
Abstract
026: Relationship between VO2-kinetics indices on recovery and various degrees of coronary artery disease
E Klainman, A Landau, G Fink
“GEFEN”-Cardiac Health Center, Givatayim, ISRAEL
Background Recovery indices of oxygen consumption (VO2) kinetics were observed as important factors to differ patients (pts) with various degrees of chronic heart failure (CHF). The significance of the relationship between such indices and various degrees of coronary artery disease (CAD) isn't yet well established.
Aim of study To find the relationship between recovery VO2-kinetics indices and various degrees of CAD, in comparison to normal individuals.
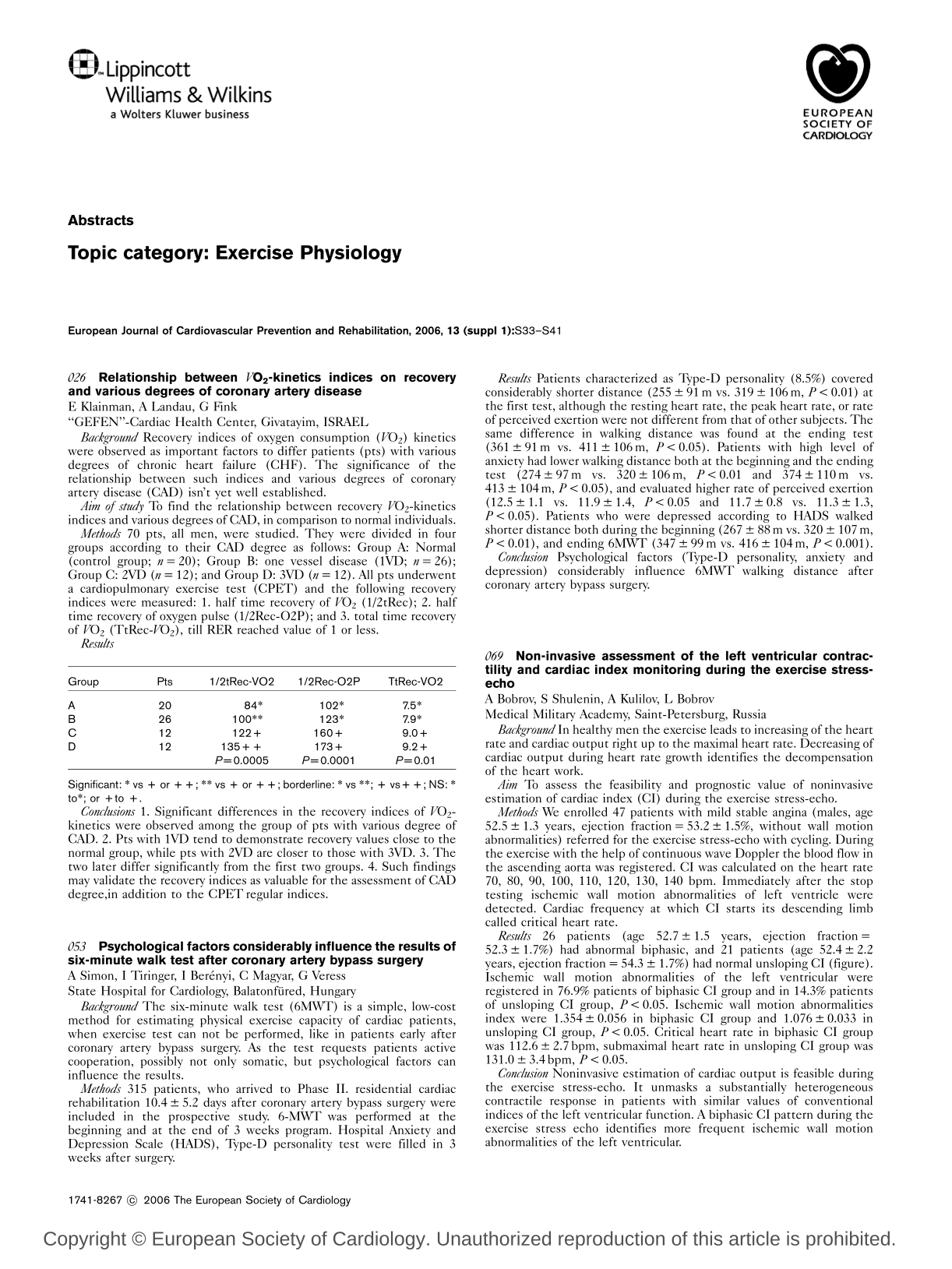
Methods 70 pts, all men, were studied. They were divided in four groups according to their CAD degree as follows: Group A: Normal (control group; n = 20); Group B: one vessel disease (1VD; n = 26); Group C: 2VD (n = 12); and Group D: 3VD (n = 12). All pts underwent a cardiopulmonary exercise test (CPET) and the following recovery indices were measured: 1. half time recovery of VO2 (1/2tRec); 2. half time recovery of oxygen pulse (1/2Rec-O2P); and 3. total time recovery of VO2 (TtRec-VO2), till RER reached value of 1 or less.
Results
Significant: ∗ vs + or + +; ∗∗ vs + or + +; borderline: ∗ vs ∗∗; + vs + +; NS: ∗ to∗;or + to +.
Conclusions 1. Significant differences in the recovery indices of VO2-kinetics were observed among the group of pts with various degree of CAD. 2. Pts with 1VD tend to demonstrate recovery values close to the normal group, while pts with 2VD are closer to those with 3VD. 3. The two later differ significantly from the first two groups. 4. Such findings may validate the recovery indices as valuable for the assessment of CAD degree, in addition to the CPET regular indices.
053: Psychological factors considerably influence the results of six-minute walk test after coronary artery bypass surgery
A Simon, I Tiringer, I Berényi, C Magyar, G Veress
State Hospital for Cardiology, Balatonfüred, Hungary
Background The six-minute walk test (6MWT) is a simple, low-cost method for estimating physical exercise capacity of cardiac patients, when exercise test can not be performed, like in patients early after coronary artery bypass surgery. As the test requests patients active cooperation, possibly not only somatic, but psychological factors can influence the results.
Methods 315 patients, who arrived to Phase II. residential cardiac rehabilitation 10.4 ± 5.2 days after coronary artery bypass surgery were included in the prospective study. 6-MWT was performed at the beginning and at the end of 3 weeks program. Hospital Anxiety and Depression Scale (HADS), Type-D personality test were filled in 3 weeks after surgery.
Results Patients characterized as Type-D personality (8.5%) covered considerably shorter distance (255 ± 91 m vs. 319 ± 106 m, P < 0.01) at the first test, although the resting heart rate, the peak heart rate, or rate of perceived exertion were not different from that of other subjects. The same difference in walking distance was found at the ending test (361 ± 91m vs. 411 ± 106 m, P < 0.05). Patients with high level of anxiety had lower walking distance both at the beginning and the ending test (274 ± 97 m vs. 320 ± 106 m, P < 0.01 and 374 ± 110 m vs. 413 ± 104 m, P < 0.05), and evaluated higher rate of perceived exertion (12.5 ± 1.1 vs. 11.9 ± 1.4, P < 0.05 and 11.7 ± 0.8 vs. 11.3 ± 1.3, P < 0.05). Patients who were depressed according to HADS walked shorter distance both during the beginning (267 ± 88 m vs. 320 ± 107 m, P < 0.01), and ending 6MWT (347 ± 99 m vs. 416 ± 104 m, P < 0.001).
Conclusion Psychological factors (Type-D personality, anxiety and depression) considerably influence 6MWT walking distance after coronary artery bypass surgery.
069: Non-invasive assessment of the left ventricular contractility and cardiac index monitoring during the exercise stressecho
A Bobrov, S Shulenin, A Kulilov, L Bobrov
Medical Military Academy, Saint-Petersburg, Russia
Background In healthy men the exercise leads to increasing of the heart rate and cardiac output right up to the maximal heart rate. Decreasing of cardiac output during heart rate growth identifies the decompensation of the heart work.
Aim To assess the feasibility and prognostic value of noninvasive estimation of cardiac index (CI) during the exercise stress-echo.
Methods We enrolled 47 patients with mild stable angina (males, age 52.5 ± 1.3 years, ejection fraction = 53.2 ± 1.5%, without wall motion abnormalities) referred for the exercise stress-echo with cycling. During the exercise with the help of continuous wave Doppler the blood flow in the ascending aorta was registered. CI was calculated on the heart rate 70, 80, 90, 100, 110, 120, 130, 140 bpm. Immediately after the stop testing ischemic wall motion abnormalities of left ventricle were detected. Cardiac frequency at which CI starts its descending limb called critical heart rate.
Results 26 patients (age 52.7 ± 1.5 years, ejection fraction = 52.3 ± 1.7%) had abnormal biphasic, and 21 patients (age 52.4 ± 2.2 years, ejection fraction = 54.3 ± 1.7%) had normal unsloping CI (figure). Ischemic wall motion abnormalities of the left ventricular were registered in 76.9% patients of biphasic CI group and in 14.3% patients of unsloping CI group, P < 0.05. Ischemic wall motion abnormalities index were 1.354 ± 0.056 in biphasic CI group and 1.076 ± 0.033 in unsloping CI group, P < 0.05. Critical heart rate in biphasic CI group was 112.6 ± 2.7 bpm, submaximal heart rate in unsloping CI group was 131.0 ± 3.4 bpm, P < 0.05.
Conclusion Noninvasive estimation of cardiac output is feasible during the exercise stress-echo. It unmasks a substantially heterogeneous contractile response in patients with similar values of conventional indices of the left ventricular function. A biphasic CI pattern during the exercise stress echo identifies more frequent ischemic wall motion abnormalities of the left ventricular.
132: Determination of reducing parasympathetic activity threshold in exercise by HRV method - a new way to prescribe training intensity in cardiac rehabilitation
J Rybicki, J Zub, A Wrzesniowski, W Grochulska, K Oleszczyk, L Polonski
Uppersilesian Rehabilitation Center “Repty” Tarnowskie Gory - Poland
Objective The aim of the study was to asses a method of determination exercise heart rate on parasympathetic withdrawal threshold (HRpwt) by HRV method in order to use it as training HR in cardiac rehabilitation (CR) and the analysis of correlation between HRpwt and HR on anaerobic threshold (HRat).
