significantly related to the maximal NT-proBNP concentrations after competition (Fig. 1). This also holds true when three extreme values are excluded (1-h exercise study, ρ = 0.84, P >0.001; 3-h exercise study, ρ = 0.74, P >0.001). Similar coefficients of correlation were also found for NT-proBNP concentrations at the corresponding time points of the competition races and the present exercise studies: ρ = 0.89 at 30 min and ρ = 0.85 at 3 h after exercise in the 1 h exercise study (P >0.001); ρ = 0.82 at 30 min and ρ = 0.81 at 3 h after exercise in the 3-h exercise study (P >0.001). Differences between resting concentrations and post-exercise NT-proBNP concentration of the competition races and the exercise studies were also significantly related (P >0.001; range of Spearman coefficient of correlation 0.73–0.84). Furthermore, increases in NT-proBNP concentrations of the 3-h exercise study correlated negatively in a moderate fashion with the weekly training volume (hours of training per week versus NT-proBNP 30 min after exercise ρ = − 0.49; hours of training per week versus NT-proBNP 3 h after exercise ρ = − 0.46; P >0.05). No correlations were found among cardiac markers and age or lactate concentrations.
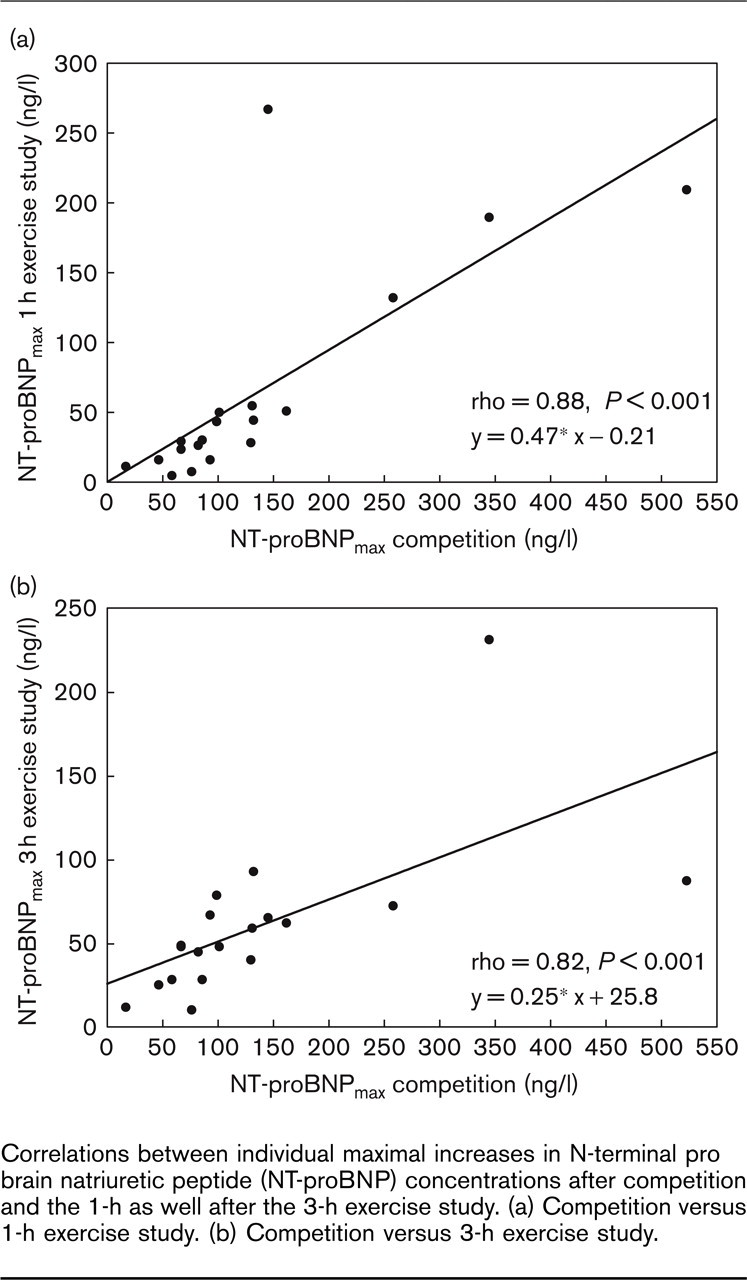
Correlations between individual maximal increases in N-terminal pro brain natriuretic peptide (NT-proBNP) concentrations after competition and the 1-h as well after the 3-h exercise study. (a) Competition versus 1-h exercise study. (b) Competition versus 3-h exercise study.
