
Abstract

011: INFLUENCE OF PHYSICAL TRAINING ON CARDIAC PERFORMANCE IN PATIENTS WITH CORONARY ARTERY DISEASE
I Korzeniowska-Kubacka, M Biliñska, B Dobraszkiewicz-Wasilewska, J Potocka, R Piotrowicz
Cardiac Rehab. Dept., National Institute of Cardiology, Warsaw, Poland
Background Exercise training has been shown to improve physical capacity in patients with CAD. However, the improvement of cardiac function, either systolic or diastolic after physical training is controversial. Seismocardiography (SCG) is a noninvasive method which can be used for assessing cardiac function before and immediately after exercise stress test (ET).
Objectives The aim of the study was to examine the influence of physical training on systolic and diastolic cardiac time intervals (CTI) and correlation between exercise capacity and cardiac function in patients (pts) with CAD.
Materials and methods Forty pts after MI, with stable CAD and abnormal left ventricular function on SCG, aged 52 ± 8 years were included to the exercise training program (TP) consisted of 16 interval trainings on cycloergometer three times a week followed by 24 trainings containing gymnastic and swimming twice a week. Before and after TP pts underwent SCG and ergospirometric ET. The following variables were measured: 1) during SCG: preejection period (PEP, msec), left ventricular ejection time (LVET, msec), PEP/LVET, isovolumic relaxation time (IVRT, msec); 2) during ergospirometric ET-duration (sec), maximal workload (max W, Mets), heart rate (HR), blood pressure (BP), double product (DP), VO2max (ml/kg/min).
Results After TP the following parameters improved significantly: 1) on SCG: PEP (126 ± 15 vs 119 ± 14, P < 0.03), PEP/LVET (0.42 ± 0.08 vs 0.38 ± 0.06, P < 0.05), IVRT (62 ± 31 vs 60 ± 15, P < 0.05); 2) during ET: duration (776 ± 120 vs 879 ± 89, P < 0.001), workload (8 ± 2 vs 10 ± 2, P < 0.001) and VO2max (22 ± 4 vs 25 ± 3, P < 0.0001). There were negative correlations between PEP/LVET and VO2max (r = −0.52, P = 0.001) and between IVRT and max W (r = −0.185, P < 0.05).
Conclusions Exercise training program caused a significant improvement of physical capacity and left ventricular systolic and diastolic function in patients with CAD. The improvement of physical capacity depended on the left ventricular performance.
017: Combined endurance-resistance training versus endurance training in patients with chronic heart failure
PJM Beckers, CJM Vrints, NM Possemiers, VMA Conraads
University Hospital Antwerp, Belgium-Cardiology-Cardiac Rehabilitation, Belgium
Aim To compare the effects of combined endurance-resistance training (CT)with endurance training(ET)only on exercise capacity, ventilatory parameters and skeletal muscle strength in patients with chronic heart failure (CHF).
Method 86 patients with stable CHF (EF ≤ 40%) were randomized into a CT-group (n = 42, 58.4 y, left ventricular ejection fraction (LVEF) 27.1%) or an ET-group (n = 44, 58.8 y, LVEF 24%). Patients trained 1 hour, 3 times a week during 6 months. ET-group trained on bikes, steppers, treadmills and arm-cycles which automatically adjusted load to training heart rate (HR). CT-group started each session with 40-min resistance training of 9 muscle groups. During 4 months only 8 minutes were spend on endurance training with gradual increase until 45 minutes later. Evaluation at baseline and 6 months consisted of a cardiopulmonary exercise test, lung function test and assessment of skeletal muscle strength.
Results Both groups benefited equally in terms of maximal workload (Wattmax) and peak oxygen consumption (VO2peak). The increase of maximal steady state workload (SSW) (P = 0.004) and the decrease in heart rate/SSW (P = 0.001) was significantly greater in the CT-group.- The decrease in VO2 t12 was significantly more pronounced in the CT-group (P = 0.003). Upper limb strength increased with 38.2% in the CT-group versus 21.4% in the ET-group (P = 0.0001). Percentage of predicted value for maximal expiratory pressure (PEmax) was significantly higher (P = 0.037) in the CT-group.
Conclusions Despite the fact that maximal exercise capacity(i.e.: VO2peak and Wattmax)did not differ, patients with CHF allocated to the combined endurance-resistance training group benefited more in terms of submaximal exercise parameters (SSW) and exercise efficiency (heart rate/SSW). Moreover, following this particular training programme, changes observed in recuperation time after maximal exercise (VO2 t1/2) and maximal expiratory pressure (PEmax), both important independent prognostic determinants, were more pronounced.
041: Increased exercise capacity and quality of life in patients with chronic heart failure participating in a group-based exercise programme
BB Nilsson, A Westheim, MA Risberg
Ullevaal University Hospital, Norway
Background In patients with chronic heart failure (CHF) both exercise capacity and quality of life (QoL) are reduced in addition to a poor prognosis. Group based exercise is cost-effective and usual in rehabilitation of other patients with heart disease. The aim of this study was to examine the effects of a group-based exercise program and counseling on exercise tolerance (ET) and QoL.
Materials and methods Eighty patients mean age 70 years, range 45-85 years, with CHF in NYHA class II-IIIB, all on optimal medical treatment were randomized to an outpatient training- and special care group (T) (n = 40) or a control group (C) (n = 40). The ejection fraction was 30.2 ± 7.6 (SD) in T and 30.8 ± 9.4 in C. The exercise programme consists of a model of dynamic interval training including both endurance, strength, respiratory and streching exercise, twice a week over a 16-weeks periode. During the exercise period the patients had 4 consultations with a CHF nurse, including diatory advice, medication adherance, symptom monitoring and social support. The effects were evaluated by: bicycle ergometer test, 6-minute walk test and “Minnesota Living with Heart Failure Questionaire”.
Results At baseline ET was 75 ± 17 watt and exercise time 346 ± 111 seconds in T and 73 ± 16 watt and 336 ± 95 seconds in C. After 6 months both ET (P = 0.001), exercise time (P = 0.001) and walking distance (P < 0.001) had increased significantly in the T group without any change in the C group. For all parameters a significant difference between the groups was observed. QoL showed a significant difference between the groups at baseline, but QoL only improved significant (P < 0.05) in the T group without any change in the C group. A significant negative correlation between ET and QoL was observed in the whole group of patients (r = −0.49, P < 0.05).
Conclusion Our results support the implementation of a group-based exercise program in addition to nurse based counceling, to improve both ET and QoL in patients with CHF.
043: Do patients maintain their exercise participation and physical wellbeing subsequent to participating in Phase III cardiac rehabilitation?
Gabrielle McKee
Trinity College Dublin, Ireland
The aim of this study was to ascertain cardiac patients perceived physical wellbeing and their exercise participation before commencing a Phase III cardiac rehabilitation, to examine how much these parameters changed immediatly post Phase III cardiac rehabilitation and 6 months later.
For this study we used three sets of information, level of fitness at entry to programme as measured by exercise stress tests (bruce Protocol), Stages of Change tool (Procaska and Diclemente) and the physical dimension of the Short Form 36 (SF 36) quality of life quetionnaire. A total of 75 patients are used in this analysis with not all data available at all time points.
Exercise stress tests were carried out on the patients at the beginning of the programme. In this study 54% of the patients had exercise capacity only equivalent to sedentary lifestyle (METS ≤ 10). The stage of change were recorded in a quatitative way (1-5) in interview to indicate the behavioral status of a patient with regard to exercise. The patients came into cardiac rehabilitation with a good awareness of exercise as a risk factor or were just beginning to plan changes relating to this risk factor (mean value = 3.64 ± 1.05). There was a significant improvement in this parameter over the whole period of the study as seen using repeated measures analysis of variance. Analysis of the results of Short Form 36: Physical dimension showed that patients entering the programme had a below normal score for the physical dimension of the SF 36 quality of life tool (mean value = 67.4 ± 23.14). Over the whole time period of the study this parameter showed significant improvement.
Conclusion At the end of phase III cardiac rehabilitation the patients had significantly improved their engagement in exercise (stages of change) and also felt physically better (Short form 36: physical dimension). Detailed analysis showed that these changes were mainly maintained but not further built on 6 months post programme.
061: Functional impairment and its role as predictor of depression among elderly patients with chronic heart failure
Judit Bakai, Klára Sándori, Anita Pratscher, Nóra Elter
State Sanatorium Sopron, Hungary
Background The aim of our study was 1, to examine the prevalence of depression among hungarian elderly patients with chronic heart failure due to systolic dysfunction; 2, to find correlation between the patients' adjustment to functional impairment and its role as predictor of depression.
Methods A sample of 50 clinically stable patients from inpatients heart failure rehabilitation programme completed diagnostic interview. Symptoms of Depression were screened by the Geriatric Depression Scale and those who were selected by the Scale were diagnosed to meet the criteria either major or minor depression by the psychiatric interview. The role of functional impairments containing domains of dependency, lack of recreational activities and concerns about beeing a burden was conducted by a new 15-item questionnaire “Adjustment to Heart Failure Interview” developed by Turvey Carolyn. The patients social status were evaluated by the social worker. The participants' clinical parameters, co-morbidities were taken from their medical records.
Results Mean age was 73 (60-92) years, 23 (43%) were women. The etiology of heart failure were in 81% ischaemic. 21 (39.6%) patients were in NYHA-II, 28 (52.8%) patients in NYHA-III, 4 (7.5%) patients in NYHA IV class respectively. We found to be depressed 26 (49%) patients by the Geriatric Depression Scale, and 5 (9.43). Patients met the criteria of major depression by the psychiatric interview. We found a high correlation between the measure Adjustment to Heart Failure Interview and the Geriatric Depression Scale (r = 0.54, determination coefficient = 0.29).
Conclusion Depression is common in heart failure patients and has a significant impact on their quality of life and prognosis. Coping strategies to functional impairment may account for the development of depression. Interventions targeting to these problems could offer an opportunity to reduce the burden of CHF.
054: Improvement of exercise capacity after acute myocardial infarction in patients included in a cardiac rehabilitation program with or without an specific exercise training protocol
Núria Casanovas, Paula Cabero, Esther Marco, Alejandro Robles, Montserrat Batlló, Marta Cabanero, Helmut Schroeder, Lluís Recasens, Ferran Escalada, Jordi Bruguera
Hospital del Mar., Barcelona, Spain
Background Cardiac rehabilitation programs(CRP) after acute MI have demonstrated improvement on quality of life, exercise capacity and long term mortality and have been included as a class I recommendation in ACC/AHA guidelines. In spite of that, extension of CRP programs is still limited, especially because of its high cost. Strategies to extent they are recommendable.
Objectives Compare changes in exercise capacity after acute MI in patients included in a CRP depending on whether they received supervised exercise training or not.
Material and methods All patients admitted for acute MI during 2003-2004 were evaluated to participate in a CRP. Patients with high risk cardiopathies, severe comorbidities or older than 75 years old were excluded. CRP was developed by a multidisciplinary team and included an educational program about ischemic heart disease, nutritional and physical activity counselling and help for smoking cessation.
Results 62 patients were included in the study and were randomised into two groups: monitored exercise training one hour daily for 5 weeks (group 1: 32 patients) and standard advise (group 2: 30 patients). Only 24 patients of group 1 (75%) completed the training program. All patients had a standard Bruce protocol exercise stress testing (EST) at inclusion and at 6 and 12 months of follow-up. Both groups improved exercise capacity at 6 months in a similar way: mean increase of EST time 0.73 vs 0.8 min (ns) and 0.6 versus 0.75 METS (ns) with an only slight reduction at 12 months. There were no differences in death (none of the patients) or readmission for cardiac causes (18.75% vs 16%, ns).
Conclusions An educational program that includes physical activity counselling can be as effective as an expensive monitored exercise training protocol to improve exercise capacity after acute MI. This apparent lack of benefit of monitored exercise can be due to the low compliance rate of patients included (75% and probably less in real life).
071: Patients' causal beliefs predict quality of life and psychological adjustment 13 months after diagnosis of acute coronary syndrome
L Perkins-Porras, DL Whitehead, PC Strike, A Steptoe
University College London, United Kingdom
Patients' beliefs about the causes of their heart problems may predict later psychological adjustment and quality of life. We investigated this hypothesis by conducting interviews and questionnaire assessments with 269 patients hospitalised for Acute Coronary Syndromes. Patients' causal beliefs and mood states were assessed using a causal beliefs questionnaire, the Hospital Anxiety and Depression Scale and Beck Depression Inventory during hospital admission and 13 months after discharge. The Medical Outcomes Short Form questionnaire was used to measure quality of life.
Factor analysis revealed that patients' beliefs about causes could be categorized into 3 domains; mental state, personal behaviour and heredity. The mental state factor included beliefs that heart problems were caused by stress, overwork, tiredness etc. Linear regression showed that higher mental state ratings predicted poorer quality of life after 13 months, and in particular, higher ratings on the general mental health scale (B = −5.1, C.I.-10.14 to −0.48, P = 0.03), adjusted for age, gender, baseline anxiety and cardiovascular disease risk score. Attributions to mental state also predicted greater anxiety after 13 months (B = 1.20, C.I. 0.34 to 2.05, P = 0.006), adjusted for age, gender, cardiovascular disease risk score, and baseline mood states. There were no associations between quality of life and beliefs in personal behaviour or heredity as causes.
Patients' attributions of heart disease to their mental state rather than to other causes may lead to self-blame and produce a negative outlook. This may then lead to difficulties with work or other daily activities, and hence social and role disabilities. Psychological interventions aimed at changing patients' causal beliefs, focussing on lifestyle behaviour, modifiable risk factors, and correcting maladaptive attributions may lead to better emotional adjustment and quality of life.
072: Improving cardiac rehabilitation in Sweden: the five hearts audit system
Joep Perk, Pelle Johansson
The Swedish Heart- and Lung Patient's Association (RHL), Sweden
Background In previous decades access to cardiac rehabilitation (CR) varied widely in Sweden in spite of national guidelines stating that CR should be available for all elegible patients. Since 1996 the Swedish Heart- and Lung Patient's Association (RHL) has been engaged in cooperation with CR specialists in a nationwide staff training and research effort: teams from all hospitals participated in post-graduate training courses and several research projects have been initiated.
Four surveys In assuring the effect and the quality of these efforts hospitals have been audited using a grading system of one to five hearts: one heart indicating an unsatisfactory level, three hearts acceptable and five hearts outstanding CR quality. Grading was based on existing national guidelines and partly on patient preferences. The surveys were performed in 1996, 1999, 2002 and 2005 by questionnaires, visits and repeated contact between a RHL county-representative and the local hospital. After the latest survey RHL created a hospital-specific website with the actual and updated content of the local programme for information to patients and staff.
Results In 1996 a majority of the hospitals showed low quality cardiac rehabilitation, in 2005 all hospitals scored acceptable or higher. Even if this is a major breakthrough in CR there remains a need for better access to nutrional counselling and stress management, which is offered to less than half of the elegible Swedish patients.
Conclusion Five Heart Project appears to have contributed to a nationwide improvement of cardiac rehabilitation but continued efforts are needed to strengthen the multidisciplinary components.