Methods 23 patients (age 48 ± 7 y) admitted 19 ± 7 days after AMI in CR program were assessed. The cardiopulmonary exercise test (CPET) on treadmill in ramp protocol was executed with recording the ambulatory ECG. The exercise time (ET) and the anaerobic threshold (AT) as well as HRat and peak oxygen uptake (peakVO2) were determined at the baseline and after 3 weeks of training pursued with an intensity of 90-95% of HRpwt. The RR intervals (RRi) were processed by FFT method in 250 RRi window sliding by step of 30 RRi for obtain of high-frequency (HF) component throughout CPET period. The successive percentage index of heart period variation (PIhpv) was calculated by “tone-entropy” method (Oida 1997). The HRpwt was defined visually by analysis of synchronic time course of HR and corresponding point on braking fashion drop in HF power spectrum as well as the same point in standard deviation of PIhpv curve. The analysis of correlation between HRpwt and HRat as well as comparison the CPET parameters before and after training were conducted.
Results There were no differences between HRpwt and HRat (104.0 ± 9.1 vs. 104.9 ± 9.7 bpm respectively, P < 0.254) and showed positive correlation (r = 0.8458, P < 0.000). The improvement in exercise variables was observed after training in ET from 699 ± 99 to 793 ± 110 s (P > 0.000), in peakVO2 from 22.1 ± 5.5 to 24.1 ± 5.7 ml/ min × kg (P > 0.001) as well as in AT from 15.5 ± 3.6 to 18.2 ± 4.1 ml/ min × kg (P > 0.000).
Conclusions Proposed method permits to defined of HRpwt in time of effort which positively correlate with value of HRat. The exercise capacity parameters increased after 3 weeks training with intensity of 90-95% of HRpwt in patients after AMI.
157: Feasibility, safety and prognostic value of exercise testing in patients aged 75 and older
G Slavich, D Tuniz, R Fregolent, L DiBenedetto
Cardiopulmonary Sciences Department, A.O. S.M.M., Udine, Italy
Purpose of the study To determine the feasibility of symptoms-limited ET for screening of CAD in this group, to evaluate the frequency of adverse outcomes and the prognostic significance, compared to younger patients.
Methods In a Regional Medical Centre, 1160 ETs were performed in one year. Test was successfully completed in 219 out of 247 elderly patients (age 78 ± 2.8, range 75-91 yrs; males: 57.5%). This group was compared to 113 consecutive patients (aged 59.4 ± 9, range 45-74 yrs, males 68.7%). Treadmill was utilized in 79.4% in the elderly, 96.3 of the control group. 36% of the elderly were on B-blockers (vs. 46%, P = 0.06); 5% were in atrial fibrillation (vs. 0.8%, P = 0.06) and 4.1% were paced (vs. none).
Results In the elderly group 28 pts (11.3%) did not complete the test (vs. < 1% in the control group) due to clinical instability (46%) or physical inability/musculoskeletal factors (54%). There was a significant difference (P < 0.001) in Exercise Time (4.6 ± 1.8 min. in the elderly group vs. 6.6 ± 2.4), METs (5.8 ± 1.8 vs. 7.9 ± 2.4), HR max (112 ± 18b/min vs. 130 ± 21) and DP (19323 ± 4356 b/min × mmHg vs. 23885 ± 5136). Reasons for termination: dispnoea was more frequent in the elderly group (4.5% vs. 0.9; P < 0.01); no differences for ST deviation, angina and fatigue. Non significant complications were observed. One patient in each group developed atrial fibrillation during effort. In 1 year follow-up there was 1 non cardiac death in the elderly (vs. 0) The incidence of major cardiac events was low (angina 8.4% in the elderly vs. 9.8; MI: 0.6% vs. 1; revascularization: 1.8% vs. 1; heart failure: 2.4% vs. 0; P = ns)
Conclusions The percentage of elderly referred for ET is significant (18.9%). In the vast majority of cases the test can be carried out (88%). ET in the elderly is safe and affords the objective evaluation of exercise capacity. These results suggest that an elderly individual capable of completing an ET has a favourable medium-term cardiovascular prognosis.
179: Evaluation quality of exercise training by heart rate variability in coronary artery disease patients
J Juskenas, J Brozaitiene
Institute of Psychophysiology and Rehabilitation, Kaunas University of Medicine, Lithuania
Objective The goal of this study was assessment quality of short-term exercise training during II rehabilitation period in coronary artery disease (CAD) patients by using heart rate (HR) variability, HR power spectrum and Poincare plots values.
Materials and methods We examined 350 CAD patients (average age 54.6 ± 9.9), 58.2% of them were post myocardial infarction (MI), 41.8% - after coronary artery bypass graft surgery (CABGS) or angioplasty (PTCA). Exercise training procedure include warming-up, bicycle (Kettler) training, strength improving in lower extremities, respiration exercises and cool-down with relaxation. HR monitoring, followed by tele-ECG, blood pressure, clinical symptoms and Borg scale registration was performed. Computerised analysis values of HR variability (HRV), power spectrum and Poincare plots, constructed from RR intervals during total exercise training procedure, were performed.
Results Positive dynamic of clinical symptoms, blood pressure, expression symptoms according Borg scale after training were determined (156.8 ± 20.9 vs. 97.6 ± 30.1 points). After training increase values of HRV (sRR, 32.5 ± 3.1 vs. 37.2 ± 3.4 ms and sLF, 12.1 ± 2.1 vs. 13.9 ± 1.9 ms) and total HRV in Poincare plots (RRt, 92.1 ± 3.8 vs. 99.3 ± 3.3 ms, ΔRRv. 65.7 ± 3.9 vs. 71.7 ± 5.1 ms, and P < 0.05) had showed restoration of HR reflex control in patients with posterior localisation and extensive MI. After CABGS in low risk patients increase values of HRV (sRR, 37.8 ± 1.6 vs. 41.2 ± 1.7 ms, sLF, 11.1 ± 1.9 vs. 13.9 ± 0.8 ms, P < 0.05) had showed positive influence of training. In CABGS patients with dominance occlusion in right coronary artery more expressed dynamic of HRVafter session was established, if compare with occlusions in other localisations.
Conclusion Positive dynamic of clinical data and heart rate variability had showed recovery of reflex control in autonomic regulation and effective individualized exercise training program for CAD patients during early rehabilitation period.
195: Intensity of training in coronary patients: heart rate on the anaerobic threshold in relation to karvonen method
J Rybicki, K Oleszczyk
Uppersilesian Rehabilitation Center “Repty” Tarnowskie Gory - Poland
Background The heart rate (HR) on anaerobic threshold (HRat) has been considered as a gold standard in determining the training HR (THR) in aerobic exercise training of cardiac patients. In the practice, the exercise training intensity (trINT) is prescribed on the level of 5080% of HR reserve (HRR) in dependence on exercise capacity and risk stratification. The aim of the study was to determinate of HRat and calculate of corresponding trINT according to Karvonen method as well as analysis of the correlation between trINTand exercise capacity for the verification of the principle “higher relative intensity of training for higher fitness patients (Ps)”.
Methods The study group consist of 42 Ps (age 50 ± 8 years) enrolled to the stationary cardiac rehabilitation (CR) program 20 ± 9 days after coronary events. The symptom limited cardiopulmonary exercise test (CPET) on treadmill in ramp protocol was executed to determinate rest HR (rHR) and peak HR (pHR) for calculation of HRR (HRR = pHR -rHR) as well as peak oxygen uptake (peakVO2), oxygen uptake on anaerobic threshold (AT) and HRat. The percentage value of trINTon HRat was calculated by transformed Karvonen formula: trINT= 100 × (HRat - rHR)/HRR. The asses correlation between trINTand peakVO2 was performed.
Results The mean value of rHR, pHR and HRR were respectively 64.5 ± 8.9; 123.8 ± 13.7 and 59.3 ± 11.7bpm as well as HRat was 101.1 ± 8.9 bpm corresponding to 62.9 ± 12.0% of trINT. The exercise capacity measured by peakVO2 and AT were 23.0 ± 4.0 and 16.0 ± 2.5 ml/min × kg respectively. The negative correlation between trINTand peakVO2 was found (r = −0.3625, P < 0.018).
Conclusions The heart rate on anaerobic threshold corresponded with 63% intensity of training according to calculation by Karvonen method. The negative correlation between intensity of training on anaerobic threshold and exercise capacity not confirm the principle “higher relative intensity of training for higher fitness patients”.
214: Early heart rate response during treadmill exercise testing is mainly determined by cardiorespiratory fitness
A Kalogeropoulos, P Mylona, B Kommata, J Chiladakis, D Alexopoulos
Division of Cardiology, University Hospital of Patras, Greece
Background Recent evidence suggests that heart rate response during early exercise stages (ΔHR) might have important prognostic implications and provide information beyond heart rate recovery (HRR). We investigated the determinants of ΔHR in a low-risk population and its correlation with HRR.
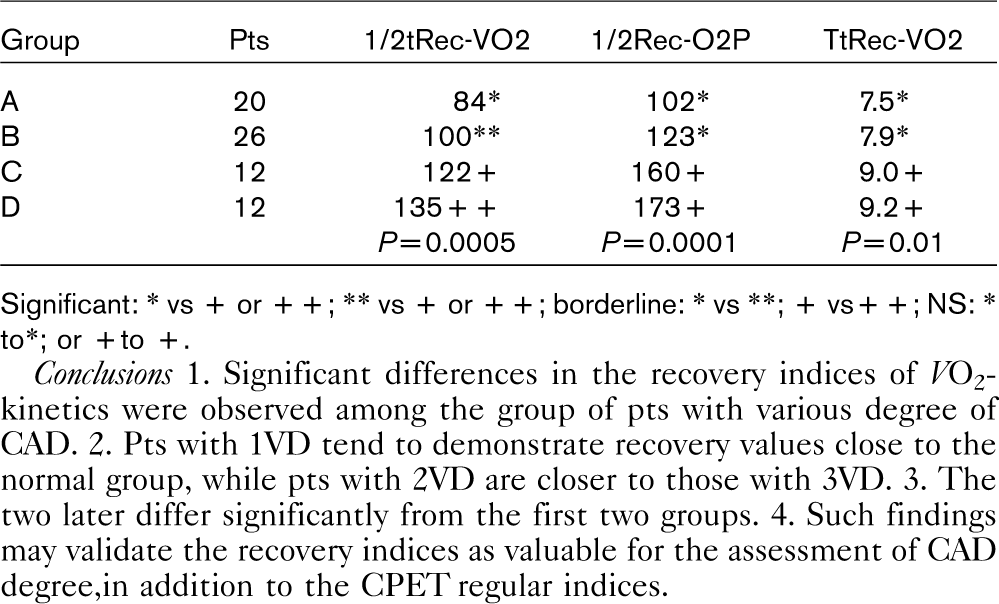
Methods We studied 176 healthy volunteers (44 ± 14 yrs, 60.2% male), without history of cardiovascular disease or known diabetes mellitus, who underwent exercise testing on a treadmill (ETT, protocol: Bruce) as part of a coronary calcium screening protocol. Subjects with rate-modulating drugs were excluded from the study. Heart rate (HR) at the end of stage I of the protocol was recorded and the increase from standing baseline HR was defined as the early response (ΔHR). HRR was defined as peak HR minus HR at 1st min of recovery.