Creatine kinase and creatine kinase-MB, creatinine, haematocrit and haemoglobin
Creatine Kinase (CK) moderately increased from 51 before to 61 (30 min after) and 60U/l (3h after) in the 1-h exercise study (P>0.01), and from 50 to 64 (30 min after) and 62 U/l (3h after) in the 3-h exercise study (P>0.001). Although CK concentrations after both exercise studies were significantly lower than after competition [P >0.001; median values after competition 58 U/l (before), 121 U/l (30 min after), 183 U/l (3 h after)], significant correlations between the increases in CK concentrations after competition and both exercise studies exist (competition versus 1-h exercise study: ρ = 0.63; competition versus 3-h exercise study ρ = 0.66; all P>0.05). CK-MB remained unchanged. Creatinine concentrations increased from 1.00 ± 0.11 (before) to 1.12 ± 0.13 (30 min after; P >0.001) and 1.06 ± 0.15 mg/dl (3 h after; P = 0.047) in the 1-h exercise study, and from 0.98 ± 0.13 (before), 1.11 ± 0.18 (30-min after; P >0.001) and 1.09 ± 0.19 mg/dl (3h after; P >0.001) in the 3-h exercise study. No correlations were found between CK, CK-MB or creatinine and cTnI, cTnT or NT-proBNP. No significant differences for haematocrit or haemoglobin concentrations were noted between the 1-h and 3-h exercise studies before or after exercise nor between the resting values on the days of competition and both exercise studies.
Echocardiography and magnetic resonance imaging
Echocardiographic parameters of pre and post-exercise examinations are given in Table 3. Heart rate 1 h after exercise was higher than before in both exercise studies (P >0.001). No significant differences were found between pre- and post-exercise fractional shortening or ejection fraction. Furthermore, systolic functions did not differ between athletes with normal and elevated cTnI, cTnT or NT-proBNP concentrations above the URL. Significant differences were found for pre- and post-exercise diastolic function (E and A peak flow velocities, E/A ratio, isovolumetric relaxation time (IVRT)) by transmitral Doppler echocardiography. TDI revealed significant decreases in diastolic parameters and a significant increase in the systolic parameter (Table 3). DE-MRI did not show hyperenhancement in any athlete (Fig. 2).
Magnetic resonance imaging derived left ventricular myocardial mass (LVM) and LVM indexed to the body surface area (LVM 162 ± 22 g; indexed LVM 81 ± 11 g/m2) were negatively correlated to the NT-proBNP concentrations after the 3-h exercise study (ρ = −0.47 and ρ = −0.69, respectively; both P >0.05). No relations were noted for NT-proBNP and LVM or indexed LVM after the 1-h exercise study nor for NT-proBNP and LV end diastolic diameters or volumes.
Discussion
In this study, the relevant findings are as follows. Exercise-induced increases of cardiac troponins after endurance exercise were not reproducible in former troponin-positive healthy endurance athletes. In contrast to cardiac troponins, endurance exercise induced reproducible increases in NT-proBNP. No relations between exercise-induced increases in NT-proBNP and cardiac troponins could be demonstrated, suggesting that different causes lead to increases in cardiac troponins and (NT-pro)BNP in endurance exercise. There was no evidence for an acute or previous myocardial cell damage by a reduced cardiac function in echocardiography or a hyperenhancement in DE-MRI. Therefore, exercise-induced elevations of cardiac troponins and (NT-pro)BNP in healthy athletes seem to be without pathological significance.
