
Abstract

005: Coffee consumption and risk of total and cardiovascular mortality among patients with type 2 diabetes
S Bidel, G Hu, Q Qiao, P Jousilahti, R Antikainen, J Tuomilehto
National Public Health Institute and University of Helsinki Helsinki, Finland
Context Higher habitual coffee drinking has been associated with a lower risk of developing type 2 diabetes. The relation between coffee consumption and risk of cardiovascular disease (CVD) has been examined in many studies but the issue has remained controversial.
Objective To assess the association between coffee consumption and CVD mortality among patients with type 2 diabetes.
Design, participants and measurement We prospectively followed 3837 randomly ascertained Finnish patients with type 2 diabetes aged 25-74 years with average follow-up of 20.8 years. Coffee consumption and other study parameters were determined at baseline using standardized measurements. The International Classification of Diseases Revisions 8, 9 and 10 were used to identify coronary heart disease (CHD), CVD and stroke cases using computerized record linkage to the national Death Registry. The associations between coffee consumption at baseline and risk of total, CVD, CHD, and stroke mortality were analyzed by using Cox proportional hazards models.
Results During the average follow-up of 20.8 years, 1471 deaths were recorded, of which 909 were coded as CVD, 598 as CHD and 210 as stroke. The multivariate-adjusted hazard ratios (HRs) in participants who drank 0-2, 3-4, 5-6, and ≥ Ý7 cups of coffee daily were 1.00, 0.77 (95% confidence interval [CI], 0.65-0.91), 0.68 (95% CI, 0.58-0.80), 0.70 (95% CI, 0.59-0.85) for total mortality (P < 0.001 for trend), 1.00, 0.79 (95% CI, 0.64-0.97), 0.70 (95% CI, 0.57-0.86), 0.71 (95% CI, 0.56-0.90) for CVD mortality (P = 0.006 for trend), 1.00, 0.78 (95% CI, 0.60-1.01), 0.70 (95% CI, 0.54-0.90), 0.63 (95% CI, 0.47-0.84) for CHD mortality (P = 0.014 for trend), and 1.00, 0.77 (95% CI, 0.50-1.19), 0.64 (95% CI, 0.41-0.99), 0.90 (95% CI, 0.56-1.45) for stroke mortality (P = 0.12 for trend), respectively.
Conclusion In this large prospective study we found that in type 2 diabetic patients coffee drinking is associated with reduced total, CVD and CHD mortality.
013: Association between intelligence, socio-economic position and coronary heart disease mortality: a population-based cohort study of 682,361 Swedish men
Karri Silventoinen, Karin Modig, Per Tynelius, Finn Rasmussen
University of Helsinki, Department of Public Health, Finland
Socio-economic inequalities in coronary heart disease (CHD) are well described but still not well understood. Associations between intelligence (IQ), social position and CHD mortality were explored in 682,361 Swedish men born 1951-1965 who participated in military conscription examination at age 18. IQ, systolic and diastolic blood pressures and BMI were measured at conscription and data on own and parental education and socio-economic position were derived from censuses in 1970, 1980 and 1990. Mortality data were obtained from the Swedish Cause of Death Register to 31st December 2001 (737 CHD deaths). Cox regression and conditional logistic regression models were used. IQ was inversely associated with CHD (HR 0.82 95% CI 0.79, 0.85). Adjustment for other risk factors attenuated this association which, however, remained strong (HR 0.92 95% CI 0.89, 0.96). The socioeconomic inequalities in CHD were weakened but not extinguished when IQ was adjusted for. The associations between IQ and CHD were of similar strengths within all socio-economic categories and also found within 215 brother pairs discordant for CHD and IQ (OR 0.76 95% CI 0.58, 1.00). IQ and social position are independently associated with CHD risk. Health education messages should be tailored according to intellectual performance of the recipients.
035: Left ventricular hypertrophy, hypertension and obesity in Tallinn population
T Shipilova, I Pshenichnikov, J Kaik, J Abina, E Solodkaya, M Saava, A Udras
Estonian Institute of Cardiology, Estonia
Objective Between 1993 and 1999 some European countries, including Estonia, showed a rapid increase in cardiovascular disease mortality. It is time to focus on public health and evaluate relationships between hypertension, obesity and left ventricular hypertrophy (LVH) in Tallinn-the capital of Estonia.
Design and methods In the framework of a population study for cardiovascular risk factors, 1119 participants (pts) aged 35 to 59, were examined, 325 men and 401 women of them underwent echocardiography. LVH was classified on the normal limits for left ventricular mass index (LVMI) < 150g/m2 for men and < 120g/m2 for women and on the relative wall thickness < 0.45 as concentric hypertrophy (CH), eccentric hypertrophy (EH), concentric remodelling (CR) and normal geometry (N). Obesity was defined by body mass index (BMI) ≥ 30 kg/m2.
Results Only 60% of men and 57.1% of women did not have obesity and hypertension. Most of them had N: 97.4% of men and 63.3% of women. Obesity was found in 9.2% of men and 15.7% of women (P > 0.05). Obese men had N only, but obese women had EH (25.4%), CR (12.7%) and N (61.9%). Hypertension was found in 15.4% of men and 12.7% of women (P > 0.05). The prevalence of combination obesity with hypertension was similar in men and women, 15.4% and 14.5%, respectively. Hypertensive women without obesity and hypertensive women with obesity had CH in 29.4% vs 32.8% of cases, respectively, EH in 27.5% vs 20.7%, CR in 9.8% vs 10.3%, N in 33.3% vs 36.2%. Hypertensive men without obesity compared hypertensive men with obesity had significantly rarely CH and EH: in 12% vs 30% and in 4% vs 16% of cases, respectively. LVMI by multiple regression was significantly positive related to systolic blood pressure (β = 0.24 SE = 0.03 R2 = 19.2), but was not significantly assiociated with BMI.
Conclusion The prevalence of obesity and hypertension was high in each gender. LVMI was significantly associated with systolic blood pressure, not with BMI.
040: Associations between dimensions of job stress and biomarkers of inflammation and infection
E Clays, D De Bacquer, J Delanghe, L Van Renterghem, F Leynen, M Kornitzer, G De Backer
Department of Public Health, Ghent University, Belgium
Objective Chronic inflammation and infection have recently been suggested as possible mediating mechanisms in the relation between job stress and cardiovascular disease. The objective of this study is to examine associations between dimensions of job stress and indicators of chronic inflammation and infection.
Methods Within a subsample from the BELSTRESS study of 892 male subjects free of cardiovascular disease, dimensions of job stress from the Job Demand-Control-Support model were related to bio-markers of inflammation-plasma fibrinogen concentrations, high sensitivity C-reactive protein (CRP) and serum amyloid A (SAA), and infection, titres against Chlamydia pneumoniae (CP), Cytomegalovirus (CMV) and Helicobacter pylori (HP).
Results A negative association was found between job control and plasma fibrinogen concentration, independent from age, education, occupation, body mass index, smoking, alcohol consumption and use of lipid lowering and anti-hypertensive medication. Perceived job stress did not correlate with CRP and SAA concentrations, or with titres against CMV, CP and HP.
Conclusions Results confirm previous findings regarding elevated plasma fibrinogen and low job control.
097: Baseline characteristics, management and in-hospital mortality of patients hospitalized with acute coronary syndromes in Greece; the GREECS study
G Kourlaba, C Pitsavos, D Panagiotakos, S Arapi, A Antonoulas, G Papanagnou, S Kosmopoulou, K Massoura, C Stefanadis; for the GREECS Study Investigators
First Cardiology Clinic, School of Medicine, University of Athens, Greece
Objective In this work we present the baseline characteristics, the management and the in-hospital outcome of people hospitalized with all clinical presentations of Acute Coronary Syndromes (ACS).
Methods A sample of 6 hospitals located in Greek urban and rural regions was selected. Almost all consecutive admissions due to ACS, from October 2003 to September 2004, were recorded. Socio-demographic, clinical, dietary, psychological and other lifestyle characteristics were recorded, too.
Results 2172 patients were included in the study (76% were men and 24% women). 38% had ST-segment elevations, 27% had non-ST-segment elevations, and the rest of them had other electrocardiographic changes. According to the discharge diagnosis, 35%, 32% and 33% of patients were diagnosed as having unstable angina (UA), non-Q-wave MI and Q-wave MI, respectively. The most common discharged diagnosis for men was Q-wave MI, while for women it was unstable angina. Male patients were younger than female patients (64 ± 13 and 71 ± 12 years for men and women, respectively). Patients with UA were more likely to have hypertension, diabetes and history of coronary heart disease as compared to those who had Q-wave MI. Moreover, UA patients tented to follow a more typical Mediterranean diet compared to MI patients. The median (and 25th, 75th percentiles) time between the overt of symptoms and the time medical care was sought was 4 (2, 10) hours. 60% of patients with ST-elevation received trombolytic therapy. The crude annual incidence rate was 22.6 per 10,000 (34 and 10.9 per 10,000 men and women, respectively) and the highest frequency of events was observed in winter. The in-hospital mortality rate was 4.3% (6.3% and 3.6% for women and men, respectively).
Conclusion This study demonstrates current information about the epidemiology of patients who suffer from ACS, in Greece.
098: Prevalence of cardiovascular risk factors in Indian patients undergoing coronary artery bypass surgery
RR Kasliwal, Manish Bansal, Sweta Agrawal, Ambar Kulshreshtha, Naresh Trehan
Escorts Heart Institute and Research Centre, New Delhi, India
Background Conventional cardiovascular risk factors (CVRFs) are known to influence short-term and long-term outcome following coronary artery bypass graft surgery (CABG). There has been recent increase in prevalence of CVRFs in general population in India but such information in patients undergoing CABG is not available.
Methods and results 1000 consecutive patients undergoing elective CABG were included and information about major CVRFs was collected in them. Mean age of the patients was 59.73 ± 9.5 years and 88.4% patients were males. 50.8% patients had BMI > 25.0 kg/m2 and 75.2% had BMI > 23.0 kg/m2 (cut-off suggested for definition of overweight in Indian population). Diabetes mellitus (DM) was present in 47.5%, hypertension (HT) in 70.9% and dyslipidemia in 85.6% patients. 23.3% patients had LDL > 100mg/dl, 72.5% had low HDL and 37.0% patients had elevated triglycerides. 19.9% patients had family history of premature CAD and 54.5% had at least one family member having CAD (irrespective of the age of onset). 9.4% patients were current smokers and another 30.2% had history of smoking in the preceding one year. 95.9% of all the patients had at least one of the 5 major CVRFs and only 4.1% patients were free of all these risk factors. Sixty-one of the 1000 patients (6.1%) were younger than 45.0 years of age. As compared to older patients, dyslipidemia, family history of premature CAD and smoking were commoner in patients < 45 years of age. In contrast, DM and HT were more prevalent in the older individuals. No in-hospital mortality was observed in the study group.
Conclusions The present study showed high prevalence of most of the conventional CVRFs, esp. DM, HT and dyslipidemia in Indian population undergoing CABG. In view of the worse prognosis seen with higher prevalence of CVRFs, the findings of the present study are really worrisome and mandate greater need to institute aggressive risk factor modification in patients undergoing CABG as well as in general population.
100: Age-related differences in baseline characteristics and inhospital mortality of patients with non-q-wave myocardial infarction and unstable angina; the GREECS study
G Kourlaba, C Pitsavos, D Panagiotakos, S Arapi, A Antonoulas, S Kosmopoulou, G Papanagnou, K Massoura, C Stefanadis; for the GREECS Study Investigators
First Cardiology Clinic, School of Medicine, University of Athens, Greece
Objectives In this work we assessed the differences on baseline characteristics of patients with non-Q-MI and UA according to their age, as well as the influence of those patients' age on the in-hospital mortality.
Methods A sample of 6 hospitals located in Greek urban and rural regions was selected and we recorded almost all admissions due to ACS, from October 2003 to September 2004. 2172 patients were enrolled in the study. Of them, 1463 were presented with non-Q-MI and UA (73% were men and 27% women). Socio-demographic, clinical, dietary and other lifestyle characteristics was recorded. Age was divided into 5 groups: younger than 45 years, 45-54, 55-64, 65-74 and older than 75 years.
Results The mean ± standard deviation age of patients with non-Q-MI and UA was 67 ± 12 years (66 ± 13 years for men and 77 ± 11 years for women). Elderly patients (age > 65 years) were more likely to be women, to have history of hypertension, diabetes mellitus, coronary heart disease and renal failure, while smoking, exposure to environmental smoke, obesity and hypercholesterolaemia were more common among younger patients. Pre-hospital delay in seeking medical care was significantly higher in older patients. In-hospital mortality rate was higher in patients ≥ 75 years (5%), while 5 years increment in age was associated with almost 30% higher odds of dying during hospitalization (OR = 1.05, 95% CI: 1.01-1.08). In-hospital mortality continues to increase with age even after adjustment for potential confounders.
Conclusions We demonstrated that although the in-hospital mortality rate is low in patients with non-Q-MI or UA, elder patients continue to be in higher risk of dying compared to younger patients. Therefore, effective therapies must be provided to those patients.
101: Characteristics, management and in-hospital mortality of non-insulin-, insulin-treated- and non-diabetic patients with an acute coronary syndrome: the GREECS study
G Kourlaba, C Pitsavos, D Panagiotakos, G Papanagnou, S Arapi, Y Mantas, K Massoura
C Stefanadis; for the GREECS Study Investigators First Cardiology Clinic, School of Medicine, University of Athens, Greece
Objectives In this work we sought to describe the baseline characteristics, management and in-hospital mortality of non-insulin-, insulin-treated- and non- diabetic patients hospitalized with all clinical presentations of Acute Coronary Syndromes (ACS).
Methods We recorded all consecutive patients admitted due to ACS at 6 hospitals located in Greek urban and rural regions, from October 2003 to September 2004. 2172 patients were included in the study (76% were men and 24% women). Socio-demographic, clinical, dietary and other lifestyle characteristics was recorded.
Results Approximately 1 in 3 patients admitted at the hospital with ACS had history of diabetes. Patients with diabetes mellitus were more likely to be older, women and to have history of coronary heart disease, hypertension and renal failure. Diabetics (insulin and non-insulin treated) sought medical care later than non-diabetics, but the difference was not statistically significant. Among patients with ST-segment elevation, diabetics and especially those treated with insulin were less likely to receive fibrinolytic agents compared to non-diabetics (59%, 50% and 41% for non-diabetics, non-insulin-treated and insulin-treated, respectively, P = 0.05). The in-hospital mortality was higher among diabetics receiving insulin (8%), followed by those not receiving insulin (6%) and lowest in non-diabetics (2%, P < 0.001). In a multivariate analysis only insulin-treated diabetics had an increased mortality rate compared to non-diabetics (OR = 5.6, 95% CI: 1.63-19.02).
Conclusions Our findings confirm that diabetics have worse prognosis after an ACS compared to non-diabetics, demonstrated by previous studies. In particular, insulin-treated diabetes is an independent risk factor for death after ACS. Therefore, more effective medications and interventions must be used in diabetics who develop ACS, in order for in-hospital mortality to be reduced.
103: Characteristics, management and in-hospital outcome of smokers and non-smokers with acute coronary syndromes: the GREECS study
G Kourlaba, C Pitsavos, D Panagiotakos, S Arapi, Y Kogias, Y Mantas, G Papanagnou, C Stefanadis; for the GREECS Study Investigators First Cardiology Clinic
School of Medicine, University of Athens, Greece
Objective In this work we investigate the impact of cigarette smoking on the management and in-hospital mortality of patients hospitalized with all clinical presentations of Acute Coronary Syndromes (ACS).
Methods Between October 2003 and September 2004, we recorder almost all consecutive patients presented with ACS at a sample of 6 hospitals located in Greek urban and rural regions. 2172 patients were enrolled in the study (76% were men and 24% women). Socio-demographic, clinical, dietary and other lifestyle characteristics, as well as the management and the in-hospital outcome of patients were recorded. Based on smoking habits, patients divided into never, former and current smokers.
Results 32%, 35% and 33% of patients declared that were current, former and never smokers, respectively. Current smokers were more likely to suffer from ST-segment elevation MI, while never smokers were more likely to suffer from unstable angina (UA). Moreover, current smokers were younger, less likely to have history of hypertension, diabetes mellitus and coronary heart disease, as well as they experienced more prolonged delay in seeking medical care after the onset of symptoms compared to former and never smokers. Thrombolytic therapy was more likely to be used in current smokers. Unadjusted inhospital mortality was higher in never smokers (5.5%, 2.5% and 3% in never, former and current smokers, respectively, P < 0.001). However, no statistically significant difference on in-hospital mortality was observed among three subgroups of smokers, after controlling only for age differences among these groups.
Conclusion We revealed that age accounted for much of seemingly improved outcome of current smokers compared to never smokers.
106: The evaluation of lipid disorders in three rural communities from Romania
P Kikeli, Z Preg, M Hubatsch, M Fejer
University of Medicine Targu Mures-Cardiac Rehabilitation Clinic, Romania
Background Lipid disorders are major correctable risk factors. There is few data for the prevalce of lipid disorders in Romanian rural communities and the prophylactic measures implemented for their correction. We studied the prevalence of lipid disorders in three rural communities from Mures County Romania.
Materials and methods The study is based on a complex evaluation of 1371 persons, in a cross sectional screening. Sex distribution of the studied population: 894 female average age 52.7 years and 477 male average age 53.6 years. There was evaluated the need for therapeutic lifestyle changes and drug treatment according to National Cholesterol Education Programme Adult Treatment Panel III.
Results The prevalence of hypercholesterolemia (TC > 200) was 48.8%, high LDL levels (> 130) 66.7%, low HDL levels (< 40) 7.3%. The prevalence of hypertriglyceridaemia (> 200) was 13.3%. The prevalence of hypercholesterolaemia and hypertriglyceridaemia rises with ageing. And is correlated with the body mass index. The prevalence of the metabolic sydrome was 19.7% affecting predominently middle aged women.
Conclusions 1. 24.7% of the studied population has already developed CHD, or CHD equivalent (diabetes mellitus, framingham risk > 20%) and needs aggressive risk control. 2. 48.9% of the population has an elevated total cholesterol level, 66.7% has high (> 130) LDL, 7.4% has low (< 40) HDL, 13.3% high (> 200) triglycerid levels. 3. The prevalence of hypercholesterolaemia significantly increases after age 29 years, and is associated with obesity and glucose intolerance. 4. The prevalence of the metabolic syndrome is 19.7%, with maximum level in 50-59 years old women. 5. Drug treatment is indicated in 42.3% of the studied population. Only a few persons were receiveing cholesterol lowering medication. 6. Therapeutic lifestyle changes are indicated in 62.1% of the studied population. 7. Population based strategies must be applied in this population at high risk.