084: Predicting long term confidence in maintaining diet and exercise lifestyle behaviour in coronary heart disease patients-a three years follow-up patient survey
M Lau-Walker
Imperial College, London, United Kingdom
Objectives To assess the measures of illness representation components in predicting measures of self-efficacy in patients with coronary heart disease.
Design A longitudinal prospective questionnaire survey exploring 300 cardiac patients illness beliefs in the south of England.
Method A cohort sample of 300 patients with coronary heart disease who were admitted to hospital were given the questionnaire measuring their illness perception (illness representation components: Identity, Consequences, Timeline and Control/Cure and Outcome expectation for diet and exercise); self-efficacy (general, diet & exercise self-efficacy measures) and demographic, illness characteristic and attendance to cardiac rehabilitation programme. The patients were asked to complete the questionnaire three times, firstly in hospital following a cardiac diagnosis before discharge and then at nine months and three years later, when participants were expected to be functioning independently of any rehabilitation programme.
Results Demographic and illness characteristics have a more significant relationship with illness representation components than with specific self-efficacy. Patients reported significantly ‘lower symptoms’ and ‘less consequence’ of their illness nine months later; and slightly higher ‘exercise self-efficacy’ three years later. After statistically control the effects of demographic, illness characteristic and attendance to a rehabilitation programme, ‘gender’ and ‘control/cure (T1)’ predict patients' diet self-efficacy and ‘route of admission’, ‘control/cure’ and ‘symptom (T2)’ predict patients' exercise self-efficacy three year later.
Conclusion A significant relationship exists between certain illness representation components and self-efficacy. The study provides evidence to support the development of an effective individualised care approach in facilitating patient long-term diet and exercise health behaviour.
086: Effects of music listening on anxiety and mood profile in cardiac patients undergoing exercise testing
A Dritsas, M Pothoulaki, RAR MacDonald, P Flowers, DV Cokkinos
Cardiology Dept, Onassis Cardiac Surgery Center, Greece
Background The aim of the present study was to examine the effects of music listening on anxiety and mood in patients undergoing exercise testing.
Methods Sixty pts (age 59 ± 10, range 33-76 yrs), 32 (53%) with coronary artery disease who underwent a treadmill exercise test on the Bruce protocol participated in the present study Pts were randomly assigned to a control (CG) (n = 30) and an experimental group (EG) (n = 30). Pts in both groups were asked to complete the State-Trait Anxiety Inventory (STAI) and the Profile of Mood States (POMS) questionnaire prior to intervention (phase A). During the exercise test EG listened to a music CD of their preference and CG did not receive music listening. After the end of the exercise test (phase B) pts in both groups completed the State form of the STAI and POMS and EG pts were asked to complete an evaluation questionnaire on the music intervention they received.
Results Mean scores for the items “active” and “energetic” in POMS differed significantly in phase B across groups (F = 8.231, P < 0.01 and F = 4.279, P < 0.05 respectively) with the EG being more “active” and “energetic” compared to CG. A negative result for myocardial ischemia was more frequently detected in EG compared to CG (P < 0.01). Significant within-group differences favoring music listening were revealed in EG for the following POMS factors: tension-anxiety (P < 0.001), depression-dejection (P < 0.05) and anger-hostility (P < 0.05). In addition, there was a significant negative correlation between state anxiety scores in phase B and duration of the exercise test (r = −0.354, P < 0.01).
Conclusions Music exhibits a positive effect on mood changes and it can motivate pts undergoing exercise testing and also influence the diagnostic outcome of the test. Music may act as a pleasant distracter during exercise possibly by diverting patients' attention from the medical procedure and relieve tension.
087: Maximal inspiratory pressure as a determinant of exercise capacity in patients with chronic heart failure
ID Laoutaris, A Dritsas, MD Brown, A Manginas, O Ionescou, M Kallistratos, PA Alivizatos, DV Cokkinos
Onassis Cardiac Surgery Center, Greece
Background Various studies report a decrease in maximal inspiratory pressure (MIP) in patients with chronic heart failure (CHF). We sought to investigate weather MIP is decreased in CHF and weather it can determine exercise capacity.
Methods We investigated 53 male patients (pts) with dilated (n = 30) and ischaemic (n = 23) cardiomyopathy, NYHA II/III, age, 58.3 ± 10.4 (mean ± SD), weight (wt), 86.7 ± 17.5 kg with an LVEF of 26.4 ± 7.9%. Patients performed a cardiopulmonary exercise test and the 6-min walk test. MIP was assessed at the first sec of inspiration at residual volume using an electronic pressure manometer with running-purpose software while resting lung volumes were evaluated by spirometry. MIP measured was compared to normal predicted value according to the Baltimore Longitudinal Study equation for men: MIP n = 126-1.028 × age + 0.343 × wt (kg).
Results MIP was significantly decreased compared to normal predicted value (83.9 ± 23.8 vs. 95.8 ± 14.7 cmH2O, P <0.001). MIP was significantly correlated with age (r = −0.4, P < 0.005), wt (r = 0.4, P < 0.001), NYHA classification (r = −0.5, P < 0.001), FVC (r = 0.4, P < 0.005), walking distance (r = 0.5, P < 0.001) and peak VO2 (r = 0.6, P < 0.001). Linear regression analysis identified a significant association between MIP and peak VO2 (P < 0.001) while calculated regression equation between MIP and peak VO2 adjusted for age and wt, equals: VO2 = 3.57 + 8.769 × 10−2 × MIP + 4.932 × 10−2 × age + 2.63 × 10−2 × wt (kg).
Conclusions MIP was found to be decreased in pts with CHF. A reference equation for determining peak VO2 in male pts with CHF according to MIP, age and weight is reported.
088: Influence of respiratory muscle training on exercise capacity in heart transplantation and chronic heart failure patients
ID Laoutaris, A Dritsas, MD Brown, A Manginas, S Adamopoulos, M Koulopoulou, M Kallistratos, P Sfirakis, PA Alivizatos, DV Cokkinos
Onassis Cardiac Surgery Center, Greece
Background We sought to investigate possible benefits of inspiratory muscle training (IMT) on exercise capacity and dyspnea in patients after heart transplantation (HTx) in comparison to chronic heart failure (CHF).
Methods Using an age and sex-matched controlled study, we studied a HTx group (n = 9, age, 44 ± 12 yrs), at least one year after the HTx, with a LVEF of 58 ± 6%, and a CHF group (n = 9, age, 47 ± 6 yrs), NYHA II and an LVEF 31 ± 9%. All patients were trained at 60% of sustained maximal inspiratory pressure (SPimax), to respiratory fatigue, 3 times weekly for 10 weeks. Pre and post-IMT, pulmonary function was assessed by spirometry, exercise capacity by treadmill testing and the 6-min walk test while dyspnea by the Borg scale at the end of the walk.
Results Post-IMT, the HTx group increased inspiratory muscle strength (Pimax, 123.9 ± 19.6 vs. 102.1 ± 16.5 cmH20, P = 0.002), endurance (SPimax, 583 ± 176 vs. 405 ± 149 cmH20/sec/1000, P = 0.018), FVC (101.6 ± 11.8 vs. 98.8 ± 8.3 Lt, P = 0.028), VO2peak (22.7 ± 2.5 vs. 20.1 ± 4.5 ml/kg/min, P = 0.048) and walking distance (560 ± 45.9 vs. 476.9 ± 51.4 m, P = 0.003). Dyspnea did not significantly change (P = NS). The CHF group also increased Pimax (121.7 ± 36.6 vs. 87.9 ± 27.6 cmH20, P = 0.002), SPimax (655 ± 259 vs. 417 ± 210 cmH20/sec/1000, P = 0.001) and FVC (107.4 ± 7.4 vs. 102.6 ± 5.1 Lt, P = 0.036). VO2Peak (21.7 ± 4.4 vs. 17.8 ± 2.4 ml/kg/ min, P = 0.01), walking distance (458.9 ± 71.1 vs. 415.9 ± 56.9 m, P = 0.001) and dyspnea (8.2 ± 1.3 vs. 9.9 ± 1.4, P = 0.000) were dramatically improved in this group. However, comparison between groups did not show a statistically significant difference in peak VO2 or walking distance change, except for dyspnea (P = 0.003).
Conclusion IMT improves exercise capacity and indices of pulmonary function in both HTx and CHF patients. A marked decrease in dyspnea, following IMT, was noted only in CHF patients.
089: The impact of sexual therapy on patients after cardiac events participating in multi-disciplinary cardiac rehabilitation program
J Klein, R Klein, E Bar-on, R Bebenishty
Shaare Zedek Medical Center, Jerusalem, Israel
Background The prevalence of sexual dysfunction in patients (pts) after acute cardiac events is high. Sexual counseling (SC) is a recommended component of Cardiac Rehabilitation (CR). Nevertheless there are only few studies evaluating the impact of SC or Sexual Therapy (ST) in CR pts. This study assesses the impact of a ST module on male pts participating in phase 2 CR after a cardiac event.
Methods We randomly assigned 92 consecutive male pts(age < 70, mean age 58), on their admission to phase-2 CR after MI/ACS and/or CABG, into a “ST group” (n = 47), and a “control group” (n = 45). We used 2 co-therapists that met with the patient and spouse for 5 hours in 3 sessions, in addition to CR. ST included: patient education, cognitive restructuring, emotional support, guided imagery, and medication (Viagra). Pts in the control group participated in usual CR program without ST. Patients in both groups were assessed using written questionnaires at 3 different times: before, at 1 month, and 3 months after ST.
Results Baseline socio-demographic, cardiac and sexual characteristics of both groups were similar. One third of pts did not resume their sexual activity within 2 months from event till starting CR. The quality of sexual activity in those who resumed activity was equally low. Among those who did not resume sexual activity-significantly more pts in the ST group resumed sexual activity within 1 month of CR, compared to control group (87% Vs 50%, P < 0.05). Compared to the control group, pts in ST significantly improved the quality of sexual function as follows: libido P < 0.04, confidence in ability to attain erection P < 0.01, satisfaction with sexual relationship with partner, and frequency of attaining erection P < 0.02, and enjoyment of sex P < 0.04.
Conclusions ST is significantly effective in improving both the frequency and the quality of sexual activity in pts post-cardiac event beyond the usual CR. ST services should be an integral part of CR.
096: Effects of different types of exercise training followed by detraining, on endothelium-dependent dilation in patients with recent myocardial infarction
Margherita Vona, Alessandro Lupi, Lorella Marini, Mikael Rabaeus, Pietro Bosso
Cardiac Rehabilitation Aosta Italy, Cardiac Rehabilitation Genolier, Switzerland
Background Exercise training is associated with improvement of the endothelial function (EnF), but little is known about the relative effect of different types of exercise training (ET).
Objectives To prospectively evaluate, the effect of different types of ET on EnF in 209 patients (pts)with a first recent myocardial infarction (MI)(< 4 weeks).
Methods EnF evaluation was done before and after 4 weeks of ET, and after detraining (DT), measuring brachial artery vasomotor reactivity using flow-mediated dilation (FMD%) and sublingual nitroglycerin (TNT); we measured also the Von Willebrand factor (VW) at baseline and after ET Pts were randomized in 4 groups: a) Group 1 (G1): controlled aerobic ET at 75% of the exercise test maximal heart rate (n = 52); b) Group 2 (G2): controlled resistance training at 60% of pretraining maximum voluntary contraction, (n = 54); c) Group 3 (G3) resistance + aerobic training (n = 53); d) Group 4 (G4): no training, (n = 50) ET consisted of four 1-hour sessions each week during four weeks, followed by 4 weeks of DT Pts were submitted to an exercise test before and after ET, and after DT.
Results At baseline the FMD was 3.9 ± 2.5% in G1, 4.3 ± 3.5% in G2, 4.8 ± 2% in G3 and 4.4 ± 3 in G4(P = ns) After ET the FMD increased to 10.5 ± 6% in G1, 10.1 ± 3% in G2, 11.9 ± 4% in G3 (P < 0.01 vs baseline for all groups), but remained unchanged in G4 (5.1 ± 3%, P < 0.01 vs G1, G2, G3). The endothelium-independent vasodilation was unchanged after ET and DT in the 4 groups throughout the study. In trained pts the VW after ET decreased by 16% (P < 0.01) similarly in G1, G2 and G3, but remained unchanged in G4. As expected, DT returned the FMD to baseline levels, (P < 0.01 vs post-training).
Conclusion In pts with recent MI ET is associated with improved endothelial function evaluated by an increase in endothelium-dependent vasodilatation and by a decrease in VW factor. This improvement was independent of the type of training and it disappeared after one month of DT.
113: Tilt training: a new challenge in the rehabilitation of patients with malignant syncope
T Reybrouck, H Heidbüchel, R Willems, H Ector
University Hospital Gasthuisberg, 3000 Leuven, Belgium
Tilt training has been considered as a useful therapy in the treatment of neurally mediated syncope (S).
The aim of the study was to assess whether patients with the cardioinhibitory type of tilt response with prolonged asystolic periods (2B) could also be successfully treated with tilt training therapy. We studied 222 patients: 61 patients with type 2B syncope were compared to other types of syncope (n = 161). The patients were tilted daily (60° inclination) until syncope or until a maximum of 45 min. Syncope was diagnosed as type 1 (mixed type) in 74 cases, 2A (cardioinhibitory without asystole) in 6, 2B (cardioinhibitory with asystole) in 61 and type 3 (vasodepressor) in 81.
The duration of asystole averaged 12.8 ± 10 s (min 3, max 60, median 9). The diagnostic tilt test was positive after 14.7 ± 10.2 min in 2B which was significantly shorter (P = 0.002) than the other types: 19.5 ± 11.4 min in type 1, 24.8 ± 13.6 min in 2A, and 21.6 ± 11.1 min in type 3. After repeated tilt testing, all patients with type 2B syncope became asymptomatic. The first negative tilt training session was reached after 2.7 ± 1 sessions for 2B and was not significantly different from the other types: 2.8 ± 1.3 sessions for type 1, 2.8 ± 1.2 type for 2B and 3.1 ± 1.4 for type 3 (P > 0.25 between groups). In patients with type 2B the first negative tilt test was reached at session 2 in 38 patients (62%), at 3 in 11 (18%), at 4 in 7 (11%), at 5 in 3 at 6 in 1 and at session 7 in 1 patient. No significant difference was found between different types of syncope.
Conclusion Patients with the cardioinhibitory type of syncope and long asystolic periods could successfully be treated with tilt training and did not require more tilt training sessions to become negative compared to other types of syncope. In more than half of the patients already the second consecutive tilt test became negative.
115: The influence of cardiac rehabilitation on HSCRP level in patients after myocardial infarction treated by percutaneous coronary interventions with or without stenting
A Zielinska-Meus, K Oleszczyk, T Zielinska, E Kosiewicz-Nosowicz, A Kusmierczyk-Pielok, T Sykosz, K Mielich, Z Karalus
Uppersilesian Rehabilitation Center Repty, Poland
Background Physical activity may play the important role in lowering risk factors by its influence on inflammation. The aim of this study was to assess the effect of cardiac rehabilitation on level of high sensitive C-reactive protein (hsCRP) in patients after acute myocardial infarction (AMI) treated by percutaneous coronary interventions (PCI) participating in a three week cardiac rehabilitation program.