Echocardiographic parameters determined 1 h before and 1 h after the 1-h and the 3-h exercise study as well as the resting heart rates during the echocardiographic examinations
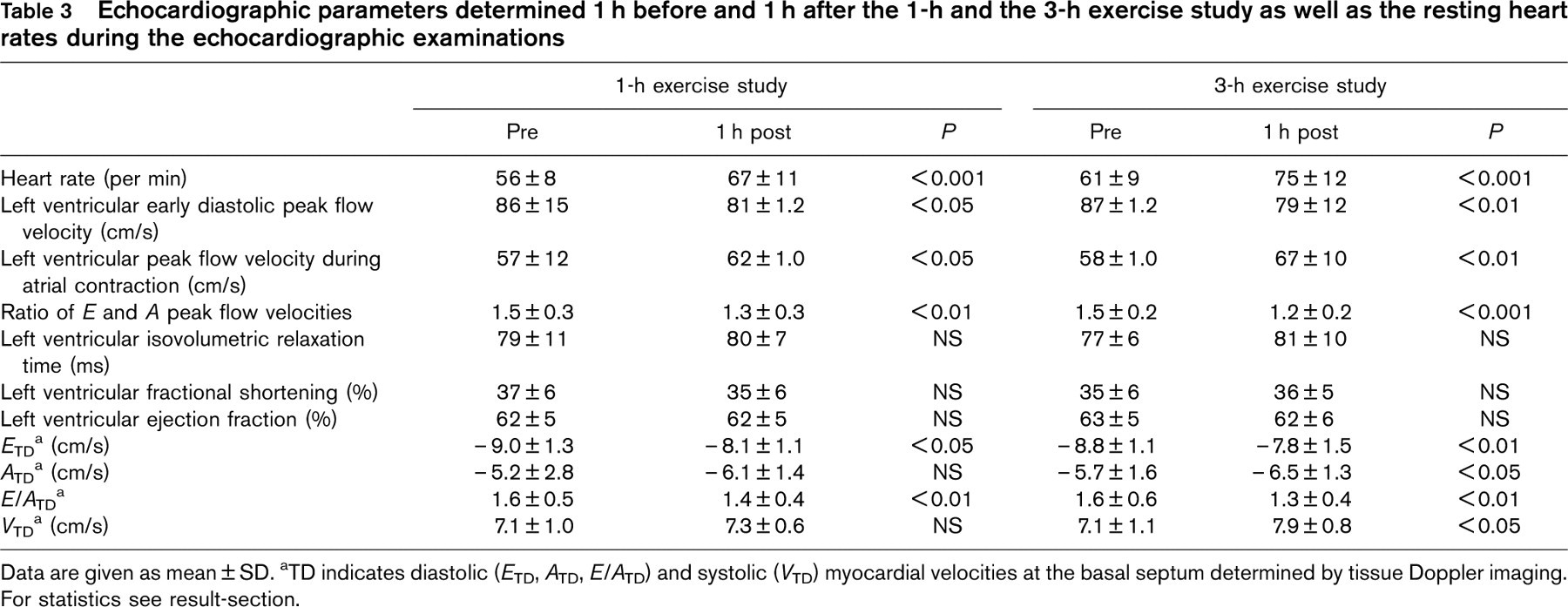
Data are given as mean ± SD. aTD indicates diastolic (E TD, A TD, E/A TD) and systolic (V TD) myocardial velocities at the basal septum determined by tissue Doppler imaging. For statistics see result-section.
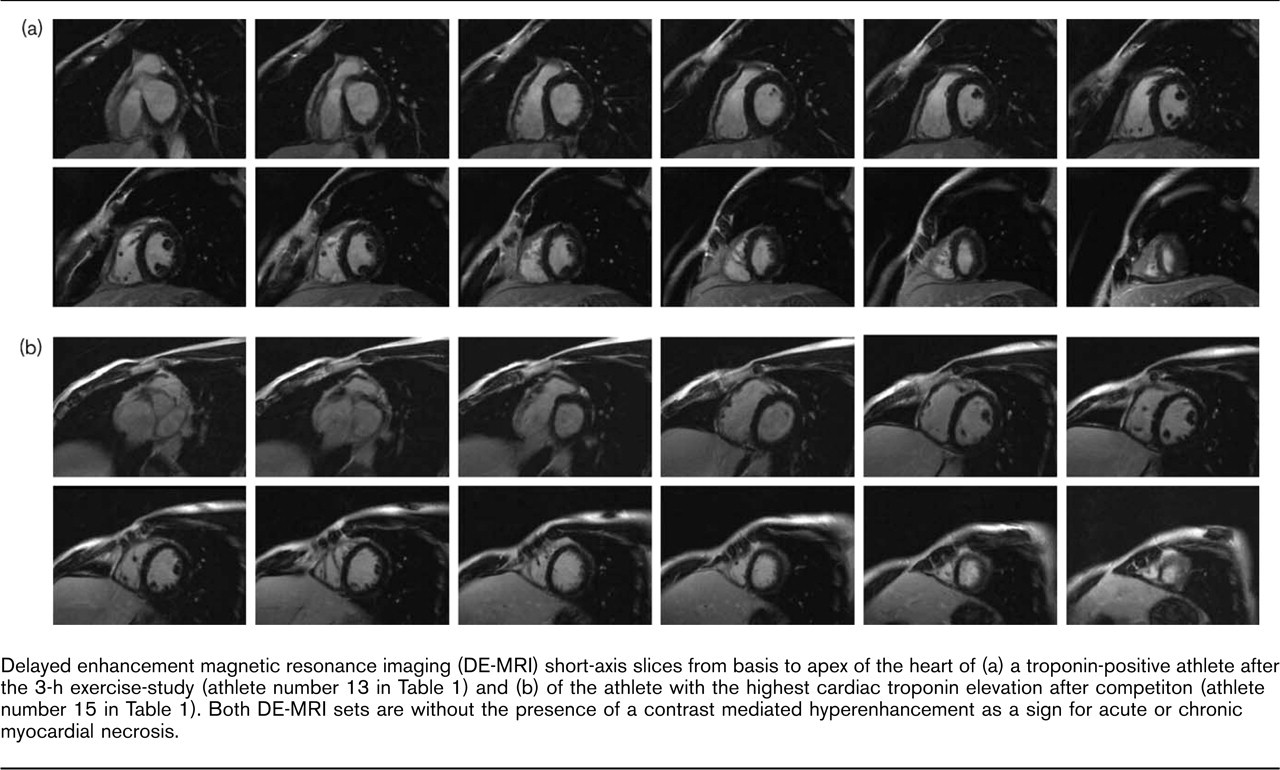
Delayed enhancement magnetic resonance imaging (DE-MRI) short-axis slices from basis to apex of the heart of (a) a troponin-positive athlete after the 3-h exercise-study (athlete number 13 in Table 1) and (b) of the athlete with the highest cardiac troponin elevation after competiton (athlete number 15 in Table 1). Both DE-MRI sets are without the presence of a contrast mediated hyperenhancement as a sign for acute or chronic myocardial necrosis.