Results Subject characteristics are presented in Table.
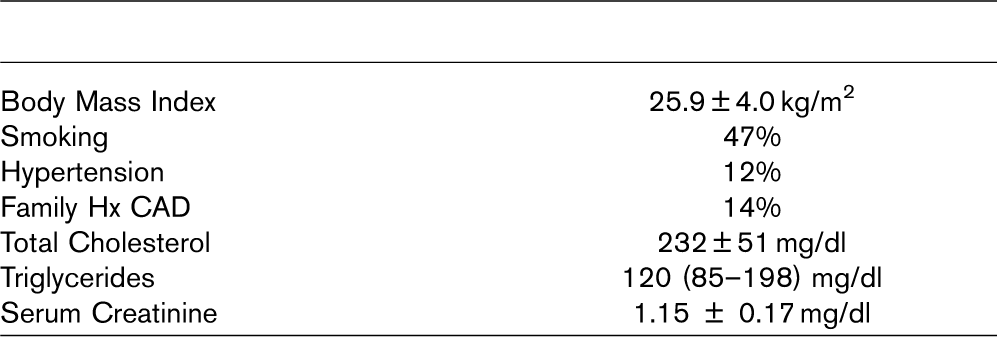
ST-segment depression suggestive of possible coronary artery disease was observed in 10 patients (5.7%). Mean exercise time was 625 ± 170 s. HR increased from 81 ± 14 bpm at baseline to 115 ± 20 bpm at the end of stage I (ΔHR = 34 ± 15bpm). Peak HR was 166 ± 21 bpm and declined to 130 ± 21 bpm at 1st min of recovery (HRR = 36 ± 11 bpm). In multivariate models including baseline characteristics and exercise variables, only exercise time (β = −0.59, P < 0.001) was found to predict ΔHR after accounting for age and baseline HR. There was no correlation between AHR and HRR (r = 0.00, P∼1.0).
Conclusions Reduced exercise capacity is associated with exaggerated sympathetic response at the onset of exercise, regardless of age and baseline HR. This response appears to be completely independent of HRR.
220: Mobilisation of endothelial progenitor cells after acute exercise in young and healthy volunteers
E Van Craenenbroeck, D Van Bockstaele, I Goovaerts, S Haine, C Vrints, V Conraads
Department of Cardiology, University Hospital Antwerp, Belgium
Background Circulating endothelial progenitor cells (EPCs) are characterized by co-expression of hematopoietic and endothelial markers. In response to tissue injury, the number increases and they contribute to neovascularization. A single episode of exercise mobilizes EPCs in patients with coronary artery disease, after exceeding the ischemic threshold. Aim of the study was to investigate the effect of acute exercise on the number of circulating EPCs in healthy volunteers.
Methods Eleven healthy students without known CV risk factors were enrolled. Venous blood was sampled before and after symptom-limited bicycle test with gas-analysis. Flow mediated dilation (FMD) of the brachial artery was assessed at baseline and after exertion using ultrasound. Circulating EPCs (CD34 + /VEGFR2 +) were analyzed by FACS after immunomagnetic CD34 + separation.
Results The absolute number of circulating EPCs increased acutely in healthy subjects following exercise (median 11 cells/ml (6-40) vs. 30 cells/ml (9-48), P = 0.034). There was no significant increase in relative EPC number within the white blood cell population. Endothelial function significantly ameliorated immediately after exercise (6.7% [5.2-8.7] vs. 8.6% [5-12], P = 0.019). There was no relation between changes in EPC counts and FMD. Even though lipid concentrations were within normal levels, exercise-induced increase in EPCs was positively correlated to LDL-cholesterol (r = 0.745, P = 0.0008) and total cholesterol/HDL cholesterol ratio (r = 0.717, P = 0.013). There was a negative correlation with oxygen consumption (VO2) at the anaerobic threshold (r = −0.830, P = 0.003) and with maximal VO2 (r = −0.636, P = 0.035).
Conclusion In young, healthy subjects, the number of circulating EPCs increased significantly after a single episode of maximal exertion. A less favorable CV risk profile (i.e. more atherogenic lipid profile, lower exercise capacity) seemed to facilitate the release of EPCs in this population.
221: Endothelial function in highly endurance-trained and sedentary young men: effects of acute aerobic exercise
Øivind Rognmo, Christian Kahrs, Tor-Halvor Bjørnstad, Bye Anja, Arnt-Erik Tjønna, Tomas Stølen, Per-M Haram, Stig Slørdahl, Ulrik Wisløff
Norwegian University of Science and Technology, Norway
Background Although regular exercise training has emerged as a powerful tool to reverse endothelial dysfunction, the effect in young, healthy subjects are less clear and data are conflicting. In the present study we determined the effect of aerobic capacity and a single bout of high-intensity exercise on endothelium-dependent dilatation, brachial artery diameter, peak blood flow, nitric oxide production and antioxidant status in healthy men.
Design Ten highly endurance-trained male athletes (mean ± SEM 23.5 ± 0.9 years, min−1), and seven-kg−1·182.6 ± 2.4 cm, 72.5 ± 2.4kg, maximal oxygen uptake 75.9 ml healthy sedentary males (25.4 ± 1.2 years, 183.9 ± 3.74 cm, 92.8 ± 3.9 kg, maximal min−1) took part in the study. Endothelium-dependentkg−1·oxygen uptake 47.7 ml dilation, brachial artery diameter and peak blood flow was measured using ultrasound and Doppler before a single bout of high-intensity exercise, 1 h, 24 h and 48 hours post-exercise. The exercise session consisted of treadmill running for 5 × 5 minutes intervals at 90% of maximal heart rate. Venous blood was drawn for measuring nitric oxide bioavailability and antioxidant status at all time-points when endothelial function was assessed.
Results and conclusion Athletes had larger arterial diameter and peak flow but similar endothelium-dependent dilation as untrained subjects, i.e. athletes had larger capacity for blood transport compared with their untrained counterparts. The observed endothelium-dependent dilation, bioavailability of nitric oxide and the antioxidant status in blood were highly dependent upon the time elapsed after the exercise-session.
224: Differences in cardiopulmonary exercise parameters in ischemic and non-ischemic cardiopathies and their response to exercise training
JP Schmid, P Hochstrasser, R Gaillet, H Saner
Swiss Cardiovascular Centre Bern, Switzerland
Background Exercise capacity and prognosis in chronic heart failure (CHF) appears to vary with the aetiology of the cardiopathy. Peak VO2 and VE/VCO2 slope have been shown to be strong predictors of outcome in these patients (pts). Whether there are differences of these parameters in pts with ischemic heart disease (IHD) and non-IHD and whether these might account for different outcomes is unknown.
Methods At the entry of a 3 months outpatient cardiac rehabilitation programme, 170 stable heart failure pts underwent a symptom limited cardiopulmonary exercise stress test (CPX). 91 pts (96.7% male, mean age 63.3 ± 9.3 years) suffered from IHD, 89 pts (76.4% male, mean age 55.6 ± 11.7 years) from non-IHD.
Results During CPX, non-IHD pts reached a higher peak VO2 (18.6 ± 5.8 ml/kg/min. vs. 16.4 ± 3.8 ml/kg/min., P = 0.017) than IHD pts and VE/VCO2 slope was lower (30.1 ± 5.6 vs. 32.7 ± 5.8, P < 0.001), although left ventricular ejection fraction (EF) was more severely depressed in the non-IHD group (26.8 ± 7.6% vs. 29.5 ± 7.1%, P = 0.010) and enddiastolic diameter (LVEDD) was larger (65.5 ± 8.1 vs. 62.7 ± 10.0 mm, P = 0.079). During the 3 months exercise training programme, peak VO2 increased by 19% in the non-IHD vs. 10% (P = 0.452) in the IHD pts group and VE/VCO2 slope decreased by 12% respectively 9% (P = 0.920). EF (+ 30% vs. +17%, P = 0.036) and LVEDD (−6% vs. −2%, P = 0.001) showed significantly different improvements in favour of the non-IHD group.
Conclusions Despite a lower EF and a larger LVEDD, peak oxygen uptake is higher and VE/VCO2 slope is lower in non-IHD pts than in IHD pts. This reflects a lower impact of the reduced left ventricular function on peripheral adaptation processes and a higher recovery potential, as confirmed by the significantly better improvement of EF and LVEDD after cardiac rehabilitation.
242: Comparison of the prognostic value of peak vo2, peak circulatory power and VE/VCO2 slope in chronic heart failure patients treated with beta-blockers
Antonio Miguel Ferreira, Miguel Mendes, Antonio Ventosa, Carlos Aguiar, Jorge Ferreira, Jose Aniceto Silva
Hospital Santa Cruz, Portugal
Background Beta-blockers (BB) improve survival in chronic heart failure (CHF) without influencing peak oxygen uptake (PVO2), a strong predictor of mortality. This raises the concern that the prognostic value of PVO2 may be impaired in this setting. The purpose of this study was to ascertain the value of PVO2 in predicting outcome in CHF patients treated with BB and to compare it with 2 new exercise parameters, the VE/VCO2 slope and the peak circulatory power (CP) defined as PVO2 × maximal systolic blood pressure (SBP).
Methods We studied 127 consecutive patients with CHF treated with BB who underwent symptom-limited treadmill cardiopulmonary testing. Using a Cox proportional hazards model, univariate and multivariate hazard ratios (HR) were determined for all variables predicting the combined end point of death or heart transplantation. The discrimination power of independent predictor variables was tested by calculating the area under a ROC curve.
