
Abstract

039: The value of brain natriuretic peptide and tissue doppler echocardiography for the diagnosis of myocardial dysfunction in top level athletes
E Oepangat, T Butz, KP Mellwig, L Faber, J Diekmann, F van Buuren, D Horstkotte
Cardiology Department, Heart center North Rhein-Westphalia, Germany
Background Brain natriuretic peptide (BNP) is a cardiac neurohormone that is secreted in response to ventricular volume expansion and pressure overload. Its measurement is used as a standard parameter for evaluation of cardiac dysfunction. The aim of this study is to see whether BNP can be used for the detection of diastolic abnormalities among top athletes.
Methods We investigated 36 male professional Handball athletes (Ath.; 27.1 ± 5.3 years). BNP at rest and after Treadmill exercise (starting at 10 km/h with increasing speed of 2 km/h every 3 minutes) were measured. Ath. were divided into 2 groups according to a normal (group A: BNP < 18 pg/ml) or an elevated BNP level (group B). Both groups were then examined by Tissue Doppler Imaging (TDI) for the analysis of systolic and diastolic velocities of the mitral annulus (MA).
Results 18 Ath.in group A had a mean BNP of 6.7 ± 0.9 pg/ml, whereas the other 18 in group B had significantly higher BNP levels (mean BNP:23.7 ± 3.6 pg/ml; P < 0.001. Peak oxygen consumption (54 ± 5 ml/min kg) was similar in both groups. Standard echocardiographic examination revealed a normal systolic function without structural abnormalities in all cases. TDI analysis all demonstrated normal findings with no significant difference of peak systolic velocities (Śseptal MA:in A: 10 ± 1 cm/s vs. B: 9.4 ± 1.5 cm/s), as well as peak early diastolic velocity (E') on lateral MA 16.8 ± 3.6 cm/s(A) vs. 16 ± 4.8(B) and 13.4 ± 3.1 cm/s (A) vs. 12.6 ± 2.5 cm/s(B) on the septal MA. The calculated EE-ratio were 5.4 ± 1.5 cm/s(A) vs. 5.1 ± 1(B;lateral MA) and 6.7 ± 1.5 cm/s (A) vs. 6.5 ± 1.8 cm/(B;septal MA) respectively.
Conclusions Elevated BNP levels in group B suggested myocardial dysfunction, but TDI showed normal systolic and diastolic velocities of the mitral annulus in both groups and does not reflect any pathologic findings. To determine a cutoff point of BNP level as a screening tool for diastolic dysfunction in athletes, a further investigation is needed.
073: Negative influence of permanent right ventricular pacing on exercise parameters in patients with reduced but not with preserved systolic function
M Wonisch, P Lercher, W Kraxner, R Maier, FM Fruhwald, B Rotman, N Watzinger, D Pätzold, P Hofmann, R Pokan
Medical University Graz, Dept. Internal Med., Div. of Cardiology, Austria
Background Patients with chronic heart failure (CHF) and implanted cardioverter- defibrillators (ICD) may have a higher incidence of new onset or worsening heart failure requiring hospitalization. The purpose of this study was to show the impact of permanent right ventricular pacing on exercise capacity and related cardiorespiratory parameters in ICD-patients with and without CHF.
Methods Seventeen patients with CHF (LVEF: 28 ± 7%) and 11 patients with preserved left ventricular systolic function (LVEF: 55 ± 9%) were prospectively studied. All patients had a dual-chamber ICD with an intrinsic atrioventricular conduction delay between 150 and 250 msec, and they performed cardiopulmonary exercise testing (CPX) on three different days. After CPX 1, patients were randomized either to back-up pacing (NONPACE) or permanent right ventricular pacing (PERMPACE). After 3 months, CPX 2 was performed and patients changed groups (crossover design); CPX 3 was performed after 3 further months.