Endurance exercise and cardiac markers Cardiac troponins I and T
Although previous studies demonstrated exercise-induced increases of cardiac troponins after prolonged exercise even by use of the newest tests without cross-reactivities with skeletal troponin [21, 22], the clinical significance of exercise-induced increases in cardiac troponins as well as of BNP or NT-proBNP is still an unsolved question. Even though an exercise-induced irreversible myocardial injury, sub-clinical myocardial cell necrosis or damage has been hypothesized [5, 7], there is evidence of a reversible injury of cardiomyocytes in obviously healthy athletes by the normalization of cardiac troponin concentrations within 24 h after exercise [12, 14, 23], leading to the assumption that these increases may be normal in healthy athletes and are without a pathophysiological significance, and also do not have any clinical or athletic consequence [4].
In the present study, only about one-third of athletes with prior elevations of cardiac troponins after competition demonstrated elevations above the URL, with clearly lower concentrations than after competition. In addition, no association between the exercise-induced increases in cardiac troponins after competition and the present exercise studies could be demonstrated. Because of this missing reproducibility, it seems unlikely that unknown or undetected coronary artery or chronic heart disease is the underlying cause of these exercise-inducecd increases. Furthermore, the absence of hyperenhancement in DE-MRI (by which myocardial microinfarction of already approximately 2g can be identified [24]) excludes an exercise-induced myocardial infarction in these athletes, and therefore supports the results of Siegel et al. [12], who also did not find abnormalities in post-race single photon emission computed tomography myocardial imaging in cTnI-positive runners after the Boston marathon. Consequently, other causes than exercise-induced myocardial infarction in healthy athletes have to be considered.
An attractive hypothesis of the exercise-induced release of cardiac troponins in healthy athletes is the reversible release of cytoplasmatic free cTnI and cTnT by leaking across the cardiomyocytes’ membrane due to a transitory increased membrane permeability [14, 25]. As there is a 6–8% free cytosolic pool for cTnT and 3–4% for cTnI, free cytosolic troponin can leak into the circulation when the integrity of the myocytes’ membrane is affected [25]. This transitory membrane leakage would also explain that cTnI remained elevated longer than cTnT after endurance exercise due to the different molecular weight (cTnI approximately 22.5 kD; cTnT approximately 37 kD) in a previous study [14], whereas in the acute phase of myocardial infarction the serum concentration of the cTnI-C complex peaks before free cTnT, which in addition remains elevated longer than the cTnI-C complex [25].
It still remains unclear, however, what affects the cardiomyocytes’ integrity during strenuous endurance exercise, allowing free cytosolic troponin to leak across the membrane. In this and a previous study [13], altogether 34 athletes were examined by non-invasive cardiological tools, and coronary artery disease as the underlying cause of an exercise-induced increase in troponin was found in one athlete only [13]. With regard to the results of Apple et al. [10] and Chen et al. [5], ischemia seems unlikely to be the reason in healthy athletes, as, in contrast to cTnI, ischemia-modified albumin was not elevated after a marathon in 19 healthy runners [10], and histological evidence of ischemic mycardial changes was missing in cTnT positive rats after 5 h of forced swimming [5].
