
Abstract
Study objective
An evaluation of the effect of ambient temperature on morbidity from acute coronary syndromes (ACS) while avoiding confounding by air pollution.
Design
An ecological study in rural Greece.
Methods
Daily admissions to hospital because of ACS were recorded for 1 year and analysed versus daily temperature and humidity.
Results
For a 1°C decrease in temperature there was a 1.6% (95% confidence interval 0.9–2.2%) increase in admissions. This effect was more prominent in the elderly. No difference was detected according to sex or type of ACS.
Conclusion
It is important to implement measures against cold in coronary heart disease prevention, irrespective of air pollution.
Keywords
Introduction
Temperature and, to a lesser extent, relative humidity have been found to interfere with health and disease [1, 2], and with cardiovascular disease in particular [3–6]. Although there is concern about the possibility of an interaction between air pollution and temperature or season [7–9], and air pollution is considered to be a confounding factor in the relationship between temperature and morbidity/mortality [6], most studies do not account for it [3, 5, 6]. In order to eliminate the factor of air pollution, this study assesses the relationship between daily emergency hospital admissions for acute coronary syndromes (ACS) and the ambient temperature in rural Greece, which is reported to have very low levels of air pollution.
Design and methods
In order to conduct this ecological study, we randomly selected five rural Greek regions (Karditsa, Lamia, Chalkida, Kalamata and Zakinthos). A total of 739 339 people reside in the study regions and comprise approximately 12% of the population residing in rural Greece (census 2001). From 1 October 2003 to 30 September 2004, the daily counts of admissions for ACS in the regions' major hospitals were obtained. Additional information included sex, age in one of two groups (less or more than 65 years old) and type of ACS (acute myocardial infarction or unstable angina). The design and the baseline characteristics of the study are described elsewhere [10].
In Greece the climate is ‘Mediterranean’ with wet, mild winters and long, hot, dry summers. Daily mean, minimum and maximum air temperatures (°C) and daily mean relative humidity (%) were used for the analysis. Daily counts of ACS per region were analysed in a Poisson regression. The meteorological variables and their corresponding quadratic terms were used interchangeably as explanatory variables. Additional explanatory variables were day-of-week, holidays and the Monday effect. All logical interactions were checked.
Results
The total number as well as the daily number of admissions varied significantly per region because of the difference in the regions' populations. The age and sex distributions were assumed to be the same in the different regions as we consider rural Greece as an entirety. A total of 1608 patients (Table 1) were registered during the study period.
When a linear model between the logarithm of daily counts and the meteorological variable was assumed, mean temperature seemed to make the best fit among all meteorological variables. Moreover, the interaction of day-of-week with region seemed to play a role. Consequently, all relative risks for event occurrence are adjusted for these variables and appear in Table 1 along with their significance level.
The introduction of the quadratic term produced inconsistent results. The addition of the other explanatory variables (holidays or the Monday effect) or of interaction terms achieved no statistically significant results.
A statistically significant difference in the dependence of admissions on temperature was found between the two age groups (P = 0.031 for the interaction between age group and mean temperature). No difference was detected when stratifying according to type of ACS or sex.
This model tends to overestimate the number of admissions at temperatures less than 3°C; however, only 3% of the observations had a temperature in that range.
Discussion
The results of this study are in agreement with part of the research that has been conducted without controlling for the factor of air pollution [3, 5]. These results are not completely in accordance with the U-shaped relationship between temperature and mortality from coronary artery disease [4]. As an explanation of the absence of the ascending limb of the U-shaped curve, Fries et al. [11] have proposed that thermal stress caused by the atmospheric conditions in a temperate climate may be too weak to influence the incidence of acute myocardial infarction significantly. Finally, there are studies reporting a monotonic increase with the average temperature in hospital admissions for all heart disease [6].
Environmental temperature has an inverse relationship with blood pressure, and increased blood pressure may lead to myocardial ischaemia [12]. Furthermore, in cold conditions fibrinogen, certain clotting factors, the platelet count and their in-vitro aggregation, are all increased and promote clotting [12].
On the other hand, the relationship between temperature and ACS may be indirectly causal as indoor smoking, loneliness and body weight [13] increase during winter.
Although we have eliminated one possible confounding factor, air pollution, the detected association may still be a result of confounding. The lesser exposure to ultraviolet radiation and the lower vitamin C intake during cold days might be responsible for the increase in ACS [13].
Data on the temperature on the spot would clarify, to some extent, the nature of the relationship between temperature and ACS. Other limitations of the study are its short duration and the fact that it does not account for the harvesting effect [6]. As far as air pollution is concerned, its role can be further investigated with a comparison between the corresponding coefficients in polluted and non-polluted areas of the same country and during the same period.
Given the fact that the association between temperature and ACS may be attributed to pathophysiological factors, it would be wise to take sufficient precautions against cold. Reinforcement of protective medication against ACS during winter has to be investigated. Finally, the adoption of a healthier lifestyle during winter is recommended.
Relative risk of event occurrence for 1°C temperature and 1% relative humidity
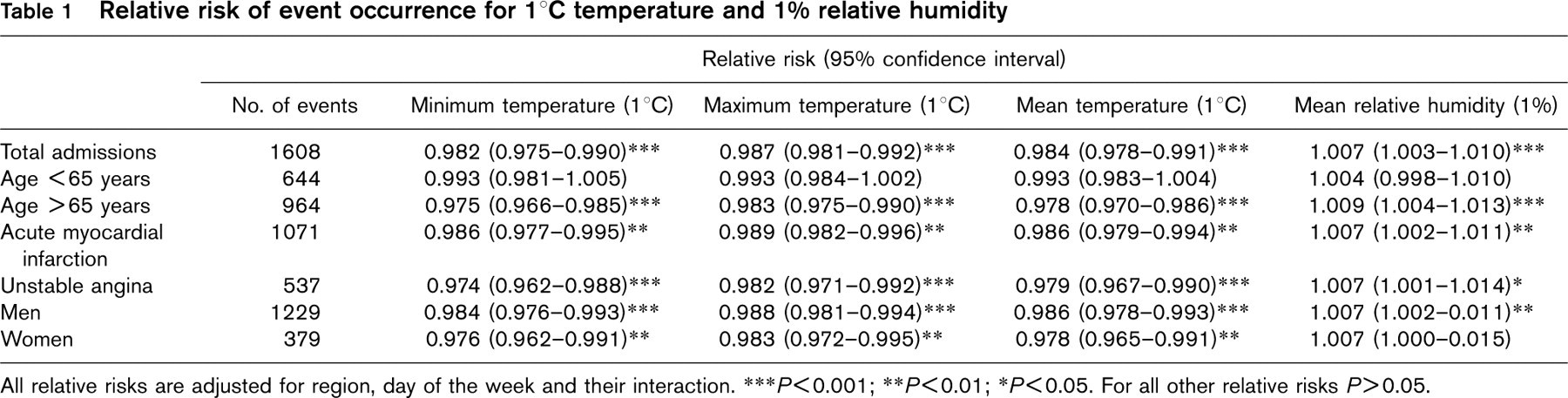
All relative risks are adjusted for region, day of the week and their interaction.
∗∗∗P < 0.001
∗∗P < 0.01;
∗∗ P < 0.05. For all other relative risks P > 0.05.