110: Predictive potential of mild changes in thyroid status on cardiovascular risk profile
O Mayer Jr., J Hrbková, J Šimon, R Pikner
2nd Dept. of Internal Medicine, Medical Faculty Pilsen, Czech Republic
Background Overt hypothyroidism was reported to increase the cardiovascular risk, notably through its effect on lipid parameters. In the present study we aimed, whether also mild changes in thyroid status (subclinical hypothyroidism or high-normal thyroid stimulating hormone (TSH)) predict increased cardiovascular risk.
Methods 453 subjects without overt hypo- or hyperthyroidism (249 males and 204 females, mean age 52.5 ± 0.39) from population-based study PILS II were included into a prospective study, with average time of follow-up 8.4 years. Predictive potential of subclinical hypothyroidism (ie. TSH > 4.5 mU/l) and high-normal TSH (ie. TSH 3-4.5 mU/l) was tested by multiple logistic step-wise regression, following variables were included into full model: age, gender, current smoking, new clinical coronary heart disease, obesity (body mass index ≥ 30), increased waist circumference (≥ 102 cm in males or ≥ 88 cm in females), hypertension (blood pressure ≥ 140/90 or antihypertensive treatment), hypercholesterolemia (total cholesterol ≥ 7 or lipid-lowering treatment), hypertriglyceridemia (triglycerides ≥ 2), impaired fasting glucose or diabetes (glucose ≥ 6.5 or antidiabetics) and overt hypothyroidism (free thyroxine levels < 9 or L-thyroxine substitution).
Results Subclinical hypothyroidism significantly predict future overt hypothyroidism [odds ratio 32.6 (4.72-224.73)] and hypertriglyceridemia [6.74(1.52-29.9)], while high-normal TSH hypercholesterolemia [2.02 (1.10-3.68)] and overt hypothyroidism again [4.96 (1.45-16.96)]; also if adjusted for age, gender and other above mentioned independent variables.
Conclusions Both subclinical hypothyroidism and high-normal TSH significantly increased risk of future overt hypothyroidism and concomitant lipid disorders.
(Supported by the Ministry of Health CZ, grant IGA 7534-3).
111: Incidence of CHD and stroke in germany from registers and estimated by a who method using national statistics
J Heidrich, J Wellmann, PU Heuschmann, U Keil
Institute of Epidemiology and Social Medicine, University of Muenster, Germany
Background Incidence of coronary heart disease (CHD) and stroke can be estimated from local, population-based registers. It is unclear, to what extent local register data are applicable on a nationwide level. Therefore, we compared German register data with estimates derived with WHO Global Burden of Disease (GBD) method.
Methods Incidence of CHD and stroke was computed with the GBD method using official German mortality statistics and prevalences from the German national health survey. Results were compared to estimates from the MONICA/KORA Augsburg register (CHD) and the Erlangen Stroke Project in southern Germany.
Results GBD estimates and register data showed good agreement: CHD (age group 25-74 years) 155,862 (GBD) versus 159,245 (register) and stroke (all ages) 157,104 versus 167,892 incident cases per year. CHD incidence among all age groups was estimated with the GBD method to be 250,000 per year (no register data available). CHD incidence in men and stroke incidence in women were underestimated with the GBD method as compared to register data.
Conclusions GBD method is a useful tool to estimate incidence of CHD and stroke. The computed estimates may be seen as lower limit for incidence data. Differences between GBD estimates and register data are discussed.
114: Characteristics, treatments and outcomes of patients with acute myocardial infarction
KD Theodoridis, DS Dourtsiou, DA Labrou, FL Borghi, ES Karras, GA Savvopoulou, NL Papadopoulou, EO Koutsogiannis, EA Panagiotidou, KA Gotsis
Department of Cardiology, General Hospital of Komotini, Greece
Aim To evaluate the epidemiological and clinical features of patients with AMI in order to achieve both optimal planning of prevention and its effective management.
Methods We studied 210 patients-148 males (M) aged 67.8 ± 10.6 and 62 females (F) aged 74.7 ± 12.2 years old-admitted with AMI. Detailed medical history was taken, complete biochemical control was made and height, weight, waist circumference were measured. The exact time of symptoms onset, call for help, arrival to emergency room and initiation of thrombolytic therapy was noted. Furthermore, medication at admission, during hospitalization and at discharge was registered, as well as complications.
Results The initial diagnosis was STE in 55.2%, ST depression (STd) 19%, non-specific ST changes(LBBB, RBBB, pacing, LVH) 22.9%, normal ECG 2.9%. The discarge diagnosis was Q-wave MI in 49%, non-Q wave MI 51%. Use of heparins, anti-thrombotic drugs, GPIIb-IIIa inhibitors, b-blockers, ACEI/ATII blockers and statins was 99%, 96.6%, 28.8%, 85.1%, 80.2% and 63.3% respectively. Among patients with STEMI, 43.7% received fibrinolytic therapy. The mean time from symptom onset to arrival was 242 min (62% of patients within 3h) and from arrival to fibrinolysis was 32 min. In-hospital mortality for patients with STE was 8.6%, for patients with STd 12.5% and for them with non specific ST-T changes 4.2%. Patients with STd had the worst baseline demographic and clinical characteristics: they were older, had history of heart disease (prior MI, revascularization, HF, permanent pacemaker as well as other co-morbid conditions: hypertension, diabetes, renal failure).
Conclusions The important delay of presentation at the emergency room is due to the significant delay of call for help, which is almost double for NSTEMI patients. Mortality was the same for M and F. More attention should be focused on the patients with worse demographic and clinical features, who were treated by non cardiologists and medication at admission was in discordance to existing guidelines.
127: Prevalence and treatment of hypertension in polish population
Maria Polakowska, Walerian Piotrowski; WOBASZ Study
National Institute of Cardiology, Poland
Background Hypertension is one of many frequent circulatory system diseases. Unfortunately many people do not know about disease and if they know they do not treat it.
Aim Estimation of frequency, efficiency and manner of treatment of hypertension in representative sample of Polish population.
Materials and methods Examination of 13545 people: 6392 men and 7153 women in age 20-74, randomly selected from Polish population. Each person had have done 3 measurements of blood pressure in sitting position. The average value from the second and the third measurements of blood pressure was taken. Data of treatment was taken from the patient's medical history. Hypertension is defined as blood pressure ≥ 140/90 mmHg and/or on treatment.
Results Average of blood pressure was 137.6/83.9 mmHg in men and 129.7/81.2 mmHg in women. Prevalence of hypertension was higher in men (42%) than in women (33%). Prevalence of hypertension increases with age. Large differentiation in regions of Poland was observed. 44% of men and 67% of women were treated. Hypertension was treated correctly only in 10% of men and 16% of women. The most often used drug was ACE-67% in men and 60% in women. Beta-blockers were used by 45% of men and by 50% of women, Ca-blockers-by 27% of men and by 24% of women, diuretics adequately-by 32% and 34%, ATII blockers-by 0.4% and by 0.2%, other drug-by 2% and 3%. Monotherapy was the most often used-in 46% of men and in 48% of women.
Conclusions Hypertension is qn often found disease in the Polish population. Efficacious treatment of hypertension was very low.
135: Association between plasma homocysteine levels and coronary artery disease: a population-based study in northern Greece
A Boufidou, A Makedou, D Adamidis, H Karvounis, K Makedou, J Gourassas, H Kesidis, C Papadopoulos, G Parharidis, G Louridas
Department of Cardiology, AHEPA University Hospital, Aristotle University of Thessaloniki, Greece
Objective Elevated plasma total homocysteine (tHcy) levels constitute a risk factor for coronary artery disease (CAD). We prospectively examined the association of fasting tHcy levels in patients in Northern Greece who had established CAD.
Patients and methods Plasma fasting tHcy levels were measured in 42 patients with angiographically documented CAD and compared to 42 age-, sex-, BMI- and smoking habit-matched control subjects. We also determined the plasma vitamin B12, folic acid and lipoprotein levels in all patients and controls. Conventional risk factors for CAD were also estimated.
Results In a univariate analysis, tHcy (mmol/l) levels were higher in patients compared to controls almost reaching statistical significance (13 (7-41) vs 11.3 (4-39); P = 0.07). Multivariate analysis of conventional risk factors showed that tHcy levels were not an independent risk factor for CAD. However, tHcy levels were significantly higher in patients with a previous history of myocardial infarction compared to patients without such a history and to controls (15 (8.8-29) vs 11.7 (7-41); P = 0.007 and 15 (8.8-29) vs 11.3 (4-39); P = 0.002, respectively). Hyperhomocysteinaemia (> 15mmol/l) was detected in 35.7% of patients and 11.9% of controls (P < 0.05).
Conclusions In Northern Greece, plasma tHcy levels may not be an independent risk factor for CAD in patients with angiographically documented CAD. However, patients with CAD have a trend towards higher tHcy levels. Additionally, plasma tHcy levels may be associated with the development of myocardial infarction.
140: The impact of initial level of systolic blood pressure on the in-hospital mortality of patients admitted with acute coronary syndromes; the GREECS study
G Kourlaba, C Pitsavos, D Panagiotakos, S Arapi, S Zombolos, Y Mantas, G Giannopoulos, C Stefanadis; for the GREECS Study Investigators
First Cardiology Clinic, School of Medicine, University of Athens, Greece
Objective In this work we sought to determine whether the levels of systolic blood pressure (sbp) at the admission is an independent prognostic factor for in-hospital mortality of patients hospitalized with all clinical presentations of Acute Coronary Syndromes (ACS).
Methods From October 2003 to September 2004, a sample of 6 hospitals located in several urban and rural Greek regions was selected, and almost all patients due to ACS were enrolled into the study (2172 patients were included in the study; 76% were men and 24% women). We recorded socio-demographic, clinical, dietary and other lifestyle characteristics, as well as the management and the in-hospital outcome of all patients, too.
Results The sbp was lower among patients presented at the hospital with ST-segment elevation (132.8 ± 26.7, 140.8 ± 25.1 and 140.5 ± 26.7 mm Hg for patients with ST-segment elevation, non-ST-segment elevation and unstable angina, respectively, P < 0.001). Female, hypertensive, diabetics, dyslipidemic and older patients had higher level of sbp compared to respective groups. Moreover, sbp of patients who received thrombolytic agents was lower than that of those who did not receive. 10 mm Hg increment in the sbp was associated with almost 20% lower likelihood of dying during hospitalization (odds ratio = 0.80, 95% CI 0.73 to 0.90). After adjustment for potential confounders, initial level of sbp continued to be statistically significant predictor for inhospital mortality (odds ratio = 0.70, 95% CI 0.54 to 0.91).
Conclusion The results of this work demonstrate that initial level of systolic blood pressure is an independent predictor for in-hospital mortality of patients with ACS.
141: Factors associated with the lesser use of thrombolytic therapy among patients with acute myocardial infarction. The impact of patients' sex and age; the GREECS study
G Kourlaba, C Pitsavos, D Panagiotakos, S Zombolos, G Koudounis, Y Mantas, G Giannopoulos, C Stefanadis; for the GREECS Study Investigators
First Cardiology Clinic, School of Medicine, University of Athens, Greece
Objectives We sought to investigate which baseline characteristics of patients with ST-segment elevation myocardial infarction (MI) affect the eligibility of thrombolytic therapy and especially the influence of those patients' sex and age on the use of fibrinolytic agents.
Methods A sample of 6 hospitals located in Greek urban and rural regions was selected and we recorded almost all admissions due to ACS, from October 2003 to September 2004. 2172 patients were included in the study. Of them, 641 were presented with ST-segment elevation MI (82% were men and 18% women). Socio-demographic, clinical, dietary, other lifestyle characteristics and the management of all patients was recorded.
Results Among 641, only 365 (57%) received thrombolytic therapy. Smokers, those patients without history of coronary heart disease, diabetes mellitus and renal failure as well as patients admitted at the hospital within 2 first hours from the onset of symptoms were more likely to receive fibrinolytic agents. The use of thrombolysis was almost 65% and 50% less common among patients ≥ 75 years compared to those < 75 years (OR = 0.34, 95% CI: 1.31-2.97) and among women compared to men (OR = 0.5, 95% CI: 0.33-0.76), respectively. Stratified analysis by pre-hospital delay time (≤ 2 h and > 2 h after the onset of symptoms), revealed that it is significantly less likely for older patients and women to receive thrombolytic agents only among those who delay seeking medical care more than 2 h after the onset of symptoms. After controlling for potential confounders, sex does not continue to be significant predictor for lesser use of fibrinolytic agents, while age seems to be an independent prognostic factor for the administration of thrombolysis.
Conclusions We demonstrated that the advanced age is associated with underuse of fibrinolytic agents, while older age and the more prolonged pre-hospital delay of women may account for the lesser use of thrombolytic therapy among female patients with AMI.
148: Greater adherence to the mediterranean diet attenuates the risk of 28-day events in open-heart surgery patients
Demosthenes Panagiotakos, Olga Vassilaki, Athanasios Manginas, Panagiotis Karioffylis, Maria Kotiou, Peter Alivizatos, Dennis Cokkinos
1st Cardiology Department, Onassis Cardiac Surgery Center, Athens, Greece
Background The aim of this work was to evaluate the effect of the adoption of this dietary pattern on the short-term (28-day) prognosis of patients who had an open-heart surgery.
Methods We enrolled 61 consecutive patients undergoing scheduled open-heart surgery; 46 were men (60 ± 13 years) and 15 were women (67 ± 11 years). The consumption of various foods was investigated as an average per week, during the past year, using a validated, semiquantitative, food-frequency questionnaire. Then a special diet score (range 0-55) was calculated that assessed adherence to the Mediterranean dietary pattern. Multiple logistic regression models were used to assess the role of diet on the outcome (death, re-hospitalization), after adjusting for various potential confounders.
Results During the 28-days following hospitalization 8 (13%) patients had an event (2 or 3.3% died and 6 or 10% were hospitalized due to CVD). Diet score was lower in patients who had an event compared to the others (24 ± 5 vs. 33 ± 4, P = 0.01). Multi-adjusted analysis reveled that adoption of Mediterranean diet (upper tertile of the score) was associated with 24% lower likelihood of having a recurrent event (relative risk = 0.46, P < 0.01), compared to a “westernized dietary pattern”. Moderate alcohol drinking was associated with 65% (relative risk= 0.35, P < 0.05, attributable risk= 53%) lower risk of death or re-hospitalization during the first 28-days following open heart surgery, while increased drinking was associated with 4-fold higher risk of events, irrespective of age, sex and several other potential confounders. Furthermore, roughly, one third of these cardiac events could be prevented through the adoption of this dietary pattern (attributable risk= 33%).
Conclusion The present study demonstrated that a background diet close to the Mediterranean dietary pattern seems to influence more profoundly cardiovascular risk in patients who had a cardiac surgery.
160: Age-associated trends in the prevalence of the metabolic syndrome and its components: effects of gender. The progenia study
Angelo Scuteri, Marco Orru, SS Najjar, Manuela Uda, Antonio Cao, EG Lakatta
1 Geriatria INRCA Rome(I), 2 INN-CNR Cagliari(I), 3 LCS- NIA-NIH Baltimore (USA)
To investigate the effect of sex on the age associated trend in the prevalence of the MetS and on the specific clustering of altered components of the MetS in a large population from Sardinia, Italy.
The ProgeNIA Study was conceived as a study of a Sardinian founder population investigating the genetics of complex traits/phenotypes, including CV risk factors and arterial properties. 6,148 subjects were enrolled (age range 14-102). According to the ATP III criteria, MetS was defined as the presence of at least 3 of the following alterations: abdominal obesity (W), hypertriglyceridemia (T), low HDL (H), elevated blood pressure (B), and impaired fasting glucose or diabetes (G). Age groups were classified as: < 35, 35-19, 50-64,¡ Ý65 yrs.
MetS prevalence was 7.1% in M (n = 185) and 6.1% in F (n = 214) and progressively increased with age in both M and F (from ∼1% in subjects < 35 yrs to 15.5% and 20%, respectively in M and F > 65 yrs). In M the prevalence of B and W was similar across all age groups, whereas H was more common in younger and G in older groups. In F, the prevalence of W, the most commonly altered component, was similar across age groups; the prevalence of B and G increased with age, whereas the prevalence of H was higher in younger group and decreased after age 50. Clustering of T-B-W (approximately 20%) and G-B-W (approximately 29%) showed similar frequency amongst subjects with the MetS in both M and F. However, G-T-B(−W) was observed in 27% of M but only in 6% of F with the MetS, whereas G-H-W(−B) was observed in 9% of F but only in 2% of M with the MetS, and H-B-W in 16% of F but only in 4.3% of M with the MetS.
The prevalence of the MetS increases with aging in both M and F. However, the specific clustering of altered components of the MetS differs by age and sex. We are planning to evaluate whether specific clusters carry the same risk for CVevents in M and F, whether they are attributable to similar mechanisms, and whether they aggregate in families.
175: Absence of metabolic syndrome defined with both NCEP and IDF critera predicts cardiovascular health significantly better in females than in males among 75-year-old people from the general population
Goran Nilsson, Par Hedberg, Tommy Jonasson, Ingemar Lonnberg, John Ohrvik
Uppsala University, Sweden
Aims The International Diabetes Federation (IDF) has recommended a new definition of the metabolic syndrome. A gender-specific comparison in predicting cardiovascular health was performed between the metabolic syndrome defined by the new IDF criteria and by the criteria of the National Cholesterol Education Program (NCEP).
Material and methods We studied cardiovascular health among 75-year old people (223 women and 210 men and; participation rate 70%) from the general population of Västerås, Sweden. Absence of the following characteristics defined cardiovascular health 1) history of myocardial infarction, angina pectoris, hypertension, heart failure, cardiac surgery, diabetes, stroke/TIA, or other peripheral atherosclerotic disease. 2) Ongoing treatment with cardiovascular drugs. 3) Resting ECG with abnormal Q-wave (Minnesota code 1.1-1.3) or atrial fibrillation. 4) Exercise test with > 1mm ST-deviation. 5) Echocardiographic abnormality including wall motion index< 2.0.