Results During a median follow-up of 14.2 months among survivors, 5 (3.9%) patients died and 11 (8.7%) underwent cardiac transplantation. Univariate analysis yielded 4 predictors of death or transplantation: PVO2 (HR 0.81; 95% CI 0.71-0.93; P = 0.003); VE/VCO2 slope (HR 1.18; 95% CI 1.11-1.26; P < 0.001); CP (HR 0.98 for each increment of 10 mmHg.ml/kg/min; 95% CI 0.97-0.99; P < 0.001); and the increase in SBP (HR 0.65 for each 10 mmHg; 95% CI: 0.52-0.81; P < 0.001). However, only VE/VCO2 slope (HR 1.18; 95% CI 1.10-1.26; P < 0.001) and the increase in SBP (HR 0.77; 95% CI 0.60-0.98; P = 0.033) remained statistically significant in the multivariate model.
Both these variables showed good discrimination power: area under ROC curve 0.87 (95% CI 0.77-0.98; P < 0.001) and 0.80 (95% CI 0.68-0.93; P < 0.001), respectively.
Conclusions PVO2 is not an independent predictor of death or cardiac transplantation in CHF patients treated with BB. VE/VCO2 slope has greater prognostic value than PVO2 and CP in this setting.
261: Combination of losartan and exercise improves endothelial dysfunction in heart failure by different pathways than either alone
PM Haram, OJ Kemi, MA Høydal, U Wisløff, Ø Ellingsen
Norwegian University of Science and Technology, Norway
Background Both losartan and exercise have beneficial effects upon endothelial dysfunction in heart failure, and we wanted to compare the endothelial effects of combining losartan and exercise, with either used alone.
Methods Female Sprague Dawley rats with CHF were randomized to either losartan treatment, exercise, or a combination of both. Acetylcholine-mediated dilatation of the abdominal aorta was used as a measure of the endothelial function. Further, the sensitivity of the endothelial function to l-arginine and oxidative stress, contribution of nitric oxide and endothelium derived hyperpolarizing factor (EDHF) to vasodilatation as well as catecholamine sensitivity was determined.
Results Exercise and losartan had similar positive effects (P < 0.05) upon acetylcholine-mediated dilatation, but no synergism was observed when combining exercise and losartan. However, exercise alone or in the combination with losartan upregulated the nitric oxide-mediated part of the relaxation while losartan alone augmented the EDHF part of the relaxation. Monotherapy with exercise or losartan led to a decreased sensitivity to addition of either l-arginine or superoxide dismutase as compared to sedentary animals with heart failure. Losartan had a major effect upon the cathecolamine-sensitivity and the reduction in LVEDP as compared to exercise.
Conclusions Both losartan and exercise has beneficial effects upon the endothelial dysfunction in heart failure. However we see complementary actions, acting through different pathways for the improvement of endothelial function.
266: Different effect of prazosin on functional and morphological cardiovascular parameters in wistar rats and SHR
R Koprdová, M Cebová, F Kristek, J Torok
Institute of Normal and Pathological Physiology, SAS, Bratislava, Slovakia
We evaluated the effect of prazosin (Pra) on systolic blood pressure (SBP), heart weight/ body weight (HW/BW) ratio, functional and morphological parameters of thoracic aorta (AT) of spontaneously hypertensive rats (SHR) and normotensive Wistar rats. We used 4 groups of 4-week-old rats: 1) Wistar rats, 2) SHR, 3) Wistar + Pra and 4) SHR + Pra. Pra was administred 10 mg/kg/day in drinking water by gavage. The experiment lasted five weeks. SBP was measured on the tail artery by the plethysmographic method. For functional study AT was excised (from 6 rats of each group), cut into rings and mounted in tissue bath for measurement of isometric contractile force. For morphological study cardiovascular system of anaesthetized animals (11 rats of each group) was perfused with glutaraldehyde fixative under the pressure 120 mm Hg. AT was excised and processed according to standard electron microscopic procedure. Geometry of AT-wall thickness (WT), inner diameter (ID), cross sectional area (CSA) and WT/ID ratio were studied in light microscope. Long-term administration of Pra resulted in decrease of SBP and HW/BW ratio in both SHR and Wistar rats. Inspite of this the geometry of ATwas affected only in normotensive Wistar rats in which (exept of ID) WT, CSA, and Wt/ID ratio were decreased. In phenylephrine-precontracted aortic rings from SHR acetylcholine-induced relaxation was inhibited at higher concentration of acetylcholine. Long-term administration of Pra to SHR prevented inhibition of acetylcholine-induced relaxation. In conclusion, different effect of Pra administration to SHR and Wistar rats was observed. In SHR Pra prevented elevation of SBP, cardiac hypertrophy (HW/BW) and impairment of endothelium-dependent relaxation without influence on geometry of AT. In Wistar rats Pra decreased SBP and evoked cardiac hypotrophy (HW/BWratio) and remodeling of AT.
The study was supported by VEGA grants 2/6139/26 and 2/6150/26.
268: Reversing metabolic syndrome with high intensity training
AE Tjønna, Ø Rognmo, PM Haram, T Stølen, JP Loennechen, SA Slørdahl, U Wisløff
Norwegian University of Science and Technology, Trondheim, Norway
Background The worldwide epidemic of the metabolic syndrome requires cost-effective tools such as endurance training for prevention and rehabilitation. The present study determines the effects of moderate- and high-intensity (interval-training) exercise upon the metabolic syndrome.
Methods 28 persons with the metabolic syndrome were randomized to either 16 weeks, 3-times per week of high-intensity interval training (HIT) (92.5% of maximal heart rate), moderate intensity (MIT) (70% of maximal heart rate; covered the same distance as individuals in the HIT-group so that only exercise-intensity differed) or a control group that received advice from their general practitioner. Endothelial function in the brachial artery was measured by ultrasound.
Results 46% in the HITand 37% in the MTG, trained themselves out of the syndrome. Body weight decreased significantly (P ≤ 0.05) in both training-groups. HIT significantly decreased systolic (P = 0.004) and diastolic (P = 0.033) blood pressure, MIT significantly (P = 0.03) decreased systolic blood pressure, no changes occurred in the control group. HIT had a 22% increase in HDL cholesterol (P = 0.036), and a decrease in fasting glucose (P ≤ 0.05). ox-LDL was significantly (P = 0.003) reduced in the HIT group. Maximal oxygen uptake increased 35% in HIT (P ≤ 0.001) and 16% in MIT (P ≤ 0.001). Endothelial dysfunction was reversed in both training group, but the effect on flow mediated dilatation was most pronounced in the HIT group.
Conclusion High-intensity training is superior to moderately-intensity training and advice from the general practitioner to reduce the markers of the metabolic syndrome.
289: Reducing cardiovascular risk factors in obese adolescents
T Stølen, AE Tjønna, R Ødegård, U Wisløff
Norwegian University of Science and Technology, Norway
Objective The aim of the present study was to compare the effects of a multidisciplinary approach and intensity-controlled interval training on cardiovascular risk factors in obese adolescents.
Methods Obese adolescents (body fat 39.5 ± 4.2%) were randomised to multidisciplinary treatment or high intensity interval training after testing peak oxygen uptake and endothelial function (flow mediated dilatation). Multidisciplinary treatment: 3 hours of physical activity and/ or practical cocking and 2 hours of group therapy each month for 13 weeks. Interval training: 4 times 4 minutes at 85-95% of maximal heart rate separated by 3 minutes active pauses twice a week for 13 weeks.
Preliminary results Interval training increased peak oxygen uptake by 13.9%, maximal oxygen pulse by 17.6%, flow mediated dilatation by 140.9% and decreased fasting blood-insulin levels by 44.2%, blood-insulin levels 2 hours after a standard glucose test by 54.8% and fat percent by 4.8%. No change was observed in the multidisciplinary treatment group, except an improvement in maximal oxygen pulse by 6.2%. The close correlation between body fat and flow mediated dilatation observed at pre test was absent after 13 weeks of interval training.
Conclusions Two weekly high intensity exercise training sessions for 13 weeks reduced several known cardiovascular risk factors, such as flow mediated dilation, low peak oxygen uptake, insulin resistance and fat mass, and resulted in that flow mediated was unrelated to fatness after the intervention period.
317: Reduced peripheral skeletal muscle mass and abnormal reflex physiology in chronic heart failure
MF Piepoli, A Kaczmarek, DP Francis, W Banasiak, A Capucci, P Ponikowski
Heart Failure Unit, Cardiac Dept, Polichirurgico Hospital, Piacenza, Italy
Background The origin of the limiting symptoms in chronic heart failure (CHF) such as breathlessness and fatigue is not clearly known. We sought to determine whether there is a relationship between skeletal muscle mass in the limbs of patients with CHF and the muscle reflex activation.
Methods We studied 105 patients with stable CHF (age 59 ± 11 years, peak VO2 15.8 ± 4.7 ml/min/kg, VE/VCO2 slope 38.7 ± 11, LVEF 26 ± 3%) and 24 age-matched normal controls (age 61 ± 10 years, peak VO2 28.9 ± 6.1 ml/min/kg, VE/VCO2 slope 26.2 ± 3, LVEF 59 ± 4%). Each subject underwent measurement of leg ergoreflex (by the regional circulatory occlusion method) and quantitative assessment of lean skeletal muscle mass in both arm and leg by DEXA.
Results Patients had an abnormally high ergoreflex ventilatory response compared to controls (absolute increase 5.1 ± 0.2 l/min vs. 0.2 ± 0.6 l/ min, P < 0.001). The systolic pressure ergoreflex response was also elevated (25.8 ± 19 mmHg vs. 12.0 ± 8.5 mmHg, P < 0.01). Patients, compared to controls, showed reduction in lean muscle mass in total (55.0 ± 9.0 kg vs. 60.3 ± 8.8 kg, P <0.01), in the leg (16.4 ± 2.8 kg vs. 19.6 ± 2.9 kg, P <.0005) and in the arm (5.6 ± 1.2 kg vs. 6.9 ± 1.1 kg, P < 0.0005). There were correlations between the ergoreflex and muscle mass (r = −0.6 for the leg), (r = −0.5 for the arm) (P < 0.05). Measures of lean tissue were also significant predictors of exercise limitation (peakVO2, r = 0.46, P < 0.0001), of increased ventilatory response to exercise (VE/VCO2 slope, r = 0.44, P < 0.0001) and but not of resting LVEF (r = 0.1, P = NS).
Conclusion Depleted peripheral muscle mass is significantly related to ergoreflex activity and exercise limitation in CHF. Ergoreflex assessment in one limb (leg) predicts lean tissue loss measured in a different limb (arm), supporting a systemic activation of the muscle reflex system in CHF.
