
Abstract
Background
Few studies exist on the effects, in terms of work capacity and safety, of exposure to moderately high altitudes in patients with stable ischemic left ventricular dysfunction. Moreover no data are currently available on the cardiorespiratory response to walks in the mountains.
Aim
The objective of this study is to evaluate the effects of altitude on effort tolerance during walks in the mountains and to determine whether exposure to altitude may be harmful to patients with ischemic left ventricular dysfunction.
Methods
Forty-five patients with stable chronic ischemic left ventricular dysfunction (ejection fraction = 35 ± 4%, and peak VO2 ≤ 18/ml/kg per min in a preliminary effort test) were compared to 24 normal subjects. All subjects underwent a series of 6-min walking tests at three different altitudes: 500, 2000 and 2970 m above sea level. Cardiorespiratory response was assessed by a validated portable instrument. The resting arterial PO2 was measured at the three altitudes.
Results
No complications were observed during any tests in either the patients or the healthy controls. Overall, healthy subjects had higher values of 6-min walking test VO2 and walked longer distances in the test than did the patients with left ventricular dysfunction. The mean distances walked in the 6-min walking test were similar at 500 and at 2000 m in both the healthy controls and the patients; at 2970 m, however, the distances decreased in both groups, and more so in the patients (−11 ± 3%) than in the controls (−5 ± 2%) (P<0.01). VO2 during the 6-min walking test remained stable when the test was carried out at 500 and 2000 m (20.4 ± 3.6 versus 19.9 ± 4.1 ml/kg per min in patients, and 30.2 ± 3.4 versus 29.8 ± 4.2 ml/kg per min in the controls; P, NS), but decreased at 2970 m by 13.9 ± 3% in patients (P<0.01) and by 6.6 ± 2.1% in controls (P<0.01) (patients versus controls, P<0.01). Finally, a similar, significant decrease in arterial PO2 was observed in both groups only at 2970 m (−29%, P<0.01).
Conclusion
Patients with stable ischemic left ventricular dysfunction had good tolerance while walking at high altitudes, but showed a moderate decrease in work capacity at 2970 m, which was greater than in normal subjects.
Introduction
The effects of high altitude and hypoxia on cardiorespiratory function have been extensively studied in normal subjects [1]. Less information is available about patients with coronary artery disease (CAD) and left ventricular dysfunction (LVD) exposed to moderately high altitudes. Given the considerable improvements in medical and revascularization treatments in recent years, there have been corresponding improvements in survival and quality of life of these patients, especially those with good effort tolerance [2], and this class of patients is becoming increasing numerous. Cardiac patients now frequently ask whether, in their condition, physical activity in the mountains is dangerous, and if so, what intensity of activity: it seems unwise to expose high-risk subjects (with LVD and poor effort capacity) to high altitudes, and contrariwise, there appear to be no contraindications for low-risk patients (without LVD and good effort capacity) [3]. There is great uncertainty [4], however, given the very few data available on the effects of exposure [5, 6] to even moderately high altitudes (2000–3000 m), about how to advise LVD patients with good effort tolerance. The limited data available are on exercise tolerance of LVD patients evaluated at 2500 m above sea level (ASL) [5] or during simulated altitude-induced hypoxia [6], but there are currently no data regarding direct measurements in the mountains, in the real conditions of exercise and environment, of cardiorespiratory response while walking, the physical activity most commonly performed at high altitude [7]. Given this lack of precise information, doctors often advise patients to avoid exposure to altitude because the reduction of oxygen pressure is regarded as potentially dangerous [8, 9] especially in patients with ischemic LVD. We therefore designed the present study to determine acute tolerance whilst walking to moderate altitudes in a group of 45 patients with CAD and LVD and good effort tolerance and in a control group of 24 healthy individuals. Hemodynamic parameters and V O2 were measured at rest and during a series of 6-min walking tests (6MWTs) performed at 500, 2000 and at 2970 m ASL. The purpose of these evaluations was to determine whether patients with ischemic LVD need to be advised against gentle exercise in the mountains.
Methods
Study population
Patients
The study group comprised 45 non-acclimatized patients with compensated ischemic LVD (mean age 58 ± 10 years) caused by coronary artery disease. Inclusion criteria for enrollment were angiographically documented coronary artery disease (luminal area stenosis > 50% in one or more coronary vessel); echocardiographic ejection fraction ≤ 40%; clinical stability for at least 3 months under optimized therapy; New York Heart Association functional class I–II; peak oxygen uptake (V O2 ) ≤ 18 ml/kg per min during a cardiopulmonary exercise test (CPET); absence of significant ischemia or angina during the CPET; absence of significant reversible ischemia, as determined by exercise symptom-limited myocardial perfusion scintigraphy; strong motivation to be in the mountains. The CPET and scintigraphy were performed whilst patients were receiving optimized medical treatment.