Results The prevalence of the metabolic syndrome according to the NCEP and IDF criteria was for women 37% and 61%; for men 25% and 46%. Absence of metabolic syndrome predicted cardiovascular health as tabulated:
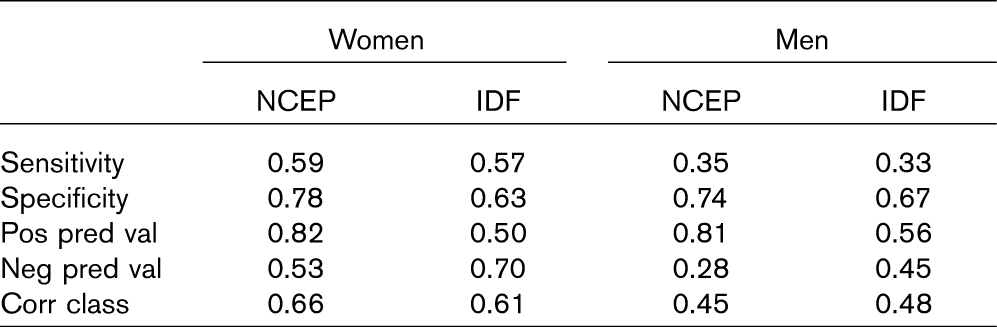
Cardiovascular health was significantly better predicted by the metabolic syndrome in women than in men. Gender differences in correctly classified were 0.21 ± 0.10 (95% CI) with the NCEP and 0.13 ± 0.10 with the IDF criteria.
Conclusion Absence of metabolic syndrome defined with both NCEP and IDF critera predicts cardiovascular health significantly better in women than in men. There is no statistically significant difference between these criteria with regard to the proportion correctly classified people among 75-year old people from the general population.
176: Depression as an etiologic and prognostic factor in coronary heart disease: a meta-analysis of 6608 events among 150<TS P>217 participants in 63 observational studies
A Nicholson, H Kuper, H Hemingway
University College London Medical School, United Kingdom
Background The role of depression as an etiological or prognostic factor in coronary heart disease (CHD) remains controversial, particularly in the light of two negative randomised controlled trials.
Objectives To quantify the effect of depression on CHD etiology and prognosis and assess the extent of confounding by coronary risk factors and disease severity.
Methods Meta-analysis of prospective cohort studies measuring depression with follow up for fatal CHD and incident myocardial infarction (etiological) or all cause mortality and fatal CHD (prognostic). We searched MEDLINE and Science Citation Index until December 2003.
Results In 24 etiological studies (131,497 people, mean follow-up 10.9 years) the random effects pooled relative risk of future CHD associated with depression was 1.76 (95% CI 1.51-2.05). Only 13 studies reported both unadjusted and adjusted results, and only 7 adjusted for smoking. These adjustments reduced the crude effect marginally from 1.91 (1.57-2.34) to 1.77 (1.41-2.22). In 39 prognostic studies (18720 patients, mean follow up 2.8 years), the random effects pooled relative risk was 1.76 (1.50-2.06). Only 10 studies reported adjustment for left ventricular function or other marker of the severity of coronary disease; and this attenuated the relative risk from 2.04 to 1.45 (1.14-1.84), a 48% reduction. In both etiological and prognostic studies, papers which did not report adjusted results had lower unadjusted effect sizes than those which did report adjusted results, (P < 0.025 and P < 0.01 repsectively).
Conclusions Depression has not been established as an independent risk factor for developing or dying from CHD because of incomplete and biased reporting of adjustment for conventional risk factors and the severity of coronary disease.
177: Incidence and prognostic implications of angina pectoris among women and men in a large ambulatory population
H Hemingway, A McCallum, M Shipley, K Manderbacka, P Martikainen, I Keskimäki
University College London Medical School, United Kingdom
Context Angina in women has often been considered a “soft” diagnosis, with “real” coronary disease predominantly affecting men, but large scale population studies have been lacking.
Objective To determine sex differences in the incidence and prognosis of angina.
Design Prospective cohort study using linked national registries.
Setting All primary care providers in Finland.
Participants Among patients aged 45-89 years with no previous history of coronary disease, we defined new cases of angina based on nitrate prescription (56,441 women, 34,885 men) or abnormal invasive or noninvasive test result (11,391 women and 15,806 men).
Main outcomes Coronary mortality at four years (n = 7906 deaths) and fatal and non-fatal myocardial infarction at one year (n = 3129 events).
Results The age standardised annual incidence per 100 population of all cases of angina was 2.03 in men and 1.89 in women with a sex ratio 1.07 (95% CI 1.06-1.09). At every age, nitrate angina in women and men was associated with a similar increase in risk of coronary mortality relative to the general population. Women with test positive angina aged < 75 years had higher coronary standardised mortality ratios than men; among those aged 55-64 it was 4.69 (95% CI 3.60-6.11) in women, compared to 2.40 (95%CI 2.11-2.73) in men, P for interaction < 0.0001. Among angina cases, event rates tended to be lower among women. There was a strong, graded relation between amount of nitrates used and event rates; women using higher doses of nitrates had comparable prognosis to men. Among diabetics with test positive angina, age standardised coronary event rates were 9.9 per 100 person years in women vs 9.3 in men (P = 0.69).
Conclusion Angina in women has a similarly high incidence to that in men, is associated with increased coronary mortality relative to women in the general population and, among easily identifiable clinical subgroups, has similarly high absolute rates of prognostic outcomes compared to men.
178: NCEP criteria of metabolic syndrome predict basal insulin resistance better than idf criteria in 75-year old people from the general population
Goran Nilsson, Par Hedberg, Tommy Jonasson, Ingemar Lonnberg, Ake Tenerz, John Ohrvik
Uppsala University, Sweden
Aims Insulin resistance is considered as the main underlying factor of the metabolic syndrome. IDF has recommended a new definition for this syndrome. This definition was compared with that of the NCEP in predicting insulin resistance. The predicting ability of waist was also included in the comparison.
Materials and methods Our cohort originated from a health survey of 75-year old people (223 women and 210 men; participation rate 70%) from the population in the city of Västerås, Sweden. Insulin resistance was defined as the gender-specific upper quartile of HOMA-index (= fasting plasma glucose, FPG mmol/Lϕasting plasma insulin, FPI mU/L / 22.5).
Results The prevalence of the metabolic syndrome according to the NCEP and IDF criteria was for women 37% and 61%; for men 25% and 46%. Median (quartiles) for FPG (mmol/L) was 5.9 (5.5, 6.6) for women and 5.9 (5.5, 6.5) for men; for FPI (mU/L) 8.5 (5.7, 12.9) for women and 8.4 (6.2, 12.4) for men; for HOMA-index 2.4 (1.5, 3.9) for women and 2.2 (1.6, 3.4) for men. ROC curve using 10-folded cross-validation identified waist as the best single component of the metabolic syndrome to predict insulin resistance (optimal cut-off point 91.5 cm for women; 96.5 cm for men). The AUC was 0.82 (0.75-0.89; 95% CI) for women and 0.70 (0.62-0.78) for men. The predictive values for insulin resistance are tabulated.
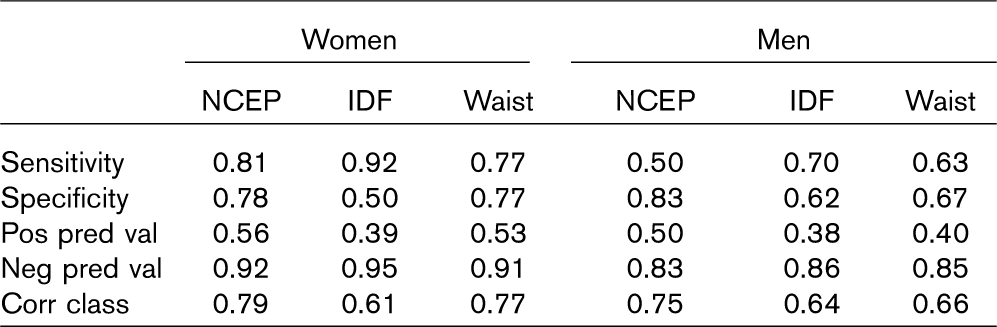
The following significant differences (mean, 95% CI) in correctly classified patients were found: NCEP/IDF 0.18 ± 0.09 for women and 0.11 ± 0.09 for men; waist/IDF 0.16 ± 0.09 for women.
Conclusions In 75-year old people NCEP performs better than IDF in predicting insulin resistance. In women waist solely performs better than IDF.
190: Influence of the climate on hospitalizations and in hospital mortality of heart failure patients: results at the north Greece
E Hatzinikolaou-Kotsakou, G Bobotis, D Tziakas, D Floros, D Stakos, A Mavridis, A Hotidis, A Kostaki, DI Hatseras
Academic Cardiology Department, Demokritus University of Thrace, Greece
Background The influence of the climate on the number of hospital admissions due to the deterioration of chronic heart failure and on inhospital mortality rate has been discussed controversially based on results of very different regional observations.
Methods We did a registry in the North Greece in which 330 consecutive patients with chronic heart failure have been enrolled to document acute admissions to the hospital and in- hospital clinical outcome. Because of the very homogeneous climate in this area we brought together the daily meteorological data and the patients' data of the time between July 2002 -and January 2005. Based on 12 biosynoptical climate classes we defined stable (classes 1-3 and 8-12) and unstable (classes 4-7) climate. We examined the influence of the unstable climate on the number of hospital admissions and on inhospital mortality.
Results During the observentional period 330 pts (median age 64 years, 62% male) with chronic heart failure had been enrolled. Unstable climate was present on 364/910 days (40%). We did not find any difference in daily hospitalization rate between unstable and stable e climate (5.8 ± 2.4 vs 5.7 ± 2.3, P = 0.30). There were no differences in pts characteristics (age, gender, heart failure etiology, and drugs treatment) on the days with unstable as compared with stable climate.
The multivariate analysis identified the unstable climate as an independent determinant of inhospital mortality (OR 1,49, 95% CI 1.12-1.99).
Conclusions Unstable climate did not influence the number of hospital admissions of chronic heart failure pts in the North Greece. Pts at risk for hospitalization dependent on climate could not be identified. Unstable climate on the chronic heart failure pts was associated with a marked increase on inhospital mortality in this group of pts in North Greece.
216: Long term use of Swedish moist snuff and the risk of acute myocardial infarction
M-P Hergens, L Alfredsson, G Bolinder, M Lambe, G Pershagen, W Ye
Institute of Environmental Medicine, Karolinska Institutet, Sweden
Background In Sweden, the use of smokeless tobacco has increased in recent decades, and today 20% of the male population are daily users of snuff. Adverse cardiovascular effects due to snuff use, could thus be of great public health relevance. However, the scientific evidence on cardiovascular risks associated with long term oral use of moist snuff is limited and inconclusive. We aimed to study whether long-term use of snuff affects the risk of acute myocardial infarction (AMI).
Methods The Swedish Construction Industry's Organization for Working Environment Safety and Health provided repeated health check-ups to construction workers between 1978 and 1993. During this period information on tobacco use and other risk factors was also collected by questionnaire. In total, 117 414 men who never smoked and without a history of myocardial infarction were followed through 2001. Primary outcome was morbidity of and mortality from AMI. Relative risk estimates derived from Cox proportional hazards regression model, with adjustment for age, body mass index and region of residence.
Results Almost 30% of the men had ever used snuff. During the follow-up, 2 164 non-fatal and 686 fatal cases of AMI were identified. The adjusted relative risks for ever snuff users were 0.89 (95% confidence interval, 0.77-1.02) for all cases, 0.87 (95% confidence interval, 0.77-1.02) for non-fatal cases and 1.29 (95% confidence interval, 1.05-1.60) for fatal cases. Among current snuff users, those who consumed one box (50 gram) or more per day had a particularly elevated risk for fatal myocardial infarction (relative risk = 2.30, 95% confidence interval, 1.23-4.34). Snuff dipping also increased the probability of mortality from cardiovascular diseases among non-fatal AMI patients.
Conclusion Our results provide little evidence that snuff use increases overall risk of AMI, although there appears to be an increased risk of fatal AMI among snuff users, particularly among heavy users.
229: Metabolic syndrome and survival following coronary artery bypass grafting surgery
AI Papathanasiou, HI Milionis, KI Kalantzi, P Gounopoulos, A Isseris, IA Goudevenos
Dept of Cardiology, University Hospital of Ioannina, Ioannina, Greece
Background The metabolic syndrome (MetS) is a clustering of interrelated cardiovascular risk factors and is associated with an increased risk of cardiovascular disease. New definitions such as that of the National Heart, Lung, and Blood Institute and the American Heart Association (NHLBI/AHA), and especially that proposed by the International Diabetes Federation (IDF) have raised concerns as to the whether they can identify high-risk population.
Objective To evaluate the association between metabolic syndrome (MetS) and survival among patients undergoing a coronary artery bypass grafting surgery (CABG).
Setting University Hospital of Ioannina, Ioannina, Greece.
Design and methods An observational study involving 1870 consecutive patients (1657 men, 212 women, mean age 58.7 ± 9.6 years), who underwent a first-ever CABG between 1986 and 2002, survived the first month and visited our outpatient clinic for scheduled examination within 6 months after the procedure. Both NHLBI-AHA and IDF definitions for the diagnosis of MetS were applied. Cox proportional hazard analysis to calculate adjusted hazard ratios (HR) were performed for both definitions.
Results During a total of 9,345 patient-years follow up (median follow up 5.2 years, range 2-16 years), 222 deaths occurred; of these 179 (80.6%) were due to cardiovascular causes. In multivariate Cox regression analysis and after adjustment for age, sex, smoking, the presence of hyperlipidemia, hypertension, and diabetes mellitus, HRs of cardiovascular mortality for NHLB-AHA-defined MetS and IDF-defined MetS were 2.51 (1.17-5.38 95% CI, P = 0.018), and 1.80 (1.07-3.00 95% CI, P = 0.025), respectively.
Conclusion In patients undergoing CABG, the presence of the MetS is associated with an increase in cardiovascular mortality. This risk seems to be moderated by applying the IDF definition of MetS.
230: The prevalence of smoking and sedentary lifestyle in adolescents
D Zdrenghea, L Vatca, G Vaidean, D Pop
Dept Cardiol, Rehab Hosp, Cluj-Napoca, Romania
Background Cigarette smoking has a high prevalence in all ages, but about 95% of adult smokers first started smoking before 18 years. Sedentary lifestyle is also prevalent at all ages, even if the physical activity is particularly important among adolescents because the atherosclerotic process starts early on.
Purpose To evaluate the prevalence of smoking and sedentary lifestyle in romanian adolescents.
Methods The study sample included 721 students 390 (54.1%) girls and 331 (45.9%) boys, aged 15-19 years, from a high school in Oradea, Romania, the data being obtained by questionnaires.
Results Among adolescents, 70% try to smoke even ones during their life; 31.5% are current smokers. Reason of smoking is for more than 80% of the subjects, curiosity, and more than 65% of current smokers have no difficulties to buy cigarettes from a store. On the other hand physical activity classes are characterized by attendance: 74.7% girls and 79% boys reported their participation in physical activity classes twice a week. Sixty percent of them exercise 30 minutes or more during these classes. Leisure-time physical activity levels are however considerably lower; 46.9% girls and 54.1% boys only watch TV or have computer activities; during weekend physical inactivity increases substantially. Sedentary pattern is more pronounced among girls and, in 75% of the cases, it is a family feature.
Conclusion School is not yet in Romania an important part of the structures involved in campaign against smoking, the habbit being extremely high among adolescents. Also, for the great majority of the highschool students, physical activity is limited to the two classes per week, offered in school, local and national efforts and national guidelines being necessary to be addressed.
233: The metabolic syndrome as a predictor of coronary heart disease and type 2 diabetes in older men
SG Wannamethee, AG Shaper, L Lennon, PH Whincup
Royal Free and University College Medical School, United Kingdom
Background and aims A new worldwide definition of the metabolic syndrome was proposed by the International Diabetes Federation (IDF) to provide a better predictor of cardiovascular disease (CVD) and type 2 diabetes. We have compared the associations between three definitions of the metabolic syndrome with risk of major coronary heart disease (CHD) events, and incident type 2 diabetes in older men. The definitions studied were the new IDF definition, and the older definitions of the World Health Organisation (WHO) and the National Cholesterol Education programme (NCEP).
Methods A prospective study of 3356 non-diabetic men with no history of myocardial infarction aged 60-79 years at baseline and followed up for a mean period of 5 years, during which there were 151 major CHD events (non fatal myocardial infarction or fatal CHD events) and 90 new cases of type 2 diabetes.
Results None of the three definitions of the metabolic syndrome were significantly associated with increased risk of CHD. The age-adjusted hazard ratio (95% CI) was 1.22 (0.83, 1.81) for IDF syndrome, 1.25 (0.89, 1.76) for WHO syndrome and 1.19 (0.84, 1.69) for NCEP syndrome. Of the components of the metabolic syndrome, only blood pressure (BP > 140/90 mm Hg; WHO criteria) and low HDL-cholesterol predicted CHD risk; no association was seen with waist circumference, blood glucose and triglyceride. However, the metabolic syndrome was strongly associated with diabetes risk, with WHO and NCEP definitions showing the strongest associations. The age adjusted hazard ratios (95% CI) were 4.49 (2.97, 6.79), 5.68 (3.66, 8.80) and 5.70 (3.68, 8.85) for IDF, WHO and NCEP definitions respectively.
Conclusion In older men the metabolic syndrome (defined by any methods) identified men at risk of diabetes but not CHD. The new IDF syndrome did not appear to better predict CHD or diabetes than previous versions.
263: Dietary intake and smoking status among participants of the pol-monica bis warsaw project
E Sygnowska, A Waskiewicz, J Piwonski
National Institute of Cardiology. Poland
Background Understanding differences in dietary patterns by smoking status is important for nutritionists and health educators involved in helping individuals to make healthy dietary and lifestyle choices.
Aim The aim of the study was to compare dietary intake according to smoking status in a representative sample of Warsaw population.
Methods The study sample included 1306 men and women aged 20-74 years. The information about smoking habits, age, education level, anthropometric measures, blood pressure and lipids profile was determined. The dietary intake was estimated with 24 -hour recall. Participants were classified as current smokers (266 men, 177 women), non-smokers (never smokers and former smokers who have not smoked for more than 10 years-272 men, 403 women) and ex-smokers (who have not smoked for less than 10 years-111 men, 77 women).