Methods 196 consecutive patients in mean age 58 ± 10.5 (152 men, and 52 women, enrolling in rehabilitation program 15-20 days after AMI treated by invasive method were analyzed. The patients were stratified on 3 groups (gr.) according to exercise tolerance assessed during exercise testing and clinical state. Group 1: 54 patients (mean age 50.9 ± 9.9) with good exercise tolerance-above 7 METS and low risk of coronary events. Group 2: 92 patients (mean age 56.6 ± 10.5) with medium exercise tolerance 5-7 METs and medium risk coronary events. Group 3: 50 patients (mean age 62.4 ± 9.6) with low exercise tolerance below 5 METs or medium to high risk coronary events. Statistics: Wilcoxon's paired test and Pearson's test correlation were used.
Results Gr. METs-before/METs-after: 1. 8.84 ± 2.17/9.96 ± 2.19∗;2. 6.48 ± 1.97/8.1 ± 2.42∗; 3. 4.4 ± 1.80/5.39 ± 2.13∗. Gr. hsCRP-before/hsCRP-after: 1. 27.98 ± 24.53/3.07 ± 2.99∗; 2. 29.53 ± 30.03/7.65 ± 14.10∗; 3. 33.23 ± 27.15/7.8 ± 14.93∗; ∗P < 0.01. Gr. correlation gradients METs vs hsCRP: 1. r = 0.44, P = 0.001; 2. r = 0.41, P = 0.001; 3. r = 0.52, P = 0.001.
Conclusions Cardiac rehabilitation in patients after MI treated by PCI decreases the level of hsCRP and improves exercise tolerance in all groups. Correlation between the gradient of METs and gradient of hsCRP was observed in all groups.
116: Combined aerobic and resistance exercise training in high-risk cardiac patients
J Jancik, P Dobsak, M Kohzuki, M Nagasaka, R Panovsky
Masaryk University, Czech Republic; Tohoku University of Sendai, Japan
Objective This study was designed to assess safety and evaluate the effects of 12-week lasting combined endurance/resistence training on the performance and aerobic capacity in patients with systolic dysfunction of the left ventricle (LVEF < 40%) and with residual ischemia (presence of at least one coronary stenosis of more than 50% of the lumen diameter).
Patients and methods 20 patients (18 men and 2 women, mean age 64 ± 9 years, mean body weight 85 ± 11 kg, mean height 174 ± 8 cm, class NYHA II—III, mean EF 33 ± 5%) were enrolled in a 12-weeks nonrandomized training program. The training session was performed 3 × a week and consisted of a 10 min warm-up phase followed by 20 min of cycling, 20 min of resistence exercise and 10 min cool-down period. Symptom-limited spiroergometry was provided before and after the rehabilitation period; the first was applied for the evaluation of anaerobic threshold (AT) to decide on the bicycle training intensity. Load intensity for the resistance training phase on the weight-lifting machine was determined by the method of 1-RM (30-60%).
Results After the training increased peak exercise oxygen uptake (VO2peak) from 17.1 ± 1.7 to 19.3 ± 3.0 ml.kg-1.min-1 (P < 0.01), VO2peak on the level of AT increased from 11.1 ± 1.8 to 12.1 ± 1,1 ml.kg-1.min-1 (P < 0.05). Symptom-limited workload increased from 99 ± 19 W to 116 ± 25W (P < 0.01) There were no exercise-related adverse events during more than 750 patient-hours of exercise training.
Conclusion Combined endurance/resistence exercise training was safe and effective in this high-risk group of patients.
Supported by the grant of TUBERO in Sendai.
117: Effective self-management cardiac rehabilitation: the heart manual
Hafrun Taylor, Louise Taylor, Mary Ramsay; The Heart Manual Programme
NHS Lothian Primary and Community Division, Edinburgh, Scotland
The Heart Manual is a rehabilitation programme designed for patients recovering from acute myocardial infarction. It has been shown to be clinically effective in repeated studies and is the United Kingdom's leading home based cardiac rehabilitation programme, and has been adopted internationally in parts of Canada, Italy and Holland. It is suitable as a stand-alone rehabilitation programme or can be integrated with existing hospital/primary care based programmes. It is flexible in its delivery to accommodate resources. An integral part of the programme is a two-day training package for health professionals. The course consists of the psychological implication of an infarct for the patient and family and the practical side of delivering rehabilitation. In the year 2005, 15,000 patients received the Heart Manual. The Heart Manual was evaluated in a major trial completed in the 1990s. Since then consistent evaluations (published/non-published) re-enforced the original results which showed: reduction in re-admissions, improved psychological adjustment, less contact with general practitioners; reduction in anxiety and depression at one year. A number of concurrent projects by the Heart Manual team include: an over-80 s effectiveness study which highlighted the positive effects of the Manual on this population group; an angina needs assessment study which defined a need for clarification of the patient pathway; recently evaluated Revascularisation (CABG/PTCA) Manual where the interim results showed equally improved outcomes at six months (Jolly et al 2005).
121: Does vocationally oriented cardiac rehabilitation increase return to work?-a randomised controlled trial
Joerg Kittel, Marthin Karoff
Institute for Research in Rehabilitation, Norderney, Germany
Background Cardiac rehabilitation supports patients to regain good physical work capacity. However, the effects on return to gainful occupation are limited. Based on multivariate analysis, the patients' motivation was proven to be the most important predictor for return to work (Perk J, Alexanderson K. Sick leave due to coronary artery disease or stroke. Scand J Public Health 2004; 32: Suppl. 63). Therefore vocational orientation should take place in the cardiac rehabilitation in order to improve the return to work. This should include a differentiated determination of the level of strain and stress in the working place, individual motivational factors and the evaluation of the functional capacity. The goal of the present study is to examine the effects of a vocationally oriented rehabilitation integrating both the system of Functional Capacity Evaluation (FCE) as well as psychosocial intervention.
Methods 300 cardiac patients with vocational problems were randomized into either a vocational intervention group (IG) or a control group (CG) with “usual care”. Counterindications for participation in the study were the condition after an acute heart operation as well as exercise capacity below 75 watts and restricted left ventricle function. All patients had been on sick leave before rehabilitation.
Results 300 persons could be recruited for the study. 231 patients (91%) were male. The average age was 47.3 + 8.1 years. 57 patients (19%) were unemployed before rehabilitation. For the 12-month catamnesis data of 197 persons are available. One year after rehabilitation 78.0% of the patients in the IG returned to work related to 60.2% in the CG (P < 0.05). 38.3% of the patients treated with usual care had been on sick leave over six months. In the IG only 16.8% have these long times of sick leave (P < 0.01).
Conclusions The results indicate a significant effect of vocationally related rehabilitation on return to work.
124: Comparative study of different training methods on exercise capacity and peripheral muscle dysfunction in severe chronic heart failure patients
P Feiereisen, M Vaillant, Y Lasar, C Delagardelle
Centre Hospitalier de Luxembourg
Background Endurance training (ET), combined endurance and strength training (CT) as well as exclusive strength training (ST) have independently shown to improve exercise capacity and to correct peripheral muscle dysfunctions in chronic heart failure (CHF) patients. The goal of our study was to compare these methods in order to see if they were equally efficient in inducing those positive training effects.
Methods 39 patients with severe CHF; mean LVEF(%): 23.8 ± 5.5, mean VO2peak (ml/min/kg): 14.5 ± 2.5, were randomly assigned to 3 training groups: 13 patients did ET, 12 did CT and 14 did ST. All groups trained three times per week during 40 sessions for the same amount of time. Before and after training, exercise capacity (VO2peak) was measured by cardiopulmonary stress testing, knee extensor muscle strength (peak torque (PT)) and endurance (total work (TW)) were evaluated by isokinetic dynamometry and thigh muscle volume was measured by CT-scan.
Results All parameters (VO2peak, muscle volume, PT and TW) significantly increased after training in each of the three training groups, with the exception of PT in the CT group. Statistical analysis for changes between the groups could not detect the superiority of any method in improvments of peripheral muscle strength or endurance. No difference between the groups was found for increases in thigh muscle volume. Concerning VO2peak, ST and ET were statistically more efficient than CT, even if all three modalities induced increases in VO2peak.
Conclusion No matter which one of the three training methods (ET, CT and ST) is applied, positive training effects on exercise capacity and peripheral muscle dysfunctions are obtained and seem equally important.
130: Quantification of mitral regurgitation in patients with severe congestive heart failure undergoing an intensive training program: reassuring news
C Delagardelle, F Robert, A Debugne, M Vaillant, P Feiereisen, F Lebrun
Centre Hospitalier de Luxembourg, Cardiology department, Luxembourg
Background Nearly all congestive heart failure (CHF) patients present with mitral regurgitation (MR). So far the influence of training on MR has not been intensively studied.
The purpose of our study was to evaluate the degree of baseline MR in a stable CHF patients group and to study the influence of an intensive training intervention on MR.
Patients and methods Our study included 60 patients, representing typical CHF patients seen in daily practice. Baseline patient data: Mean age 59.3 years, NYHA 2.6, left ventricular ejection fraction (LVEF) 23.9%, VO2 peak 14.7 ml/kg/min. They were enrolled in a randomized controlled study comparing different training methods. They underwent a radionuclide ventriculography, to measure LVEF, and an echocardiography before and after a training intervention of 40 sessions, 3 times weekly, during 3-1 months. The following echocardiographic parameters were measured: Left ventricular enddiastolic diameter (LVED) and color flow doppler of MR. In case of at least moderate MR quantification using tne proximal isovelocity surface area method (PISA) was performed. Mild MR, in which this method was not applicable, were arbitrarely quantified as a regurgitation volume of 5 ml.
Results 1) Mean LVED was at baseline 66.9 mm, after 3 months 66.0 mm (P = ns); 2) In the training group mean LVEF was at baseline 23.9% and after 3 months 30.3% (P = 0.0001), in the control group 24.8% and 27.3% (P = ns); 3) At baseline 63% (38/60) had a mild (5 ml) and 37% (22/60) a moderate MR (mean 16.7 ml); 4) For the whole group of 60 patients mean MR volume was at baseline 9.1 ml and 9.9 ml after 3 months (P = ns); 5) The mean value of the moderate MRs, which was 16.7 ml at baseline remained 16.8 ml after 3 months (P = ns).
Conclusions 1) LVEF increased significantly after 3 months of intensive training; 2) 2/3 of the patients (63%) present at baseline with a mild and 1/3 (37%) with a moderate MR; 3) Quantitatively measured MR was not significantly influenced by the training intervention.
134: Can low risk cardiac rehabilitation patients be fast-tracked into a long term maintenance community based exercise programme?
HJ Arnold, NJ Samani, SJ Singh
University Hospitals of Leicester, UK
Background On hospital discharge patients eligible for cardiac rehabilitation are conventionally offered out-patient hospital based programmes. After graduation they are encouraged to continue long term maintenance in the community. The aim of the research was to determine if low risk patients can be fast tracked straight into a community maintenance programme.
Method 97 patients were randomised using a minimisation technique into either an outpatient hospital rehabilitation group run by a specialised multidisciplinary team, or fast-tracked into a community group run by a British Association of Cardiac Rehabilitation fitness instructor. For the purpose of the study both programmes consisted of 1 hour of supervised exercise per week, for 6 weeks. Patients in the hospital group had the option of attending 6 risk factor/life style modification education sessions. Those attending the fast track group were provided with written information. Functional capacity using the incremental shuttle walking test (ISWT) along with hospital anxiety and depression scores were analysed.
Results 51 patients (47 male) mean (SD) age of 59.27 (9.53) years took the conventional approach and 46 patients (44 male) mean (SD) age of 59.72 (8.94) years took the fast-track route. Both groups demonstrated a statistically significant increase in ISWT distance post rehabilitation, mean increase 52.55 meters, 95%CI 31.95 to 73.15, (P < 0.001) and 59.35 meters 95% CI 38.10 to 80.59, (P < 0.001) for conventional and fast track groups respectively. Post rehabilitation the conventional group showed a significant reduction in depression (P = 0.032) and the fast-track group demonstrated a significant reduction in anxiety (P = 0.049).
Conclusion The data demonstrates that both groups secure a statistically significant improvement in functional capacity. In the short term patients randomised to the ‘fast track’ programme do as well as those patients randomised to the conventional hospital based group.
143: Effect of long-term cardiological rehabilitation on HDL-cholesterol level in patients with previous mi treated with simvastatin.correlation between training intensity and HDL changes
D Kalka, J Bolanowski, M Sobieszczanska, W Marciniak, A Bak, E Metner, J Janczak, J Adamus
Department of Cardiological Rehabilitation “Medar”, Wroclaw, Poland
A goal of the study was assessment of the effect of long-term cardiological rehabilitation on HDL-cholesterol serum level and analysis of the correlation between training intensity and HDL changes. The study population comprised 67 patiens with CAD (33 females, 34 males) aged 54-72 yrs (mean: 59.83 ± 0.96 yrs). The both groups were comparable concerning treatment (beta-blockers, ACEI, statins), clinical presentation, echocardiography parameters (EF, LVEDD) and BMI values. The patients were referred to rehabilitation after the invasive treatment: CABG-27 patients and PCI-39 patients. The control group constituted 32 patients with previous MI, not subjected to rehabilitation. Rehabilitation comprised a 45-min cycloergometer training with the loads increasing with time, broken by the 2-min rest with low load 3 times per week, with generally improving exercises 2 times per week. Comparison between the two analyzed groups concerned the following parameters: (1) HDL-cholesterol concentration for the patient and the control groups before the rehabilitation: 51.09% mg vs 51.63% mg (NS); (2) delta value of the HDL level for the patients and the controls after rehabilitation: 2.26%mg vs −0.84% mg (P < 0.01). Furthermore, correlation between HDL level delta, and final training work and training work delta was analyzed. The Pearson's correlation coefficients was −0.012 for the final training work and −0.035 for the training work delta. The two coefficients did not show a statistical significance. In the result of the 6-month rehabilitation performed in the patients with previous MI, the statistically significant increase of the HDL concentration occurred, which did not correlate either with final training work or with training work delta. Thus, the found HDL-cholesterol rise did not depend on the training load applied.
145: Only women had long-term weight loss in cardiac rehabilitation, men need cooking exercise for achieving long-term weight loss
Helena Hämäläinen, Arja Virtanen, Monica Röberg
Social Insurance Institution, Research Department, Turku, Finland
Background Obesity is a common problem among cardiac patients, and hence, cardiac rehabilitation should include specifically designed dietary counselling. Our aim was to study if patients taking part in rehabilitation at four rehabilitation centres are able to lose weight and if the weight loss persists up to the one-year follow-up.
Patients and methods The patients (n = 134, 107 M, 27 F, age range 39-64 yrs) took part in two weeks' in-patient rehabilitation, in follow-up examinations at the centre after 4 months and in a postal follow-up questionnaire survey 12 months after the first in-patient period. Rehabilitation included exercise training, discussions with a psychologist and a social worker, and dietary counselling usually in groups but also individually. All the four rehabilitation centres had slightly different methods in their dietary counselling. At baseline, women were slightly heavier than men (BMI 29.5 ± 5.3 vs. 28.7 ± 4.0 kg/m2, NS).