Exclusion criteria were severe valvular heart disease, pericardial effusion, pacemaker, effort-induced or spontaneous angina, severe cardiac arrhythmias, peripheral vascular disease, chronic lung disease, systemic or hematological illnesses (e.g. anemia or polycythemia), hepatic or renal failure (creatinine > 2.5 mg/dl), uncontrolled systemic arterial hypertension at rest (systolic pressure ≤ 140 mmHg or diastolic pressure ≤ 85 mmHg); pulmonary hypertension (echocardiographic arterial systolic pressure > 30 mmHg).
The baseline evaluation included clinical history and examination, a resting electrocardiogram, chest radiographs, blood chemistry (complete blood count, tests of hepatic and renal function, levels of electrolytes), and a trans-thoracic color Doppler echocardiogram.
All patients performed a baseline maximal CPET, reaching a respiratory exchange ratio (RER) above 1.10; V O2 and V CO2 were monitored by a portable instrument (VMax ST; SensorMedics Co., Yorba Linda, California, USA), which was later used to evaluate respiratory parameters during the 6MWT (see below). The patients exercised on a computer-driven cycle ergometer (X-Scribe II; Mortara Instrument Inc., Milwaukee, Wisconsin, USA) following a ramp protocol, starting at 0W with incremental steps of 10W every minute. The peak V O2 was taken to be the highest V O2 measured during the final 30 s of exercise.
Controls
The control group consisted of 24 non-acclimatized voluntary healthy subjects (57 ± 11 years) with no history of cardiovascular disease. These participants were non-smokers. Inclusion criteria were a normal heart rate, arterial blood pressure (without any drugs) and electrocardiogram, as well as a low probability of coronary heart disease, as assessed by the Framingham algorithm [10]. Professional athletes and expert mountaineers were excluded.
Study design
The healthy controls and the patients performed nine 6MWTs with oxygen uptake measurements, using a portable instrument, according to the following protocol: day 1, series of three 6MWTs at 500 m ASL at our hospital; day 3, series of three 6MWTs at 2000 m ASL (Pila, Aosta Valley); day 5, series of three 6MWTs at 2970 m ASL (Cime Bianche, Matterhorn) (Fig. 1).
All subjects were transported to 2000 m ASL by car; the altitude of 2970 m ASL was reached by cable car in 20 min. All the tests were performed in August in order to avoid excessive climatic stress for patients.
All 6MWTs were repeated after a 30-min period of rest. The tests were administered by physiotherapists and performed in the hospital garden (day 1), on a previously measured 40 m-long, flat surface free of obstacles; in the mountains (days 3 and 5), on previously measured 40 m-long flat clearings (Fig. 1). Participants were asked to remain still for at least 3 min before commencing exercise, in order to stabilize gas measurements and were instructed to walk as far they could in 6 min; they were encouraged every 30 s in a standardized fashion and time was called every 2 mins. The first test was used as a familiarization trial and not considered for further analysis. The average of the second and third tests were taken as an estimate of the walking and cardiorespiratory performance of each participant.
Patient during a walking test at 2970 m above sea level.
During each 6-min period the following parameters were considered: mean distance walked (measured in metres), heart rate, blood pressure, maximal V O2 , V CO2 , minute ventilation, and respiratory rate. We also measured, at the three different altitudes, oxygen saturation with a percutaneous pulse oximeter (OTIS 500; Spencer-Italia, Parma, Italy) and resting arterial P O2 and P CO2 in blood samples obtained from the radial artery: these analyses were performed immediately with a portable blood-gas analyzer (I-Stat-1; Abbott Diagnostics, Abbott Park, Illinois, USA) which was appropriately calibrated for temperature and barometric pressure.
Blood pressure was measured at rest and immediately after stopping the 6MWT with a manual sphygmomanometer (the same at each altitude). The tests were continued until the end of the sixth minute or the onset of significant symptoms or side effects, such as chest pain or dizziness, potentially excessive dyspnea or dangerous arrhythmias, as assessed by the telemetric control. At the end of the 6 min, the distance walked was measured and the patients were asked to express a judgment on their perceived fatigue using the Borg scale, a visual analog scale from 0 to 20, with 20 signifying maximum fatigue [11].
During the 6MWT participants carried a VMax ST (SensorMedics Co.), a small portable system that can be used anywhere to test any individual. The unit (650 g, battery included) is attached to the upper part of the chest, thereby assuring its stability during exercise without hindering limb movements. The system measures oxygen uptake (V O2 ), carbon dioxide output (V CO2 ), minute ventilation (V E) and respiratory rate (RR) in a breath-by-breath mode.