Results Current smokers tended to be younger with less education than non- and ex-smokers. The average body mass index of current smokers (26.8 kg/m2 in men, 26.4 kg/m2 in women) was the lowest of the 3 groups both in men and in women. Men and women who smoked ate more meat products and added animal fat but less fruit than non- or ex-smokers. The differences in nutrients intake among persons with different smoking status after adjustment for age, education and season of research, were rather small. Energy, fats and niacin intake tended to be higher in smokers than in the other 2 groups. In male smokers the lowest intake of vitamin C was observed. There were not any differences in vitamin and minerals supplementation among persons with different smoking status. Alcohol intake was higher in smokers than in former and non- smokers.
Conclusions Smoking is one of the most important cardiovascular risk factors. Smokers have a less healthy diet than non- or ex-smokers which can enhance that risk.
265: The role of vitamins and minerals supplementation in nutrition of urban and rural population-Pol-MONICA bis project
Anna Waskiewicz, Elzbieta Sygnowska, Walerian Piotrowski, Jerzy Piwonski
National Institute of Cardiology, Poland
Aim To estimate patterns of supplement use among Polish urban and rural population and the relationship between supplement use, dietary habits and cardiovascular risk factors.
Methods and results Supplements use (vitamins A, C, E, calcium, magnesium), nutrient intake and cardiovascular risk factors were examined in the frame of Pol-MONICA bis Project. In 2001 randomly selected population samples-1329 men and women from urban (Warsaw city) and 1398 from rural (former Tarnobrzeg voivodeship) population, aged 20-74, took part in this study. The use of vitamins/minerals supplement was reported by 20% men and 28% women from urban and 8% and 17% from rural population respectively. Use of supplements was more frequent among persons with university education, full-time employment and people consuming other medicines. There were not significant differences in cross sectional analysis in cardiovascular risk factors (HDL-, LDL- and total cholesterol, smoking status, body mass index, blood pressure) between supplement users and nonusers. The role of supplementation in nutrition was different in cases of minerals and vitamins. Calcium and magnesium were used in the doses not sufficient (5-15% total intake) to eliminate the risk of deficiency. Vitamins were taken in amounts much higher (40-80% total intake) than Recommended Dietary Allowances (RDAs). Among 6-19% people, doses of vitamins A and E 10-times exceeded the RDA.
Conclusion There is a need to develop and implement programs aimed at improving the supplement use in Poland
295: Obesity has higher impact for the presence of cardiovascular risk factors in women: a mesyas registry subanalysis
Alberto Cordero, Martín Laclaustra, Montserrat León, Clara Bergua, Beatriz Ordoñez, Isaac Pascual, Monica Nájar, Jose-Antonio Casasnovas, Alfonso del Río, Eduardo Alegría; MESYAS REGISTRY
Clinica Universitaria de Navarra, Pamplona. Spain
Background Obesity and overweight are increasing progressively, leading to an increase in cardiovascular risk factors related to insulin resistance or excess of weight and, also, in atherothrombotic events.
Methods and results The MESYAS Registry (Metabolic Syndrome in Active Subjects) is a cross-sectional study that included active workers recruited in their annual health examinations. Body mass index (BMI) was used to diagnose overweight (25.0-29.9 kg/m2) and obesity (> 30 kg/m2). Metabolic syndrome (MS) and cardiovascular risk factors were assessed according to the modified ATP-III recommendations that use BMI instead of waist circumference. Among the 19,041 subjects included (80% males), mean age 42.2 (10.7), the prevalence of MS was 12.0% (95% CI 11.8-12.2), overweight 44.6% (95% CI 44.0-45.2) and obesity 17.3% (95% CI 17.0-17.5). Women had lower prevalence of all cardiovascular risk factors. Multivariant analysis showed a strong association of overweight (OR: 2.4; 95% CI 2.2-2.6) and obesity (OR: 5.3; 95% CI 4.7-5.9) to the presence of any other two criteria of the MS. The impact of age for the presence of MS was higher in women because the highest quartile of age showed a significantly higher odds ratio in women than in men (8.5 vs. 4.1). Overweight and obesity showed significant associations with the presence of all cardiovascular risk factors, except for low-HDL in women, and significantly higher association in women for the presence of diabetes (OR: 13.6; 3.8-48.6), MS (OR: 10.6; 7.6-14.8), hypertriglyceridemia (OR: 8.6; 5.6-13.1), and impaired fasting glucose (OR: 3.7; 2.6-5.3).
Conclusions Overweight and obesity are strongly related to classical cardiovascular risk factors, atherogenic dyslipemia and MS in active subjects. The impact of the excess of weight for these situations is even higher in women.
300: The impact of smoking on three years survival after an acute coronary syndrome
VN Nicolaou, IE Papadakis, DB Panagiotakos, CN Couremenou, X Krinos, PG Marnelos, NM Bourboulis, EN Karatzis, AK Tsakiris, PD Skoufas
First Cardiology department, Red Cross Hospital, Athens, Greece
Objectives To evaluate the factors which are related with the continuing of smoking of patients with an acute coronary syndrome.
Methods 367 patients (309 male, 80%) who were admitted to our cardiological clinic the period 2000-2001 for an acute coronary syndrome were studied for three years. The mean age of the patients was 63 ± 12 years. 229 (64%) were smokers before the acute coronary syndrome. During the follow-up, their parameters were reconsidered every 6 months. (Collaboration grade 69%)
Results Despite doctors' recommendations, 120 smokers (52%) continued smoking after the acute coronary event through the period of the three years. Smokers were principally male (P = 0.007), had a higher body mass index (mean BMI = 27. 4 ± 3.4, P = 0.05) and had a negative medical history for cardiovascular disease. In the three years period, 34 patients died from the 252 who participated in the follow up (14%). Smokers who continued smoking after an acute coronary syndrome had four times greater probability to die in the three years period in comparison with those who ceased smoking (P = 0.01). Cease smoking reduces 73% the likelihood for cardiovascular death, after adjusting for other risk factors such as age, gender, blood pressure and body weight.
Conclusions The impact of smoking on cardiovascular danger is well established. Nevertheless a lot of work must be done on the level of secondary prevention for cardiovascular disease, because almost 50% of the smokers continue smoking after an acute coronary syndrome.
306: What is the evidence for the presence of cardiovascular risk factors in a rural South African population? results of the SASPI project
M Thorogood, MD Connor, FGR Fowkes, GA Lewando Hundt, SM Tollman, I Tzoulaki; The SASPI study
Warwick Medical School, University of Warwick, United Kingdom
In the past there has been little evidence of the presence of risk factors for cardiovascular disease in rural South Africa, but the population is experiencing rapid social and economic change. Increasing prevalence rates for diabetes and hypertension are now being reported. As part of the southern African Stroke Prevention Project (SASPI) carried out in the Agincourt sub-district of Limpopo Province in rural South Africa we have found a prevalence rate for stroke survivors in the population over 15 years of age (300/100 < P > 000 95% CI, 250 to 357) which is about half the number expected in a high income country, higher than previously found in Africa. We have carried out a cross-sectional study of cardiovascular risk factors in adults aged over 35 years in Agincourt sub-district, including measuring for the first time in an African population the ankle brachial index. This is known to be a good marker of subclinical atheroma and of the risk of future cardiovascular events. We found a high prevalence of smoking in men (31.9%), although the amount smoked was low. Smoking was rare in women. There was a striking difference in mean body mass index between men and women (22.8 kg/m2, 95% CI 21.7-23.9 compared with 27.2 kg/m2 95% CI 26.4-28.1) We found a high prevalence of hypertension (43%), but relatively low levels of total cholesterol. However, we found that the prevalence of a low ankle brachial index of < 0.9, (indicative of significant atheroma and higher cardiovascular risk), increased with age from 3.9% in 40-49 year olds to 39.7% in those 70 years and older. The distribution was very similar to that reported in Western populations and suggests that this population has sub-clinical peripheral atheroma and is at increased risk of future cardiovascular events. Urgent consideration should be given to instituting preventive measures.
307: The effect of the environment on uptake of physical activity in Norfolk, UK
C Foster, M Thorogood, C Grundy, M Hillsdon, B Sheehan, N Wareham, M White
Warwick Medical School, University of Warwick, United Kingdom
Despite strong evidence that physical activity is important in the prevention of cardiovascular disease, population surveys show that only a minority of the population are active at recommended levels (at least 150 minutes of moderate intensity physical activity per week). We analysed a cross sectional study of people's perceptions of their environment in relation to the amount of physical activity undertaken, and found that women were more likely to be active if they perceived that it was safe to walk in their locality and if there were nearby services, such as shops, but men were not affected by these considerations. To investigate the relationship between objectively measured environmental factors and the physical activity of men and women we have carried out a secondary analysis of data from the Norfolk cohort of the European Prospective Investigation of Cancer (EPIC). We used Geographical Information Systems (GIS) and multivariate models to relate 13,500 participants' reported levels of physical activity with a range of measures of the local environment. Younger age, higher social status and higher educational level were consistently associated with higher levels of different physical activities. Road traffic density was an important predictor of uptake of cycling. Access to green space and area levels of crime were not associated with walking for recreation. Distance to facilities had either no effect or only a small effect on the uptake of different activities. Future research should use both perceptions and objective measures of the environment to examine the relationship between individual, environmental and psychosocial variables. Methods should include using GIS and multi-level modelling to examine determinants of different types of physical activity for different population groups.
320: Trends in lipids profile in Northern Poland during 7 years follow-up
J Bellwon, K Chlebus, D Zielinska, J Siebert, W Sobiczewski, M Gruchala, A Rynkiewicz
Medical University of Gdansk, Gdansk, Poland
Background The socio-political transition has substantial influence on lifestyle and dietary habits. The aim of our study was to assess trends in lipids profile during 7 years of follow up in a cohort recruited in Northern Poland.
Material and methods We have examined 511 subjects, employees of one company, mean age 44.7 ± 8.2 years, 403 men and 108 women, who did not present symptoms of cardiovascular (CV) diseases at baseline. Medical history, physical examination, total cholesterol (TC), HDL and LDL cholesterol and triglycerides (TG) measurements were performed at baseline and after 7 years of follow up. We have analyzed lipids in subjects with and without major CV events.
Results There were 61 CV event survivors and 4 CV deaths. In subjects without CV events there was no change in TC and TG after follow up; 226 ± 48, 223 ± 41 mg/dl and 150 ± 113, 155 ± 107 mg/dl respectively. However LDL decreased significantly from 148 ± 41 to 141 ± 37 mg/dl (P < 0.05) TC/HDL ratio from 5.1 ± 2.0 to 4.5 ± 1.4 (P < 0.001) and HDL increased from 48 ± 15 to 53 ± 14 mg/dl (P < 0.001). In CV events survivors TC decreased significantly from 249 ± 49 to 226 ± 57 mg dl (P < 0.05); LDL from 170 ± 49 to 135 ± 46 mg/dl (P < 0.001); TC/HDL ratio from 5.8 ± 2.4 to 4.6 ± 1.7 (P < 0.005). HDL and TG did not change 48 ± 18 to 53 ± 16 mg/dl and 180 ± 155 to 186 ± 158 mg/dl respectively. At baseline both groups differed significantly in all parameters except for HDL; TC (P < 0.001), LDL (P < 0.001), TC/HDL ratio (P < 0.05), TG (P < 0.05). After 7 years both groups differed significantly only in TG level (P < 0.05). Only 15 subjects (3.3%) received hypolipemic medication ordered by their GP, otherwise there was no specific hypolipemic medical intervention in this cohort.
Conclusions We have observed a beneficial shift in most lipid fractions in studied cohort, particularly in subjects given lifestyle advice. The observed lipid profile changes may reflect life style changes, mostly in diet.
323: Changes in prevalence of hyperlipidemia in GDANSK port workers during 7 years follow-up
J Bellwon, K Chlebus, D Zielinska, W Sobiczewski, M Gruchala, A Rynkiewicz
Medical University of Gdansk, Gdansk, Poland
Background In countries under socio-political transition there is important change in lifestyle and dietary habits. The aim of our study was to assess changes of lipids abnormalities prevalence during 7 years of follow up.
Material and methods We have examined 511 subjects, employees of one company, mean age 44.7 ± 8.2 years, 403 men and 108 women, who did not present symptoms of cardiovascular (CV) diseases. Medical history, physical examination, total cholesterol (TC), HDL and LDL cholesterol and triglycerides (TG) measurements were performed at baseline and after 7 years of follow up. Hypercholesterolemia (HTC) was diagnosed when TC > 190 and TG < 150mg/dl; hypertriglicerydemia (HTG) when TG > 150 and TC < 190mg/dl and mixed hyperlipidemia (MHL) when TC > 190 and TG > 150mg/dl. For analysis we divided the subjects into two groups with and without CV events during the follow up.
Results There were 61 CV event survivors and 4 confirmed CV deaths. In whole cohort there was no change in prevalence of hypercholesterolemia 45.8% and 44.8%, hypertriglicerydemia 4.1% and 4.0% and hyperlipidemia 32.7% and 33.9%. Unfortunately in subjects without CV events there was also no change in prevalence of hypercholesterolemia 45.6% and 46.8%, hypertriglicerydemia 3.7% and 3.5% and hyperlipidemia 31.5% and 32.9%. In subjects with CV events prevalence of hypercholesterolemia decreased significantly from 46.8% to 31.2% (P < 0.05). There was insignificant trend to increase hypertriglicerydemia from 6.3% to 8.2% and hyperlipidemia from 39.2% to 41.0%. Only the CV event group 15 subjects received hypolipemic medication ordered by their GP, otherwise there was no specific hypolipemic medical intervention in observed population.
Conclusions There is inefficient diagnosis and treatment of hyperlipidemias in northern Poland despite high cardiovascular morbidity and mortality.
324: Development of the metabolic syndrome in Northern Poland during 7 years of follow-up
J Bellwon, K Chlebus, W Sobiczewski, M Gruchala, D Ciecwierz, A Rynkiewicz
Medical University of Gdansk, Gdansk, Poland
Objective The metabolic syndrome (MS) definition contains risk factors not included in commonly used cardiovascular risk algorithms and probably improves cardiovascular risk estimation. The aim of our study was to compare the prevalence of MS development based on two, ATP III and IDF, MS definitions.
Methods We have examined 511 subjects, employees of one company, mean age 44.7 ± 8.2 years, 403 men and 108 women, who did not present symptoms of cardiovascular diseases. Medical history, physical examination, ECG, blood pressure twice in the sitting position, lipids and fasting glucose measurements were performed at baseline during routine medical check up and after seven years of follow up. The metabolic syndrome was diagnosed according to ATP III and IDF criteria.
Results At baseline 111 (21.7%) subjects fulfilled ATPIII criteria and 152 (29.8%) subjects fulfilled IDF criteria of MS (P < 0.005). After 7 years of follow up 141 (27.6%) subjects fulfilled ATPIII criteria and 213 (41.7%) subjects fulfilled IDF criteria of MS (P < 0.001). The increase of prevalence during follow up was significant for both definitions (P < 0.05) for ATPIII and (P < 0.001) for IDF There were 61 CVevent survivors and 4 confirmed CV deaths. In subjects without CV events prevalence of MS increased significantly from 19.4% to 26.6% for ATPIII criteria (P < 0.05) and from 26.4% to 41.4% for IDF criteria (P < 0.001). In CV event survivors prevalence of MS did not change for ATP criteria 34.2% and 32.9% and for IDF criteria 48.1% and 43.0% (ns). In subjects with CV events prevalence of MS was significantly higher than in those without CV event at baseline (P < 0.005) for ATPIII, (P < 0.001) for IDF criteria and after 7 years (P < 0.01) for ATPIII, (P < 0.05) for IDF criteria.
Conclusion The prevalence of metabolic syndrome is almost twice higher using IDF metabolic syndrome criteria than ATP III criteria.
325: Predictive value of new metabolic syndrome definition
J Bellwon, K Chlebus, W Sobiczewski, M Gruchala, D Ciecwierz, A Rynkiewicz
Medical University of Gdansk, Gdansk, Poland
Objective The metabolic syndrome (MS) definition contains risk factors not included in commonly used CV risk equations. MS can give additional information in estimation of CV risk. The aim of our study was to compare the predictive value of MS diagnosis for development of diabetes mellitus (DM), arterial hypertension (HA) and cardiovascular (CV) event of two ms definitions ATP III and IDF.
Methods We have examined 511 subjects, employees of one company, mean age 44.7 ± 8.2 years, 403 men and 108 women, who did not present symptoms of cardiovascular diseases. Medical history, physical examination, ECG, blood pressure twice in the sitting position, lipids and fasting glucose measurements were performed at baseline during routine medical check up and after seven years of follow up. The metabolic syndrome was diagnosed according to ATP III and IDF criteria.
Results At baseline 111 (21.7%) subjects fulfilled ATP criteria of MS and 152 (29.7%) subjects fulfilled IDF criteria of MS (P < 0.005). After 7 years of follow up 141 (27.6%) subjects fulfilled ATPIII criteria of MS and 213 (41.7%) subjects fulfilled IDF criteria of MS (P < 0.001). During 7 years of follow up 135 subjects were diagnosed with HA, 37 with DM and 61 suffered CV event. Positive predictive value of MS diagnosis based on ATPIII and IDF criteria for diagnosis during seven years of follow up for HA were 50% and 46%, for DM 22% and 18%, for CV event 24% and 25% respectively. Negative predictive value of MS diagnosis based on ATPIII and IDF criteria for diagnosis during seven years of follow up for HA were 79% and 80%, for DM 96% and 97%, for CV event 87% and 89% respectively, all ns.
Conclusion The prevalence of metabolic syndrome is higher using IDF metabolic syndrome criteria than ATPIII criteria, but the predictive value for hypertension, diabetes and cardiovascular events are similar for both definitions.
334: Cardiovascular risk factors incidence in patients with aortic prostheses for degenerative vs other lesions
Dana Velimirovici, Maria Rada, Delia Berceanu, DM Duda-Seiman, Simona Dragan, D Gaita, A Cocoana, Livia Barbu, Silvia Mancas
Preventive Cardiology and Cardiovasc. Rehabilitation Clinic Timisoara, Romania
Objectives Aortic degenerative lesions show significant similarities with atherosclerotic lesions, the risk factors for their development being the same. The purpose of the work is to assess the incidence of cardiovascular risk factors (CRF) in patients with aortic prostheses for degenerative vs. other (rheumatic, congenital, etc.) lesions.
Methods We studied 75 patients after aortic valvular replacement with mechanic/biological prostheses for degenerative (group A) or other lesions (group B). Male patients were predominant (68%), mean age was 63 ± 9 years. Studied CRF were: BP ≥ 140/90 mmHg; BMI ≥ 30kg/m2; TC ≥ 200 mg/dl; diabetes mellitus (fasting plasma glucose ≥ 126 mg/ dl); smoking or ex-smoker state. Statistical processing: mean value ± standard deviation;%; unpaired t test.