Results The change in weight in men and in women by the first follow-up was −0.1 ± 3.2 kg vs. —1.5 ± 1.7 kg and by 12 months + 0.4 ± 4.3 vs. −2.0 ± 3.7 kg (P = 0.019). Differences were observed between the four rehabilitation centres. Long-term weight decline was seen in men only in one centre which used group counselling but included cooking sessions in the programme. In small groups, the patients prepared the meal for the whole group and at the same time discussed issues concerning healthy cooking. This practical training motivated the patients best to make changes in their dietary habits.
Conclusions Women were more motivated by a need to change dietary habits for the purpose of losing weight than men. Practical “hands-on” counselling is useful in motivating men to do beneficial changes in their diet.
151: Assessment of correlation between cardiological training intensity and resting pulse changes in patients with chronic cad treated with beta-blockers
D Kalka, J Bolanowski, M Sobieszczanska, W Marciniak, A Bak, A Chorebala, J Adamus
Department of Cardiological Rehabilitation “Medar”, Wroclaw, Poland
One of the positive effects of long-term exercises on cardiovascular system is resting pulse rate lowering resulting mainly from sympathetic tone decrease. A goal of the study was assessment of 6-month ambulatory cardiological rehabilitation influence on resting pulse rate in the patients with CAD treated with beta-blockers. Analysis of correlation between training intensity and changes of resting pulse rate was performed. The study comprised 103 patients (69 men and 34 women), aged 46-79 yrs (mean: 61.2 ± 0.8 yrs) with chronic CAD. The patients were referred to the rehabilitation after invasive treatment or ACS episode. The all patients were assessed as clinically stable. The means were following, EF: 57.0 ± 0.8%, LVEDD: 52.0 ± 1.0 mm, and BMI: 28.3 ± 04. The all patients were taking beta-blockers at least for six months, and the dosages were not modified during the rehabilitation. Rehabilitation comprised 45-min cycloergometer training with 4-min interval loads increasing with time and broken by 2-min rest with 10 Watt load (3 times/week) and generally improving exercises (2 times/week). The statistical analyses concerned the mean and the standard error mean of the pulse rate, measured after 5-min rest before the exercise onset, taken from the first and the final three training sessions. The following parameters were analyzed: (1) resting pulse rate at the beginning and at the end of the rehabilitation cycle: 72.18 ± 2.77/min vs 66.93 ± 3.53 (P < 0.01); (2) correlation between delta of resting pulse rate and final training work and training work delta; Pearson's coefficient for final training work was −0.079, and for training work delta was −0.097; the both coefficients were insignificant. Conclusion: In the result of the 6-month cardiological rehabilitation the statistically significant reduction of resting pulse rate was observed. However, there was no significant correlation between delta of resting pulse rate and final training work and delta of training work.
154: Influence of combined carbohydrate and physical load on blood lipoproteins, glucose, insulin and no levels in coronary heart disease patients with normal and impaired tolerance to carbohydrates
DM Aronov, MG Bubnova, NV Perova, NA Logunova
State Centre for Preventive Medicine, Moscow, Russian Federation
Aim To study the influence of combined carbohydrate and physical load (CGPL) on parameters of lipid and carbohydrate metabolism and NO production in coronary heart disease (CHD) patients (pts)and in healthy men.
Patients 43 men, aged 35-64, were included in the study, 15 of them were healthy (without CHD sighs after coronary angiography), 14 pts had CHD I-II FC with normal tolerance to carbohydrates and 14 pts were with CHD and impaired carbohydrate metabolism. All pts underwent standard glucose load (GL)of 75 g and 1 hour later performed stress test until 95% of maximum heart rate was reached. Blood samples were taken before and 2 and 4 h after GL.
Results In healthy men (group 1) 4 h after CGPL significant decrease of total Ch (−6.3%), TG (−11.8%) levels and increase of HDL-Ch (+ 4.4%) level, while in CHD pts the increase of TC and LDL-Ch levels was observed. The insulin level after CGPL significantly rose in group 1 and 2 pts (with normal tolerance to glucose), but in group 3 pts (impaired tolerance to glucose) the rise of insulin level was higher and longer. The NO concentration rose after CGPL in healthy men (+ 15.4%, P < 0.05) and decreased in group 2 pts (−38.7%, P < 0.02) and in group 3 (−18.8%, P < 0.05). Parameters of physical work performance (PWC) in healthy men after CGPL did not change, in CHD pts we observed significant decrease of PWC parameters. We registered higher and longer (> 3 h) increase of levels of insulin, LDL-Ch, TG and decrease of NO concentration in CHD pts with impaired tolerance to glucose (group 3).
Conclusion we observed opposite effects of CGPL on blood levels of lipids, insulin and NO concentration in healthy men and in CHD pts. The elevation of blood levels of NO, HDL-Ch and decrease of blood LDL-Ch and TG levels were registered in healthy men. CHD pts especially with impaired tolerance to glucose responded with decrease of NO concentration and prolonged increase of levels of atherogenic lipids and insulin and worsening of PWC.
155: Cardiac rehabilitation lower mortality after myocardial infarction
C Sorensen, OS Mortensen, L Olsen, ML Larsen
Aarhus University Hospital, Denmark
Aim To study the effect on mortality in relation to post AMI patients participating in cardiac rehabilitation programs versus patients not participating.
Methods 730 post-AMI patients (in the DANAMI 2-trial) under 76 years were offered different levels of follow up depending on the rehabilitation programs in the local hospital and their own preferences. Going through each individual patient file, it was possible to classify the follow up as documented comprehensive cardiac rehabilitation or no rehabilitation.
Results The mortality among patients participating in cardiac rehabilitation programs were significantly lower than among patients not participating. Total cholesterol levels in the two groups were the same after one and 3 years, whereas physical score, daily exercise and smoking cessation were improved significantly in the rehabilitation group. The patients in the rehabilitation group were 3.1 years younger than the patients in the no rehabilitation group. However, the differences found were not explained by the age difference.
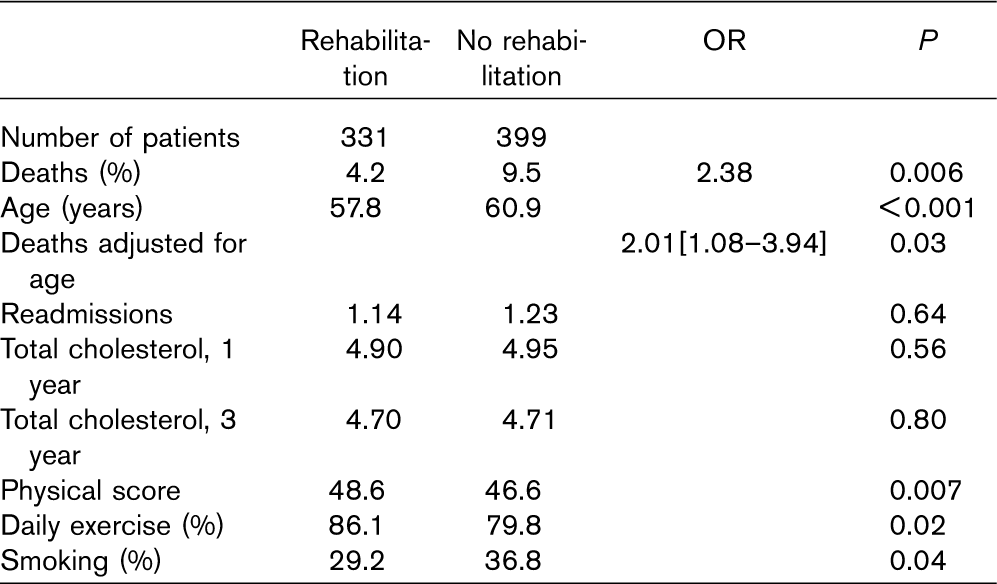
Conclusions Participating in a cardiac rehabilitation program lower mortality after a myocardial infarction.
159: Evaluation of physical efficiency and selected psychological aspects in patients with non-complicated myocardial infarction treated with direct PTCA
E Smolis-Bak, M Wojcicka, B Kazimierska, R Dabrowski, J Tylka, R Piotrowicz
Institute of Cardiology, Warsaw, Poland
Background Direct percutaneous coronary angioplasty [PTCA] improves prognosis in patients with acute myocardial infarction [AMI]. The aim of the study was comparison of physical efficiency, quality of life parameters between patients with non-complicated myocardial infarction treated with direct PTCA and men from control group with no history of infarction and coronary artery disease.
Methods Study group consisted of: group A-15 men after myocardial infarction with low cardiovascular risk, group B-control group, healthy men with no history of coronary artery disease. Patients age, BMI, style of life were similar in both groups. Patients after AMI were treated with beta-blockers, ACE-inhibitors, aspirin, clopidogrel and statins. On the 7th day after AMI following procedures were performed: three step Bassey walking test acc.to Smolis-Bak modification, index of physical efficiency: index of HRs with standard walking velocity (4 km per hour), Quality of Life questionnaire SF-36, J.E. Ware & C.D. Scherburne, in Tylka modification.
Results HRs index was significantly lower in A group: 69.9 versus 84.26 in group B (P < 0.005). There were no statistically significant differences in max.workload (METS), max.walking velocity and increase of heart rate after exercise between groups. Resting and max. heart rate (HR)values were significantly lower in group A in comparison with B, respectively: 64.8 vs 82.5 group B (p < 0.05) and 74.8 vs 93.5 group B (P < 0.005). No differences in subjective evaluation of quality of life were observed.
Conclusions Lack of differences in METS, max. walking velocity and increase of HR indicate for similar exercise tolerance in both groups. Evaluation of selected psychological aspects reveals that non-complicated infarction does not influence quality of life of patients. Complex and early hospital rehabilitation (since 1st day) results in similar to healthy men level of physical efficiency in patients after AMI treated with direct PTCA.
161: The importance of pulse wave velocity in hypertensive patients which are to be included in a rehabilitation program
Stela Iurciuc, M Iurciuc, Livia Barbu, S Ursoniu, D Gaita, CA Sarau, Laura David, D Duda-Seiman, Silvia Mancas
Department of Cardiovascular Rehabilitation, Timisoara, Romania
Background The pulse wave velocity (PWV) represents a method of evaluating the arterial rigidity. Recent epidemiological studies have proved that the PWV and the pulse pressure (PP) represent independent predictors of cardiovascular mortality in hypertensive old subjects. The change of arterial rigidity appears in initial states of arterial hypertension, and this is why the early identifying of PWV values could allow the identifying of and intervention on the complications of hypertensive disorder.
Methods We studied 89 subjects, with average age of 55.22 ± 11.69 years; of which: men: 47.19% and women: 52.81%, with essential hypertension: normal high, grade 1 and 2 (ESC-ESH 2003). The subjects have been evaluated from a clinical and paraclinical point of view according to the standard protocol of inclusion in the recovery program. The PWV of the carotid-radial (PWVc-r) has been determined for all subjects through automatic monitoring using the Complior device.
Results We have noticed that the following cardiovascular risk factors (CVRF): male aged over 55 associates prevalently with values of PWVc-r over 10 m/s (bivaried analysis through the chi square test: O r = 3.11; 95%CI: 1.20-8.07), the same correlation has also been obtained for smokers with PWVc-r values > 10 m/s (Or =3.39; 95%CI: 1.13-10.20). There is also a simple linear correlation between PWV (the dependent variable) and the following independent variables: the systolic blood pressure (SBP) and the pulsed pressure PP (r = 0.24, P = 0.027).
Conclusion Evaluating the arterial rigidity by measuring the aortic PWV may constitute a reference in the evaluation of the benefits of the cardiovascular rehabilitation program for a hypertensive patient. Follow up data reviles: the arterial rigidity correlates positively with some CVRF: males aged over 55, as well as with the condition of being smokers. The SBP, as well as the PP values modify the arterial rigidity parameters like PWV.
162: Complication rate during Phase II. residential cardiac rehabilitation after coronary events
É Csendes, I Berényi, A Simon, I Tiringer, F Endersz, J Csuhaj, É Szeles, G Veress
State Heart Hospital, Balatonfüred, Hungary
Background We investigated the occurence of complications and adverse events among patients participating in phase II. residential cardiac rehabilitation program, after coronary event (myocardial infarction, transluminal coronary angioplasty or coronary artery bypass graft operation). We determined the factors, that can influence the rate and seriousness of these events. 724 patients were included in the study prospectively, 302 after myocardial infarction (MI), 64 after transluminal coronary angioplasty (PTCA), 358 after coronary artery bypass graft (CABG), respectively.
Results During the rehabilitation program 25.5% of patients suffered from complication, the most frequent events were pleural effusion (5.6%), pericardial effusion (3.9%), Dressler's syndrome (3.5%), heart failure (2.9%), difficulties with heeling of wounds (2.6%), angina pectoris (2.3%), and atrial fibrillation (2.1%). 168 patients (23.2%) could complete the rehabilitation program in spite of these complications, 19 patients (2.6%) had to be transferred to other hospital wards. There was no difference in complication rate among men and women. The rate of complications were different in the patient groups composed according to the last coronary event (16.6% after AMI, 6.2% after PTCA, 37.2% after CABG, P < 0.001). Elderly patients (≥ 65 years) had higher complication rate (31.8% vs. 21.3%, P < 0.01). The rate of adverse events were between 0 and 42.6% in a data matrix, built up according to three categories (gender, coronary event, and age groups).
Conclusion With simple categories we can identify those patients, who had higher complication rate during phase II. residential cardiac rehabilitation program after coronary event.
165: Effects of a walking training on autonomic cardiac regulation in post CABG patients
Jadwiga Wolszakiewicz, Maria Biliñska, Bogna Foss-Nieradko, Ryszard Piotrowicz
National Institute of Cardiology, Warsaw, Poland
Background Autonomic tone is considered as a cardiovascular risk factor. There is only few information regarding the effects of exercise training on autonomic regulation in post CABG patients.
Objective The aim of our study was to assess the influence of walking training (WT) on the autonomic tone and on the efficacy of the early phase of cardiac rehabilitation in post CABG patients.
Methods 38 patients (p) (36 men and 2 women) mean age 62 ± 9 years, 10 ± 2 days post CABG were included to the study and randomized into two groups: GA-19 p, qualified for cardiac rehabilitation (CR) according to national standards plus additional WT (6 sessions for 6 minutes per day); GB-19 p-trained only according to standards. All p underwent: 1) 6-minute walking test (6 MWT) during which walking distance (m) was assessed: at the beginning (I-6 MWT), at the end of CR (II-6 MWT) and 3 months post CABG (III-6MWT), 2) 24-h Holter monitoring performed on the day before discharge (I-Holter) and after 3 months (II-Holter) which examined time (SDNN) and frequency (LF, HF) domain of HRV. In addition, the influence of WT on cardiac events 3 months post CABG was assessed.
Results Walking distance increased significantly in both study groups (GA: 316 vs 374 vs 423, P < 0.01; GB: 305 vs 365 vs 418, P < 0.01). There were no differences in time and frequency domain of HRV between the groups in I-Holter (GAvsGB SDNN: 96.71 vs 86.26, P = ns; LF: 75.66 vs 78.25, P = ns; HF: 45.08 vs 47.08, P = ns). Only additional WT in GA improved the time (SDNN: 96.71 vs 113.25, P < 0.05) and frequency domain (LF: 75.66 vs 55.47, P < 0.05) of HRV in II-Holter comparing with I-Holter. There were no differences in the incidence of cardiac events in both groups after 3 months.