The Triple V transducer from Jaeger (Hoechberg, Germany) accurately measures a wide range of flow rates (tidal breathing to 20 l/s) in varied conditions (−20†C to + 40†C). Accurate and rapid analyzers measure oxygen and carbon dioxide concentrations, adjusted for barometric pressure, air temperature and humidity, at every breath. The system was calibrated before each test with two gases for two-point calibration and the time delay of sampling was also measured during calibration. The VMax ST was connected to a PC by a bi-directional telemetry system that allows two-way communication for transmission of data from the participant and audio feedback to the participant. The radio transmission range was more than 1000 m. Data on each breath were also saved in an internal flash memory for safety reasons until the data were downloaded to the PC.
Heart rate was simultaneously and continuously recorded by the VMax ST and these data were also transmitted to the PC. The computer screen was observed by a cardiologist throughout the 6MWT; heart rate and any arrhythmias were constantly monitored (all simple and complex arrhythmias were individually counted).
6MWT V O2 (expressed in milliliters per kilogram per minute) and the other respiratory parameters were recorded as the mean values during the last 60 s of the walking test. Data were collected and analyzed using the Vision Software by SensorMedics Co. A 12-lead electrocardiogram was carried out at each altitude, both at rest and immediately after the end of the last 6MWT, and analyzed according to standard criteria.
Reproducibility
In a preliminary study, when a series of three 6MWTs were performed on two different days in 20 healthy volunteers, the variability of the mean of the distance walked was 1.7%, (range 0.4–2.8%). No statistical differences were found in the V O2 between the two repeated series of 6MWT. These findings confirm previous reports on the reproducibility of the 6MWT [12].
Statistical analysis
Statistical analyses were performed using SPSS software (version 12 for Windows; Chicago Illinois, USA). Data are presented as mean ± SD. Intragroup and intergroup comparisons of the effect of altitude on exercise and cardiorespiratory parameters were performed using ANOVA for repeated measures, followed by the Tukey post-hoc test. Relations between demographic, clinical and functional variables (age, body mass index, ejection fraction, previous pulmonary edema, history of smoking, site of previous myocardial infarction, distance walked at baseline 6MWT performed at low altitude) and the percentage decrease in the 6MWT V O2 at 2970 m (with respect to 500 m altitude ASL) were assessed by linear regression analysis. A P value below 0.05 was considered statistically significant.
Ethical approval
The protocol was approved by the local Ethical Committee. Written informed consent was obtained from each participant before entry into the study.
Results
The demographic and clinical data of both groups are listed in Table 1. No significant differences were found in age, sex or anthropometric data between the patients and healthy controls. Forty-two patients had a history of acute myocardial infarction, while 44 patients had undergone revascularization after acute myocardial infarction or because of pulmonary edema (seven patients). All events occurred at least 6 months before entry into the study. The medical treatment is listed in Table 1: drug therapy remained unchanged throughout the study and at the three different altitudes. During the cardiopulmonary cycle ergometer test the peak V O2 was 22.6 ± 3.9 ml/kg per min in patients and 33.2 ± 5.5 ml/kg per min in the healthy controls.
All participants completed the trial; no test was interrupted because of arrhythmias, angina, dyspnea, ischemia or other symptoms or complications.
Hemodynamic parameters
Resting heart rate did not differ at 500, 2000 and 2970 m in patients or healthy controls (Table 2). The resting systolic arterial blood pressure in patients with LVD was 116 ± 10mmHg at 500 m, and increased significantly at both 2000 m (129 ± 14mmHg, P <0.01) and 2970 m (137 ± 16 mmHg, P <0.01). The resting systolic arterial blood pressure of normal subjects did not change from 500 to 2000 m (117 ± 14 to 120 ± 18 mmHg; P, NS) but increased significantly at 2970 m, though to a lesser extent than in the patients with LVD (126 ± 12 mmHg, P = 0.02 versus 500 m) (P <0.01 for the intergroup comparison).