Hence, other explanations than myocardial ischemia inducing cardiomyocyte membrane leakage have to be addressed. Possible explanations may be intracellular calcium alterations [26, 27], effects of free radicals [28], elevated catecholamines, alterations in glucose and fat metabolism or mechanically induced disruptions of the cardiomyocytes’ membrane with rapid resealing [27]. Exercise-induced affections of cardiomyocytes may, however, promote gene expression to improve cellular adaptation and repair mechanisms as well as to induce cellular growth, and in conclusion may also have protective effects after a training period [5, 27]. Nevertheless, further studies are needed to examine these assumptions.
N-terminal pro brain natriuretic peptide
Produced by cardiomyocytes, BNP or NT-proBNP represent myocardial wall stress [1], which is elevated during exercise. As a counter-regulatory hormone, BNP reduces myocardial wall stress by an increase in natriuresis, vasodilation [29] and by sympatho-inhibitory effects [30]. Furthermore, we have postulated previously that BNP acts as a cytoprotective and growth-regulating hormone during and after exercise [14, 31] to protect the myocardium from multifocal cardiac fibrosis [32] and inadequate hypertrophy [33]. Although resting levels and exercise-induced increases in (NT-pro)BNP have been shown to be related to age [14, 34, 35], this relationship could not be demonstrated in the present study. In contrast to cardiac troponins, however, the exercise-induced increase in NT-proBNP, although lower than after competition, was reproducible, and correlated negatively to the amount of training spent per week and to the LVM: athletes with higher training volumes and higher LVM demonstrated minor increases in NT-proBNP, probably due to their better adapted myocardium on endurance exercise bouts. This result therefore further supports the hypothesis of the cytoprotective and growth-regulating properties of BNP in endurance exercise, regulating myocardial adaptation in healthy athletes [31], and has to be differentiated from patho-physiological exercise-induced increases in patients with stable coronary artery disease and exercise-inducible myocardial ischemia [36].
Endurance exercise and cardiac function
Although some athletes presented elevations in cardiac troponins and NT-proBNP after exercise, no associations could be demonstrated with cardiac function. In both exercise studies, the mean left ventricular ejection fraction remained unchanged (even in those athletes with cardiac troponins elevated above the URL), and by TDI a significant increase in the myocardial systolic velocity at the basal septum was measured. These observations further support the assumption that endurance exercise can induce minor elevations of cardiac troponins without representing cardiac damage or necrosis. Nevertheless, Shave and colleagues [9] were able to show that a significant exercise-induced cardiac fatigue will not appear before approximately 5 h of endurance exercise. Hence, the exercise durations in the present study may have been too short to induce a significant decrease of left ventricular systolic function. The concentrations of the cTnT-positive athletes reported by Shave et al. (range: 0.01–0.02 μg/l) [9], however, were exceeded in the present study by three athletes without post-exercise echocardiographic abnormalities. Similar to the results of Shave et al. [9], we also found a decrease in the diastolic function by the E/A-ratio, which has to be attributed (as well as the higher myocardial tissue velocity of the basal septum) to the higher post-exercise heart rate, and therefore is without pathological significance.
Even though previous studies suggested a relationship between exercise-induced cardiac fatigue and exercise-induced cardiac damage [8, 37], the present results do not support this assumption. Considering the missing relations between parameters of cardiac function and cardiac troponins or NT-proBNP, it seems unlikely that increases in these markers after strenuous endurance exercise in healthy athletes indicate myocardial necrosis. Because the increases in cardiac troponins and NT-proBNP in the present study were without evidence of irreversible myocardial damage, they may be a more physiological than pathophysiological phenomenon, inducing and regulating myocardial adaptations on endurance exercise in healthy subjects.
Limitations
Although intensities of 95–100% IAT and 75% IAT were chosen for the 3-h and the 1-h exercise studies to guarantee a sufficient stress for the cardiopulmonary system, the stress during competition has probably been higher. Furthermore, further effects on the cardiopulmonary system within the time interval between competition and the present study can not be excluded, even though athletes’ training habits remained unchanged and signs for blood concentration or dehydration differences between the competition races and the present study were not noted.
Conclusion
Endurance exercise can induce increases in cardiac troponins in healthy endurance athletes under special conditions (especially during endurance competitions), which do not represent irreversible myocardial damage but probably reversible transitory membrane leakage of cardiomyocytes and, therefore, seem to be without pathological significance. The exercise-induced releases of free cytoplasmatic cardiac troponins as well as of BNP may induce cardiomyocytes’ adaptation on endurance exercise and modulate myocardial hypertrophy in healthy athletes. The underlying cellular mechansims of exercise-induced releases in cardiac troponins and (NT-pro)BNP, however, have to be studied in the future to better understand their role in endurance exercise on the athlete's heart.