Conclusion The walking training as a additional element of the early phase of cardiac rehabilitation post CABG caused a significant improvement in exercise capacity and cardiac autonomic tone.
172: Response to exercise training in ICD vs non-ICD patients in a heart failure population
JP Schmid, M Anderegg, C Heimgartner, H Saner
Swiss Cardiovascular Centre Bern, Switzerland
Background Patients (pts) with an implantable cardioverter defibrillator (ICD) were reported to have an attenuated response to exercise training compared with non-ICD pts. The reason remains unclear, but differences in left ventricular function have been postulated. We therefore compared the effect of a cardiac rehabilitation (CR) programme in ICD vs non-ICD patients with an ejection fraction < 45%.
Methods The CR programme was attained 3 times a week for 3 months. 26 pts with an ICD (84.6% male, mean age 59.5 ± 10.8 years) were compared with 148 pts without ICD (86.5% male, mean age 59.5 ± 11.4 years). The outcome was measured by cardiopulmonary exercise testing, echocardiography, BNP measurement and health related quality of life (HRQOL) questionnaires (Minnesota Living With Heart Failure Questionnaire and Hospital Anxiety and Depression Score).
Results At baseline, ICD pts had a significantly lower ejection fraction (EF; 24.5 ± 5.9% vs 28.4 ± 7.0%, P = 0.005). Peak VO2 (16.3 ± 4.8 vs 17.6 ± 19.6 ml/kg/min., P = 0.056), BNP (360 ± 246 vs 409 ± 421 pg/ml, P = 0.726) and left ventricular enddiastolic diameter (LVEDD; 66.8 ± 8.0 vs 63.7 ± 9.1 mm, P = 0.108) did not differ significantly between the two groups. Differences in improvements in peak VO2 (P = 0.380) and EF (P = 0.178) as well as reductions in LVEDD (P = 0.275) and BNP (P = 0.213) were not statistically different between the two groups. There were no baseline differences in HRQOL between the two groups, and total MLHFQ score improved in both (P = 0.972), but the HADS anxiety score increased in ICD pts, whereas it decreased in non-ICD pts (P = 0.029).
Conclusions In a population of chronic heart failure pts attaining a CR programme, ICD pts represent a group of pts with a more severe clinical impairment. Improvements are similar as in the non-ICD population, except for anxiety, which means, that this issue should be addressed specifically in ICD pts.
180: Motor development in children with congenital heart diseases compared to healthy peers
B Bjarnason-Wehrens, S Dordel, S Schickendantz, K Krumm, C Gogol, D Bott, K Brockmeier
Institute for Cardiology and Sports Medicine, German Sport University Cologne, Germany
While numerous studies have investigated exercise tolerance in children with congenital heart diseases (CHD) few have focused on their motor abilities. The aim of this study was to evaluate motor development in CHD-children compared to healthy peers.
A sample of 194 children (106 boys, 88 girls, mean age 10.0 ± 2.7 yrs) representing a spectrum of CHD (single ventricle to fully corrected heart defects) was compared to a representative control group (CG) of 455 healthy children (220 boys, 235 girls, mean age 9.6 ± 2.17 yrs). The body-coordination-test for children (KTK) was used to examine motor development. ANOVA and Chi-Quadrate were used for statistical analysis.
KTK testing revealed 39.7% of the CHD-G had normal and 1.5% good motor development, while 26.8% showed moderate and 31.9% severe motor disturbances. By comparison, in the CG 8.6% scored good and 69.5% had normal motor development, whereas 16.5% displayed moderate and 5.5% severe motor disturbances. The differences between the groups were significant (P < 0.001). The mean age- and gender-adjusted motor quotient (GMQ) was significantly lower in the CHD-G compared to the CG (79.6 ± 18.9 vs. 96.6 ± 15; P < 0.001). This was also true of all KTK subtests (MQ1-4). Depending on the presence and/or degree of residual sequelae (RS) the CHD-G were divided into two groups (A: no or moderate RS, B: significant RS). In Group B the mean GMQ was significantly lower than in group A (75 ± 19.3 vs. 83 ± 17.9; P < 0.01). In both subgroups mean GMQ was significantly lower (P < 0.01) than in the CG.
These results demonstrate deficits in the motor development in CHD-children. This was seen in the children with significant RS as well as in those with no or mild RS. Parental overprotection and the resulting lack of physical activity may contribute to this. Participation in supervised programs for the promotion of motor abilities can help to limit motor deficits in CHD-children and prepare and support their integration with peers.
183: Disability, health beliefs and emotional state in angina patients in primary care
NA Stuckey, H Taylor, M Andrew, L Taylor, C Bickler, M McGovern
Lothian Primary Care Organisation, United Kingdom
Background The rehabilitation of patients after M.I. and CABG is now reasonably well established. The number of patients with angina exceeds that of these two groups and no clear structure exists to meet their rehabilitation needs and this may need to be managed in the long term, within Primary care. Work by Lewin and Furze (2000, 2001, 2003) has indicated that angina patients have significant health beliefs which influence behaviour, disability and emotional state.
Aims of study To identify the current experience and needs of angina patients in relation to developing a rehabilitation structure, and elicit views of both primary and secondary care clinicians on patient needs and development of potential care pathway.
Methods 762 patients in two GP practices were screened to identify angina patients meeting inclusion criteria. Those meeting inclusion criteria (329) were sent questionnaires asking about experience of care, identification of needs, physical and psychological symptoms, (CLASP), function and disability (SIP) and health beliefs (York Angina Beliefs Questionnaire). A proportion from each practice were interviewed by the research nurse to provide more qualitative data. Primary and Secondary care staff views were elicited on the needs of angina patients and pathway of care.
Results Questionnaire measures indicated high levels of misconceptions, disability and emotional distress which were strongly correlated. Symptoms of angina and breathlessness were well controlled and did not account for the degree of disability. Patient interviews indicate significant need in relation to understanding of condition, risk factor management and management of disability and psychological issues. Clinicians responses indicate consistency in some key components of a desirable pathway and what should be available to patients with angina. Specific areas of need were identified in terms of training and potential for improvement in the pathway.
186: Cardiac rehabilitation improves long-term survival after acute coronary syndrome
K Viswanathan, N Artis, K Bailey, C Morrell, R Das, N Kilcullen, JH Barth, AS Hall; The EMMACE-2 Investigators
Leeds General Infirmary, United Kingdom
Objective To assess the impact of cardiac rehabilitation on the long-term mortality of patients with acute coronary syndrome (ACS).
Design Prospective observational registry across 11 adjacent hospitals in West Yorkshire, United Kingdom.
Methods The EMMACE-2 study included 2461 consecutive consenting patients validated to have ACS during a 6-month period (Apr to Oct 2003). 2067 patients, who were discharged alive from hospital and for whom data on referral for cardiac rehabilitation was available, were included in the analysis. Patients were categorised based on the British Cardiac Society working group definition into 4 groups: Unstable angina, Troponin positive ACS (i.e. myocyte necrosis, not MI), Non ST-elevation MI (NSTEMI) and ST-elevation MI (STEMI). Median long-term follow-up for mortality was 786 days.
Results Referral for cardiac rehabilitation was a significant predictor of long-term all-cause mortality among patients discharged alive from hospital (HR 1.665; 95% CI = 1.372 to 2.02, P < 0.001). After multi-variate analysis with correction for age, baseline heart rate and systolic BP, cardiac rehabilitation was an independent predictor of long-term mortality (HR 1.26; 95%CI = 1.03 to 1.53, P = 0.02). Patients referred for rehabilitation were significantly less likely to die across each of the BCS categories of Troponin positive ACS (HR 1.627; 95% CI 1.036 to 2.557; P = 0.035), NSTEMI (HR 1.961; 95% CI 1.444 to 2.662; P < 0.001) and STEMI (HR 1.749; 95% CI 1.021 to 2.998; P = 0.042). Only 34% of troponin positive ACS patients (153/452) were referred for cardiac rehabilitation as compared to 69% of NSTEMI patients (527/765). This is notable as the long-term post-discharge mortality in patients with troponin positive ACS was comparable to that of patients with NSTEMI (22.6% vs. 21.8%)
Conclusion Cardiac rehabilitation improves long-term survival in patients with acute coronary syndrome and should be offered to all patients with evidence of myocyte necrosis or MI.
189: Benefits of performance-specific parameters after a one year ambulant cardiac rehabilitation (Phase III)
H Traninger, H Harpf, L Harpf, S Harb, G Tscheppe, P Hoffmann, M Wonisch
Institute of active exercise therapy Eggenberg, Graz, Austria
Background Regular exercise training is accepted as basis of cardiac rehabilitation programs. The aim of the study is to show the progress of the performance from 60 persons after a one year ambulant rehabilitation, based on the Austrian guidelines for cardiac rehabilitation (1), which recommend exercise for at least 2 times per week.
Methods 57 male patients (age: 60 + 10 years, height: 175 + 8 cm, weight: 81 + 11 kg) attended a one year ambulant cardiac rehabilitation program, including 30 minutes endurance cycling training and 25 minutes strength or flexibility training twice a week. A symptom limited incremental cycle ergometer test was done at the beginning of the therapy (e1), after 6 month (e2) and after 12 month (e3). The intensity of the training was established individually with either a heart rate (HR) according to 50-70% of maximal power output (P max) or the HR corresponding to 75-85% of the heart rate threshold.
Results The average presence was 70 + 33%. Medication could be changed according to the individual decision of the physician, but was fairly identical. All subjects showed a significant increase of maximal power out put from 144 + 47 W (e1) to 165 + 47 W (e2) and 175 + 49 W (e3) respectively, which was 18 + 19% and 25 + 23% respectively. The average (HR) at (100 W) changed significantly from 111 + 16 beats per minutes (bpm) (e1) to 107 + 19 bpm (e2) respectively 103 + 14 bpm (e3) respectively.
Conclusion There is a huge amount of evidence based studies (2) suggesting physical training 4-7 days per week. In this group of patients good progress in performance parameters could be achieved with guided training twice a week. However, the goal should be to reach a weekly energy consumption of additional 1700-3000 kcal. This means that it is getting more and more important to make the patients aware of the fact that they should do further exercises in addition to the regular training units.
201: Evaluation of the impact of the long-term complex rehabilitation measures in coronary heart disease patients after successful coronary angioplasty
D Vasiliauskas, L Jasiukevièienë, V Grias, J Marcinkevièienë, R Raugalienë, M Beresnevaitë, L Leimonienë, V Tumynienë
Kaunas University of Medicine, Institute of Cardiology, Lithuania
Aim of the study To evaluate the impact of the long-term complex rehabilitation in coronary heart disease patients after successful coronary angioplasty.
Object and methods Ninety patients after successful coronary angioplasty in cases of acute myocardial infarction, stable or unstable angina pectoris underwent Doppler echocardiography and ergospirometry. They practice 6 month-term lifestyle modification and risk factors correction, exercise programs and psychological rehabilitation. Measurements were repeated after 6 and 12 months. Ninety patients were studied as controls and used only medicamental treatment without rehabilitation complex programs.
Results After 6 months in rehabilitation group patients statistically significant (P < 0.05) improved exercise capacity and respiratory efficiency data: gas exchange ratio RQ (1.16 ± 0.14 vs 1.08 ± 0.07), oxygen consumption at anaerobic threshold AT VO2 (17.3 ± 7.2 vs 20.8 ± 5.4 ml/kg/min), oxygen ventilatory equivalent VE/VO2max (27.3 ± 5.3 vs 24.9 ± 4.3).
The Doppler echocardiographic findings revealed significant (P < 0.05) improvement: index of left ventricular wall movement decreased (1.65 ± 0.25 vs 1.59 ± 0.31) and ejection fraction increased (42.2 ± 7.22 vs 48.04 ± 5.45%), left atrium decreased (60.8 ± 3.9 vs 58.2 ± 2.3 mm), and left ventricular wall thickness decreased. Improved ergospirometric and echocardiographic data were established after 12 months too. Were no positive changes of these instrumental findings in controls, but it was determined significant (P < 0.05) augmentation in left ventricular end diastolic diameter in control group.
Conclusion Long-term complex rehabilitation and secondary prevention is effective and workable measure improving left ventricular systolic function, respiratory efficiency and attenuating abnormal remodeling in coronary heart disease patients after successful angioplasty.
205: Analysis outcomes of cardiovascular rehabilitation program
J Brozaitiene, E Bovina, G Ziliukas
Institute of Psychophysiology and Rehabilitation, Kaunas University of Medicine, Lithuania
Aim of the study To analyse outcomes and values of heart rate (HR) autonomic control in post myocardial infarction patients (MI) during 2 years cardiovascular rehabilitation (CR) program.
Materials and methods We studied 458 MI patients: 30 patients (pts) were send on for coronary artery bypass graft surgery (1 group), 34 pts-for coronary angioplasty (2 group), 195 patients were followed-up during 2 years (3 group) and 24 patients of them died (4 group). Evaluation functional status (FS), counselling for physical activity, nutrition, behaviour modification, drug regime were core components of CR program. Clinical, biochemical, instrumental (ECG, bicycle exercise test, echocardiography) and analysis of HR variability, hemodynamics were performed during follow-up periods. On the ground of 11 syndromes and expression of symptoms quantitative indexes of functional status (FS%-zero percents means absence of pathological symptoms, while 100%-their maximal expression, poor state) and efficacy of rehabilitation (ER%) were assessed.
Results According to our data in 1-3 pts groups rare than in group with lethal outcomes arrhythmias (8.1 vs. 21.1%), repeated MI (5.1 vs. 29.2%), NYHA class 3 (48.1 vs. 70.8%), lower use in beta blockers (p < 0.05) were established. Bigest index of FS (accordingly, 47.1, 44.1, 45.8, 50.4%) and lower index of ER (5.7, 10.3, 8.9, 3.3%) were in 1 and 4 groups than in others (P < 0.05). Increased impact of humoral regulation (óVLF, accordingly 12.3 ± 8.1, 25.1 ± 7.9, 22.9 ± 6.8, 28.3 ± 7.2 ms) was established in 4 group patients than in 1-3 groups. Binary logistic regression model, with use values of HR variability and hemodynamic during early rehabilitation period, enabled 87% predict probability of events (R2 = 0.50, P < 0.05).
Conclusion In myocardial infarction patients with lethal outcomes poor functional state and lower efficacy of early CR was appropriate. Prepared binary logistic regression model enabled 87% predict outcomes of CR.
217: Maximal strength training improves endothelial function similar to that observed after moderate intensity endurance training in obese adults
Gjertrud Tyldum, Inga Schjerve, Arnt-Erik Tjønna, Tomas Stølen, Per-M Haram, Ulrik Wisløff
Norwegian University of Science and Technology, Norway
Background The worldwide epidemic of obesity requires cost-effective tools such as strength- and endurance training for prevention and rehabilitation. Maximal oxygen uptake and endothelial function are now established as robust markers of future cardiovascular morbidity and mortality. It is well established that obesity and endurance training reduce and improves both, respectively, whilst little is known about the effects of maximal strength training. The present study determines the effects of moderate- and high-intensity (interval-training) exercise and maximal strength training upon maximal oxygen uptake and endothelial function in obese adults.