Study population
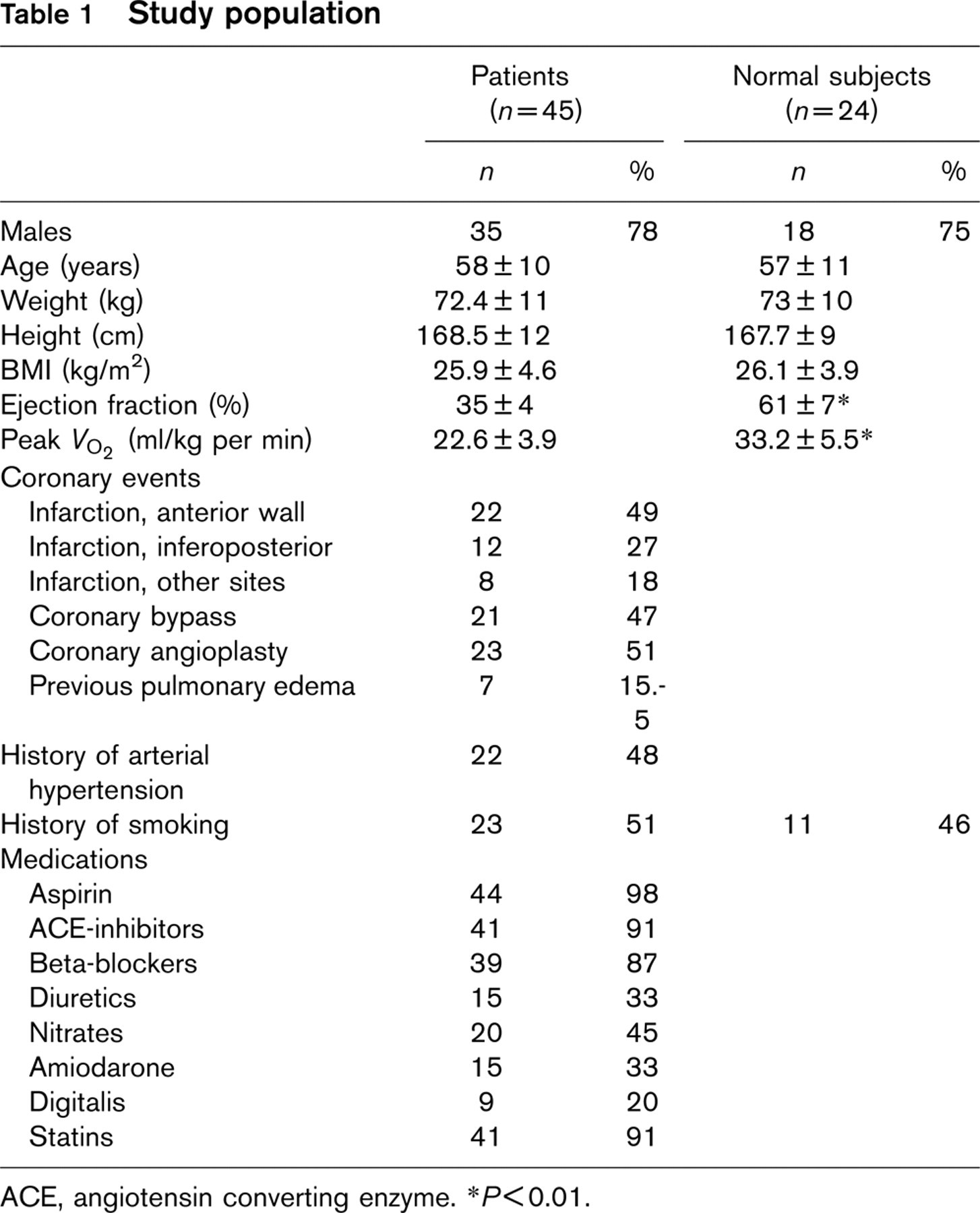
ACE, angiotensin converting enzyme. ∗P<0.01.
Arterial P O2 did not change at 2000 m compared with 500 m in either group, but was significantly lower at 2970 m (−29%, P <0.01) than at 500 m in both groups (from 86 ± 11 to 61 ± 5 mmHg in patients and from 89 ± 9 to 63 ± 7 mmHg in controls, P, NS for the intergroup comparison) (Table 2).
The oxygen saturation at rest was also unchanged in both groups at 2000 m compared with 500 m, but was significantly lower at 2970 m (Table 2) without any significant differences between the two groups.
Effects of altitude on 6-min walking test
Healthy participants had higher values of peak V O2 and walked longer distances in the 6MWT than did patients, as expected. The mean distances walked were similar at 500 and 2000 m in both groups (517 ± 70 m versus 520 ± 90 m in patients, and 652 ± 88 m versus 645 ± 70 m in controls), but decreased at 2970 m in both groups (461 ± 67 m in patients, P <0.01, 619 ± 77 m in controls, P = 0.02). The decrease was greater in patients (−11 ± 3%) than in healthy subjects (−5 ± 2%) (P <0.01).