319: The relation of limiting symptoms of chronic heart failure to skeletal muscle ergoreflex activation
MG Poltavskaya, IV Molchanova, AV Chaplygin, AL Syrkin
Moscow Medical Academy, Cardiology Clinic, Russian Federation
Background In chronic heart failure (CHF) decreased ventilatory efficiency, breathlessness and fatigue are supposedly caused by skeletal myopathy via ergoreceptor activation. The aim of the study was to determine whether the limiting symptoms of CHF are related to muscle ergoreflex activity.
Methods Ergoreflex ventilatory (VE, % maximal) and diastolic blood pressure (DBP, mmHg) responses to handgrip exercise (regional circulatory occlusion method) and functional capacity [cardiopulmonary exercise test and Duke Activity Status Index (DASI)] were measured in 50 patients with LVEF < 45% (age 63.7 ± 8.8): 16 NYHA class I (VO2peak 18.7 ± 2.4 ml/min/kg, DASI 37.2 ± 5.3), 20 class II (VO2peak 14.9 ± 1.8 ml/min/kg, DASI 28.8 ± 5.6), 14 class III (VO2peak 10.8 ± 2.0 ml/min/kg, DASI 16.9 ± 4.8); and in 30 control age matched post infarction asymptomatic patients with LVEF > 55% (VO2peak 26.7 ± 4.6 ml/min/kg, DASI 52.5 ± 3.7).
Results NYHA class I patients, though limited in VO2peak and DASI had no significant elevation of ergoreflex VE and DBP responses to exercise and of VE/VCO2 slope (6.0 ± 1.8% vs. 2.3 ± 0.1%; 0.70 ± 0.01 mmHg vs. 0.60 ± 0.01 mmHg, 33.8 ± 1.6 vs. 29.5 ± 4.6, P = ns for all). Enhanced reflex effects and VE/VCO2 slope were found only in symptomatic patients compared to controls (NYHA class II/ III: VE increase 27.5 ± 2.1%, P < 0.002/37.6 ± 2.5%, P < 0.001; DBP increase 3.10 ± 0.02 mmHg, P < 0.02/4.70 ± 0.01 mmHg, P < 0.04; VE/ VCO2 slope 47.8 ± 0.9, P < 0.003/51.1 ± 0.7, P < 0.002). Ergoreflex VE response correlated with VE/VCO2 slope (r = 0.75, P < 0.05) and decrease of VO2peak (r = −0.64, P < 0.05) in patients not receiving beta-blockers and with DASI irrespective of therapy (on metoprolol r = −0.46, P < 0.05; without beta-blockers r = −0.57, P < 0.05).
Conclusion The association of ergoreflex overactivation with symptomatic stages and correlation with subjective functional index supports the ‘muscle hypothesis’ of origin of limiting symptoms in CHF.
337: Clinical relevance of functional and depressive scores in patients with chronic heart failure
Maria Nikolaou, John Parissis, Kalirroi Kourea, Dimitrios Farmakis, Vassiliki Bistola, Constantinos Papadopoulos, Dimitrios Karatzas, Gerasimos Filippatos, Stamatis Adamopoulos, Dimitrios Kremastinos
Heart Failure Clinic, Attikon University Hospital, Athens, Greece
Aim Limited exercise capacity and emotional distress are associated with clinical deterioration and adverse outcomes in chronic heart failure (CHF) patients. We assessed the clinical value or representative depression (Beck Depression Inventory self -assessment instrument (BDI), Zung self-rating depression scale) and functional scores (Kansas City Cardiomyopathy Questionnaire (KCCQ) and Duke Activity status index) in CHF patients and correlated them with their neurohormonal activation and exercise capacity.
Methods We studied 120 CHF patients (LVEF < 40%, mean age 65 ± 5 yrs, mean NYHA 2.6 ± 0.6) during their hospitalization in our department, using the above depression and functional questionnaires. Plasma BNP and six-minute walk test (6MWT, as a marker of exercise capacity) were also evaluated.
Results 42 out of 120 (35%) patients had a Zung score > 50 and a BDI score > 10 and have been characterized as having depressive symptoms. Depressives had significantly lower Duke (13.2 ± 9.9 vs. 23.6 ± 13, P < 0.05) and KCCQ functional (37.4 ± 15% vs. 52.6 ± 19.5%, P < 0.05) scores. Furthermore, there were significantly higher levels of plasma BNP (1080 ± 105 vs. 975 ± 85ng/ml) as well as reduced exercise capacity (6MWT 270 ± 130 vs. 337 ± 133 m, P < 0.001) in patients with depressive symptoms. Significant correlations were observed between plasma BNP and Zung (r = 0.30, P < 0.05), Duke (r = −0.40, P < 0.01) and KCCQ functional (r = −0.31, P < 0.05) scores.
Conclusion CHF patients with depressive symptoms, as estimated by the relevant scales, have impaired scores of physical activity, which may be associated with excessive neurohormonal activation and reduced exercise capacity.
349: Heart rate recovery after exercise is related to the heart rate variability in patients with heart failure
E Straburzynska-Migaj, H Wachowiak-Baszynska, R Ochotny, A Cieslinski
1st Dept. of Cardiology, University School of Medical Sciences, Poznan, Poland
Background The reduction of heart rate immediately after exercise is thought to be a function of a reactivation of the parasympathetic nervous system. Heart rate variability (HRV) is considered a measure of cardiac autonomic control. Both are decreased in patients with heart failure (HF). Our aim was to test the hypothesis that the difference in the heart rate recovery (HRR) after treadmill cardiopulmonary exercise test in patients with heart failure might be associated with indices of HRV.
Methods We investigated 58 patients with HF, sinus rhythm; mean age 51.3 ± 10 yrs, NYHA class 2.4 ± 0.8, LVEF 27.6 ± 7.9%. Time domain HRV parameters were measured based on 24-hour Holter monitoring. Maximal cardiopulmonary exercise test was performed in all patients. HRR was defined as a difference between peak exercise heart rate (HR) and HR measured 1 min (HRR1 = HRmax - HR 1 min after exercise) and 2 min after exercise (HRR2).
Results Patients were divided into two groups according to the median value of HRR1: group I (HRR16) and group II (HRR1 > 16). Patients of gr. I in comparison to gr. II had lower LVEF, were higher NYHA class, had lower peak VO2. HRR1 was 10.3 ± 4.8 vs. 25 ± 7, and HRR2 was 26.4 ± 9 vs. 44 ± 9; respectively group I vs. II; P = 0.00000. There were significant differences in HRV parameters between groups: SDNN 92.3 ± 33.5 vs. 109 ± 30; P = 0.03; SDANN 78.6 ± 30.6 vs. 99.6 ± 26; P = 0.003. There was significant correlation between HRR1 and SDNN (r = 0.34; P = 0.01), SDANN (r = 0.39; P = 0.002) and trend with SDNNI (r = 0.23; P = 0.08) and also between HRR2 and SDNN (r = 0.39; P = 0.002), SDANN (r = 0.41; P = 0.001), SDNNI (r = 0.32; P = 0.01).
Conclusion HRR at 1 and 2 minutes after exercise was related to HRV time domain indices. Further investigation is needed to establish if HRR, which is easier to determine, has the same prognostic value as HRVin patients with heart failure and if it could be used as a substitute for HRV analysis.
350: Metabolic compensation and ECG-diagnosis of ischemic heart disease in patients with type 2 diabetes mellitus
AnA Aleksandrov, IZ Bondarenko, SS Kukharenko, MN Yadrichinskaya, II Dedov
Endocrinology Research Center, Academy of Medical Science, Moscow, Russia
Background Myocardial ischemia causes the changes of myocardial action potential, which are reflected with the depression of STsegment on ECG. The main energy substrates in diabetic heart are fatty acids, which are formed from plasma triglycerides. The alterations of energy metabolism can alter the cardiac action potential formation in diabetic hear, that would explain the lower capacity of ECG to diagnose the myocardial ischemia in patients with diabetes.
Materials and methods 29 patients with DM 2 types (middle age 56.8 + 0.97 years) were studied. Ischemic heart disease was diagnosed with the standard treadmill test and stress - echocardiography. There were diagnostically significant ST-segment depression on electrocardiography stress-test and wall motion abnormalities on stress - echocardiography in all patients. HDL and triglycerides concentrations were measured with standard laboratory kids.
Results There were tendencies to statistically significant negative relationship between depth of ST-segment depression and plasma level triglycerides (r = −0.343, Ð = 0.064) and positive relationship between depth of ST-segment depression and plasma level LDL (r = 0.413, Ð = 0.079). The sum of ischemic ST-segment depression depths (7.6 + 1.37mm vs. 5.8 + 0.71mm; P = 0.011) was significantly higher in patients with normal level of triglycerides, than in patients with elevated ones. There were significant correlations between level of glycosylated hemoglobin HbA1c and depth of ST-segment depression (r = −0.385; P = 0.048).
Conclusion Capacity of electrocardiography to diagnose the myocardial ischemia in patients with diabetes mellitus depends on intensity of metabolic diabetes disorders such as plasma levels of triglycerides and glycosylated hemoglobin.
352: Endothelial function in individuals with metabolic syndrome: effects of acute and chronic aerobic exercise
AE Tjønna, Ø Rognmo, T Stølen, JP Loennechen, SA Slørdahl, U Wisløff
Norwegian University of Science and Technology, Trondheim, Norway
Background Although regular exercise training has emerged as a powerful tool to reverse endothelial dysfunction, the effect in individuals with metabolic syndrome is less clear. In the present study we determined the effect of a single bout and chronic exercise, comparing high-intensity training with moderate intensity training effects upon endothelium-dependent dilatation.
Methods 28 persons with the metabolic syndrome were randomized to 16 weeks, 3-times per week of either high-intensity interval training (HIT) (92.5% of maximal heart rate), moderate intensity training (MIT) (70% of maximal heart rate; covered the same distance as individuals in the HIT-group so that only exercise-intensity differed) or control group that received advice from their general practitioner. Endothelium-dependent dilation was measured using ultrasound before a single bout of exercise, acutely after exercise, 24 h, 48 h and 72 hours post-exercise, and the same measures were repeated after 16 weeks of exercise.
Results One bout of HIT improved endothelial function, with a peak immediately after exercise, and it lasted for at least 72h (P ≤ 0.001). MITalso improved endothelial function, but the effect disappeared at a place between 24-48 hours (P ≤ 0.01 only at 24 h). The control group showed no changes. After 16 weeks of training, HIT also improved endothelial function, but now the effect disappeared a place between 48-72h post exercise (P ≤ 0.05). In the MIT group endothelial function was only improved acutely after exercise (P ≤ 0.05). The control group showed no changes. When looking at baseline changes in endothelial function before and after the 16 weeks of training, HIT had a 170% increase (P ≤ 0.0001), MIT had a 104% increase (P ≤ 0.01), while control group had no changes.