Methods 42 adults with BMI of 36 ± 5 were randomized to 12 weeks, 3-times per week of either high-intensity interval training (HIT) (92.5% of maximal heart rate), moderate intensity (MIT) (70% of maximal heart rate; covered the same distance as individuals in the HIT-group so that only exercise-intensity differed) or a maximal strength training group (ST) (5RM × 4 in leg-press and 3 × 30 repetitions of exercise for abdominal and back muscles). Endothelial function in the brachial artery was measured by ultrasound.
Results Body weight and BMI decreased significantly (P ≤ 0.05) in both endurance training-groups and tended to decrease in strength trained subjects (P = 0.11). Maximal oxygen uptake increased by 34% in HIT (P ≤ 0.001), 16% in MIT (P ≤ 0.001), and 10% in ST (p < 0.01). Endothelial dysfunction was reversed in all training groups, but the effect on flow mediated dilatation was most pronounced in the HIT group. No traditional blood-marker of cardiovascular disease changed during the experimental period.
Conclusion Maximal strength training improves endothelial function similar to that observed after moderate intensity endurance training in obese adults. Whether the effects are additive to that observed in endurance-trained subjects should be addressed in future studies.
219: A single weekly bout of exercise may reduce cardiovascular mortality
Ulrik Wisløff, TomNilsen, Wenche Drøyvold, Siv Mørkved, Stig A Slørdahl, Lars Vatten
Norwegian University of Science and Technology, Norway
Background The observation that exercise training reduces cardiovascular mortality is robust and consistent, but the amount and intensity of exercise that is required for risk reduction is not yet resolved.
Methods We studied the association between exercise amount and intensity and cardiovascular mortality in 27,143 men and 28,929 women who were free from known cardiovascular disease at the beginning of follow-up between 1984 and 1986. The relative risk of death was calculated as the rate of death among participants within a given physical activity category as compared to the rate of death in the reference category (no physical activity). We used Cox regression analysis to adjust for age and other potentially confounding factors.
Results After 16 years (SD 4 years) of follow-up, 2946 (10.8%) men and 2486 (8.6%) women had died from ischemic heart disease or stroke. A single weekly bout of exercise of high intensity reduced the risk of cardiovascular death, both in men (relative risk, 0.61, 95% confidence interval, 0.49-0.75), and women (relative risk, 0.49, 95% confidence interval, 0.27-0.89), compared to those who reported no activity. There was no additional benefit from increasing the duration or the number of exercise sessions per week. The risk reduction related to exercise increased with increasing age in men, but not in women.
Conclusions These results challenge the current recommendation that expenditure of at least 1000 kcal per week is required to achieve exercise-induced protection against premature cardiovascular mortality.
236: Effects of cardiac rehabilitation on pulmonary function in patients with chronic heart failure
D Zieliñska, J Bellwon, A Rynkiewicz, S Bakula
Department of Rehabilitation, Medical University of Gdansk, Gdansk, Poland
Background Respiratory system becomes affected very early in the natural history of chronic heart failure. These abnormalities comprise structural changes of the lung with concomitant impairment of respiratory function. The aim of our study was to evaluate the impact of regular exercise training on spirometry results in patients with chronic heart failure.
Methods We examined 43 patients with stable heart failure, NYHA class II-III, 37 due to coronary artery disease and 6 due to dilated cardiomyopathy, 37 men and 6 women, age 62 ± 8 years. All patients underwent a 3 week supervised ambulatory exercise training program, which included interval exercise on cycle ergometer and both aerobic and strength training with exercise intensity at 60-80% of the peak heart rate. Afterwards patients were instructed how to continue the exercise training program at home for 9 weeks. Symptom limited cycle ergometer exercise tests with 25 Watt increments every 3 minutes were performed before and after controlled exercise training and after home-based training. Spirometry was performed using MES with LungTest1000 program. Vital capacity VC, forced expiratory vital capacity VC ex, forced inspiratory vital capacity VC in, forced expiratory volume in 1 second FEV1 and FEV1%VC were analysed.
Results There were positive significant correlations between exercise capacity assessed by exercise test time and VC r = 0.46 (P < 0.05) and between exercise capacity and FEV1 r = 0.42 (P < 0.05) before the training. After the training VC did not change 95.9 ± 18.6 and 97.6 ± 17.0% of normal, VC ex and VC in increased significantly from 3.6 ± 1.0 to 3.9 ± 0.9 (P < 0.05) and from 3.6 ± 1.0 to 3.9 ± 0.9 L (P < 0.05) respectively. Dynamic lung volumes FEV1 and FEV1 %VC did not change after the training 2.6 ± 0.8 to 2.8 ± 0.7 L and 69.8 ± 12.1 to 72.6 ± 8.1% respectively.
Conclusion Exercise training improved forced expiratory and inspiratory volumes in patients with chronic heart failure.
239: Illness perceptions in cardiac patients attending a cardiac rehabilitation programme
K Slack, HM McGee, D Hevey, JH Horgan
Department of Cardiology, Beaumont Hospital, Dublin 9, Ireland
Background Studies of patients' own perceptions of illness have shown that these can influence recovery. This study assessed perceptions of illness before and after outpatient (phase III) cardiac rehabilitation (CR). Since age and gender can influence illness perceptions, these were also considered.
Methods Consecutive patients attending CR were included. Demographic, clinical and secondary prevention profiles were recorded. Perceptions of illness were assessed by the Illness Perceptions Questionnaire-Revised (IPQ-R) and psychological well-being by the Hospital Anxiety & Depression Scales (HADS) pre- and post-CR.
Results 133 of 135 patients invited participated with 121 (90%) completing post-CR measures (58% men and 58% aged 65 + years). Positive changes in perceptions were noted following CR-patients were more likely to see their condition as chronic (and less likely to see it as cyclical), had a more coherent view of their condition and had fewer negative emotional representations. Younger patients were more aware of serious consequences of their condition but also saw it as more controllable. Nonetheless they were more anxious than older patients. Women had a less coherent view of their illness, felt it was less controllable and reported more negative representations than men. Changes over the course of CR did not change these age and gender differentials.
Conclusions Findings indicated positive changes in illness perceptions after CR. However, age and gender variations indicated stable differences that need addressing. Older and female patients could benefit from targeted interventions if negative perceptions of illness are to be counteracted to assist in long-term secondary prevention.
240: Exercise capacity following Phase III cardiac rehabilitation: are improvements influenced by age or gender?
D Dodd, HM McGee, D Hevey, JH Horgan
Department of Cardiology, Beaumont Hospital, Dublin 9, Ireland
Background Many older people and women do not participate in cardiac rehabilitation (CR) programmes. Very few studies have evaluated CR outcomes for older people (i.e. aged 75 + years). This retrospective study assessed whether improvements in exercise capacity are similar in younger and older patients (75 + years).
Methods Identified eligible cardiac patients admitted during a four-year period. Consecutive patients admitted to hospital who completed a phase III CR programme were identified through hospital information systems. To identify adequate numbers of those aged 75 + (particularly women) for assessment, records over 4 years were assessed. Matching for gender and age with groups aged 51-74 and < 50 years, 241 eligible patients were identified (68 were aged 75 + with 33% (n = 23) being women. Demographic and risk factor profiles were recorded alongside exercise capacity measurements pre- and post-CR.
Results Both younger and older men had higher exercise capacity pre-CR, i.e. baseline exercise capacity was on average 9.6 METs (younger men), 5.9 METs (older men), 7.0 METs (younger women) & 5.0 METs (older women). Post-CR increases averaged 3 METS acrosss groups. There were no significant differences in exercise capacity improvements by patient groups post-CR, i.e. all patients, regardless of gender and age, improved similarly.
Conclusions Findings showed that CR is beneficial in improving exercise capacity across the complete age and gender spectrum. However, equivalent improvement for older people, since they started with lower absolute physical capacity, may be clinically more meaningful in terms of maintaining independence. CR should be strongly advocated for older as well as younger patients.
241: Adoption of the cardiac rehabilitation information system as a national audit mechanism for Ireland
M Kiernan, HM McGee, R Flynn, D Hevey
Health Services Research Centre, RCSI, Ireland
Background The Cardiovascular Health Strategy (1999) recommended development of a national cardiac rehabilitation information system. This system, called the Cardiac Rehabilitation Information System (CRIS), was developed through consultation. CRIS involves an annual Service Assessment Form detailing programme staff, equipment and patient throughput and a Patient Assessment Form recording details of all patients eligible for cardiac rehabilitation from hospital admission entry to the end of phase III rehabilitation. All programmes were encouraged to adopt CRIS as an audit system from January 2005. Uptake of CRIS was assessed six months later.
Methods All 39 hospitals providing cardiac rehabilitation services were surveyed by postal questionnaire in Summer 2005. Information on use of CRIS or other databases was obtained.
Results 37 of 39 hospitals responded. Of these, 34 provided phase III (out-patient) programmes. A total of 19 (56%) used CRIS with 3 others using other systems (i.e. 65% overall using information systems). A further 8 had advanced plans to use CRIS (23%) with only 4 hospitals (12%) unsure about plans for information systems. At patient level, information on over 3,000 patients had been collected since January. At service level, 24 centres had dedicated facilities with 10 sharing facilities. 26 services referred patients to HeartWatch.
Conclusions CRIS has already been adopted widely in cardiac rehabilitation services. Two in three services now have an information system with most others about to start. Patient and service level information will be invaluable in describing cardiac rehabilitation achievements and needs into the future.
260: Effects of early cardiac rehabilitation exercise training in old patients after heart surgery
B Eder, P Hofmann, D Brandt
Center for Cardiac Rehabilitation, SKA RZ-St. Radegund/PVA, Austria
Aim The effects of additional walking (W) or cycle ergometer (C) training on exercise performance were compared to a standard rehabilitation program after heart surgery in old patients.
Methods Sixty (32 m, 28 F) patients (73.1 ± 4.7 yrs) were randomly assigned in 3 groups. Subjects performed a symptom limited cycle ergometer test and completed a 6-minute walk test (6MWT). The MacNew quality of life questionnaire was used. All tests were performed before (Pre) and after (Post) four weeks of cardiac rehabilitation. Control (Co) patients underwent a standard training program. Groups Wand C completed the standard training program with additional structured and regulated W or C training.
Results In Pre no significant differences were detected between groups for maximal oxygen uptake (VO2max) (W: 13.5 ± 2.5 ml/kg/min; C: 13.3 ± 1.9 ml/kg/min; Co: 12.4 ± 2.4 ml/kg/min) maximal power output (P max) (W: 45.8 ± 13.2W; C: 45.6 ± 15.8W; Co: 40.2 ± 12.3W), maximal heart rate (HRmax), (W: 103 ± 17bpm; C: 102 ± 13bpm; Co: 104 ± 16 bpm), rating of perceived exertion at Pmax (RPEmax) (W: 14.5 ± 1.8; C: 14.6 ± 1.7; Co: 14.5 ± 1.2), distance in the 6-MWT: W: 321 ± 82 m; C: 335 ± 73 m; Co: 304 ± 80 m) and global QOL score (W: 5.8; C: 5.5; Co: 5.3). Post training these variables improved significantly within all three groups (VO2max: + 25-27%; P max: + 34-38%; HRmax: + 6-15%; RPEmax: + 15-16%; 6-MWT: + 24-30%; QOL global: + 12-16%). No significant differences between groups were found at Post except for P max in C compared with Co (P < 0.05).
Conclusions The cardiac rehabilitation program improved significantly exercise performance and QOL in old patients after heart surgery irrespective of amount and mode of training. Additional training caused no significant superior benefits except for P max. However, a trend was seen for a functional adaptation dependent on specifity and amount of time spent in exercise training.
274: Exercise tolerance after early cardiac rehabilitation correlates with quality of life in patients 3 months after an acute coronary syndrome
I Przywarska, A Brychcy, J Dalkowski, S Borowicz-Bienkowska, E Deskur-Smielecka, P Graczyk, A Jegier, K Szmigielska, P Dylewicz
University School of Physical Education, Rehabilitation Hospital, Poznan, Poland
Aim To verify which of the following parameters: physical activity before acute coronary syndrome (ACS), left ventricular ejection fraction (LVEF), exercise tolerance before early cardiac rehabilitation, or exercise tolerance after the rehabilitation correlate with quality of life in patients 3 months after ACS.
Subjects 58 patients aged 36-78 referred to cardiac rehabilitation 17 ± 0.9 (mean ± SEM) days after ACS.
Methods Before rehabilitation program all patients performed a treadmill exercise test, had an echocardiography with LVEF calculation, and their physical activity before ACS was estimated based on the Stanford questionnaire. At the end of the rehabilitation program patients performed a second exercise test. Patients' quality of life was assessed with the Euro-QoL EQ-5D questionnaire 3 months after ACS. The rehabilitation program lasted 3 weeks and consisted of 15 training sessions. The program included: callisthenics, cycle ergometer training with intensity of 50% of the heart rate reserve, and Nordic Walking.
Results The mean exercise tolerance before rehabilitation program was 7.2 ± 0.33 METs, and after the program 8.9 ± 0.38METs (P < 0.001). The mean change in exercise tolerance during the rehabilitation program was 1.7 ± 0.26 METs. The LVEF was 51 ± 1.0%. The mean overall health-related quality of life 3 months after ACS was scored 69.9 ± 1.9 in the EQ-5D 0-100 scale. The following significant correlations were found: between exercise tolerance after the rehabilitation program and EQ-5D score (r = 0.42, P < 0.001), between exercise tolerance before the program and EQ-5D score (r = 0.34, P < 0.01), and between the change in exercise tolerance and EQ-5D score (r = 0.31, P < 0.03). No significant correlation was found between LVEF and EQ-5D score.
Conclusion Exercise tolerance after early cardiac rehabilitation and increase in exercise tolerance correlate with quality of life in patients 3 months after an acute coronary syndrome.
278: Interval and continuous training in cardiovascular rehabilitation
J Siegelova, L Mifkova, M Novak, B Fiser, P Homolka, H Svacinova, F Varnay, P Vank, L Spinarova, J Vitovec
St Anna Teaching Hospital, Faculty of Medicine, Masaryk University, Brno, Czech Republic
Aim The objective of the study was to evaluate the physiological effectiveness and the influence of two modifications of aerobic training: interval (IT) and continuous (CT) one on physical performance and aerobic capacity in patients with coronary heart disease.
Methods Twenty two males with coronary heart disease (age 57 ± 9 years) were randomly divided in two groups. All patients were examined by symptom-limited spiroergometry and passed three-month training programme of 60 min 3 times a week (10 min of warm-up phase, 25 min of aerobic phase, 15 min of resistance training, 10 min of relaxing phase). The first group (n = 11, IT) passed the aerobic phase the interval training, (30-second work phases with work load intensity on the level of anaerobic threshold alternating with 60-second recovery phases) with intensity of 5 W; the second group passed the aerobic phase of the programme with continual work load of intensity on the level of ventilatory anaerobic threshold (CT, n = 11). After the termination of three-month rehabilitation programme the spiroergometry was repeated.