Resting results
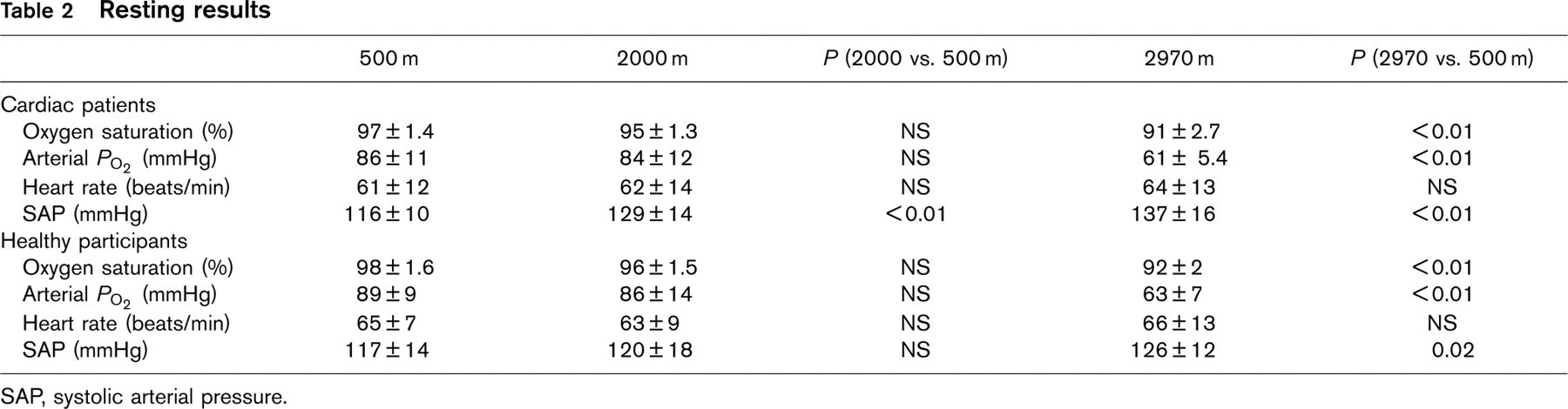
SAP, systolic arterial pressure.
V O2 measured during the 6MWT at 500 m was lower (by approximately 10%) than the peak V O2 at maximal exercise during the CPET, in both groups of subjects.
In both groups, 6MWT V O2 was unchanged from 500 to 2000 m (20.4 ± 3.6 versus 19.9 ± 4.1 ml/kg per min in patients, and 30.2 ± 3.4 versus 29.8 ± 4.2 ml/kg per min in controls; P, NS). At 2970 m the 6MWT V O2 decreased significantly in both groups (17.6 ± 3.9 ml/kg per min in patients, 28.2 ± 3.2 ml/kg per min in controls; P <0.01). Once again the reduction was greater in cardiac patients than in healthy participants: the 2970 m altitude induced an absolute decrease of V O2 of approximately 3 ml/kg per min among patients (−13.9 ± 3%) and of 2 ml/kg per min among healthy subjects (−6.6 ± 2.1 %) (P <0.01 for intergroup comparison).
The perception of fatigue, assessed using the Borg scale, was similar at all three altitudes among the cardiac patients, but in all cases significantly greater than that perceived by the healthy subjects (P <0.05).
The only baseline (at 500 m) demographic, clinical or functional variable that was significantly correlated with the decrease in V O2 at 2970 m was the distance walked at 500 m (P <0.001): the correlation between the above parameters is shown in Fig. 2.
The decrease of oxygen pulse was −15% in cardiac patients and −7.1% in healthy subjects (P <0.01 for intragroup and intergroup comparisons) (Table 3).
The maximal respiratory rate during exercise increased progressively with altitude: this increase was considerably more substantial in patients (+ 54%) than in the healthy controls (+ 36%) (P <0.01 for intragroup and intergroup comparisons). Conversely, maximal minute ventilation during exercise (V E) increased less in patients than in healthy controls (P <0.01 for intragroup and intergroup comparisons) (Table 3).
The maximal heart rate at the end of the 6MWT increased significantly (P <0.01) at 2000 and 2970 m in patients (from 103 ± 17 beats/min at 500 m to 120 ± 16 and 135 ± 17 beats/min, respectively); heart rate also increased in the healthy subjects, but to a lesser extent than in the patients (P = 0.01 for the intergroup comparison) (Table 3).