Conclusion One bout of HIT improved endothelial function both before and after chronic exercise, while the effects in the MIT group were less pronounced.
357: Exercise testing for assessment of autonomic dysfunction in patients with familial amyloidotic polyneuropathy type I
C Azevedo Coutinho, G Cantinho, MJ Correia, I Conceição, MG Varela, AR Victor, A Bernardes, A Silva, MG Lopes
Santa Maria Hospital, Portugal
Background Heart rate (HR) response to exercise measured by chronotropic index (CI) and heart rate recovery (HRR) immediately after exercise reflect cardiac autonomic control. Familial amyloidotic polyneuropathy type I (FAP-I) is a hereditary disorder characterized by progressive sensory-motor and autonomic neuropathy. We sought to determine CI and HRR in FAP patients (pts) and to correlate with I-123 metaiodobenzylguanidine (MIBG) myocardial imaging and heart rate variability (HRV).
Methods Exercise stress tests were performed in 36 FAP pts (age = 41 ± 14 years) with different stages of the disease (19 with neurological involvement-group I and 17 asymptomatic carriers-group II) and in 36 age-matched control subjects. CI was defined as: (peak HR-rest HR)/(220-age-rest HR) with CI < 0.8 defined as low. Abnormal HRR was defined as a fall in HR during the first minute after exercise ≤ 18beats/min. FAP pts also underwent heart to mediastinum (H/M) MIBG uptake and time and frequency domain HRV analysis from 24-h Holter recordings.
Results FAP pts had significantly higher rest HR, lower exercise duration and lower CI and HRR than the healthy subjects. The decrease in HRR observed in FAP pts correlated with SDNN (r = 0.51, P = 0.002) total power (r = 0.58, P = 0.0002), VLF (r = 0.57, P = 0.0003), LF (r = 0.55, P = 0.0005) and HF (r = 0.5, P = 0.002) while the CI correlated with LF/HF (r = 0.39, P = 0.02) and MIBG uptake (r = 0.41, P = 0.02). Group I differ from group II by significantly lower CI (0.63 ± 0.23 vs. 0.81 ± 0.24, P < 0.03) and HRR (20 ± 9 vs. 27 ± 12 beats/min, P < 0.04). The CI was decreased in 15/19 group I pts and in 5/17 group II pts (P = 0.008) and the HRR was abnormal in 9/19 group I pts and in 3/17 group II pts (P = ns).
Conclusions CI and HRR, which are easy to calculate from data contained in exercise testing, can be very useful to identify autonomic imbalance in FAP. The abnormal HRR seems to be related to the decreased vagal activity and the attenuated CI to the sympathetic denervation.
420: The influence of beta-blocker therapy on correlations of nyha class, duke activity status index and 6 minute walk test with cardiopulmonary indices in chronic heart failure
MG Poltavs.kaya, IV Molchanova, AV Chaplygin, AL Syrkin
Moscow Medical Academy, Cardiology Clinic, Russian Federation
Background The diagnostic value of popular indices of functional status in chronic heart failure (CHF) such as NYHA class, Duke Activity Status Index (DASI) and 6 minute walk test in relation to peak O2 consumption (VO2) has been established before beta-blocking agents (BB) became the standard of therapy of this condition. There is evidence that BB improve symptoms but do not benefit peak VO2 (due to restraint of maximal heart rate and other mechanisms) and ventilatory levels. The aim of the study was to evaluate whether chronic BB therapy alters correlations of subjective functional indices with VO2 and ventilatory response to exercise (VE/VCO2 slope) in patients with CHF.
Methods We studied 50 patients with stable CHF: 24 - not receiving BB (age 64.7 ± 9.1 years, LVEF 26.9 ± 9.0%, peak VO2 14.4 ± 1.3 ml/ min/kg, VE/VCO2 slope 44.5 ± 0.8) and 26 matched patients on BB (age 62.3 ± 8.4 years, LVEF 25.6 ± 8.0%, peak VO2 15.2 ± 1.4 ml/min/kg, VE/ VCO2 slope 43.5 ± 0.7). Functional capacity was assessed by NYHA class, DASI, 6 minute walk test and symptom limited cardiopulmonary treadmill test.
Results In patients not receiving BB NYHA class, DASI and 6 min walk distance correlated with peak VE/VCO2 (r =-0.41; 0.59 and 0.62 respectively) and with VE/VCO2 (r = 0.56; −0.74; −0.48) (P < 0.05 for all correlations). In patients on BB therapy these parameters correlated neither with peak VO2 (NYHA class/DASI/6 min distance: r = −0.12/ 0.31/0.12) nor with VE/VCO2 (r = 0.36/0.21/0.13) (p = ns for all correlations). 6 min walk distance predicted symptom-based indices in both groups (without BB/on BB: NYHA class r = −0.58/-0.57, P < 0.05 for both; DASI r = 0.82, P < 0.001/r = 0.65, P < 0.01).
Conclusion In patients with CHF treated with beta-blockers NYHA class, DASI and 6 min walk distance correlate with each other but do not predict peak aerobic capacity and ventilatory efficiency.
425: Cardiorespiratory and muscular fitness are associated with lower central and total adiposity in a cohort of Greek women
G Nassis
Faculty of Physical Education and Sport Science, University of Athens, Greece
Recent evidence suggests that high cardiorespiratory fitness is related to favorable body composition both in children and adults (Nassis et al., Eur J Clin Nutr 2005; 59:137-141). Data on the effect of muscular fitness on total and central fatness are limited (Fogelholm et al., Int J Obes 24 Jan 2006, Epub ahead of print). The aim of the present study was to examine the association of cardiorespiratory (CRF) and muscular fitness with total and central adiposity in women. Three hundred and sixty-two women (18-58 years) volunteered for this study. CRF was evaluated with the UKK Institute 2-km walking test. Women walked the distance as fast as possible and the heart rate was measured immediately after the completion of the trial. The fitness index (FI), which indicates the fitness category with respect to persons of the same age, was calculated on the basis of age, body mass index (BMI), time taken to complete the walk and heart rate. Muscular fitness was assessed with the number of sit-ups completed in 30 sec. Total and central adiposity were evaluated with BMI and waist circumference (WaistC), respectively. Pearson correlation coefficient was employed to examine associations between variables since data were all normally distributed. About 34% of these women were overweight and obese whereas WaistC was above 88 cm in 10.5% of the subjects. FI was associated with lower BMI and WaistC (r = −0.289 and r = −0.276, respectively, P < 0.01). Number of sit-ups completed was also negatively related to BMI and WaistC after controlling for age (r = −0.192 and r = −0.305, respectively, P < 0.01). These findings suggest that both CRF and muscular fitness are associated with lower total and central adiposity in this group of women. These relations cannot establish causation but, given the limitations of the study, they suggest that both aerobic and muscular fitness should be improved to minimize the adverse effects of obesity.
432: Influence of menstrual cycle on myocardial contractility and chest pain during echocardiographic exercise stress test in premenopausal women with Angina and without stenosis in coronary arteries
A Grzybowski, W Puchalski, B Zieba, K Storoniak, W Sobiczewski, R Targonski, M Gruchala, A Butkiewicz, D Janczyk, A Rynkiewicz
I Dept. of Cardiology, Medical University of Gdansk, Poland
Objectives There is a lack of information on the relation between menstrual cycle and the results of echocardiographic exercise stress test performed during supine bicycle exercise. The purpose of the study was to estimate the influence of menstrual cycle on exercise stress test results in women with angina and normal coronary angiography.
Methods Premenopausal women (n = 28) with regular monthly menses presented typical angina, positive exercise stress ecg test and normal coronary angiogram were recruited for the study. Exercise stress echocardiography during supine bicycle exercise was performed once a week for four consecutive weeks. Women were randomly started on the trial protocol irrespective of their position in the menstrual cycle. We used bicycle 25W/2 min protocol to achieve at least 85% of the maximal heart rate or angina. Occurrence of angina, time to angina, blood pressure and segment myocardial contractility were analyzed. Blood samples were drawn before each stress test for FSH, LH, B-estradiol, progesterone estimation to define the position in menstrual cycle.
Results The rate of segmental left ventricular hypokinesis observed during exercise stress echocardiography was not significantly related to menstrual cycle (in early follicular, late follicular, early luteal and late luteal phase in 4, 4, 2 and 2 subjects, respectively). Angina occurred in early follicular, late follicular, early luteal and late luteal phases in 71%, 61%, 54%, 75% respectively, differences not significant. Time to chest pain was the longest in the late follicular phase (281.8 ± 128.2 sec) compared to early follicular (236.7 ± 101.5 sec), early luteal (203.7 ± 86.0 sec) and late luteal phase (240.4 ± 107.7 sec), P < 0.05.
Conclusion In women with typical angina and without significant stenosis in coronary arteries the position in menstrual cycle influences the time to angina but not myocardial contractility during echocardiographic exercise stress test.
434: The relationship between cardio respiratory fitness and lipoproteins in postmenopausal women
SE Barber, D Barker, LB Tan, KM Birch
Centre for Sport and Exercise Sciences, University of Leeds, United Kingdom
The menopausal transition in women is associated with an increase in the risk of cardiovascular disease (CVD). Whilst increased cholesterol is a major risk factor in postmenopausal women (PM), low concentrations of HDL appear to be more prognostic than high LDL concentrations. Cardio respiratory fitness (CRF) is associated with a reduction in CVD risk and thus this investigation aimed to assess the relationship between CRF and lipoproteins in PM. 42 PM (mean age 57.59 ± 3.29 yrs) were assessed for CRF via a Bruce test and assigned to a low/medium (< 40th percentile VO2 peak) or a medium/high (40th percentile) CRF group according to the Aerobic Centre Longitudinal Study classifications. Participants were assessed for percentage body fat (%F: skin fold assessment) and waist (W) and hip (H) circumferences. A fasting venous blood sample was analysed for total cholesterol (TC), HDL, LDL, and triglycerides (TG). CRF groups were compared using student t tests. The exercise duration (8.3 vs. 10.2 min: P < 0.01) and VO2 peak (23.57 vs. 31.65 ml/kg/min: P < 0.001) of the low/medium CRF group was significantly less than the medium/high CRF group respectively. %F, W, H and W:H were significantly higher in the low/medium CRF group (P < 0.05). There were no differences in TC, LDL, TC:HDL ratio or TG concentrations between the two groups (P > 0.05). HDL was not significantly different between the low/medium and medium/high CRF groups (1.95 vs. 2.3 mmol/l respectively, P = 0.07), however when participants were split into < 30th or 30th percentile VO2 peak, the difference in HDL (1.92 and 2.3 mmol/l) became significant (P < 0.05). The correlation between HDL and VO2 peak (r 2 = 42% P < 0.05) was abolished when %F, but not W or H were controlled for in a partial correlation. In postmenopausal women higher CRF is associated with improved body composition and HDL concentrations. The difference in HDL concentrations appears to be related to %F and not differences in regional fat distribution.