Results Patients with CHF showed a significant reduction of maximal values for workload (117 ± 48W vs 108 ± 46W P <0.01), oxygen consumption (22.5 ± 6.4 ml.min.kg−1 vs. 21.0 ± 5.3 ml.min.kg−1, P < 0.05), and oxygen pulse (14 ± 4.0 ml vs. 13 ± 3.7 ml, P < 0.05) with PERMPACE compared to NONPACE. The ventilatory efficiency was significantly lower with PERMPACE compared to NONPACE. Patients with preserved LEVF showed no significant differences in these measured parameters. No differences were found for maximal heart rate, minute ventilation, carbon dioxide production, and the respiratory exchange ratio in both groups.
Conclusions Within 3 months permanent right ventricular pacing significantly reduced several cardio-respiratory parameters of exercise in patients with CHF but not in patients with preserved left ventricular systolic function. For patients with CHF and sufficient atrioventricular conduction, every effort should be made to minimize permanent right ventricular pacing.
255: Tissue doppler analysis of the peak systolic velocity of the mitral annulus in top level athletes
F van Buuren, T Butz, KP Mellwig, Y Kim, A Fründ, E Oepangat, O Oldenburg, C Langer, D Horstkotte, L Faber
Dept Cardiology, Heart Center NRW, Ruhr University Bochum, Bad Oeynhausen, Germany
Background In order to prevent athletes from sudden cardiac death (SCD) new methods are needed for the identification of athletes with pathologic left ventricular hypertrophy or hypertrophic cardiomyopathy (HCM). In literature, the best differentiation of pathologic hypertrophy from physiologic hypertrophy was provided by a systolic mitral annular velocity < 9 cm/s assessed by Tissue Doppler Imaging (TDI). The aim of our study was the analysis of the peak systolic velocity of the mitral annulus (MA) in top level handball players of the german first national league.
Methods We examined 93 consecutive athletes by conventional echocardiography according to the ASE guidelines. Systolic and diastolic function was assessed by Doppler analysis of the left ventricular filling and by pulsed Doppler tissue imaging (TDI) of the MA.
Results The mean left ventricular enddiastolic index was 26 ± 3 mm/m2 (> 30 cm/m2 in 14 athletes (15%)). Enddiastolic thickness of the septum was 10 ± 2 mm (> 12 mm in 16 athletes (17%)), of the posterior wall 9 ± 2 mm. No structural heart disease was found and global and regional systolic function was normal in all athletes. Peak oxygen consumption was 55 ± 7 ml/min/kg.
Mean systolic velocity S' was 10.2 ± 2.2 cm/s at the lateral and 9.3 ± 1.5 cm/s at the septal MA. S' was less than 9 cm/s in 18 (19%) individuals at the lateral and in 33 individuals (35%) at the septal MA. 11 athletes showed a S' of less than 9 cm/s at both sides of the MA without having any clinical or echocardiographic abnormalities, familiar history of HCM and especially no hint for phenotypic HCM.
Conclusion TDI analysis of peak systolic annular velocities may provide helpful additional information for the discrimination between physiologic and pathologic left ventricular hypertrophy, but the suggested cutoff value has to be evaluated in further trials.
262: Electrocardiographic patterns in 455 elite athletes from Serbia
Nenad Dikic, S Mazic, S Ostojic, J Suzic, M Dabetic, A Djordjevic Dikic, D Radovanovic, S Zivanic
Sport Medicine Association of Serbia, Serbia and Montenegro
Background Regular intensive exercise training is associated with structural and functional changes of the myocardium which are reflected on the 12 lead electrocardiogram (ECG) as different abnormalities.
Objective The objective of this study was to analyze the ECG patterns in elite athletes from Serbia. We have used the method used by Pellicia et al.
Methods and results We analyzed ECG patterns in 455 athletes (aged 20.45 ± 4; 79% male) who were participating in 6 sporting disciplines (basketball, football, swimming, rowing, cycling and judo). ECG patterns were distinctly abnormal in 37 athletes (8.31%), mildly abnormal in 90 (19.61%), and normal or with minor alterations in 328 (72.08%), shown on table with all the details.