Results We have found an significant (P < 0.05) increases of maximal achieved work load (before versus after; IT: 104 ± 46 vs. 143 ± 49 W, CT: 113 ± 33 vs. 142 ± 34 W) and aerobic capacity (IT: 1682 ± 529 vs. 2166 ± 649 ml.min−1, CT 1713 ± 421 vs. 2045 ± 449 ml.min1). In spite of the fact that the group with interval training performed 2.5-3 times less work in each training unit, the performance and aerobic capacity parameters after the termination of three-month programme did not statistically significantly differ from the group with continuous training.
Support—MSM 0021622402, IGA MZ CZ 7983-3.
282: Influence of nordic walking on exercise capacity and physical fitness in patients during second phase of rehabilitation after an acute coronary syndrome
M Wilk, P Kocur, A Rozanska, E Deskur-Smielecka, I Przywarska, S Borowicz-Bienkowska, P Dylewicz
Dept. of Cardiac Reh, University School of Physical Education, Poznan, Poland
Aim The aim of the study was to investigate the influence of Nordic Walking on exercise capacity and physical fitness in patients during second phase of rehabilitation after an acute coronary syndrome (ACS).
Material and methods The study population consisted of 40 patients hospitalized on a cardiac rehabilitation ward 14 to 28 days after ACS. On admission and after completing the rehabilitation program patients performed a treadmill exercise test and the Fullerton Functional Fitness Test (consisting of the following items: 30-second chair stand, arm curl, 6-minute walk, chair sit-and-reach, back scratch, an 8-foot up-and-go). 10 subjects were assigned to a control group (C group), which followed a standard training program, 20 patients to a group which additionally performed Nordic Walking 5 times a week (NW group), and 10 patients in addition to the standard rehabilitation program participated in regular walking (without poles; RW group). Each session of Nordic Walking or regular walking lasted 40 minutes and consisted of a 3-kilometer walk interrupted by breaks during which respiratory exercises and stretching were performed.
Results Exercise tolerance improved significantly in all study groups. However, the percent of increase in exercise tolerance in the NW group was greater than in RW and control groups (30%, 21%, and 14%, respectively). The 6-minute walk distance increased by 22% in the NW group, by 8% in the RW group, and by 17% in the control group. The results of the remaining Fullerton test items improved in similar degree in all study groups.
Conclusion Nordic Walking increases exercise capacity and physical fitness in patients during second phase of rehabilitation after ACS.
285: Exercise training and cardiovascular autonomic function in obese patients
H. Svacinova, J Necasova, M Tarasova, J Siegelova, B Fiser, L Svoboda, I Hruby, D Zeman
St Anna Teaching Hospital, Faculty of Medicine, Masaryk University Brno, Czech Rep
Objective The study was designed to analyze the impact of exercise training on heart rate variability (HRV), baroreflex sensitivity (BRS) and aerobic fitness in obese patients (OB) with (OBH) and without (OBN) hypertension.
Design and methods We examined 27 obese patients (OB, age 56.6 years, BMI 34, 6 men, 21 women, 11 patients with DM type 2) before 12 weeks of exercise therapy and after them. The HRV, BRS, aerobic fitness and anthropometric values were evaluated in two subgroups-with hypertension (OBH, n = 15, age 57 years, BMI 34.3) and without hypertension (OBN, n = 12, age 56.1, BMI 33.6). HRV was determined by spectral analysis of short-term heart rate record (Varia Puls T3) in supine position with metronome-controlled breathing (0.33 Hz). We evaluated the power spectra of HRV (total power TP log ms2, LF log ms2, HF log ms2, LF/HF ratio). BRS was determined by spectral analysis of spontaneous fluctuations of systolic blood pressure and cardiac intervals (Finapres, 5-min record, metronome-controlled breathing at frequency 0.33 Hz). The aerobic fitness (VO2max,Wmax) was determined by spiroergometry.
Results Both in OB and OBH the BRS values (5.3 ± 2.8 vs.6.7 ± 3; 5.4 ± 2.8 vs. 7.1 ± 3.1; P < 0.05) and VO2max/kg (16.5 ± 4.3 vs.19 ± 4.2) increased significantly, as well as Wmax/kg (0.96 ± 0.4 vs. 1.2 ± 0.36) in OBH. Body weight, BMI and waist circumference decreased significantly in all groups. In OB group we found out boundary decrease of the LF/HF ratio (−0.2 ± 1.1 vs.-0.49 ± 0.9, P = 0.05); in OBH favourable trend in HF was present (5.2 ± 1 vs. 5.5 ± 0.8, P = 0.06) as well as in OBN in LF/HF ratio (−0.2 ± 1.4 vs. − 0.59 ± 1.2, P = 0.09).
Conclusion In obese patients exercise treatment increased BRS and aerobic fitness, also anthropometric values were favourably influenced. In HRV values the trend to improvement of sympathovagal balance was found. This favourable effect was more strongly demonstrated in OBH.
Supported by MSM 0021622402.
287: Early results of comprehensive cardiac rehabilitation after biventicular pacemaker implantation
G Veress, B Merkely, J Masszi, L Gellér, J Faluközy, V Kutyifa, G Veress Jr., G Mikes, A Simon, IJ Dobran
State Heart Hospital Balatonfüred, Hungary
Background Cardiac resyncronisation achieved through biventicular pacing (BIV) produces clinical benefits in pts with heart failure who have wide QRS (LBBB).
Objective There are no systematic data about the clinical efficacy of comprehensive cardiac rehabilitation programme (CCRP) in pts after BIV.
Method We randomly assigned 21 pts with BIV to CCRP group and 17 pts with BIV vere enrolled to a controll group with conventional follow up, without CCRP. Clinical effects of BIV + CCRP were prospectively investigated and compared with those pts without CCRP.
Results After 4 weeks residental CCRP 6 min walk test increased from 385 ± 67.57 m to 445.88 ± 113.8 m (P < 0.1 N.S.) BMI decreased from 27.49 ± 3.83 to 26.38 ± 3.63 and NYHA functional class improved from 3.22 ± 0.66 to 2.71 ± 0.48 (P: 0.14 N.S.). In this group (CCRP) at 8 months check-up NYHA class was 2.09 ± 0.54, BMI: 25.04 ± 2.01 EF: 35.61 ± 7.96%, 6 min walk test: 487.5 ± 147.56 m. In control group (17 pts with BIV but without CCRP) at 8 months follow up we observed the following results: NYHA class: 2.41 ± 0.79, BMI: 26.72 ± 3.38, EF: 34.07 ± 7.42%, and 6 min walk test 342.35 ± 118.39 m (P < 0.02) respectively.
Conclusion Our results demonstrated a better functional capacity in those pts with BIV who participated in 4 weeks residential programme. This study was conducted in a short duration and the number of pts with BIV was relatively small therefore the long term benefits of CCRP need to be assessed by additional prospective large scale multicenter studies.
290: Cardiac rehabilitation of patients with implantable cardioverter defibrillator
J Masszi, J Faluközy, A Simon, G Dozzi, G Mikes, G Veress
State Heart Hospital Balatonfüred, Hungary
Comprehensive cardiac rehabilitation of patients with heart disease is an effective treatment. In our study we evaluate whether the residential rehabilitation treatment of patients with implantable cardioverter defibrillator (ICD) is also an effective and safe procedure.
Between 2000 and 2005 we studied 52 patients with ICD who underwent residential comprehensive cardiac rehabilitation. The average age of the patients was 62.62 ± 8.06 years, the average BMI was 29.48 ± 4.29 kg/m2. The echocardiographic parameters: the left ventricular (LV) ejection fraction was 37.59 ± 9.73%, the LV diastolic dimension was 65.71 ± 7.95 mm, the LV systolic dimension was 54.18 ± 9.03 mm, with an average of 1.93 ± 1.06 degree of mitral valve regurgitation. The patient performed 72.19 ± 20.31 W, and 4.52 ± 1.18 MET on exercise test with 101 ± 22.61 /min. maximal heart rate and 9.42 ± 1.33 ml/min/kg VO2max. The average NYHA class was 2.62 ± 0.52.
During the rehabilitation the patients took part in medical, psychological, dietary education and regular low intensity (2-4 MET) exercise training (gymnastic and bicycle or treadmill training) with an average training pulse of 88 ± 10.89/min. corresponding with the exercise test results. The physical condition of the patients improved, the six minutes walk test increased significantly from 346.25 ± 95.30 m to 467.83 ± 187.59m (P < 0.012). During the exercise training the patient did not experience ICD shock (26.9% of the patients got ICD shocks or ATP earlier).
We conclude that the residential cardiac rehabilitation is an effective and safe procedure of patients with ICD.
293: Effectiveness of cardiac rehabilitation in patients with supraventricular tachycardia with and without catheter ablation
IJ Dobran, JFaluközy, JMasszi, ASimon, ITiringer, DApró, GVeress
State Heart Hospital Balatonfüred, Hungary
Objectives The aim of our prospective randomized study is to analyze data on Quality of Life (QoL) collected from patients with symptomatic paroxysmal supraventricular tachycardia (PSVT) after radiofrequency catheter ablation and cardiac rehabilitation (group 1) versus PSVT without catheter ablation, but with drug therapy and cardiac rehabilitation (group 2).
Methods Data of 47 patients in Group 1 with average age of 63 ± 10 years male 50% vs. 58 patients in Group 2 with age of 56 ± 6 years, male 60% were analysed. The QoL assessment was made using Medical Outcomes Survey Short Form 36-item questionnaire (SF-36) with a 6 months follow-up after. Physical Function (PF), Role-Physical (RF), Body Pain (BP), General Health (GH), Vitality (Vit), Social Functioning (SF), Role Emotional (RE), Mental Health (MH) were compared in Group 1 vs. Group 2. We also evaluated the data based on the patient's gender. The differences were considered as significant by error probability P < 0.01.
Results In Group 1 the PF was 14.5%, the BP 15.1%, the RE 13% and the MH 10% significant higher vs. Group 2 (P < 0.01). Both groups have reached similar QoL values in GH, Vit and SF (n.s.). RF and GH showed the lowest and similar worst values in both groups. The female patients showed a 11% improvement of QoL in Group 1 vs. male patients and a 6% improvement of QoL in Group 2 vs. male patients.

Conclusion Our data show that catheter ablation is resulting in a significant improvement of QoL on values of PF, BP, RE. The cardiac rehabilitation and drug therapy in patients with PSVT reach similar improvement of QoL in values of GH, Vit anf SF. The female patients reported in both groups greater improvement of QoL vs. the male patients.
297: Effect of a combined endurance/resistance training on left ventricular remodelling in patients after a first myocardial infarction
JP Schmid, M Anderegg, M Romanens, C Morger, M Noveanu, G Hellige, H Saner
Swiss Cardiovascular Centre Bern, Switzerland
Background Aerobic endurance training (ET) is safe after an acute myocardial infarction and has been shown to exert a positive effect on left ventricular (LV) remodelling. Concerning resistance training (RT), there is considerable reluctance to apply this training modality, because of concerns of the negative consequences of an increased wall stress as a result of a higher blood pressure load.
Methods At least 4 weeks after a first acute myocardial infarction and an invasively measured ejection fraction < 45%, 47 patients (pts) were prospectively randomized to a combined ET/RT (1 × ET and 2 × RT per week) or an ET alone (3 × per week) during 12 weeks. ET was effectuated at an intensity between 70% and 85% of peak heart rate. RT used a target of 60% of the 1 repetition maximum and 2 sets per session. 17 patients were randomised to the ET/RT group (15 male, 55.3 ± 10.3 years), 21 pat. to the ET group (17 male, 57.0 ± 9.6 years), 9 pat. did not complete the study. At baseline, 3 and 12 months patients underwent a symptom limited cardiopulmonary exercise test and magnetic resonance imaging to assess exercise capacity and LV remodelling.
Results At study entry, EF had increased from 41.2 ± 4.7% to 50.4 ± 12.7%. The VO2 increase after the training programme was similar in the 2 groups (ET/RT: 24.0 ± 4.4 to 26.3 ± 6.2 ml/kg/min., P = 0.068; ET: 23.2 ± 6.0 to 25.1 ± 6.7 ml/kg/min., P = 0.010; difference between the groups: P = 0.725). EDV increased slightly over 1 year in both groups (ET/RT: 206 ± 41 ml to 210 ± 48; ET: 183 ± 44 to 186 ± 52 ml) but without statistically significant differences between the groups (P = 0.914).
Conclusion Compared with an exclusive ET, the combination of ET with a RT does not lead to a more pronounced left ventricular dilatation after a first extensive myocardial infarction.
302: Health outcomes after different rehabilitation programmes in patients with coronary artery disease
Stefan Höfer, Marion Platter, Karl Mayr, Axel Philippi, Alfred Gassner, Helmut Schwann, Kurt Machreich, Werner Benzer
Dept. of Med. Psychology and Psychother., Medical University Innsbruck, Austria
Background Health-related quality of life (HRQL), anxiety and depression are relevant outcome parameters for patients referred to cardiac rehabilitation (CR) programmes. The aim of this study was to identify changes in HRQL, anxiety and depression over time after a 4 week-inpatient CR programme compared with a 6 month-outpatient or no CR programme.
Design The study was carried out as a prospective multicenter study.
Methods All patients (n = 216; mean age 56.3 ± 11 years; 21.3% female), were assessed at baseline, one and three months after initial cadiac event (55% PCI, 15.3% CABG and 29.7% myocardial infarction). HRQL was assessed by the MacNew Heart Disease Quality of Life Questionnaire (MacNew). Depressive and anxiety symptoms were assessed with the Hospital Anxiety and Depression Scale (HADS). 62 patients were treated with inpatient and 87 with outpatient CR programmes, whereas 67 patients did not complete any CR programme.
Results Patients following inpatient CR showed a sharp initial improvement in global HRQL (0.7 ± 0.1 MacNew P <.01) and a decrease in anxiety and depressive symptom scores (1.32 ± 3.01, 1.63 ± 2.6 P < .05). Outpatient CR patients showed a constant improvement in global HRQL (0.31 ± 0.09 MacNew; P <.01) and in anxiety and depression symptom scores (1.23 ± 3.35, 0.84 ± 3.68; P < .01). Patients without CR reported no improvement in global HRQL (0.13 ± 0.1 MacNew; P=ns). After 3 months outpatient patients reported a further improvement of their global HRQL (0.15 ± 0.08 MacNew P= .01). However no further reduction in anxiety and depressive symptoms could be observed.
Conclusions The present study demonstrates the positive short-term effect of a 4 week inpatient CR programme and the positive long term effect of a 6 month outpatient CR programme on HRQL. Therefore the combination of inpatient and outpatient CR programmes is recommended to maintain positive health outcomes in patients with clinical manifestations of coronary artery disease.
304: A novel manualised home based rehabilitation programme for ICD patients improves physical health and activity levels and reduces psychological morbidity and unplanned re-admissions at 6 months
RJP Lewin, S Coulton, H Cox, D Frizelle, G Kaye
University of York, United Kingdom
Background There has been no previous multicentred trial of cardiac rehabilitation for patients with ICDs. Many of these patients have difficulty attending a hospital based programme. This research evaluated a home based programme.in a multicentred, intention-to-treat trial with cluster randomisation of 8 large implantation centres in the UK.