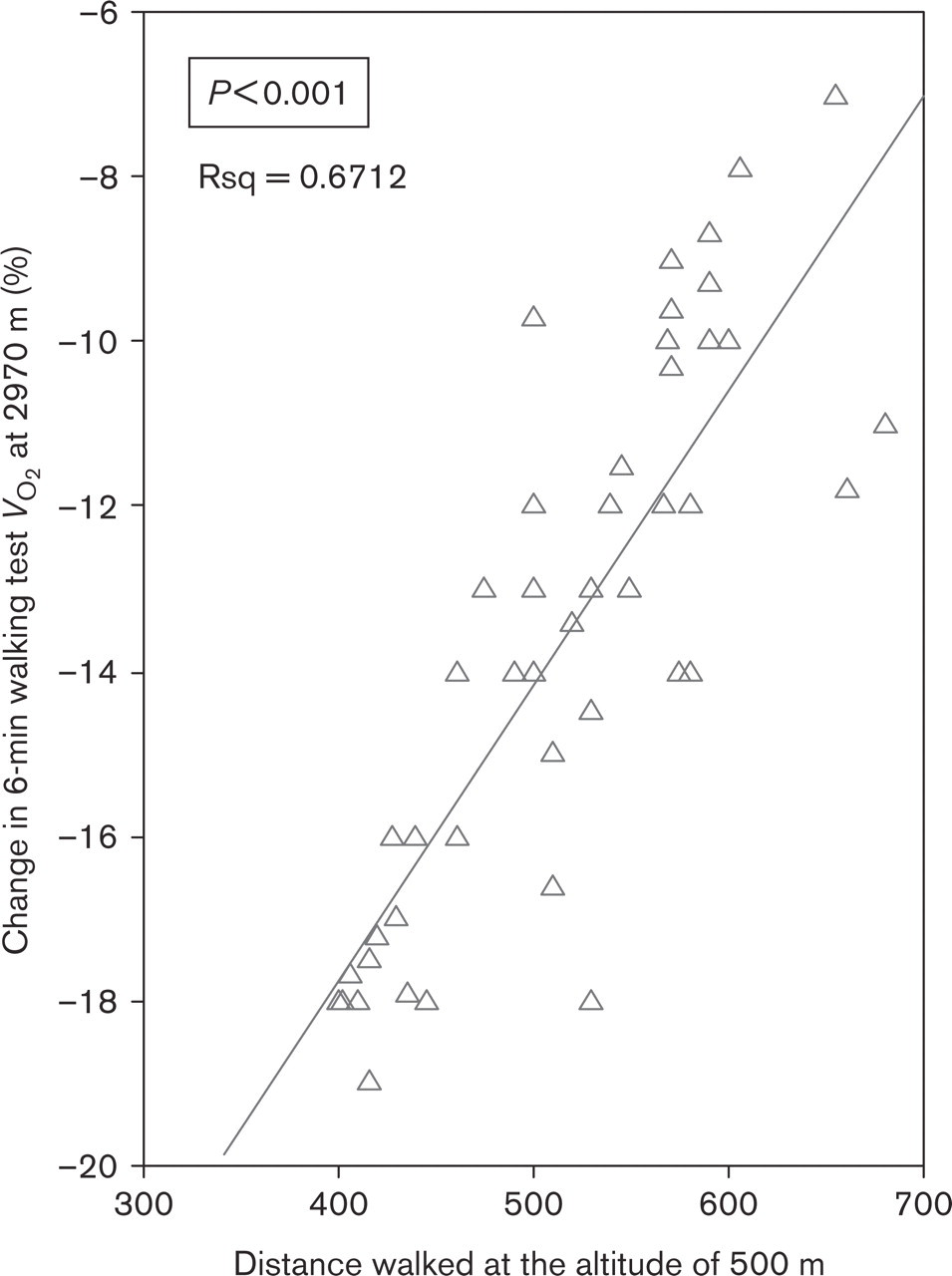
Correlation between distance walked at 500 m and percentage change in 6-min walking test V O2 at 2970 m in patients with ischemic left ventricular dysfunction
The systolic arterial pressure at the end of the 6MWT increased substantially more in patients than in the healthy controls: in fact at 2970 m the maximal value was 198 ± 21 mmHg in the patients with LVD whereas it was 178 ± 25 mmHg in healthy subjects (P <0.01) (Table 3).