Results Echocardiographic examination is done in small group of athletes with ECG abnormalities but without significant cardiac changes.
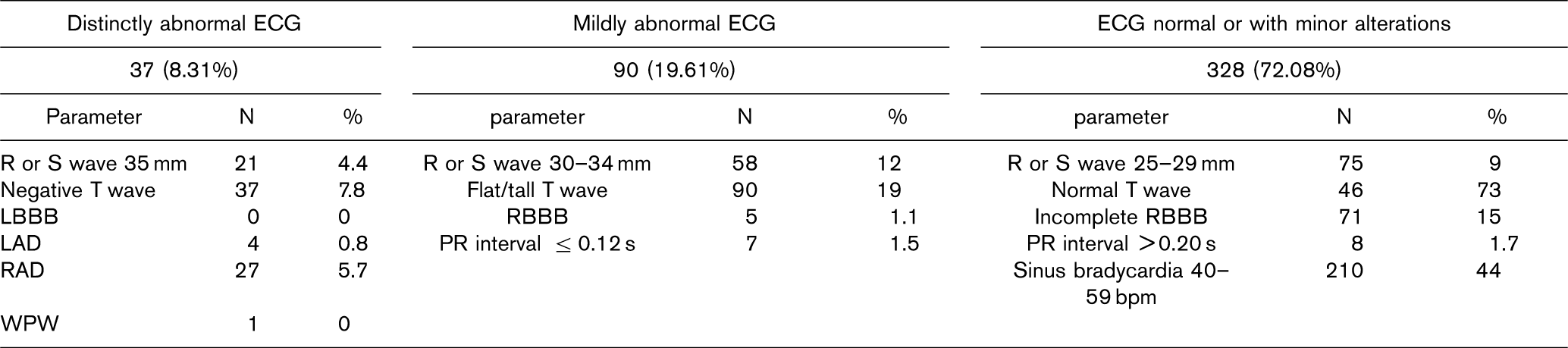
Conclusions Significant numbers of athletes (28%) in this large cohort had ECGs that were distinctly or mild abnormal, which could be explained as consequence of long-term, intense athletic training and it is usually indicative for athlete heart syndrome. We consider this method of analyzing ECG pattern as a very important one, as a triage for further echocardiographic examination, especially in low income countries where cost/benefit ration is important factor in prescreening examination of the athletes.
351: The value of transtelephonic electrocardiographic transmission in the preparticipation screening of athletes
S Karavasiliadou, E Kouidi, Th Samaras, S Chatzimihailidou, M Petraki, J Sahalos, A Deligiannis
Sports Medicine Laboratory, Aristotle University, Thessaloniki, Greece
The electrocardiograms (ECG) is recognized as a necessary examination in the preparticipation screening of athletes but its diagnosis demands the presence of cardiologist, which increases the difficulties as elevates the cost of the examination. The purpose of the study was to evaluate the feasibility and effectiveness of transtelephonic ECG transmission (TET)in athletes, during their medical screening directly from the playfield from General Practitioner (GP). Data was obtained from 506 amateur soccer players of the prefecture of Thessaloniki, aged 20.5 ± 6.2 years. In case of “abnormal” findings from the medical history, physical examination and/or ECG, the last was transmitted from the field to the medical base for further evaluation by a cardiologist, which was direct and explicit. According to the diagnosis, the athletes were submitted to further examinations as echo study, stress test and 24-hour Holter monitoring of ECG or blood pressure. Totally, 142 ECGs were transmitted either by plain old (76%) or mobile telephony (24%). Successful ECG transmissions were achieved by 93% and 91%, respectively. The mean time of ECG receiving and storage was 180 ± 46 sec and transmission 60 ± 23 sec using digital electrocardiograph. In total, 102 of the transmitted ECGs were found to be “abnormal” from the GP. However, only in the 74 the cardiologist agreed with the first diagnosis. Negative T waves were observed in 28, incomplete RBBB in 27 and arrhythmias in 6 of the submitted ECGs. The 28.3% of the athletes had a positive family history. The 8.1% reported symptoms, such as chest pain during exercise. Mild systolic murmur had the 15.2% and hypertension the 0.4% of the athletes. Finally, 49 athletes were submitted to echo study, 7 to stress test and 2 to Holter monitoring. All of them were permitted to participate in physical activities. Our results demonstrate that TET in sports medicine is a workable facility, providing the application of medical screening in a great number of athletes.