Results Aortic degenerative lesions were more frequent (group A = 60%). The incidence of CRF shows that aortic degenerative lesions are associated with a higher prevalence of risk factors: hypertension 56% (P = 0.004), hypercholesterolemia 45.33% (P = 0.0001) and obesity 22.66% (P = 0.006). Diabetes mellitus was present only in group A (10.66%). There were no significant differences regarding the ex-smoker state. There is a risk factors aggregation in group A, 53.33% of the patients being with at least 3 risk factors. Patients in group B had 1-2 CRF (56-66%).
Conclusions Degenerative aortic lesions are accompanied by a higher prevalence of classical CRF, compared to other aortic lesions. Hypertension, hypercholesterolemia and obesity, because of their incidence, modify the cardiovascular risk profile in aortic valvular disease.
336: Severity and prognosis of acute coronary syndromes in patients with metabolic syndromes
Z Babic, V Nikolic Heitzler, N Bulj, M Pavlov, V Radeljic, T Krcmar, V Erdeljic
University Hospital Sestre milosrdnice, Zagreb, Croatia
Metabolic syndrome is a combination of visceral obesity, arterial hypertension, insulin resistance, glucose intolerance and dyslipidaemia. This entity causes increased cardiovascular risk in 25-35% of developed world population and it can be expected that prevalence of this syndrome will increase in quoted growing old population. It can be expected that acute coronary syndromes are more severe and have worse prognosis in patients with criteria for metabolic syndrome.
In this study the authors collected data on 267 patients who had suffered from acute coronary syndromes (STEMI, NSTEMI, unstable angina pectoris) and were hospitalized in the Coronary Care Unit, University Hospital “Sestre milosrdnice”, Zagreb, Croatia. Investigated patients were divided in three groups: group with metabolic syndrome, group of obese patients without criteria for metabolic syndrome and lean patients group. The groups of patients were compared according to the severity level and the prognosis of acute coronary syndromes.
The severity of the acute coronary syndromes was estimated using the cardioselective markers value, ECG changes, echocardiography and coronarography findings, early and late complications, the number of days of hospitalization in CCU, and also the general and cardiovascular in-hospital mortality. Prognosis of the acute coronary syndromes was estimated by incidence of MACE, general mortality, the appearance and CCS level of angina pectoris and rehospitalization rate during follow up period of 1 year.
In conclusion, authors found the significant difference among the investigated groups. The highest level of severity and the worst prognosis of acute coronary syndromes were in patients with metabolic syndrome. This emphasizes importance of early diagnosis and comprehensive treatment of metabolic syndrome.
339: The relationship between hepatitis b virus surface antigen and angiographic coronary artery stenosis in Chinese
Min Pan, Wenping Jiang, Zhihua Liu, Jianhua Zhu, Xiangjun Yang, Chunlan Yang, Rongchun Shen, Shaoqing Ju, Xiaohong Yu
Department of Cardiology, Affiliated Hospital of Nantong University, People's Republic of China
Aim Recent findings suggest a causative role of infections in the pathogenesis of atherosclerosis. Several published studies reported strong association between hepatitis B virus surface antigen (HbsAg) carrier and carotid atherosclerosis. We aimed to investigate the clinical relationship between HBsAg and angiographic coronary artery stenosis, as well as levels of C-reactive protein (CRP) in Chinese, a population with relatively high prevalence of hepatitis B virus.
Methods 627 cases of consecutive coronary angiography were recruited and divided into coronary artery disease (CAD) group and non-CAD group. The diagnosis of CAD was confirmed by angiography, defined as at least 50% stenosis of at least one major epicardial coronary involved vessels. The extent and severity of the coronary artery was investigated using CAD score. HBsAg and levels of CRP were measured by enzyme linked immunosorbent assay (ELISA) in every patient prior to angiography, then positive percentages of HBsAg were compared among different groups.
Results The average positive percentage of HBsAg in total 627 cases was 6.38% (40/627), and the positive percentage of HBsAg was 6.44%(31/481) in CAD group and 6.16%(9/146) in non-CAD group, respectively, there was no significant difference between two groups (Pearson x2 =0.0148, P = 0.9033). Also, there was no statistical difference of positive percentage of HBsAg to be found among groups with different extent and severity of coronary lesion (P > 0.05). Of all 627 cases, mean CRP levels (5.58 ± 0.74) mg/L in HBsAg positive and (5.45 ± 0.82) mg/L in HBsAg negative showed no significant difference between the two groups (t = 0.9758, P = 0.3295). Similar results were also found when divided into CAD group and non-CAD group. Multiple logistic regression analysis showed HBsAg positive did not related to CHD independently (OR = 1.13, 95% CI = 0.31-1.75, P = 0.4276).
Conclusion HBsAg positive have no relationship to coronary artery stenosis and CRP levels in Chinese.
346: The health knowledge concerning CVD prevention and hypertension in relation to some socio-demographic factors and health status
A Piwonska, W Piotrowski, J Piwonski, W Bielecki, K Kozakiewicz, J Gluszek, U Biela, T Zdrojewski; for the WOBASZ group
National Institute of Cardiology, Warsaw, Poland
Background Insufficient knowledge of CVD risk factors, unawareness of diseases and their complications cause the limitation of CVD prevention effectiveness. So we evaluated the knowledge concerning hypertension (HT) and CVD prevention methods (PM) in relation to gender, age, education level (EL), hypertension status, coronary artery disease history (CADH) and positive family history (FH) of CVD death.
Methods Data came from the polish population sample-14769 persons (6977 men and 7792 women), aged 20-74, screened in 2003-2005. We analyzed how many persons were familiar with their blood pressure (BP), the upper limit of normal BP, HT complications and PM.
Results 51% of men and 56% of women said they knew the upper limit of normal BP (P < 0.0001), but 30% located it in normotension, 40% in the 1st grade HT and 6%-8% considered it greater than 160/100mmHg. 59% of men and 69% of women declared they knew their BP (P < 0.0001). One third of them incorrectly classified it as normal or high. Stroke (58% men, 69% women, P < 0.01) and myocardial infarction (respectively 60% and 65%, P < 0.01) were the most often mentioned HTcomplications, but 32% of men and 23% of women did not know any of them (P < 0.01). Older, higher educated persons, with FH or with HT had greater knowledge on HT. Out of PM the most often mentioned were: higher physical activity (54% men, 58% women, P < 0.0001), smoking cessation (42% and 40%, NS) and healthy life style (36% and 39%, P < 0.0001). More men than women knew nothing about PM. Younger and higher educated persons had greater knowledge on CVD prevention. Unexpectedly, persons with FH and those with CADH did not presented greater knowledge concerning PM than those without.
Conclusions Knowledge concerning hypertension and CVD prevention was still insufficient in polish population. Women had greater knowledge than men. Age, education level, hypertension status and family history of CVD death were significant modifiers of knowledge level.
348: Genetic variation in alcohol dehydrogenase and beneficial effect of alcohol consumption on myocardial infarction. results from the monica/kora study
J Heidrich, J Wellmann, C Reitz, U Keil
Institute of Epidemiology and Social Medicine, University of Muenster, Germany
Background Epidemiological studies show that light to moderate alcohol consumption lowers the risk of coronary heart disease (CHD). Recently, it has been suggested that alcohol metabolizing enzyme alcohol dehydrogenase 3 (ADH3 or ADH1C) modifies the association between alcohol consumption and CHD risk. We highlight the current scientific evidence and investigate the relationship between alcohol intake and CHD with regard to ADH3 in a German population.
Methods We used data from the population-based MONICA/KORA Augsburg study. Alcohol consumption was assessed at baseline among 3674 men and women aged 25-74 who were followed from 1995 to 2002 with respect to fatal and non-fatal coronary events. ADH3 genotype (y1y1 = fast alcohol metabolism; y1y2 = intermediate alcohol metabolism; y2y2 = slow alcohol metabolism) was specified. The association between alcohol intake and CHD according to ADH3 genotype was investigated using multivariate Cox proportional hazards models.
Results Mean age was 48.6 years in both men and women. During follow-up, 53 fatal and non-fatal myocardial infarctions occurred among men and 19 among women, respectively. Distribution of ADH3 genotype among males was as follows: homozygote fast 38.7%; homozygote slow 15.1%; and the remaining 46.2% heterozygote. Males with either homozygote or heterozygote slow allele and 20 grams alcohol intake/day had a CHD-risk of 0.69 (95% CI 0.18-2.55). Risk of CHD in males with any slow allele decreased with increasing alcohol intake while CHD risk in those with homozygote fast alleles showed a J-shaped function.
Conclusions ADH3 genotype may modify the association between alcohol consumption and CHD. Males with slow allele may profit particularly from moderate alcohol consumption.
358: An innovative approach to large scale population screening, notification and education of healthy individuals at risk of hypercholesterolemia
MH Sayers, S Goudar, J Centilli, S Myers
University of Texas Southwestern Medical School and Carter Blood Care, United States of America
In the United States, about 40,000 adults, who consider themselves in good health, volunteer to donate blood. All of these individuals are screened, at each donation, for serological markers of infectious disease.
We decided that this screening could provide a ideal opportunity to give donors information about cardiovascular risk if we supplemened the mandated infectious disease testing with a measurement of nonfasting total cholesterol. For this reason, all volunteers donating at Carter BloodCare, the community independent blood program serving Dallas, Fort Worth, and Waco in Texas, USA have total cholesterol levels determined at each donation. They are encouraged to track their results, which are kept private, but can be retrieved from the blood center's web site. This site records if an individual retrieves his or her results.
While information covering an average of 250,000 adults per year since 1998, over all age ranges, has been analyzed, particular attention has been paid to young adults, since they are a group least likely to have had a total cholesterol measurement made previously and most likely to benefit from the knowledge of their cholesterol level.
We found that in the 17 to 19 year old age range, 6.14% of males and 6.74% of females had total serum nonfasting cholesterols greater than 200 mg/dl. Only 20% of the males and 24% of the females retrieved their results.
This surveillance confirms that screening of volunteer blood donors is valuable in identifying a group for whom health education about cardiovascular risk is essential.
359: Hypertriglyceridemic waist in dyslipidemic families. association with adiponectin, atherogenic dyslipidemia, proinflammatory, prothrombogenic and prodiabetogenic changes
H Vaverkova, D Jackuliakova, D NovotnÝ, D Karasek, M Halenka, M Budikova, L Slavik
III. Int. Clin. Medical Faculty and University Hospital Olomouc, Czech Republic
Background Waist circumference is considered as a good marker of visceral fat, which is the source of many adipocytokines and plays an important role in the development of insulin resistance. As it was suggested by Canadian authors, increased waist in connection with increased triglycerides (TAG) can reflect the presence of many cardiometabolic risk factors involved in atherogenesis.
Objectives The aim of our study was to evaluate association of the so called hypertriglyceridemic waist (HTGW) with adiponectin concentrations, dyslipidemia, markers of inflammation, thrombosis and insulin resistance.
Patients We examined 284 dyslipidemic patients and their family members of our outpatient lipid clinic (143 M/141 F), mean age 44.9 ± 14.9 years. HTGW was defined as waist ≥ 90 cm in M and ≥ 80 cm in F + TAG ≥ 2.0 mmol/L. All results were adjusted for age + sex (and to waist respectively).
Results Subjects with the presence of HTGW (+)/n = 87;32F + 55M/ in comparison with HTGW (−) did not differ in LDL-C, but they had significantly lower serum adiponectin concentrations (P < 0.0001), higher TC (P < 0.0001), TAG (P < 0.0001), nonHDL-C (P < 0.0001), apoB (P < 0.0001), lower HDL-C (P < 0.0001) and apoA1 (P < 0.0001), higher tPA (P = 0.041), PAI-1 (P < 0.0001), hsCRP (P = 0.001), ICAM-1 (P = 0.003), uric acid (P < 0.0001), fasting glycemia (P = 0.003) and other markers of insulin resistance-insulin, HOMA, C-peptide, proinsulin (all P < 0.0001). Significantly higher were also SBP (P = 0.003) and DBP(P < 0.0001). After further adjustment for waist, all differences remained significant (at least P < 0.05) with the exception of hsCRP, tPA, ICAM-1, glycemia, SBP and DBP.
Conclusion HTGW is associated with lower adiponectin, with more atherogenic dyslipidemia and with increased markers of insulin resistance and inflammation/thrombosis. Thus, this simple pattern of HTGWcan be considered as a good marker of increased atherogenic risk and should be used routinely in clinical practice.
Supported by grant IGA MZ CR NR/9068-3.
360: Effects of the menopause on blood pressure. A population study
R Cifkova, J Pitha, M Lejskova, V Lanska, S Zecova
Institute for Clinical and Experimental Medicine, Prague, Czech Republic
Objectives The incidence of cardiovascular (CV) disease in women increases after the menopause; the mechanism by which menopause exerts its effect on the CV system is still unknown. Blood pressure (BP) increased more steeply around the menopause. The aim of our study was to elucidate the impact of the menopause on BP in a population random sample.
Design and methods In 2003-2005, a population random sample of 908 women (all residents of a Prague district) aged 45-55 years was examined (respondence rate, 63.9%); complete data were available from 873 individuals involved in this analysis. Women were considered pre- or postmenopausal if their follicle-stimulating hormone (FSH) levels were ≤ 40 or > 40 IU/L, respectively.
Results We found 505 pre- and 368 postmenopausal females. As both groups differed in age (49.0 ± 2.49 vs. 51.6 ± 2.14 yrs; P < 0.001) and BMI (26.3 ± 0.22 vs. 25.4 ± 0.27 kg/m2; P < 0.05), BP and heart rate were adjusted for age and BMI and did not show any difference (118.7 ± 0.7/78.7 ± 0.4 mmHg; 71.2 ± 0.4 beats/min. vs. 119.0 ± 0.9/ 79.2 ± 0.5 mmHg; 69.9 ± 0.5 beats/min; n.s.). Prevalence (27.9 vs. 29.6%), awareness (67.4 vs. 72.5%), treatment (48.9 vs. 56.0%) and control (39.7 vs. 39.4%) of hypertension did not differ either. Multiple regression analysis showed SBP and DBP to be dependent on BMI and heart rate both in pre- and postmenopausal women. No difference in BP slopes in pre- and postmenopausal women was found.
Conclusions In our, rather homogeneous, population random sample of females aged 45-55 years, the menopause, as determined by FSH levels, was not shown to affect BP levels. Similar results were obtained if menopausal status was assessed using patient's history of menstrual bleeding. Thus, the rise in BP after the menopause appeared to be due to increased BMI and ageing rather than to ovarian failure per se.
370: Are social inequalities in coronary heart disease mortality in britain getting wider? An analysis of time trends from 1978 TO 2004
SE Ramsay, RW Morris, PH Whincup, LT Lennon, SG Wannamethee; British Regional Heart Study
University College London, United Kingdom
Objectives To examine whether social inequalities in coronary heart disease (CHD) mortality are increasing over time between 1978-2004, as some previous investigators have suggested.
Methods A socio-economically representative population-based study comprising 7735 men, aged 40-59 years, recruited in 1978-80 from 24 British towns were followed-up until 2004 through the National Health Service Central Register (162, 903 person years at risk). Social class was based on Registrar General's social class classification. Relative hazards and absolute risk differences for CHD death comparing manual with non-manual social classes were calculated.
Results 1001 CHD deaths occurred during follow-up (0.61% per annum). During follow-up a decline in CHD mortality was observed in both manual and non-manual men. The overall hazard ratio comparing manual and non-manual CHD mortality rates was 1.51 (95% CI 1.32-1.73, P < 0.001). However, the relative difference between these groups increased over time; for example, in 55-59 year olds the hazard ratio was 1.99 in the first 5 year period of follow-up (early 1980s), and 2.68 in the 15-20 year period of follow-up (late 1990s). Across all age groups the relative increase over a 20 year calendar period was 1.73: 95% CI 0.98-3.08, P = 0.061. However, with the marked decline in CHD mortality rates, the absolute difference in rates of CHD death between nonmanual and manual groups fell from 4.2% in 1980 to 1.8% in 2000.
Conclusion The relative difference in CHD mortality between manual and non-manual social class groups did not decrease during this period, indeed it may even have increased, although (because of falling CHD mortality rates) the absolute difference decreased. However, there is still considerable scope for reducing social inequalities in CHD mortality in the new millennium.
379: Some antropometric data, habits, and family medical history in young people
OY Tomashevska, YI Dzis, IY Dzis, Danylo Halytsky Lviv National Medical University, Ukraine
Development of the metabolic syndrome (MS) and atherosclerosis starts in young age. The aim of our study was to reveal their risk factors in young people. Methods and results: We examined 392 medical students, 192 males and 200 females, aged 18-33 years (median 20.8 + /0.1). It was performed measurement of body mass index (BMI), waist and hip circumference (WC, HC), blood pressure (BP), and body fat percentage (BFP) based on electric resistance. Students filled in questionnaires concerning their habits and family medical history. T Student test was used for statistics. Overweight was detected in 16.7% and 4.5%, obesity class 1 in 1% and 1% of males and females respectively. Increased WC ≥ 94 cm in males and ≥ 80 cm in females was documented in 10.3% and 13.4%. High BFP was present in 29.5% and 36.5%, too high BFP in 14% and 5.3% males and females respectively. There were normal values of BMI in 62.5% males and 87.3% females with increased BFP. It means that in 27.1% males and 36.5% females there is decreased muscle mass due to low physical activity, because only 35.4% of males and 10.1% of females had moderate to intensive physical exercises ≥ 150 min/ week. BP ≥ 130/85 mmHg was noted in 47.7% males and 19.8% females. In females systolic BP correlated with BMI (r = + 0.324, P < 0.05) and HC (r = + 0.394, P < 0.05). Dietary imbalance was noted in 66.7% males and 56.2% females. It consisted in excessive sugar/salt consumption, deficit of fruits/vegetables, other fibers, proteins, using of margarines, fried vegetable oils, and/or high energy diet. Smoking was noted in 38.9% and 8.8%, mild alcohol consumption 79.6% (moderate in 7.8%) and 59.5%, presence of cardiovascular diseases (CVD) in 1st degree relatives in 37% and 19% males and females respectively.
Conclusion There is high occurrence of different risk factors of MS, CVD and type 2 diabetes mellitus in young people, especially in men. We work on introduction of a preventive program regarding their life style modification.