Walking test results
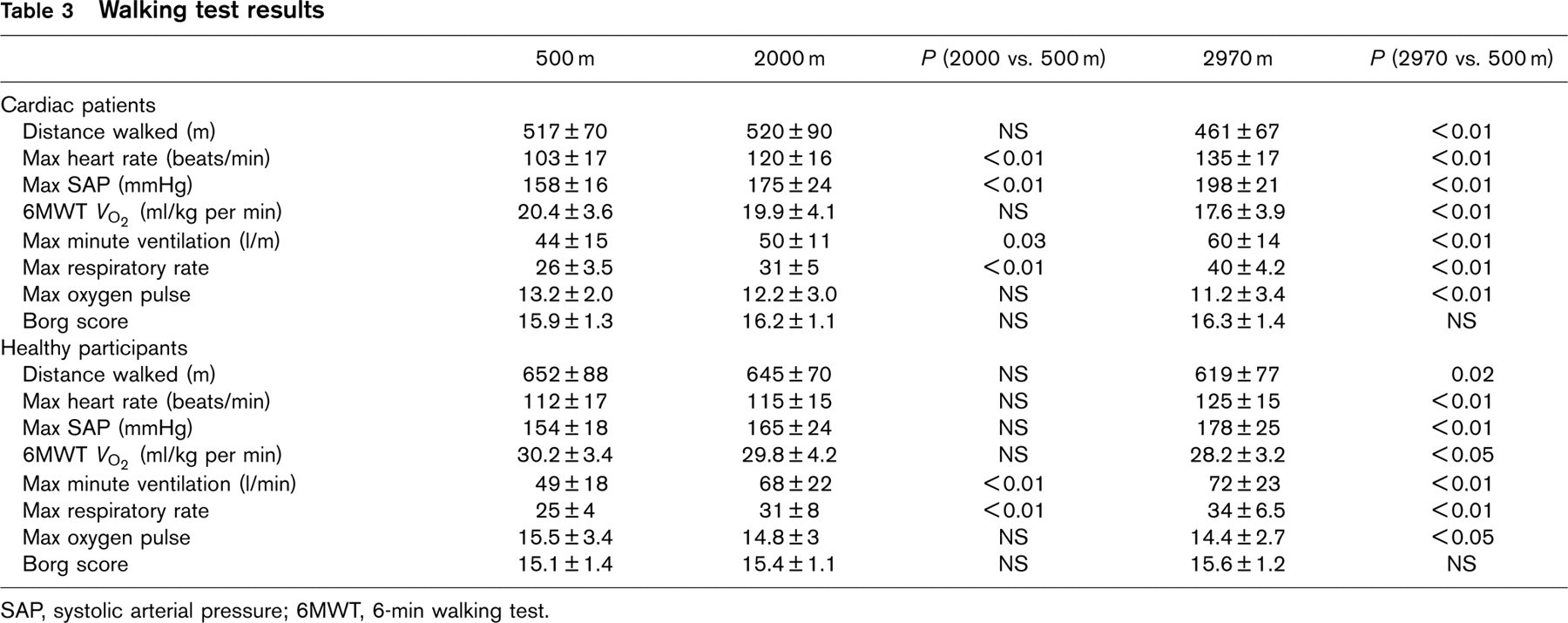
SAP, systolic arterial pressure; 6MWT, 6-min walking test.
Discussion
The aim of this study was to assess whether patients with stable ischemic LVD and good effort tolerance can safely perform mild exercise at moderate to high altitudes (2000 and 2970 m). This information is of relevance to many patients who seek advice on recreational or business activities in the mountains. No studies have been reported on exercise tolerance of patients with LVD while walking in the mountains.
There were three main findings: a moderate decrease in performance at 2970 m (−11% in walked distance, about −14% in maximal V O2 ); the absence of any significant differences in exercise tolerance at 2000 m compared with 500 m; no clinical complications were observed during the tests or throughout the trial.
We designed our study because, in our opinion, there is uncertainty about how to advise patients with ischemic LVD and good effort tolerance wishing to go to moderately high altitudes (2000–3000 m) given that very few such patients have been studied, and those that have been evaluated were assessed with different protocols: without cardiorespiratory function evaluation [5] or in simulated altitude-induced hypoxia [6]. Our sample of 45 patients is not wholly representative of all patients with ischemic LVD, but the advantage was that this was an extremely homogeneous group of patients and constituted the largest series ever studied with the same protocol.
Our study was conducted in a mountain setting, allowing us to evaluate patients’ performance and physiological responses in real conditions of exercise and environment (barometric pressure, temperature, humidity, wind). We chose the 6MWT to evaluate patients and normal subjects, as this test mimics the physical activity generally required by patients in the mountains. This constant workload exercise is being increasingly used to assess daily functional capacity, exercise tolerance and physical training effects in healthy subjects [13–15] as well as in patients with heart failure [16–20], sometimes combined with an analysis of cardiorespiratory function [16–19], and has recently been demonstrated to have a good reproducibility [12, 20]. In order to optimize the reproducibility and minimize the risk of any significant variability, our patients underwent three tests at each altitude (nine tests in all): the first test was considered a familiarization trial and was excluded from further analysis. Thus, at each altitude we computed the mean of the other two tests to obtain reliable results, in accordance with the recent statement from the American Heart Association [21]. Furthermore, in a preliminary study in which we had assessed the reproducibility of our 6MWT protocol in 20 healthy volunteers on two different days we found no statistical differences.