452: Influence of body mass index on exercise testing parameters
R Fregolent, D Tuniz, G Slavich
Cardiopulmonary Sciences Department, AOSMM, Udine, Italy
Objective The purpose of the study was to compare exercise parameters in patients with BMI 30 and patients with BMI < 30.
Methods 180 patients (aged 60.47 ± 12.7; males:114) were studied prospectively for diagnostic in 109 (60.6%) and functional evaluation in 71 (39.4%) with symptoms-limited treadmill exercise testing (Bruce protocol). Patients with BMI 30 were 41 (22.8%); males: 29 (71%); mean age: 59.24 ± 11.04 (vs. 139 in the BMI < 30 group; males:61%; mean age: 60.82 ± 12.64).
Results there was no significant difference between the groups in maximal heart rate (HR) (130.1 ± 20.2 beats/min in the group with BMI 30 vs. 130.6 ± 23.9), maximal systolic blood pressure (BP) (179.7 ± 30.7 mmHg vs. 175.3 ± 24.8), maximal diastolic BP (87.1 mmHg ± 12.3 vs. 84.2 ± 8.9), after the first minute of recovery HR (114.1 beats/min ± 21.2 vs. 110.6 ± 22) and the BP at third minute of recovery (152.8 mmHg ± 21.7 vs. 148.9 ± 22.6). There were significant statistical differences in: -exercise time (4.85 ± 1.8 min vs. 6.5 ± 2.9; P = 0.0004); increase of systolic BP (mmHg) over exercise time (min): 11.3 ± 9.9 mmHg/min vs. 6.8 ± 5.5; P = 0.0002; increase of HR over exercise time (min): 11.5 ± 6.6 beats min vs. 9.4 ± 5.2; P = 0.0034; HR recovery:15.95 ± 8.1 beats/min vs. 20.1 ± 10; P = 0.02.
Conclusions Preliminary results of this still ongoing study highlight that BMI ≥ 30 patients show a significant reduction of exercise time and HR recovery and greater HR and BP increase over minutes of exercise.
455: Relative intensity of aerobic training recommendations depend on mode of exercise
Manfred Wonisch, Peter Hofmann, Guenther Schwaberger, Gerhard Smekal, Rochus Pokan
Medical University Graz, Dep. Internal Med., Div. of Cardiology, Austria
Objective Training recommendations for aerobic exercise are often given as percentage of maximal heart rate (HR) or oxygen consumption (VO2) for all groups of endurance athletes as well as for prevention and rehabilitation. It is, however, unclear, if these recommendations are valid for all modes of aerobic exercise.
Methods Seven competitive triathletes (age: 27 ± 3 years, weight: 73 ± 10 kg, height: 183 ± 5 cm) were examined on three different days. They performed a maximal test on three different ergometers, i.e. treadmill, cycle ergometer and handle ergometer in randomized order to determine VO2, workload (P), HR, blood lactate concentration (La) and the corresponding individual aerobic (AT) and anaerobic threshold (ANT).
Results Maximal values were as follows: treadmill: VO2max: 68 ± 6 ml/ min/kg, Vmax: 19 ± 1 m/s, HRmax: 191 ± 7 1/min, Lamax: 9.5 ± 1.9 mmol/ l; cycle ergometer: VO2max:69 ± 7 ml/min/kg, Pmax: 416 ± 34W HRmax: 187 ± 7 1/min, Lamax: 12.6 ± 1.8 mmol/l; handle ergometer: VO2max: 47 ± 5 ml/min/kg, Pmax: 188 ± 24W HRmax: 176 ± 7 1/min, Lamax: 10.5 ± 2.1 mmol/l. The values at AT for treadmill vs. cycle vs. handle ergometer were: for VO2 46 ± 2 (68 ± 6%) vs. 35 ± 4 (51 ± 6%) vs. 17 ± 2 ml/min/kg (40 ± 3%), and for HR 148 ± 8 (78 ± 4%) vs. 127 ± 11 (68 ± 5%) vs. 113 ± 13 1/min (64 ± 7%). The values at ANT for treadmill vs. cycle vs. handle ergometer were: for VO2 59 ± 3 (87 ± 5%) vs. 54 ± 4 (78 ± 4%) vs. 31 ± 3 ml/min/kg (66 ± 7%), and for HR 175 ± 5 (91 ± 2%) vs. 163 ± 8 (87 ± 3%) vs. 146 ± 12 1/min (83 ± 6%).
Conclusion The relative intensity for exercise prescription of aerobic training is strongly coupled to the mode of exercise. To obtain a comparable metabolic strain (i.e. AT and ANT) exercise with more muscles involved need a higher relative percentage of VO2max and HRmax compared to exercise with less muscles involved. These findings should have wide implications for exercise intensity recommendations for all groups of athletes as well as for prevention and rehabilitation.
463: Peak exercise cardiovascular physiology during pregnancy
D Barker, D Schlosshan, S Barber, H McLoughlin, G Mason, LB Tan
Leeds General Infirmary, United Kingdom
Background Cardiovascular physiology of pregnancy at rest has been extensively studied, but how pregnancy alters cardiac reserve and cardiovascular physiology during peak exercise has not been systematically investigated, especially in longitudinal studies.
Objective We investigated peak exercise physiology in pregnancy and compared the results to the non-pregnant state.
Method We conducted a longitudinal study on 35 female volunteers (mean age 32 ± 6 years [range 18-41] who performed symptom-limited cardiopulmonary exercise tests (CPX). Tests were performed during pregnancy (mean gestation 32 weeks ± 6 weeks and then repeated 7 ± 4 months postpartum. The postpartum test was used as the control non-pregnant test. Measurements of peak oxygen consumption (VO2) and haemodynamic indices were obtained. Peak cardiac output (CO) was measured non-invasively using the CO2 re-breathing technique. Peak cardiac power output (CPO) was calculated from the product of CO and mean arterial pressure. Cardiac reserve (CRsv) was calculated by taking resting CPO from peak CPO.
Results Participants reported more tiredness during late pregnancy and showed significantly lower exercise duration (9.0 ± 2.1 vs. 10.8 ± 2.7 mins, P < 0.001) and absolute peak VO2 (1897 ± 279 vs. 2066 ± 410 mls min−1, P < 0.001) during pregnancy than the non-pregnant control. Despite this, there was no significant decrease in peak CO (15.0 ± 1.8 vs. 15.5 ± 2.2 lmin−1, P = 0.3) peak CPO (3.44 ± 0.6 vs. 3.50 ± 0.6watts, P = 0.6 or cardiac reserve (2.54 ± 0.62 vs. 2.67 ± 0.64watts, P = 0.3).
Conclusion Despite significantly lower exercise duration and peak VO2 during late pregnancy, directly measured cardiac function (CO, CPO, CRsv) at peak exercise was well preserved. Such a dichotomous relationship between the indirectly and directly measured parameters of cardiac function implies that symptom and exercise capacity changes during pregnancy may not truly reflect changes in cardiac function.
465: Correlation between 6-minute walk test and maximal stress testing parameters in pacemaker patients
LAP Sousa, RR Britto, EA Baião, BG Oliveira, SM Baracho, F Pacífico, A Oliveira, VT Carvalho, VCV Barros, A Ribeiro
Federal University of Minas Gerais, Newton Paiva University Centre, Brazil
Background and objective 6-minute walk test (6′T) is an established tool in the management of heart failure patients, although its utility in pacemaker (PM) clinic is uncertain. We evaluated the safety and the utility of 6′T in a PM clinic, as well as its correlation with maximal stress testing (ST).
Methods 24 stable rate-responsive PM patients (48 ± 14 years, 11M, 11VVI) underwent standard 6′T and maximal treadmill ST (CAEP protocol). A ROC curve was used to evaluate the performance of 6′T walked distance in prediction of good aerobic fitness, defined as maximal VO2 > 10 METs in ST.
Results 6′T was not related to significant complications or arrhythmias in simultaneous Holter monitoring. There were strong correlations between 6′T mean walked distance (557 ± 95m) and ST maximal VO2 (35 ± 12 ml/Kg/min, r = 0.71, P < 0.001), maximal HR in 6′T and ST (r = 0.69, P < 0.001) and final BP (r = 0.49, P = 0.016). The area under ROC curve was 0.92 and a walked distance > 538 m had 90% sensitivity and 79% specificity in recognizing maximal VO2 > 10 METs.
Conclusion 6′T and ST parameters were strongly correlated. 6′T is safe in PM patients and may be useful in PM clinics in recognizing well fitted patients that may not need to be submitted to a maximal ST.
514: Glimepiride and miocardial ischemia in diabetes mellitus type 2
An Aleksandrov, I Bondarenko, S Kukharenko, M Yadrichinskaya, I Dedov
Endocrinology Research Centre, Moscow, Russian Federation
Objective The aim of this study was to compare the effect of glimepiride and previous oral antidiabetic sulphonylurea drugs on the ischemic threshold during the exercise tests in patients (pts)with DM type 2 and ischemic heart disease.
Design An 8-week nonrandomized, crossover, controlled, open study investigating the effect of glimepiride on the ischemic threshold. 14 type 2 diabetics pts (8 males/6 females; aged 56.5 ± 6.9 years) had reproducible positive Stress-Echo tests for myocardial ischemia. The first test (1st) was done with previous antidiabetic sulphonylurea drugs before starting glimepiride treatment, the second test (2nd) four weeks after mono-therapy of glimepiride and before restarting initial oral sulphonylurea drugs, the third test (3rd) four weeks after restarting initial sulphonylurea drugs. The ischemic threshold was assessed with: heart rate blood pressure and oxygen consumption at the onset of 1.5 mm ST-segment depression and at peak exercise; at exercise duration and at the recovery of ST-segment depression and at the pain onset in seconds. Antianginal and antiischemic therapy was unchanged during the study.