356: Are the exercise-induced cardiac adaptations associated with the aerobic capacity in professional soccer players?
N Koutlianos, G Hatzopoulou, K Tsorbatzoglou, E Kouidi, A Deligiannis
Sports Medicine Laboratory, Aristotle University, Thessaloniki, Greece
Aerobic capacity contributes substantially in soccer performance and maximal oxygen uptake (VO2max) is traditionally considered as the major index of aerobic fitness. However, it is not yet documented in this popular sport discipline whether the extent of central adaptations significantly affects VO2max modulation. Thus, the purpose of the study was to investigate the potential interaction between anatomical and functional cardiac indices and VO2max in professional soccer players. Eighty-four professional soccer players, competing in 3 clubs of the premier Greek division, participated in the study. The mean age of the sample was 26.0 ± 3.9yrs old (range 17-34 yrs) with 11.7 ± 4.5 mean years of training (range 8-25 yrs). All subjects underwent physical examination, electrocardiogram, echo study for left ventricular mass (LVM), end-diastolic volume (EDV) and ejection fraction (EF) assessment and treadmill spiroergometric test for VO2max measurement. The results are presented in the following table:
In conclusion, cardiovascular efficacy was not found to affect remarkably the aerobic capacity in top-level soccer players. The cardiac adaptations in these athletes seems to be the outcome of both long-term aerobic and anaerobic exercise training; moreover, the peripheral adaptations such as muscle capillary density and enzyme activity may have an impact on aerobic performance modulation.
409: Importance of rhabdomyolysis in military training -methods for controlling its effects
AF Gomes, R Pombo, V Brás, A Remédios, M Pragosa
Hospital Militar de Belém - Lisbon, Portugal
Background Medical support to military activity acts upon 3 fundamental areas: selection/classification, training and operations. The need to face episodic outbreaks of rhabdomyolysis during physical training for officer course of infantry cadets and of candidates to special forces led us to try to identify causes and propose corrective measures.
Objectives 1. To identify biochemical patterns of response to physical exercise during military training in portuguese population; 2. To produce recommendations for the effectiveness of training and control of inherent risk.
Population Young men, running physical programs of officer's promotion course (Group A) and of special forces'course (Group B).
Methods Blood and urine specimen were analyzed before, during and after critical tasks. Critical tasks were “continuous 24 hour instruction” (Group A) and “forced march” (25 km for about 2H40M - Group B).
Results Plasma values of muscle enzymes were consistently superior to reference values from international experience in both groups, although Group A values doubled Group B's. Groups were also compared as to methods of training, cycles of work-rest, rhythm of hydration, load carried and nutrition. Although special forces training is traditionnaly considered more demanding than any other, their metabolic effects were better controlled, fact that derives from a better methodology and monitoring.
Conclusions 1. Military training, according to its purposes, must respect physiological limits; 2. Monitoring must allow for parameters that can predict risk; 3. Military training support must rely on prompt diagnostic methods, adequate human and material resources in maximal readiness.
504: Systematic assessment of those engaged in sports and exercise: report of the task force on sudden cardiac death in Ireland
EB Shelley, W Keena, J Galvin, C O'Brien, B Maurer; Task Force on Sudden Cardiac Death
Department of Health and Children, Hawkins House, Dublin 2, Ireland
The Task Force (TF) on Sudden Cardiac Death (SCD) examined the evidence on screening for risk of SCD. Most SCDs are attributable to CHD and occur in older adults. In the general population, first degree relatives of SCD cases < 40 years are the priority group for assessment for conditions such as cardiomyopathy and channelopathy.