Although the 6MWT can be considered sub-maximal exercise, in this study the V O2 measured at the end of the standardized 6MWT at low altitude was only 10% lower, on average, than the peak V O2 of a symptom-limited exercise test, in both patients and healthy subjects. These data indicate that our patients were able to perform an almost maximal effort test both at low and moderate altitudes: similar results have also been reported for tests at sea level [15–18].
Resting heart rate did not differ at the different altitudes: we believe that the lack of difference was probably due to the fact that the majority of our patients were treated with β-blockers and sometimes with β-blockers plus amiodarone.
The patients’ blood pressure rose at moderate altitude. In a previous report [5] blood pressure was unchanged at 2500 m: the difference could be explained by the higher number of patients with a history of hypertension in our study (48 versus 4%). LVD patients frequently have a history of hypertension [22] and therefore optimizing medical treatment before exposure to high altitude is mandatory.
The distance walked and the maximal V O2 decreased more in LVD patients than in normal subjects, despite a similar reduction in resting arterial P O2 . This is the first time arterial P O2 has been measured directly in cardiac patients in a mountain setting. Levine et al. [23] showed similar decreases in P O2 in seven cardiac and 13 non-cardiac subjects studied at simulated altitude: the hypoxemia was associated with activation of the sympathetic nervous system (demonstrated by an increase of urinary norepinephrine excretion). Erdmann et al. [5] studied patients with LVD in the mountains: they compared a bicycle stress test performed at 1000 m with the same test at 2500 m. In their trial the decrease of work capacity was moderate and similar in healthy subjects and in LVD patients, but the conditions were different from those in our study: the altitude was lower, V O2 was not measured, and the tests were performed indoors on a cycle ergometer. The harsher outdoor conditions could result in poorer performance in cardiac patients, but the aim of our study was specifically to assess physical activity in conditions normally encountered in the mountains. Interestingly, we did not observe any differences (with the exception of blood pressure) between 500 and 2000 m, while we found significant differences at 2970 m. In our population, patients with less work capacity (i.e. a shorter distance walked at 500 m) had the worst exercise performance at 2970 m ASL. These findings concord with those of a study by Agostoni et al. [6], in which the work rate in hypoxia decreased more in patients with a worse work rate at low altitude. These results indicate that patients with lower exercise tolerance at baseline should reduce their exercise intensity at 3000 m ASL by about 20%. Thus, pre-exposure sea level exercise testing (6MWT or CPET) is likely to be useful in providing activity guidelines for individual patients.
Various mechanisms have been considered to explain the reduction in exercise capacity during acute exposure to high altitude: since a reduction of cardiac output does not seem to be the only cause [24], changes in autonomic balance [25] and impaired left ventricular diastolic function [26] have also been suggested to be involved.
A recent study [27] on eight patients with coronary artery disease in a simulated exposure to 2500 m altitude showed a significant decrease in exercise-induced coronary reserve (− 18%), explained by the authors as abnormal exercise-induced vasomotion. One can speculate that a similar decrease in coronary reserve could have contributed to the decreased exercise tolerance recorded in our coronary patients.
The maximal rate pressure product and respiratory rate during exercise increased with altitude in the normal subjects, in accordance with findings of a study by Nihishara [28], but notably more so in cardiac patients; this suggests that hypoxia caused greater sympathetic activation in our patients than in the normal subjects. Despite the greater increase in respiratory rate, ventilation increased much less in the cardiac patients than in the healthy subjects, in accordance with a lower workload and a lower metabolic rate.
Clinical implications
This is the first study to have shown that physical activity in the mountains, in this case brisk walking at moderately high altitudes (2000–3000 m), in patients with stable LVD (determined clinically and by accurate functional evaluation) seems to be well tolerated and risk free. At 3000 m, however, it is advisable that LVD patients reduce their work rate by about 10–20%, depending on their baseline cardiac effort performance. A gradual ascent to altitude, early limitation of activity to a less vigorous level than that tolerated at low altitude, pre-ascent physical conditioning and rigorous blood pressure control should all help to minimize cardiac risk [3].
Patients with coronary artery disease, who are encouraged to perform physical activity in order to slow the progression of their disease [29] could be particularly gratified and motivated by the possibility of being able to do so in the majestic setting of mountains.
Limitations
Since neither a classical stress test nor Holter recordings were performed, it is not possible to exclude that episodes of silent ischemia were induced by the exercise at altitude. Such episodes do, however, seem to be improbable, given that no ischemia was detected by the preliminary myocardial scintigraphy, the patients were receiving optimized medical therapy and they had only a modest reduction in exercise tolerance.
In conclusion, we have demonstrated that non-acclimatized patients with stable ischemic LVD seem to have a good tolerance to moderate altitudes. We observed a moderate decrease in their work capacity at 2970 m, which was predictable from their baseline exercise performance.