382: Trend of mortality rates, diabetes mellitus: state of RIO DE JANEIRO, 1998-2003
M Grimmer, MRM Teixeira, ACS Chazan, CLS Pestana
Secretariat for Health of the State of Rio de Janeiro/Brazil
Background Rio de Janeiro State's ageing population contributes for prevalence of non-communicable diseases and risk factors. The NCD respond for 60% of deaths in the state. The prevalence of diabetes, which reaches people irrespective of race, sex or socio-economic conditions, is 7.6% among adults.
Methodology The Mortality Information System-SIM and DATASUS-IBGE population data were used for crude taxes of mortality in years 1998-2003 and mortality rates standardized per age by European population, year 2000. Data were plotted in graph of trends and the ascribable risk assessed. Domiciliary Inquiry on Risky Behaviors and Cited Morbidity of NCD of National Cancer Institute/Ministry of Health was also employed.
Results The amount of deaths for Diabetes in females is greater than in males. A falling trend of mortality rates for DM among females, standardized per European population year 2000 was observed; among males the trend is to stabilization. Deaths of males surmount females' in 40-59 years old group, while above 60 years old this relation reverses. For both sexes, the deaths for DM increases with age, evidencing the importance DM acquires as population ages.
Conclusion The fast ageing of the population and the ascension of chronic conditions produced a gap between health problems and systems, focused in a model of acute cases' treatment. The confrontation of chronic illnesses, especially diabetes mellitus, challenges the country in next years. Promoting health strategies should be implemented to change the current scene.
396: Calcific aortic stenosis: another face of atherosclerosis?
Luis Adão, Vânia Enes, Marlene Fonseca, Francisco Sampaio, Lino Santos, Manuel Gonçalves, Madalena Teixeira, Vasco-G. Ribeiro
Centro Hospitalar de Vila Nova de Gaia, Portugal
Background Calcified “degenerative” aortic stenosis is currently the most common valvulopathy in industrialised countries. Renewed interest for aortic valve disease has evolved in recent years. The latest development refer that apparently the initiation and progression of this disease appears similar to those described for atherosclerosis.
Objectives To compare the prevalence of coronary artery disease and cardiovascular risk factors between old patients with isolated aortic stenosis versus organic mitral valvulopathy.
Methods Retrospective study that included 473 patients older than 65 years, with isolated aortic stenosis or organic mitral disease, which underwent preoperative coronary angiography from January/1999 to December/2003. Evaluated parameters: age, sex, cardiovascular risk factors and significant coronary artery disease (angiographic stenosis ≥ 50%).
Results The isolated aortic stenosis was more frequent (n = 391). We didn't find significant differences in age (73.9 ± 9.1 vs. 71.2 ± 9.1 years). The male sex was more prevalent in the isolated aortic stenosis (60.6% vs. 34.2%, P < 0.001). The patients with isolated aortic stenosis had more dyslipidemia (20.7% vs. 6.1%; P < 0.01). There wasn't significant differences in the prevalence of hypertension (38.4% vs. 29.1%), diabetes (14.1% vs. 14.6%), smoking (5.6% vs. 3.7%) or family history (3.1% vs. 3.7%). The presence of coronary artery disease was higher in patients with isolated aortic stenosis (22.3% vs. 9.8%; P = 0.01).
Conclusions In our population, isolated aortic stenosis was more associated with dyslipidemia and coronary artery disease. The nature of that association needs further studies.
399: The impact of climatological parameters on the incidence of paroxysmal atrial fibrillation
A Douras, K Tsatiris, K Pikros, T Kirlidis, D Kapsalas, T Tsaknakis
Ahillopoulion General Hospital of Volos, Cardiology Department, Greece
Background Climatological Parameters (CP) have been shown to influence the incidence of several cardiovascular diseases. An issue of limited investigation is the impact of CP on Paroxysmal Atrial Fibrillation (PAF). To address this scope, we conducted a prospective study of hospitalizations rates because of PAF in the region of the city of Volos, during a period of 2 winter months.
Material and methods The study comprised 64 consecutive patients of a mean age 60.6 y.o. (29 men, mean age 54.5 y.o and 35 women, mean age 65.4 y.o) who were admitted in the Cardiology Department of our Hospital because of PAF. The Cardiology Department is the only organized cardiology unit in the region. The number of the daily admissions for PAF was correlated with the following regional CP, obtained from the National Observatory of Athens: the daily Mean Temperature, the Relative Humidity Percentage, the Atmospheric Pressure (maximum, minimum, mean), the daily Variation of Atmospheric Pressure as well as its Difference from the preceding day. Stastical analysis was performed with the use of coefficient of correlation of Pearson(r) as well as with the application of regression analysis. A P value of less than 0.05 was considered to indicate statistical significance.
Results For all the CP, except the Relative Humidity Percentage (RHP), the statistical analysis revealed no significant correlation with the incidence of PAF. In regression analysis the daily admissions for PAF had a significant positive correlation with RHP, with a coefficient of 2.2 (CI:0.17-4.270). Plots of the daily RHP versus the daily admissions for PAF suggests a linear relationship.
Conclusion An association between humidity and PAF incidence is established in the present study, which has not been investigated before. According to these results, the prone to PAF patients should be advocated to avoid to be exposed to humid weather. Further research is needed to elucidate the role of CP on the occurrence of PAF.
400: Evidence of myocardial adrenergic innervation abnormalities in hyperlipidaemic subjects: the beneficial effect of statins
ME Marketou, EA Zacharis, SI Koukouraki, VK Prassopoulos, DA Arfanakis, F Karageorgou, AN Giaouzaki, NS Karkavitsas, PE Vardas
Cardiology Dept. Heraklion University Hospital Heraklion, Crete, Greece
Background Hyperlipidaemia results in endothelial dysfunction and myocardial perfusion abnormalities even in the absence of any organic heart disease. We investigated the association of dyslipidaemia with myocardial adrenergic innervation disturbances using I 123 -metaiodobenzylguanidine (I 123 -MIBG) and assessed the effect of statin therapy thereupon.
Methods We included 25 hyperlipidaemic subjects (18 men, aged 59 ± 10 years, while 15 healthy volunteers served as a control group. All subjects underwent a planar and a SPECT myocardial imaging of the heart after an intravenous infusion of 5mCi I 123 -MIBG. Heart to mediastinum ratio (H/M) was used for quantitative assessment of adrenergic innervation, 10 minutes and 4 hours after drug infusion, while SPECT scintigraphy evaluated the regional distribution of adrenergic activity. Fifteen of the hyperlipidaemic subjects received 40 mg/day atorvastatin for 6 months, while the remaining ten received placebo. An I 123 -MIBG study was repeated at six months.
Results The H/M ratio at 10 min and 4 hours in hyperlipidaemics was 1.79 ± 0.21 and 1.73 ± 0.27 respectively; significantly lower than normals (2.25 ± 0.9 and 2.19 ± 0.10 respectively, P < 0.05 for both) and was improved under atorvastatin treatment (1.97 ± 0.7 and 1.9 ± 0.22 respectively, P < 0.05). During SPECT scintigraphy, 17 hyperlipidaemic subjects (68%) showed defects in the inferior wall, nine (36%) displayed additional regional disturbances in myocardial adrenergic activity in the anterior wall and ten subjects (40%) in the apex. These defects were ameliorated mostly in the inferior and anterior wall on re-evaluation, but only in those receiving atorvastatin. No regional disturbances were detected in healthy subjects.
Conclusions This is the first study to show a high prevalence of myocardial adrenergic innervation disturbances in hyperlipidaemic subjects, while the A effect further intensifies the beneficial role of statins.
404: Predictors of incidence of hypertension in a working population
F Leynen, E Clays, G De Backer, F Kittel, M Kornitzer
Dép. Epidémiologie et Promotion à la Santé-Ecole de Santé Publique-ULB, Belgium
Background Besides genetic and bioclinical risk factors, environmental and psychosocial characteristics have been associated with blood pressure (BP) elevation-the relationship between perceived job stress (JS) and ischemic heart disease could thus be partly mediated through an increase in BP. We examined prospectively the relationship between baseline characteristics of the Belstress population, including JS, and the incidence of hypertension (HT) in the second survey.
Methods A total number of 2821 workers who participated in the Belstress-1 project, were included in a second survey after a mean time interval of 6.6 years. JS was investigated by Karasek's Job Content Questionnaire. Only subjects with a systolic BP (SBP) < 140 mmHg, a diastolic BP < 90 mmHg and not taking antihypertensive drugs at baseline were eligible.
Results Of this sub sample of 1082 men and 562 women, respectively 15.2% and 10.0% had an elevated BP (SBP ≥ 160 or DBP ≥ 95 mmHg) or was taking antihypertensive medication at the second survey. In logistic regression analysis incidence of HT was most strongly and significantly related to baseline SBP (OR ≥ 130- < 140 mmHg compared to < 120 mmHg: 5.56 (3.29-9.41)∗∗∗), body mass index (OR ≥ 30 kg/m2 compared to < 25 kg/m2: 3.21 (1.73-5.95)∗∗∗), company (OR highest incidence of HTcompared to lowest incidence: 5.53 (2.08-14.70)∗∗) and psychological job demands (OR tertile 2 compared to tertile 1: 1.93 (1.25-2.98)∗∗). No significant relationship was observed with age, educational level, occupation, alcohol consumption, smoking, job control, social support at work, waist circumference and physical activity.
Conclusions Based on these prospective data we can suggest that, indepentently from a large set of covariates, incidence of HT is positively associated to baseline SBP, BMI, and PJD.
Important differences are observed from one company to the other. This could possibly be explained by work site specific health promotion and prevention strategies.
408: Ankle brachial index is an independent predictor of all-cause and coronary mortality in healthy middle-aged working Belgian men after eighteen year follow-up
JC Wautrecht, M Dramaix, G De Backer, M Kornitzer
Hôpital Erasme, Université Libre de Bruxelles, Brussels, Belgium
Background Ankle brachial index (ABI) has been shown to be an independent variable in different epidemiological studies. We report here results of 18.4 years median follow-up, the longest at the best of our knowledge, in healthy middle-aged working males using the ABI as an independent variable.
Materials and methods 2363 male subjects aged 40 to 55 years were selected in different Belgian industries and attended a screening examination. The screening procedures included standardized questionnaires on angina, intermittent claudication, smoking behaviour, education level, type of occupation and history of diabetes mellitus. Each subject had to undergo the measurement of blood pressure, Body Mass Index, and ABI. ABI was considered abnormal if ≤ 0.9. Blood samples were drawn to measure total-, HDL- and LDL cholesterol, and triglycerides. Proportional hazards (PH) Cox models was applied to derive crude and adjusted hazard ratios (HR) and their 95% confidence intervals (95% CI).
Results Of 2363 subjects, 2291 (97%) had ABI measurements. One hundred subjects (4.4%) had an ABI ≤ 0.9. Among the 2291 men who were screened for ABI, 305 (13.3%) died during the follow-up: 278 (12.7%) in the > 0.9 ABI group and 27 (27%) in the ≤ 0.9 ABI group. After all potential confounding risk factors were tested for selection, ABI ≤ 0.9 predicted an increased risk of all-cause mortality (HR 1.8; 95% CI 1.2-2.6) independently from history of coronary heart disease, age, smoking, systolic blood pressure and BMI. The independent predictive power of ABI ≤ 0.9 for coronary mortality was 2.4 (95% CI 1.1-5.3). There were no significant interaction between ABI and the other variables included in the models.
Conclusion Even after 18 years follow-up, ABI measured in healthy middle-aged working Belgian men remains an independent predictor of all-cause and coronary mortality. Measurement of ABI, a very simple tool, should be recommended as part of check-up in healthy men at midlife for optimizing late primary prevention.
410: Prevalence and control of cardiovascular risk factors in Russian patients with chronic obstructive pulmonary disease
V Pyankov, Y Chuyasova
Kirov State Medical Academy, Kirov, Russia
Objective To estimate the prevalence and control of cardiovascular risk factors and associated clinical conditions in Russian patients with chronic obstructive pulmonary disease (COPD).
Design and method 134 hospitalized men with exacerbation of COPD were included in this study. The mean age of the patients was 64.0 ± 10.2 years. In all patients blood pressure and anthropometric measurements, laboratory tests (LDL-cholesterol, whole capillary blood glucose), instrumental investigations (echocardiography and duplex ultrasound) and questionnaire interviews were performed.
Results The arterial hypertension was detected in 36.5% of cases (49 patients): grade 2 hypertension-in 75.5% (37 patients), grade 3 hypertension-in 24.5% (12 patients). 79.6% of patients with arterial hypertension (39 cases) were older then 55 years. All patients were cigarette smokers (mean smoking history was 41.4 ± 9.7 pack-years). Dyslipidaemia (LDL-cholesterol > 4.0 mmol/l) was detected in 12.7% (17 patients). Abdominal obesity (abdominal circumference ≥ 102cm, BMI > 30 kg/m2) was revealed in 2.9% of cases (4 patients). Associated clinical conditions such as a history of myocardial infarction and angina were revealed in 9.7% of cases (13 patients). Lower extremity peripheral arterial disease was detected in 2.2% of cases (3 patients). Diabetes was detected in 2.2% of cases (3 patients). Only 3.7% (5 patients) had well cardiovascular risk factors control.
Conclusions Our study confirmed high prevalence and low control of cardiovascular risk factors and associated clinical conditions in Russian patients with COPD. Prognosis of these patients is characterized by an increased risk for cardiovascular ischemic events. Physicians should detect and treat these risk factors in patients with COPD in time to prevent severe complications.
412: Recent cv mortality decrease in the Czech republic is due to treatment and secondary prevention rather than to primary prevention
J Bruthans, Z Kamberska
Podøipská nemocnice Roudnice n.L., CZ, Czech Republic
A decrease in cardiovascular (CV) mortality in the Czech Republic started in the mid-1980s, accelerated in early 1990s and continued at lower pace in recent 4-5 years. Standardized CV mortality decreased 1986-2004 by 37.8% in male, by 35.4% in female. Mortality decrease has been more pronounced in acute than in chronic forms of CV diseases. There were rapid and profound positive changes in nutrition and life style and decrease in risk factors after change of political system in early nineties, namely in HDL cholesterol levels, but they slowed down or halted in recent 6-7 years, except for arterial hypertension (further blood pressure decrease and improved control of hypertension in population documented). Drug and interventional therapy and medical secondary CV prevention increased rapidly and steadily since mid nineties (EUROASPIRE I, II, extended Czech MONICA), e.g. share of patiens with AMI treated by direct PCI became the highest in the world (7260 direct PTCA per 10 million pop., Prague I, II, VINO Study and AMI register).
Whereas the major factor influencing CV mortality in nineties was the change of life style and decrease of some CV risk factors, further decrease of CV mortality since late nineties can be ascribed mainly to medical treatment of CV diseases and to secondary medical prevention. Primary prevention impact remained limited. Social differences in CV morbidity and mortality, in level of classical (smoking, overweight) and new risk factors (unemployment), in nutrition and even in access to medical therapy and prevention increased. CV morbidity and mortality shifted towards higher age and lower social strata. Therapy and secondary prevention in older and socially handicapped patients becomes more difficult and costly and of more limited effect. So progress in primary prevention remains reasonable and economically tentative alternative to costly therapy and medical secondary prevention.
421: Long and short-term mortality in acute myocardial infarction in swedish men and women
K Dudas, G Lappas, A Rosengren
Department of Medicine, Sahlgrenska University Hospital/Östra, Göteborg, Sweden
Background Prognosis after AMI has improved considerably over the last two decades. However, changes in long-term outcome over time has not been well studied. We studied out-of-hospital mortality, one-year, and five-year mortality in first-ever AMI in Sweden, using nationwide registries.
Method Data from the Swedish Hospital Discharge and Cause-specific Death Registers were used. All first-ever hospital admissions with AMI or deaths from coronary heart disease (CHD) without prior hospitalisation during the period 1987 to 2002 were included and analysed separately for the age groups < 55, 55-64, 65-74 and 75-84 years. Five-year mortality was studied in patients with a first event before 1998.
Results Deaths from CHD outside hospital decreased, with annual decreases of between 3% and 6%, more markedly in older patients but with no sex differences. In the hospitalised population 1-year mortality decreased by 4 to 6%, more in older patients, but with no difference between men and women. Even more pronounced changes were seen for 5-year mortality, with 6-9% annual decrease, again more markedly in older men and women.
Conclusion In first CHD events in Sweden, there are substantial reductions in out-of hospital mortality, in one-year mortality but above all in long-term mortality in the hospitalised population, suggesting decreasing severity in acute coronary disease, as well as effects of improved treatment. The most substantial reduction in long-term mortality was seen in the oldest men and women.
426: Abdominal obesity as related to risk of diabetes, metabolic syndrome and coronary disease in turkish men: a prospective study
Onat Altan, Uyarel Huseyin, Hergenç Gulay, Karabulut Ahmet, Albayrak Sinan, Can Gunay
Turkish Society of Cardiology, Turkey
Objectives We aimed to investigate, determinants of abdominal obesity and its clinical impact on metabolic syndrome (MS), diabetes (DM) and coronary heart disease (CHD) in men. Methods: Prospective evaluation of 1638 male participants (aged 48.5 ± 12.3), representative of Turkish men. For components of MS, criteria of NCEP guidelines were adopted, modified for abdominal obesity. Follow-up constituted 9650 person-years.
Results Insulin level (relative risk [RR] 1.40 for doubling), C-reactive protein (CRP) and heavy smoking (protective) were independent predictors of newly developing abdominal obesity. High triglyceride and low HDL-cholesterol were significantly associated already with waist girth quartile II, apolipoprotein B with quartile III. In predicting elevated BP, hazard ratio (HR) of waist girth (1.77) was more powerful than a decade of age. Waist girth significantly predicted future MS from Quartile II on [RR of 2.7 (95% CI 1.39; 5.26)] independent of fasting insulin and CRP levels, whereby its HR (2.4) was equivalent to quadrupling of fasting insulin levels. CRP independently predicted MS. HR of waist girth (1.51) was significant in predicting DM when controlled for five confounders. Abdominal obesity conferred no significant risk for CHD or overall mortality independent of elevated BP, CRP, or smoking. As judged by sensitivity and specificity rates for future CHD, DM and MS, abdominal obesity was most appropriately defined with a waist girth of ≥ 95 cm, and an action level 1 of ≥ 87 cm was proposed for MS.
Conclusions Serum insulin, CRP levels and (inversely) heavy smoking are predictors for abdominal obesity in Turkish men. Atherogenic dyslipidemia and elevated blood pressure are associated significantly already with modest rises in waist girth adjusted for age and smoking. Increasing waist girth was predictive of MS, more strongly than being predictive of DM. Risk for CHD or overall mortality imparted by abdominal obesity is mediated by risk factors it induces.