In relation to sports and exercise, current tests are not sufficiently sensitive and specific to recommend medical testing of all athletes for risk of SCD. Risks of obesity and physical inactivity must also be considered. Pre-participation assessment should be tailored to the intensity of the activity and the level of competition.
Those aged 14 years who are active informally, e.g. walking or cycling, should be encouraged to self-administer a questionnaire re family history and personal history and symptoms. Where positive, medical advice should be sought.
A questionnaire should be offered to those 14 who join a sports club or gym but are not involved in very competitive sports. A national protocol should be agreed to include a model questionnaire, procedures for obtaining informed consent, questionnaire administration and referral for medical assessment.
For moderate or vigorous intensity sports at national, provincial or county level, the national protocol should include guidelines on medical assessment of all athletes at these levels, and on indications for referral to cardiology and specialist centres. After a sudden cardiac event, medical assessment should be offered to all team members.
Education programmes for athletes should emphasise the dangers of performance enhancing, recreational and other drugs. Pre-participation assessment should explore the use of such drugs.
The TF recommended training for sports and medical personnel on the implementation of risk assessment protocols and the establishment of a register to support the programme.
The TF would welcome further discussion of these issues in a European context.
536: Tissue doppler analysis of diastolic heart function in top level athletes
T Butz, F van Buuren, L Faber, Y Kim, C Langer, O Oldenburg, E Oepangat, N Bogunovic, D Horstkotte, KP Mellwig
Dept Cardiology, Heart Center NRW, Ruhr University Bochum, Bad Oeynhausen, Germany
Background The distinction between pathological left ventricular hypertrophy (pLVH; e.g. in hypertrophic cardiomyopathy), and physiological LVH in athletes (athletes heart) is sometimes difficult. Impaired diastolic left ventricular function (dLVF) has been shown to be an early hallmark of pLVH, whereas athletes are reported to have a normal or even supernormal dLVF. Therefore, the analysis of dLVF by Doppler tissue imaging (DTI) might be very useful in the differential diagnosis.
Methods 83 consecutive athletes (national handball league) were studied by echocardiography according to ASE guidelines, including an analysis of dLVF by flow Doppler of left ventricular filling, and by pulsed DTI of mitral annulus (MA) motion.
Results In all athletes systolic function was normal, and no structural heart disease was found. Mean enddiastolic thickness of septum (10 ± 2 mm) and posterior wall (9 ± 2 mm) were normal. The mean enddiastolic LV index was 2.9 ± 0.3 cm/m2. Exercise testing showed a peak oxygen consumption of 54 ± 7 ml/min/kg. Mean early diastolic velocity (E') was 16.4 ± 3.6cm/s at the lateral and 13 ± 2.9 cm/s at the septal MA. Mean E'/A'-ratio was 2.4 ± 0.8 at the lateral MA, and 1.8 ± 0.6 at the septal MA. The ratio of early LV filling velocity (E) over E' (E/E') was 5.2 ± 1.2 (lateral MA) and 6.6 ± 1.7 (septal MA). Characteristics of a restrictive filling pattern (E/A-ratio > 2.0, deceleration time of E < 150 ms) were found by flow Doppler in 10 of these 83 athletes (12%). However, by a (super-) normal E' and an E'/A'-ratio of > 1.0, dLVF was judged as normal in all cases.
Conclusion DTI is very helpful in the assessment of diastolic left ventricular function in athletes, and should be used for differentiation between physiologic and pathologic LVH.
575: Cycling and the heart, short term follow-up of 17-year-old cyclists
Jan Hoogsteen, Johan van Lierde, Jan-Paul van Mantgem, Jan Outhof, Luc Janssens, Norbert van Hemel, Ernst van der Wall
Department of Cardiology Maxima Medical Centre Veldhoven, Netherlands
Aim Cycling is the only sport where both aerobic and anaerobic power are trained and pushed to maximal levels over long periods. It is unclear how young elite athletes respond to this heavy isotonic and isometric loading of the cardiac system over several years.