Results Changes in the kind of hypoglycemic therapy were not followed with significant changes of concentrations of HbA1c and glucose in blood. Exercise duration of the 2nd test after glimepiride treatment was greater than during the 1st and the 3rd tests at the initial antidiabetic drugs (449.30 ± 133.10 vs. 415.40 ± 162.50, P < 0.05; 449.30 ± 133.10 vs. 400.70 ± 152.60, P < 0.05), as were peak rate pressure product (beats.min−1.mmHg.102) (297.40 ± 43.70 vs. 285.90 ± 51.50, P < 0.05 and 297.40 ± 43.70 vs. 263.30 ± 54.70; P < 0.05) and peak oxygen consumption products (MET) (6.90 ± 1.40 vs. 6.30 ± 1.20, P < 0.05; and 6.90 ± 1.40 vs. 6.10 ± 1.30, P < 0.05 respectively).
Conclusion These findings suggest that the chronic treatment DM type 2 with high insulin-independent hypoglycemic activity sulfonylureas may lead to increase of ischemic threshold in diabetic coronary patients.
516: Insulin resistance and myocardial function in patients with type 2 diabetes mellitus and ischemic heart disease
An Aleksandrov, I Bondarenko, U Majorov, I Martyanova, S Kukharenko, M Yadrichinskaya, I Dedov
Endocrinology Research Center, Moscow, Russian Federation
Background Insulin resistance is considered to be one of leading factor in pathogenesis of type 2 diabetes mellitus. It is revealed, that the level of insulin resistance is an independent risk factor for development of coronary arteries disease. The aim of this study was to determine a role of insulin resistance on formation of functional capacity in ischaemic heart in patients with type 2 diabetes mellitus.
Materials and methods There were investigated 13 patients with type 2 DM having positive results of stress-echocardiography with EST (treadmill was performed using Bruce protocol, post-exercise echocardiography images with digital technology being obtained within 90 seconds of exercise termination). All of enrolled patients had reproducible signs of ischemia on previous stress 0.9 kg/m2). ± 2.2 years, BMI 30.1 ± tests. There were 8 men and 5 women (age 59.2 1.3%. All ± 1.2 mmol/l, mean HbAlc −7.2 ± Mean fasting blood glucose was 7.7 included patients were treated with oral glucose-lowering drugs. Stress-echocardiography was performed with spirography using Weber protocol (parameters of expirated air were monitored during the test). The LV wall motion abnormalities were estimated on 16 sector model according to the guidelines of the American Society of Echocardiography. Insulin resistance (M-index) was investigated with the ≤ euglycemic clamp ≥ after standard preparation.
Results Despite absence significant relationships between insulin resistance, left ventricular architecture and ECG-test characteristics there were significant correlations between M-index and the maximal consumption of oxygen -VO2 (r = −0.652; P = 0.022) and the maximal expirated of carbonic gas - VCO2 (r = −0.731; P = 0.007) during physical exercise. Thus, insulin resistance really influences on parameters of functioning efficiency of the cardiovascular system in patients with type 2 diabetes mellitus.
534: The role of active muscle mass on cardiovascular drift
Nickos Geladas, Stelios Kounalakis, George Nassis, Maria Koskolou
Faculty of Physical Education and Sport Science, University of Athens, Greece
During prolonged steady state exercise, heart rate (HR) increases and stroke volume (SV) decreases in a progressive manner; this phenomenon is named cardiovascular drift (CVdrift) and is known to be negatively affected by hyperthermia and dehydration. Furthermore, CVdrift is worse in cycling than running regardless of subjects' thermal and water status. The purpose of this study was to explore the role of active muscle mass on CVdrift. Twelve healthy subjects (24.3 ± 3.8yrs) cycled for 50 min on two occasions: a) with two legs (2L) and b) with one leg (1 l). Oxygen uptake (VO2) in 2 l and 1 l was 60% and 30% of 2 l VO2max, respectively. VO2, cardiac output (CO)(rebreathingmethod), heart rate, rectal temperature (Tre) and mean skin temperature (Tsk) were recorded during exercise. Left leg EMG of vastus lateralis (VLiEMG) was also recorded, and plasma and blood volume changes (%PV,%BV) were calculated. CO, HR, VLiEMG, were higher (P < 0.01) in 2 l than 1 l. Throughout exercise, the rate of SV decline and the respective HR rise were greater in 2 l than 1 l. For instance, at the 50th min of exercise ΔSV was −20.8 ± 0.8 ml/beat in 2 l and −13.3 ± 1.3 ml/beat in 1 l (P < 0.05); similarly, ΔHR was + 18.5 ± 0.8 beats/min and + 10.7 ± 1.0 beats/min, in 2 l and 1 l, respectively (P < 0.01). At the end of exercise, CO tended to decrease from the steady state values in 2 l (ΔCO = −0.92 ± 0.3 l/min, P = 0.07), whereas no such change was observed in 1 l (ΔCO = −0.15 ± 0.2 l/min, P = 0.86). In 2 l condition, 60% of the variance in HR rise was explained by BV drop and VLiEMG increase. Tre and Tsk did not reach significance in the prediction model. In conclusion, cardiovascular drift is exaggerated in 2-leg compared to 1-leg exercise, despite the fact that VO2 in 1 l was half of the VO2 in 2 l. The observed differences cannot be attributed to subject's thermal status. It is suggested that muscle input plays a role on cardiovascular regulation during steady state prolonged exercise performed with large muscle mass.
566: Temporal changes in cardiopulmonary exercise test in patients with dilated and ischaemic cardiomyopathy and heart failure in B-blocker era
D Tsiapras, V Vartela, S Adamopoulos, S Kyrzopoulos, I Pagoni, V Katsiopi, G Theodorakis
2nd Cardiology Department, Onassis Cardiac Surgery Centre, Athens, Greece
Background Cardiopulmonary exercise(CPEx) is widely used for the objective evaluation of heart failure (HF) patients (pts). The introduction of b-blockers in HF has improved survival in both dilated (DCM) or ischemic cardiomyopathy (ICM) pts.
Objective The aim of the study was to investigate any differences in the changes of the CPEx parameters during follow up studies in HF pts with DCM or ICM.
Methods Seventy pts with HF, randomly referred for CPEx, more than once, during the last 3 years were included. All were under optimal treatment (according to the referring physician) which included b-blockers, ACE inhibitors. CPEx test was carried out using the Dargie protocol and maximal O2 consumption (VO2max), maximal CO2 production, maximal ventilation (VE) and the percent ratio of VO2max achieved to VO2max predicted (%VO2max pred) were estimated in all pts and tests. Group 1 included 45 DCM pts and Group 2 25 ICM pts.
Results Group 1 pts were younger (44.6 ± 16.2 vs. 59.2 ± 10.9, P < 0.001) without difference in LV ejection fraction (28 ± 8 vs. 29 ± 7%,p:ns). The time between first and last test was similar in both groups (11.4 ± 8.2 vs. 10.9 ± 7.5 months, P:ns). There was a difference between the two groups in VO2 max (19.7 ± 5.6 vs. 17.1 ± 4.2 ml/kg/ min, P < 0.001), in VE (63.5 ± 21.8 vs. 57.2 ± 16.3 l/min, P < 0.05) and in the %VO2 max pred (58.1 ± 17.8 vs. 53.5 ± 11.3%, P < 0.05). During follow-up only in 16/45 (35%) of group1 pts and in 8/25 (32%) of group 2 VO2max showed an increase (P:ns). No difference was detected between the groups in both the decrease of VO2max (−1.8 ± 3.7 vs. −1.1 ± 3.4 ml/ kg/min), VEmax (−2.24 ± 26.1 vs. −2.99 ± 12.9 l/min) and %VO2max pred (−4.5 ± 12.1 vs. −2.4 ± 9.6%) and the rate of this decrease (VO2max: −0.2 ± 0.7 vs. −0.1 ± 0.5 ml/kg/min/month), VEmax: −0.52 ± 8.1 vs. −0.15 ± 2.51 l/min/month) and %VO2max pred (−0.44 ± 2.25 vs. −0.17 ± 1.45%/month).
Conclusion Pts with HF and optimal treatment are expected to have similar changes in CPEx parameters irrespective of the aetiology (DCM or ICM).
591: Effect of exercise on postprandial lipemia and insulin resistance
JQ Zhang, LL Ji, VS. Fretwell
Univeristy of Texas at San Antonio, United States of America
As part of the syndrome X, hypertriglyceridemia (HTG) and insulin resistance are strongly associated with cardiovascular disease. We examined the effect of exercise duration on postprandial lipemia (PHTG) and insulin sensitivity. Each of the 10 male subjects (age = 34 ± 1.8, fasting triglyceride (TG) = 263 ± 27 mg/dl, VO2 max = 38 ± 1.3 ml/kg/min, body fat = 23.6 ± 1.0%, glucose = 6.4 ± 0.51 mg/dl, insulin = 22.2 ± 2.4) performed a control trial (Ctr, no exercise), and 3 exercise trails at 60% of their VO2max for 30 min (30T), 45min (45 T) and 60min (60 T). In each trial, subjects had a meal containing 100 g of fat. In exercise trials, subject jogged on a treadmill for a designated time period 12 h before the meal. Blood samples were taken at 0 h (before the meal), and 2 h, 4 h, 6 h, 8 h, and 24 h after the meal. The plasma triglyceride (TG), the area score under TG concentration curve (TG score, high score indicating a slow removal of TG), and insulin resistance (HOMA: homeostatic model assessment) were analyzed. Both 45Tand 60T had lower (P < 0.04) TG scores (area scores under TG level curve; high TG score indicates slow removal of TG; TG scores: Ctr = 1251 ± 184, 30T= 1066 ± 130, 45T = 863 ± 96, 60T= 875 ± 140) than Ctr, but there were no difference between Ctr and 30T. TG scores did not differ among exercise trials. HOMA in all three exercise trials were lower (P < 0.01) than Ctr (HOMA: Ctr = 6.83 ± 1.1, 30T = 5.28 ± 1.1, 45T = 5.18 ± 1.0, 60 T= 5.32 ± 1.1) and there were no differences among the exercise trials. The results suggest that exercise at 60% VO2max for 45 min or longer may significantly attenuate PHTG and exercise for 30 min may be sufficient to increase insulin sensitivity in men with HTG and insulin resistance.
Supported by American Heart Association-Texas Affiliate Grant