429: Obesity and overweight in relation to socioeconomic status
L Björck, DS Thelle, L Lissner, A Rosengren; Intergene programme
Department of Medicine, Sahlgrenska University Hospital/Östra, Göteborg, Sweden
Background Overweight and obesity are by and large, the results of weight gain from youth to middle age. Socioeconomic determinants for weight gain from young adulthood to middle age have not been well studied.
Methods The Intergene programme was conducted during April 2001-August 2004 in the Göteborg municipality and region. 1702 men (47%) and 1906 women (53%), 45-75 years were included. We examined weight gain from self-assessed weight at the age of 20 until middle age in relation to socioeconomic status in Swedish men and women.
Results Women with higher education did not only gain less weight in per cent over time in age groups from 45 to 65 +, but also had a lower mean BMI in all age groups at the examination. Mean BMI in younger men and women (< 45) with high education, based on measured weight and height was 25.3 and 23.8 kg/m2 respectively. This increased with age and in ages 65 + mean BMI was 26.7 and 26.4 respectively. Among all women, regardless of education and age group, the self estimated BMI (height and length) at age 20 was about 21. In men with low education the estimated BMI was about 22, except in men 65 + (born before 1940), who had a mean BMI at age 20 of about 21. In women aged 45 to 54 and 55 to 64 weight gain was 19 and 21% respectively in women with low education compared to 16% in corresponding groups with high education. In older women (65 +) the weight gain was 20 and 18% respectively in low and high education groups. In men there was no significant difference between men with high and low education with respect to weight gain from the age of 20. In women, but not in men, we found a significant lower weight in smokers, compared to non-smokers.
Conclusions In men there was less difference in self-assessed weight at the age of 20, in current weight as well as in weight gain, in relation to education, whereas women with high education, both gained less weight during life and had a lower current weight, compared to women with lower education.
437: The increase in the burden of cardiovascular diseases and diabetes during 2005-2025: the impact of ageing and obesity
WMM Verschuren, A Blokstra, CA Baan, RT Hoogenveen, HC Boshuizen; Centre for Prevention and Health Services Research
National Institute of Public Health and the Environment, Netherlands
Background The incidence and prevalence of chronic diseases rise with age. Therefore, in the near future the burden of cardiovascular diseases and diabetes is expected to increase in ageing populations.
Methods We projected the disease burden for the period 2005-2025 in the Netherlands, based on demographic changes (ageing of the population) and the effects of an increasing prevalence of overweight/ obesity (body mass index (BMI) ≥ 25 kg/m2). We will report here the results for myocardial infarction (MI), cerebrovascular diseases (CVA) and diabetes type II (DM). We used a dynamic multi-state transition model, which has been especially developed for modelling changes in disease incidence and prevalence, taking into account changes in lifestyle factors and risk factors (such as smoking, obesity, but also age).
Results Based on ageing alone, prevalence of MI will increase from 310.000 in 2005 to 365.00 (+ 18%) in 2025, prevalence of CVA from 185.000 in 2005 tot 290.000 (+ 57%) in 2025 and prevalence of DM from 550.000 in 2005 to 870.000 (+ 58%) in 2025. A continuation of the increasing trend in overweight/obesity will especially have a large impact on the prevalence of DM, leading to a total prevalence in 2025 of 940.000 (+ 70% compared to 2005). When the increase in BMI will be accelerated, and the prevalence of overweight/obesity will reach American levels, the number of diabetics in the Netherlands will be more than 1 million in 2025 (+ 90% compared to 2005).
Discussion The burden of MI, CVA and DM will substantially increase in the next 20 years. The increase in MI due to ageing, is partly counteracted by the downward trend in incidence rates of MI. For CVA and DM the increase due to ageing is almost 60% in the next 20 years. For DM this increase might even be as big as 70-90%, depending on the magnitude of the rise in prevalence of overweight and obesity.
445: Risk factors and 5-years survival after CABG
M Zdravkovic, M Ristic, N Milic, SU Pavlovic, M Deljanin, D Zdravkovic, N Milinic, R Zivkovic
Hospital Medical Center Bezanijska Kosa, Serbia and Montenegro
Background Serbia, except Hungary, has the greatest incidence of coronary artery disease in Europe. Risk factors for CAD are well known and sometimes they are multiple.
Aim The aim of the study was to evaluate the incidence of risk factors in patients with CABG and its influence on 5-years survival after CABG.
Methodology Risk factors were evaluated in 250 patients with CABG operated in 1999 and 2000. Follow-up period was 60 months. Survival rate was 84.2%.
Results The most frequent risk factor was smoking, both in men and women. Even 88.8% of the patients were smokers. 80% of patients had positive family history and 68% had hypertension. Hyperlipoproteinemia was found in 81.6% of patients with CABG and 27.6% were with obesity. Every fifth patient had diabetes mellitus. Using multivariante analysis we found that smoking was the independent risk factor for worse 5-year survival, since other risk factors did not influence 5-years survival.
Conclusion All investigated risk factors are significantly frequent in patients with CAD and CABG comparing to normal population (P < 0.05). However, only smoking influences 5-year survival after CABG.
448: Secondary prevention in high risk patients with CAD: from guidelines to clinical practice
DS Dourtsiou, JP Bozia, KD Theodoridis, DA Labrou, FL Borghi, ES Karras, GA Savvopoulou, NL Papadopoulou, EA Panagiotidou
KA Gotsis Department of Cardiology, General Hospital of Komotini, Greece
Aim To examine adherence to current guidelines for primary and secondary prevention in high-risk patients.
Methods 526 consecutive patients with hypertension were studied (221 males (M) and 305 females (F) aged 64.8 ± 8.2 years old) who were examined in the outpatient clinic. 189 of them (116 M and 73 F aged 65.5 ± 7.7 years old) had known CAD or equivalent. Detailed medical history was taken and height, weight, waist circumference were measured. Lipid levels and fasting plasma glucose (FPG) were examined as well.
Results 16% of the patients were smokers (M:20.8%, F:8.2%) and 42% ex-smokers (M:63.8%, F:6.8%), 43% were obese (M:37%, F:52%) while 14% had normal body weight. 79.5% claim that they have examined at least once their lipid levels, 67.5% state they have hyperlipidaemia and 59% are under lipid lowering therapy (TC: 194 ± 31, LDL: 115 ± 26, LDL < 100mg/dl: 27.8%). 8.4% do not receive lipid lowering therapy (TC: 276 ± 82, LDL: 171 ± 59, LDL < 100 mg/dl: 8.3%). 11.4% claim they have normal lipid levels (TC: 221 ± 41, LDL: 150 ± 38, LDL < 100 mg/dl: 5.6%) and 21.1% do not know (TC: 234 ± 48, LDL: 155 ± 45, LDL < 100 mg/dl: 7.1%). 83% have examined their FPG levels and 36% have known diabetes (DM). FPG examination disclosed IFG in 18.2% and DM in 8.8% of patients (WHO classification 1999). Although 57.5% claim that BP is satisfying controlled, in 12.4% a BP < 140 mmHg was measured while 28.5% (M: 21%, F: 40%) had BP > 180 mmHg.
Conclusions There is a discordance between guidelines and clinical practice. Secondary prevention in patients with CAD and other coexisting risk factors is insufficient. One out of 5 do not know their lipid and FPG levels, while the majority of the rest of them either is not under lipid lowering therapy or is treated insufficiently. Only 1 out of 5 has succeed lipid target levels and more than 1 out of 4 have abnormal glucose regulation that are not aware of. Furthermore, BP is not under control (only 1 out of 8 had admission BP in the acceptable limits).
454: Different levels than expected in visceral fat and waist circumference on a Latinoamerican population
C Ponte, C Mendoza, N Vargas, I Brajkovich, L Machado, J Isea-Pérez
Department of Cardiology “Dr. Domingo Luciani” Hospital. Caracas, Venezuela.
Values of waist circumference as an anthropometric correlate to visceral fat representative of cardiovascular risk have been defined for European, Japanese and North Americans and from them extrapolated to Latino American populations to assist in metabolic syndrome diagnosis. This situation can be misleading both to individuals and populations alike since the extrapolated measurements could not reflect the real values for them.
To evaluate the real level of visceral fat and waist circumference of a Venezuelan population we have conducted a study in a cohort of 97 cardiovascular healthy individuals (48 men and 49 women, 18 to 69 years old) who attended the Radiology Department at 6 hospitals in Caracas, Venezuela, from July to November 2005. All the subjects were evaluated in a standardized manner to obtain waist circumference in centimeters and amount of visceral fat; this last was done in Hounsfield units using helical computed tomography measurements obtained at the L4-L5 vertebrae level.
This waist circumference and amount of visceral fat were correlated. Following data previously published, a visceral fat area of 100 cm2 was considered associated with alterations in cardiovascular risk profile.
The waist circumference correlated (liner regression) with the 100 cm2 amount of visceral fat for these subjects was 89 cm for men (r = 0.7207; P < 0.0001); and 88 cm for women (r =0.8597; P = 0.0001).
These newly determined levels of waist circumference are different than the ones previously used and clearly emphasize the importance of locally obtained measurements of biological significance.
473: Self reported diabetes predicts risk of cardiovascular death differently in men and women in high risk European countries: the score project
C McGorrian, AP Fitzgerald, T Leong, EB Hand, IM Graham
The Adelaide and Meath Hospital, Tallaght, Dublin 24, Ireland
The SCORE risk prediction charts do not include diabetes mellitus as a separate risk factor, and suggests that the calculated 10 year risk of fatal cardiovascular event should be multiplied by two in diabetic men and four in diabetic women. We examined the incidence of diabetes in this large cohort, and compared hazard ratios for diabetes in the “high risk” countries: Denmark, Britain, Scotland, Norway, Sweden and Finland.
The constituent studies questioned patients on whether they had diabetes, or whether a doctor had told them that they had diabetes. Using a Cox regression model, with age as time variable, we modelled the hazard ratios for self reported diabetes in those subjects free of cardiovascular disease at the start of the surveys. We controlled for blood pressure, serum cholesterol and smoking.
In total, 122 108 subjects were included, 1564 of whom had self-reported diabetes (1.3%). Some heterogeneity was noted between the hazard ratios for men and women in the different cohorts. In a combined model, stratified by cohort, the hazard ratio associated with self reported diabetes was 2.91 in men (95% CI 2.55-3.33) and 5.37 in women (4.42-6.52), P < 0.000. Interaction analyses demonstrated that the gender differences in the Finnish, Norwegian and the total combined cohorts were significant.
Calculated hazard ratios for self reported diabetes in men and women
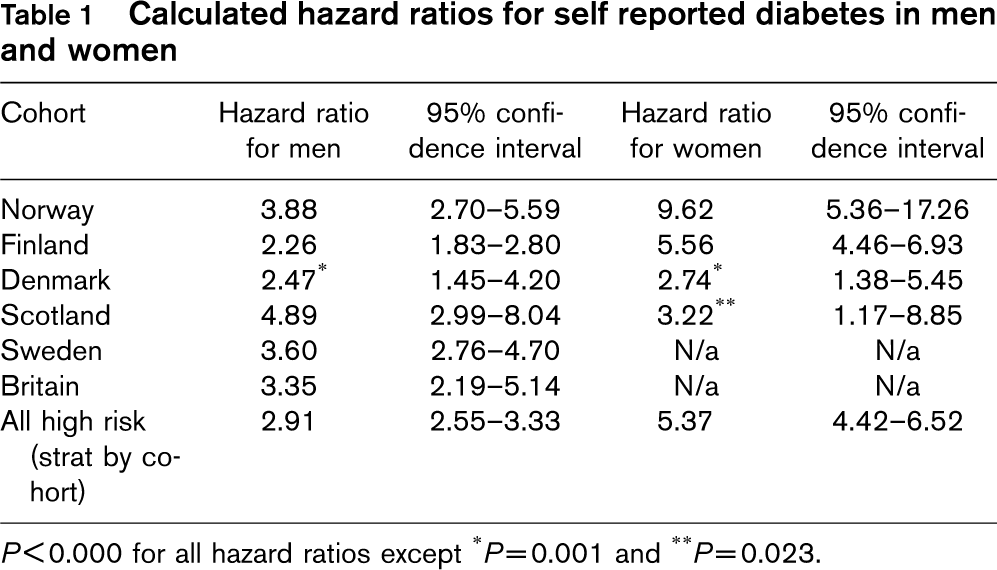
P<0.000 for all hazard ratios except
∗P=0.001 and
∗∗P=0.023.
Self-reported diabetes is a significant risk factor for CVD, and its effect varies in men and women. Future risk prediction systems should incorporate an indicator of glycaemic status.
484: Trends in myocardial infarction in Portugal: 1993-2003
P Marques-Vidal, S Marques-Vidal, C Matias Dias
Centro de Nutrição e Metabolismo, IMM, Faculdade de Medicina de Lisboa, Portugal
Objective to assess the trends in myocardial infarction (MI) in Portugal for period 1993-2003.
Methods Data from all hospital admissions that occurred in the Portuguese National Health Service (SNS) between 1993 and 2003. Only patients whose first diagnoses were coded 410, 411 and 412 (ICD-9) were included.
Results 138,958 hospitalizations for MI were analysed (92,238 men and 46,720 women). In men, the number of hospital admissions for MI increased from 6,317 in 1993 to 9,582 in 2003 (a 52% increase), whereas for women the corresponding figures were 3,047 and 5,396 (a 77% increase). This increase was stronger among subjects aged over 75 in both genders. Mortality rates were higher in women, and decreased from 17% in 1993 to 14% in 2003, whereas in men the corresponding figures were 11% and 8%. After adjusting for year, women with MI were significantly older than men (71.4 ± 0.1 vs. 63.4 ± 0.1, P < 0.001). Conversely, no between-gender differences were found regarding total duration of hospital stay, although men remained slightly more time on ICU (1.3 ± 0.1 vs. 1.1 ± 0.1 days for women, P < 0.001). Finally, after adjusting for age and gender, total hospital stay decreased significantly from 11 to 9 days in 1993 and 2003, respectively (P < 0.001).
Conclusion The number of hospital admissions for MI has increased considerably in the last 10 years in Portugal, namely among women. Mortality has decreased, but women present a higher mortality, partly due to being older.
486: Non-participation and mortality in different socio-economic groups; finrisk population surveys in 1972-1992
K Harald, V Salomaa, P Jousilahti, S Koskinen, E Vartiainen
National Public Health Institute, Helsinki, Finland
Declining response rates pose a serious threat to the validity of estimates derived from epidemiological studies. If respondents and non-respondents differ systematically from each other, the results of the study can be biased. We conducted a population-based cohort study to investigate differences in the socio-economic structure between respondents and non-respondents and the contribution of these differences to total and cardiovascular mortality. Data comprised 32354 male and female participants and 4890 non-participants aged 35-74 who belonged to the sample in one of the five FINRISK surveys in 1972, 1977, 1982, 1987 or 1992. The average response rate of the surveys was 84%. Respondents and non-respondents were followed-up until the end of 2001. We found that the lower socio-economic groups were overrepresented among non-respondents both in men and women. Manual workers had a lower response rate compared to employees and this was also true for the lowest income tertile compared to the highest tertile. When comparing the relative risk of death using the highest socio-economic group of the participants as the reference group, we found that although the socio-economic gradient was similar for participants and non-participants, i.e. the lower groups had a higher risk of death, the risk was at a higher level among non-respondents. This was especially the case for the lower socio-economic groups of non-participants. For example, male manual workers who did not participate, had a 3.18 (CI 95% 2.52-4.01) times higher risk of dying than upper-level employees who participated. The corresponding excess risk for male manual workers who participated was 1.74 (CI 95% 1.41-2.15). We conclude that basing analysis on participants did not substantially distort the relative risk of death associated with socio-economic position. However, it did underestimate the absolute risk.
513: Italian national register of major coronary events: attack rates and fatality in different areas of the country
Luigi Palmieri, Alessandro Barchielli, Giancarlo Cesana, Enrico de Campora, Carlo-Alberto Goldoni, Paolo Spolaore, Massimo Uguccioni, Federico Vancheri, Diego Vanuzzo, Simona Giampaoli
Istituto Superiore di Sanità, Rome, Italy
Aim The national register is a monitoring surveillance system of fatal and non-fatal events in the general population ages 35-74 years; it was launched in Italy at the end of the 1990's with the aim of estimating the occurrence and fatality of coronary events in different geographical areas of the country.
Materials and methods Two sources of information were used to assess current events: death certificates and hospital discharge diagnosis registers. Once the events were identified through the International Classification for Diseases-ICD9 codes and the duration of the event, the number of current events in each single area was multiplied for the positive predictive value of each specific mortality or discharge code derived from a sample of suspected events validated by applying the MONICA Project diagnostic criteria. Attack rate was calculated as the mean value of a two-year period, dividing the average number of estimated events by the average resident population; case fatality was calculated at 28 days from admission as fatal and total events ratio.
Results Attack rates are higher in men than in women: mean age-adjusted (Italian population 1998) attack rate of all areas was 33.9 per 10,000 men and 9.1 per 10,000 women; age-adjusted 28-day case fatality was higher in women (35.5%) than in men (27.3%). Statistically significant geographical differences in comparison with the mean attack rate of all areas were found both in men and women. Case fatality rates result significantly heterogeneous when compared among areas in men but not in women.
Conclusions Results show that there still exist some differences in the geographic distribution of attack rate and fatality of coronary events which seem to be independent from the North-South gradient. These data show the feasibility of implementing a population-based register, essential for cardiovascular diseases surveillance.
546: Defining risk factor profile of patients with and without coronary artery disease, in a population group in a European country with high burden of heart disease: a case control study from Romania
Umair Mallick, Marcus Flather, Maria Dorobantu, Gabriel Tatu, Ana Fruntelata, Tiberiu Spircu, T Zhang, Ameet Bakhai, Duolao Wang, Craig Ritchie; RACS Investigators
Royal Brompton Hospital, London, United Kingdom
Background The age adjusted risk of coronary artery disease (CAD) is rising in countries with economies in transition, particularly in Eastern European region.
Objective We evaluated profile of risk factors for Coronary Artery Disease including demographic and socio-economic factors in a sample of Romanian population and investigated potential causes for this.
Methods In a single centre Case Control study in a main University Hospital, we enrolled 200 cases with and without ST elevation acute coronary syndromes (ACS), and 200 age and sex matched (± 2 years) Control subjects (without CAD) over a period of 14 months.