Method and results 46 young cyclists of 17 years of age underwent annually cardiac investigation over a 5 year period. Anthropometrical variables, ECG, echo-Doppler cardiographic examination and exercise were carried out yearly. The minimal heart rate and PR interval changed clearly (65.2 ± 12.6 versus 57.4 ± 10.0 beats/min (P < 0.005) and 149.8 ± 21.5 versus 160.6 ± 18.7 ms (P < 0.05). At baseline electrocardiographic left ventricular hypertrophy related positively to echocardiographic left ventricular mass index. Over the 5 year period left ventricular mass increased significantly from 252.8 ± 60.9 to 280.1 ± 61.4 gram (p < 0.05) and relative wall thickness showed a clear remodeling of the ventricles. At baseline and after 5 year following eccentric and concentric remodeling was apparent in a minority of the cyclists, whereas the intermediate type remodeling was apparent in 31(67%) and 36(78%) cyclists respectively. Functional cardiac changes of the cyclists including stroke volume at rest significantly declined over the years (105.4 ± 29.2 versus 94.7 ± 20.1 ml, P < 0.05) whereas aerobic power, maximal oxygen-uptake and oxygen pulse significantly increased (350.4 ± 42.2 versus 381.9 ± 55.8 watt, P < 0.005, 60.8 ± 7.4 versus 64.9 ± 8.0 ml/kg/min, P < 0.05 and 20.8 ± 3.6 versus 24.5 ± 3.4 ml/heartbeat, P < 0.005 respectively). The increase in stroke volume during exercise was more outspoken in older cyclists than in younger cyclists.
Conclusion Training and competition in cycling initiate various cardiac adaptations ranging from rate, AV conduction and left ventricular morphology and functioning. Heavy training schedules and competition in cycling at young ages do not induce short-term pathological cardiac changes.
584: How to promote physical activity in europe? a call from central and eastern region (CEE)
Radu M Negoescu, Wojciech Drygas; for CINDI-ROMANIA 2000 and CINDI-POLAND groups
Institute of Public Health in Bucharest, Romania
The last meeting of the EuroPRevent's ancestors in Leuven has remarked huge unexploited health resources laying in community physical activity (PA) and pointed to innovative initiatives taken in CEE countries.
Data from Pucioasa - Romania show% of men featuring medium & high levels of total PA is close to those with “PA of every kind” in Moscow (68% vs. 74%), and higher than% of people with regular PA in Canada (36%. Spare time PA (57% Males, 33.2% Females) compares favorably with Moscow residents (22% M, 17% F), even if much of declared leisure PA is actually work-at-home related to family survival in difficult times. However, with some 300 minutes of mild effort per week, those Romanians ideally fulfill ESC recommendations of 30 minutes mean PA in the most day of the week.
The stake in both West and East is to promote health-intentional regular exercise. Giving people the PA taste may rely on community events, lesser on commercial runs and more on health-related actions like Heart Runs at the national Days of the Heart or the World Heart Day in September or still at May 10th - the prospective WHO's World PA Day. Anglo-Saxon Terry Fox Runs for Cancer Research spread Eastward combining charities with PA. Much more challenging induction of sustained PA may use the Polish model “Put your heart on its feet” (2001) that award people collecting at least 80 “moderate move points” along 30 consecutive days of the 3 summer (Poland) or autumn (Romania) months. Thus Poland and on its track Romania, Czech Republic, Slovenia and Russia have already accumulated experience in cultural models that a priori are not particularly prone to PA for health.
Sharing Central-Eastern European experience with other experts across Europe, recognizing diversity of social-economical milieus but also detecting communalities in shaking inertia that separates sedentary individuals and communities from a healthy, active and productive life may clearly lead to healthier Euro-hearts.