Results Data from 167 cases matched in pairs with 84 controls was analyzed. Mean age of the population was 61 years and 32% were females. More cases had history of hypertension, stroke, diabetes or a family history of CAD (4%, 9%, 16% and 58%) as compared to controls 40% (P ≥ 0.001), 1% (P = 0.02), 14% (NS) and 38% (P = 0.002) respectively. Higher stress (P = 0.008, OR 2.91, CI 1.32-6.31)), increased BMI (P = 0.003, OR 1.08, CI 1.01-1.16)) and Waist/Hip ratio (P = 0.001, OR 4.22, CI 1.74-10.25) were significant predictors of developing an ACS. Cases appeared better educated (43% vs 31%; P = 0.07), had higher income (106 vs 75 $US per month) and interestingly were more likely to live in urban areas. Controls appeared to have lower cholesterol levels (P = 0.001), and better diet and exercise habits.
Conclusions Similar to the findings from Western European Countries, our data also reflects presence of conventional risk factors in the Romanian subjects. However, stress and poor socio economic status can be regarded as particularly important in this part of Europe. An increased susceptibility of affluent and better educated sectors to develop ACS should be further investigated particularly in relation with the conventional risk factors. Well designed public health programs, based on locally available data about risk factors, can reduce burden of CAD in these regions.
550: Dietary intake and food sources of polyunsaturated fatty acids in belgian women
Isabelle Sioen, John Van Camp, Stefaan De Henauw
Department of Public Health-Ghent University, Belgium
The intake of total fat, saturated, mono-unsaturated, poly unsaturated fatty acids (SFA, MUFA and PUFA) and individual n-6 and n-3 PUFAs was estimated in 641 female subjects (18 to 39 years), randomly selected in 2002 in the city of Ghent, Belgium.
Food intake was recorded on two days for the estimation of energy, total fat, SFA, MUFA, PUFA, linoleic (LA), á-linolenic (LNA), arachidonic (AA), eicosapentaenoic (EPA), docosapentaenoic (DPA) and docosahexaenoic (DHA). Mean total fat intake was 77.6 g/d (34.3% of total energy intake (%E)). Mean intake of fatty acid subgroups was 30.9 g/d (13.7%E), 29.6 g/d (13.1%E) and 13.4 g/d (6.0%E) for SFA, MUFA and PUFA, respectively. The mean intake of LA was 11.9 g/d (5.3%E), that of LNA was 1.4 g/d (0.6%E), with a mean LA/LNA ratio of 8.7. The mean intake of AA was 55.9 mg/d (0.03%E). The mean intake of the long chain (LC) n-3 PUFAs was 77.8 mg/d (0.04%E), 25.3 mg/d (0.01%E) and 131.3 mg/d (0.06%E), respectively for EPA, DPA and DHA.
In view of recommendations, the total fat, SFA and MUFA intake is high. In contrast, the PUFA intake is very low on population level. The intake of LNA and LC n-3 PUFAs was in a majority of individuals below the recommendations of for LNA and for EPA + DHA. Main sources for fat and SFA were dairy products and sweet products (pastry and desserts), whereas the group of fats and oils and the group of meat, poultry and eggs were the main sources of MUFA and PUFA. For both LA and LNA, fats and oils were of major significance, followed by cereal products. The main sources of LC PUFAs were fish and seafood, and meat, poultry and eggs. The former was of major importance for the n-3 LC PUFAs and the latter for AA.
Conclusion Population intake for omega-3 PUFAs is low compared to recommendations. From a public health perspective, it seems desirable to take initiatives tackling this problem.
552: Cardiovascular disease risk estimation in the old. adapting and extending the score chart using data from the reykjavik study of subjects over age 70
T Aspelund, V Gudnason; Reykjavik Study phase 6: 1990-1996
Icelandic Heart Association. Iceland
Background Risk charts for cardiovascular disease (CVD) are mainly available for people of age 35 to 70. Further cohort studies with new data are needed to produce a systematic CVD-risk assessment for the old. SCORE system based risk chart for fatal cardiovascular disease was derived from the Reykjavik study.
Methods Data from 748 men and 929 women (mean age 76 years, range 70-87) without previous coronary event at entry between 1990 and 1996 was used. The 95th percentile of follow-up time until death or January 1st 2003 was 10.9 years. Fatal coronary heart disease (CHD) and fatal non-CHD CVD endpoints were defined as in the SCORE system. Weibull survival model stratified by gender with age as time scale and delayed entry was applied using the STATA software. 10-year risk of fatal CVD was computed in a single step and by adding together the 10-year fatal CHD and non-CHD CVD risk. The risk factors used were systolic blood pressure (BP), total cholesterol, and smoking. Also considered were hypertension (HTN) medication use, diabetes and family history of myocardial infarction (fhMI).
Results People above 70 years are of considerably higher 10-year risk of fatal CVD than younger people estimated from conventional risk factors. The most significant risk factors were BP levels, HTN medication use, and smoking. Subjects entering already on HTN medication had significantly higher risk (HR= 2.54) of fatal CVD irrespective of BP levels. Risk of fatal CHD increased with increasing cholesterol but there was a non-ignorable u-shape effect of cholesterol on non-CHD CVD risk. The effect of cholesterol on total fatal CVD risk in the old is not as prominent as in younger individuals. Diabetes (HR = 1.65) and fhMI (HR = 1.36) were significant risk factors in the old.
Conclusions Similar format of the SCORE risk chart can be applied to the elderly if HTN treatment is taken into account. Guidelines regarding diabetes, family history of MI are valid for the old as for the young.
558: The chronic psycho-social stress as major risk factor for heart disease and death in Romania
Radu M Negoescu; for the CINDI-PUCIOASA 2000 group
Institute of Public Health in Bucharest, Romania
Background A short series of postmortem data from 1989's Romania suggest 9% of country's CVD mortality-one of the highest in Europe-is left unexplained by structural heart and vasa conditions. Since then psychosocial stress (PS), exacerbated after the revolution over an already undermined terrain, is strongly suspected to have triggered arrhythmic incidents or SCD in a significant number of asymptomatic individuals.
Methods Pucioasa in Sub-Carpathians (16,3000 inhabitants) has been chosen as EURO-CINDI demonstration area due to the mix urban and rural life style common in Romania. The life style questionnaire applied to a random sample of 564 subjects (272 Males-M, 292 Females-F) with 43.8 + −14.6 (SD) years (y) of age included a chapter devoted to PS factors that were classified cf. to Dato's 10 items scale as minors (items 3,5,6,8) or majors.
Results Prevalence of majors items of 54.3% in M and 50.9% in Franked PS as the first among CINDI common risk factors for noncommunicable diseases, given smoking prevalence of 48.9% in M and 26.7% in F or daily use of alcohol by 25.9% M and 11.0% F. Top prevalence of majors items in M was 75% at 45-49 y then decreased, while F reached 70% at 50-54 y then stayed the course. Loss of job was most frequent in both M and F (average weight 21.5%) but in F that peak at 30-44 y was accompanied by family dissolution (around 4%), despite their sustained active coping on Lazarus' scale. Consequently, while among the 52.5% chronic patients CVD morbidity peaked 30.3%, mental disorders scored not less than 5.0% mainly in F at 35-39 y.
Conclusion The life style found in a typical Romanian town was primarily featured by major psychosocial stress (mainly accused by young adult females) followed by excessive smoking in bots genders, and alcohol abuse in men. This deadly triad is perhaps synergizing for a quite long lapse of time holding undeservedly the life expectance at birth in early 2000's Romania significantly under the European average.
562: The role of vagal function in the prevention of and risk for cardiovascular disease and mortality
JF Thayer, RD Lane
The Ohio State University, United States of America
Cardiovascular disease (CVD) is the leading cause of death and disability worldwide. The understanding of the risk factors for CVD may yield important insights into the prevention, etiology, course, and treatment of this major public health concern. We review the evidence for the role of vagal function in the risk for cardiovascular disease and mortality. Using a broad range of indicators of vagal function including resting heart rate, heart rate recovery, heart rate variability, and baroreflex sensitivity we show that decreased vagal function is associated with an increased risk for morbidity and mortality. These effects are independent of traditional risk factors including hypertension, diabetes, cholesterol, smoking, obesity, physical inactivity, family history, and age. Moreover, we show that decreased vagal function is associated with both traditional and emerging (inflammation and psychosocial stress) risk factors as well as modifiable and non-modifiable risk factors. Most importantly we provide evidence to support the notion that decreased vagal function precedes the development of a number of risk factors and that modification of risk profiles in the direction of lower risk is associated with increased vagal function. Thus exercise, diet, and other factors that increase vagal function may emerge as important new cardiovascular disease prevention strategies. We close with a brief overview of the neural concomitants of vagal function and suggest that a model of neurovisceral integration may provide a unifying framework within which to investigate the impact of risk and prevention factors on cardiovascular disease.
565: Epidemiological characteristics of acute myocardial infarction in population of NIS
I Burazor, M Burazor, S Ciric-Zdravkovic, S Nagorni, M Lazovic, L Pesic
Clinic for Cardiovascular Diseases, Clinical Center Nis, Serbia and Montenegro
Background and aims Acute myocardial infarction (AMI) accounts for the majority of deaths around the world. During the last years the number of patients with AMI admitted to CCU of our clinic has raised. We wanted to present the distribution of AMI and major characteristic among the population of Nis.
Methods We analyzed data of all patients with AMI who have been admitted in Coronary Care Unit of Clinic for Cardiovascular Diseases in Nis, since the formation of the Unit in 1974.
Results Since January 1974 till July 2005 the number of patients who were hospitalized with diagnosis acute myocardial infarction was 7662 of which 6535 had AMI with ST segment elevation (61.23 years of age, 67.78% males) of whom 15.9% died during hospital stay. The youngest patient was 18 and the oldest 94 years of age old. AMI is the most frequent in April and May; while in July the number of patients was the lowest. In 1974 total of 121 patients was admitted to CCU, in 1984 the number increased up to 201 pts, in 1994 the total was 234 pts and in 2003 the number was 435 pts. The majority of patients were smokers (63%), 59% had hypertension, 43% pts had dyslipidemia, 29% diabetes mellitus. There was no difference in localization (47% anterior vs 49% inferior). The first fibrinolytic treatment was applied in 1985, the totals of 28% pts were given streptokinase and other agents.
Conclusions The results of our study showed that between patients with myocardial infarction the majority were man. Unfortunately, the incidence of AMI in last several years increased, mostly after the bombing in 1999. Among risk factors, the majority of patients were smokers.
582: Sex differences in angina pectoris: meta-analysis of international variations in 53 studies in 23 countries
Claudia Langenberg, Elizabeth Barrett-Connor, Jacqueline Damant, Harry Hemingway
Department of Epidemiology and Public Health, University College London, UK
Background The male excess of myocardial infarction is remarkably consistent across countries with widely differing absolute rates of coronary mortality. Sex differences in angina, a more common manifestation of coronary disease, have not been investigated across countries.
Objectives To determine sex differences in angina prevalence in women and men from countries with different myocardial infarction death rates.
Data sources We searched MEDLINE and EMBASE and contacted experts until December 2005. Acute myocardial infarction (AMI) mortality rates corresponding to survey year, participant age and country were obtained from the WHO mortality database.
Study selection Healthy population studies that included the Rose angina questionnaire.
Results 53 studies of 12,882 angina cases in 157,922 women and 10,947 cases in 145,421 men, from 23 countries (17 languages) were included. Angina prevalence varied widely, from 1.49-15.4% in women and 0.81-15.1% in men. Overall, a female preponderance of angina was observed with a mean female versus male prevalence ratio of 1.22 (range 0.40-3.4). This female excess was seen in surveys with a mean age of women ≥ 50 years (1.23), 51-64 years (1.21) and ≥ 65 years (1.25), and among surveys carried out before 1980 (1.32), between 1980-89 (1.29) or after 1999 (1.11). Meta regression analyses yielded similar results, the pooled sex ratio from a random effects model was 1.19 (95% CI 1.11, 1.27) with significant heterogeneity between studies (P ≥ 0.0001). The mean sex ratio for AMI mortality was, by contrast, 0.28, with rates in women ranging from 1.1-1564.4 per 100,000. Angina prevalence was not associated with AMI mortality in either sex, nor was the sex ratio in angina associated with the sex ratio in AMI.
Conclusions Women have a similar or higher prevalence of angina compared to men across countries with widely differing coronary mortality, over time, and at differing ages. Male sex is not a risk factor for angina.
585: Impact of ethnic background and methylenetetrahydrofolate reductase genotype on age at onset of coronary artery disease among women in Israel
Aviv Mager, Nira Koren-Morag, Mordechai Shohat, Shadan Lalezari, Alexander Battler, David Hasdai
Rabin Medical Center, Beilinson Campus, and Tel-Aviv University, Tel Aviv, Israel
Background An association between the c677t mutation in the methylenetetrahydrofolate reductase (MTHFR) gene with the risk and age at onset of coronary artery disease (cad) has been demonstrated in some populations with certain ethnic backgrounds. However, the specific effect of this mutation on the development of CAD in women is not well-established. We examined the possible effects of the MTHFR genotype and ethnic background on age at onset of CAD in women in Israel.
Methods We studied 135 Jewish women with well-documented CAD (62 Ashkenazi, 44 oriental and 29 with other origins) in whom CAD symptoms first developed at age < 65 years. DNA samples from 278 women served as control.
Results CAD symptoms developed later in Ashkenazi than in Oriental ones or women with other origins (at 51.0 ± 7.2 years, 48.3 ± 7.5 years and 46.3 ± 7.7 years, respectively, P = 0.016, 2-way ANOVA). Among Ashkenazi women, the MTHFR T/T (homozygous mutant) genotype was less common in those who had CAD onset at age > 50, 6.4%, than either in those who had CAD symptoms earlier (25.8%), or the Ashkenazi control subjects (23.3%, P = 0.037 and P = 0.045, respectively). Among women with Oriental or other origins, these differences were not significant. Logistic regression analysis showed that the T/T genotype was associated with a marked increase in the risk of CAD onset at age < 50 years (OR = 3.87, 95% C.I., 1.12-13.45, adjusted for risk factors and origin) and a trend towards an influence of ethnic origin (P = 0.08). As compared to Ashkenazi women, the risk of early development of CAD associated with the T/T genotype among Oriental ones was 0.46 (95% CI, 0.189-1.114) and among women with other origins-5.84 (95% CI, 1.76-19.34). An increment of one risk factor increased the risk of earlier onset of CAD by 42% (OR = 1.42, 95% CI, 1.06-1.89).
Conclusions Among Israeli women, the age at onset of CAD is influenced by the MTHFR genotype and by the ethnic origin. The mutation has a stronger effect on women of Ashkenazi than Oriental origin.
592: Twenty-five years monitoring of coronary heart disease risk profile of ukrainian population
I Gorbas, I Smyrnova, O Kvasha, N Davydenko, O Malatskivska
Research Institute of Cardiology, Kyiv, Ukraine
Comparison of results of accomplished epidemiological investigation of urban male and female population aged 20-64 years (1975 persons) with the same indicators, which have been done 25 years ago (2435 persons) allows to analyze dynamics of epidemiological conditions of coronary heart disease development in Ukraine and corresponding epidemic situation in the region.
During the period of 25 years it has been noticing change for the worse of risk profile of male population depending on increasing of the prevalence of arterial hypertension (≥ 140/90 mm Hg) by 9.2% and low physical activity-by 20.4%. Among female population the frequency of hypercholesterolemia (≥ 6.2 mmol/l) rose by 8.7%, smoking-by 10.0% and low physical activity-by 16.1%. The prevalence of another risk factors still remains stability high. The frequency of main risk factors consists: among male population-smoking-44.0%, arterial hypertension-39.8%, low physical activity-39.1%, overweight (25.0 ≤ BMI ≤ 29.9 kg/ m2)-37.5%, hypercholesterolemia-22.4%, hypertriglyceridemia (≥ 2.1 mmol/l)-15.0%, obesity (BMI ≥ 30.0 kg/m2)-14.6%; among female population-low physical activity-48.6%, arterial hypertension-30.8%, overweight-29.5%, obesity-23.6%, hypercholesterolemia-23.0%, smoking-16.5%, hypertriglyceridemia-9.5%.
Thus, during 25 years in Ukraine unfavourable level of epidemiological conditions for creating and progressing of coronary heart disease among urban population has been remaining.
600: G Allele of MCP1 promoter polymorphism increases the cardiovascular risk in patients with ischemic heart disease
A Teren, J Lietava, M Bucova, P Blazicek, M Takac, A Dukat; Homocystein Slovakia Study
2nd Dep Int. Med., Teaching hospital, Commenius University, Bratislava, Slovakia
Background Smoking is an unequivocal risk factor for ischemic heart disease (IHD), i.e. affecting arterial wall via increased inflammatory reaction, however, its relationship to gene polymorphisms regulating the inflamation is unclear. We analysed the influence of −2518 A/G promoter polymorphism in gene for monocyte chemoatractant protein 1 (MCP1), important regulator of inflammatory reaction, on clinical penetrance of IHD in association with nicotinism and metabolic syndrom.
Methods We have genotyped 303 subjects (mean age 57.7 ± 12.65 yrs), 157 men (57.8 ± 12.37 yrs), and 146 women (57.59 ± 12.99 yrs), 223 (73.6%) patients with proven IHD (62.5 ± 9.05 yrs) and 80 controls (44.3 ± 11.66 yrs). 140 probands had smoking history.
Results The frequency of G allele was 44.6%, 33.7% for AG, and 10.9% for GG genotype. Allele A had frequency of 89.1%, 55.4% with AA genotype. We found no difference in distribution of alleles according to presence of IHD and/or IM, res. the age of their onset. G allele in smokers, but not in non-smokers, was associated with preliminary increase of risk for both IHD, and IM as well as for levels of C-reactive protein (CRP) ≥ 1 mg/l. Cox regression model shown premature increase of the risk for IM with years of smoking in presence of allele G. This relatioship was not observed in ex-smokers with increasing years of non-smoking. Allele G in females was furthermore associated with levels of both glucose > 6.1 mmol/l res. > 5.6 mmol/l (P = 0.03; res. P = 0.04), and with MS criterion for blood pressure (P = 0.008). Generally, the frequency of G allele was found to be higher in females with MS (P = 0.02) but not in males with MS.
Conclusion G allele for MCP1 promoter polymorphism is associated with premature onset of ischemic heart disease in smokers. Hypothetically, G allele have more pronounced impact in female patients with metabolic syndrome via increased blood pressure, glycemia and C-reactive protein.