Patients A series of adult patients undergoing implantation with an ICD.
Interventions The control group received usual care. The experimental group usual care plus a rehabilitation programme delivered by a specialist arrhythmia nurse, prior to and immediately after implantation and continuing after discharge through 4 phone contacts over 12 weeks.
Main outcome measures Quality of Life (SF12),% of patients ‘borderline’ or ‘case’ for Anxiety or Depression (Hospital Anxiety & Depression Scale), Activity Limitations (Seattle Angina Questionnaire, SAQ), planned and unplanned admissions to hospital.
Results 192 patients were consented. Multi-level modelling (to take into account the clustered nature of participants within centres) showed differences in the physical component of the SF-12 (mean difference 3.08; CI 1.13 to 5.04) and the physical limitations subscale of the SAQ (mean difference 2.22; CI 0.11 to 7.22) at the 0.05 level in favour of the intervention group. Similarly there was a greater reduction in the intervention group in the proportion with co-morbid depression, reduction of 13.2% vs. 2.1% and anxiety reduction 20.8% vs. 12.7%. Significant differences, intervention vs. control, were also observed in terms of planned ECGs (88.9% vs 66.3%) and unplanned emergency admissions (11.1% vs 24.5%).
Conclusions Rehabilitation provides clinically worthwhile benefits to ICD patients. The ICD Plan, a manualised self-help, home-based programme appears to be a useful tool that could help arrhythmia teams deliver rehabilitation to patients undergoing ICD implantation.
311: Does normalization of a previously ischemic exercise electrocardiography in asymptomatic patients predict a better prognosis than a persistently ischemic response?
CL Calin, C Sinescu, F Pater
“Bagdasar-Arseni” Emergency Hospital-Bucharest, Romania
Objective The aim of this study was to detected if normalization an ischemic ST segment at treadmill exercise in asymptomatic subjects is associated with a better prognosis than if the response test remains ischemic.
Methods We included 176 patients witch effectuated one another exercise EKG test in the last three years. This patients were divided in three groups, based on their ST segment response at treadmill exercise test using Bruce protocol: group 1 = 96 patients with normal ST segment response, group 2 = 51 patients with ischemic response (ST segment is downsloping or horizontal more than 1 mm during or after exercise test), group 3 = 29 patients with ST segment change from an ischemic to a normal response.
Results Patients were follow-up one year for cardiac events: pectoris angina, myocardial infarction or arrhythmia. Risk factors analyzed were: Age-group 1: 52 ± 16; group 2: 62 ± 11; group 3: 65 ± 13; P = 0.0001; Hypertension-group 1: 12%; group 2: 20%; group 3: 26%; P = 0.009; Smoke-group 1: 11%; group 2: 41%; group 3: 27%; P = 0.0001; Cholesterol-group 1: 171 ± 43 mg/dl; group 2: 206 ± 37 mg/dl; group 3: 185 ± 39 mg/dl; P = 0.21; Gender male-group 1: 66%; group 2: 82%; group 3: 74%; P = 0.011.
Events-group 1: 5.6%; group 2: 19.4%; group 3: 6%; P = 0.01. In group 2 the risk of cardiac events is higher than in group 1 or in group 3. Between group 1 and group 3 are not significantly differences for cardiac events, but prognosis for group 3 of patients is more favorable than for group 2.
Conclusion The changes in the aspect of ST segment after treadmill exercise from ischemic to normal is more favorable in time than if persist ischemic response at asymptomatic patients.
314: Lifestyle changes after myocardial infarction
CL Calin, C Sinescu, A Caltea, F Pater
“Bagdasar-Arseni” Emergency Hospital, Department of Cardiology, Bucharest, Romania
Objective The aim of this study was to demonstrated if it possible to change the life style after myocardial infarction (MI).
Methods We included 215 patients (179 male mean age 54 ± 15 years old) who were follow-up one year after MI. The dates were obtained by questionnaire while the periodic control visits.
Results The results are (before vs. after MI): Smoke: 64% vs 19%; Diabetes mellitus: 12% vs 12%; Hypercholesterolemia: 38% vs 9%; Hypertension: 34% vs 6%; BMI: 32 ± 7 m2/kg vs 28 ± 7 m2/kg; HDL-cholesterol: 29 ± 7 mg/dl vs 40 ± 7 mg/dl; Physical activity: 41% vs 72%; Healthy diet: 17% vs 76%. Risk factors: smoke, hypercholesterolemia, hypertension, BMI, HDL-cholesterol were changed during the year after MI. The positive changes in risk factors are particularly explained by increased physical activity, used a healthy diet, increased to use lipid lowering drugs, reduced BMI.
Conclusion Changing life style is difficult to achieve for patients without will who have a reduced physical activity and many risk factors. Most important factors for the success belong company (family, friends, etc.).
316: Extramatch: exercise training meta analysis of trails in chronic heart failure patients: effect of concomitant drug therapy
MF Piepoli, DP Francis, CD Davos, AJS Coats; ExTraMATCH Collaborative
Imperial College School of Medicine, University of London, UK
Objectives ExTraMATCH Meta Analysis has shown that exercise training program significantly reduced mortality and the secondary end point of death or admission to hospital. The effect of concomitant therapy has been unclarified. We aimed to determine whether concomitant therapy may effects the beneficial effect of exercise training program among patients with chronic heart failure and left ventricular dysfunction.
Review methods ExtraMATCH selected randomised trials of an exercise training program versus control in patients with chronic heart failure and left ventricular dysfunction from which results were available before December 2000. Trials had to use a method of randomisation that precluded prior knowledge of the next treatment to be allocated and comparisons had to be unconfounded. The main outcome measures included death, and the combined endpoint of death or hospitalisation for cardiac and non-cardiac cause.
Results Nine data-sets satisfying the entry criteria were identified, including 801 patients. For an average of 213 days of exercise, survival increased by mean 140 days (P < 0.01). The beneficial effect of training was maintained also in CHF patients on ACE-inhibitors (74% of the population) both on survival (HR 0.29, 95%CI 0.7-1.0, P = 0.05) and on the combined endpoints of survival and free from hospitalisation (HR 0.54, 95%CI 0.2-1.0, P = 0.05). Similarly, for beta-blockade, a favourable trend for beneficial effect of the combination of beta-blockade and exercise training, both on survival (HR 0.56) and on the combined endpoints of survival and free from hospitalisation (HR 0.52). However the population on beta-blocker was limited (14.5%) making these differences not significant.
Conclusions Favourable trend for beneficial effect of the combination of beta-blockade and exercise training allows to hypothesise that the benefit of training on survival and hospitalisation reduction may be maintained also in patients under b-blocker therapy.
321: The role of the nurse in cardiovascular risk reduction programmes
S Ünsar, Z Durna
Trakya University Edirne Health College Edirne, Turkey
Coronary artery diseases (CAD) are the major cause of mortality and morbidity in adult people at our country just like the world. After CAD diagnosed, medical, surgical and interventional methods are certain and it needs high cost, but coronary atherosclerosis is a disease which can be prevented or delayed.
Epidemical and clinical trials have demonstrated that modifiable and unmodifiable risk factors lead to CAD. Unmodifiable risk factors include age, sex, family history and race. Major modifiable risk factors include smoking, hypertension, diabetes mellitus, obesity; minor modifiable risk factors include physical inactivity, psychosocial factors, oral contraceptive use etc.
It was determined trials about risk factors interventions for CAD patients provided life expendancy, increased life quality, decreased interventional treatments such as coronary artery bypass grafting and percutaneous transluminal coronary angioplasty and decreased myocardial infarction incidance. The treatment of cardiovascular risk factors is a part of optimal care for people who are under high cardiovascular risk and CAD. The treatment of risk factors suggests collaborative effort of nurses, dieticians, cardiologists, hospitals and health care systems. The nurse has an important role in primary and secondary prevention of CAD. The nurse has a continual and active role in health education in cardiac rehabilitation programmes to be applied in risk reduction factors. The nursing strategies in risk reduction factors are measurement and monitoring of risk factors, counselling and life-style advice, support and encouragement, family support, information regarding treatment regimens.
This article will discuss the important of cardiovascular risk factors and the role of nurse in risk reduction programmes.
326: Improved ventilatory performance at submaximal effort following exercise training in severe CHF patients is independent of improvement in maximal aerobic capacity
R Reuveny, A Pinchas, Z Iakobishvili, R Stein, A Battler, T Ben Gal
Department of Cardiology, Rabin Medical Center, Beilinson Campus, Petach Tikva, Israel
Background Exercise training is known to cause symptomatic improvement in patients with congestive heart failure (CHF) and is accepted as an integral part of treatment in patients with advanced CHF It has previously been shown that CHF patients improve quality of life following exercise training irrespective of improvement in maximal oxygen consumption (VO2).
Aim Since effort dyspnea is a major hallmark of CHF symptoms, we looked for the ventilatory effect at submaximal exercise that can improve symptomatology during daily activity.
Methods 10 patients (9 male), age 56 ± 12 y, LVEF 25% ± 6.7%, were included in the study. All patients underwent 3 months of exercise training twice a week. Cycle cardiopulmonary exercise test, to determine VO2max and the anaerobic threshold (AT), as well as 6 minute walk test (6MW) and Minnesota score were evaluated before and after training. In order to determine the effect of exercise training on ventilatory parameters during submaximal exercise, we compared the slope of the increase in minute ventilation (VE), respiratory rate (RR), and CO2 production (VCO2) during incremental cycling, at matched work rates, before and after exercise training.
Results VO2max, AT, 6MW and Minnesota score before and after training were 12.6 ± 2.6 and 13 ± 3.1 ml/min/kg (P = NS) and 8.5 ± 1.3 and 9.0 ± 1.7ml/min/kg (P < 0.05) and 426 ± 128 and 546 ± 122m (P < 0.001) and 64 ± 15 and 50 ± 14 (P < 0.005) respectively. The slope of the increase in VE, RR, and VCO2 before and after training were 0.499 and 0.458 l/min/watt, 0.359 and 0.307 f/min/watt, and 16 and 14 ml/min/watt respectively (P < 0.001).
Conclusion Exercise training in severe CHF patients resulted in improved ventilatory performance at submaximal exercise, irrespective of the increase in VO2max. The reduced ventilatory demand and improved efficiency may result in less dyspnea during daily activity. A larger scale study to confirm this finding is warranted.
340: Effect of R213g polymorphism of ec-sod gene on endothelial response to exercise in dilated cardiomyopathy
G Otiman, S Dragan, A Anghel, C Marian, S Iurciuc, D Gaita, S Mancas
Dept of Medical Policlinics, University of Medicine and Pharmacy Timisoara, Romania
Background Improvement of endothelial dysfunction(ED) is a main goal of rehabilitation in heart failure. Mutations of eNOS and ecSOD genes accelerate ED and may contribute to an impaired response to exercise. Aim:to evaluate the effect of R213G polymorphism of the ecSOD gene on ED in patients with dilated cardiomyopathy undergoing exercise training.
Methods We studied 60 pts, mean age 59.43 ± 8.41, mean EF 34.26 ± 5.62% divided in 2 groups: grA:30 pts with ischemic cardiomyopathy (IDCM)and grB:30 pts with idiopathic cardiomyopathy (non IDCM), and 30 healthy controls (C) matched for age and sex. Endothelium dependent brachial artery flow-mediated dilation (FMD) was assessed by a protocol previously described by Coretti et al. at baseline and after 30 days. Genotyping of R213G polymorphism was made from leucocitary DNA by PCR. Each group was divided in two equal subgroups according to R213G presence. All pts underwent an intensive daily exercise training program tailored individually, for 30 days.
Results Results are expressed as mean ± SD. Percent FMD represents the change from baseline in brachial artery diameter. Baseline FMD (%) R213G (+): A =-8.05 ± 1.01, B =-7.64 ± 1.11, C = 3.57 ± 0.46 (P <.0001); R213G(−): A= −6.1 ± 0.85, B =-5.49 ± 1.53, C = 6.34 ± 1.43 (P < .0001); FMD at 30 days (%) R213G(+): A= − 7.09 ± 0.89, B= −4.7 ± 1.01, C = 5.86 ± 1.68 (P < .0001). R213G(−): A= 1.4 ± 5.81, B = 4.32 ± 0.77, C = 6.26 ± 1.43 (P < .0001). At baseline, brachial artery reactivity was of vasoconstrictory type in both groups compared to controls. Physical training improved FMD values in the absence of R213G, but did not correct them. The presence of R213G polymorphism significantly reduced the benefit of exercise training on expected improvement of ED. IDCM pts seemed to benefit less than nonIDCM pts from training for improvement of ED.
Conclusions R213G polymorphism may play a key role in the severity of ED of DCM patients and could counteract the benefit of therapeutic interventions on endothelial function improvement.
345: Effect of cardiac rehabilitation on exercise capacity in different subsets of patients with coronary artery disease
F Sampaio, N Bettencourt, P Mateus, M Teixeira, V Gama
Cardiology Department-Centro Hospitalar de Vila Nova de Gaia, Portugal
Background Exercise capacity is a powerful predictor of prognosis in men with known coronary artery disease (CAD). The positive effect of cardiac rehabilitation programs (CRP) on exercise capacity has been reported previously. Whether some subsets of patients with CAD benefit most from regular exercise is still to be determined.
Methods Forty-two patients (mean age 54.57 ± 11.92; 78.6% male) with known CAD referred to a structured CRP, underwent cardiorespiratory exercise testing before and after the program. Exercise capacity was evaluated through peak oxygen consumption (pVO2). We analysed variables that could influence the effect of the CRP on pVO2.
Results Peak VO2 increased significantly after the program in the overall population (from 31.6 ± 8.79 to 33.9 ± 9.01 ml/kg/min; P = 0.003). This increase was not influenced by gender or age. Patients with pVO2 values bellow the median before the CRP increased from 24.9 ± 5.97 to 28.0 ± 7.65 ml/kg/min (P = 0.002), while those with initial pVO2 above the median increased from 38.9 ± 4.3 to 40.3 ± 5.2 ml/Kg/min (P = 0.24). In patients with depressed left ventricular function (ejection fraction (EF) ≤ 45%), pVO2 increased from 28.2 ± 7.93 to 32.3 ± 9.8 ml/Kg/min (P = 0.003); in those with EF>45%, pVO2 increased from 33.3 ± 8.83 to 34.7 ± 8.64 ml/kg/min (P= 0.41).
Conclusion In our population, patients with a worse functional capacity and depressed left ventricular function had a more significant increase in pVO2 after enrolment in a CRP, suggesting that it is in this patients that these programs can have a more significant prognostic impact.
354: Effects of exercise training on cardiac autonomic function in diabetic patients Type II with cardiac autonomic neuropathy
M Pagkalos, E Kouidi, N Koutlianos, G Koukouvou, E Konstantinidou, K Mandroukas, E Pagkalos, A Deligiannis
Sports Medicine Laboratory, Aristotle University, Thessaloniki, Greece
Patients with type II diabetes frequently present cardiac autonomic neuropathy (CAN) which is associated with various cardiovascular disorders both at rest and exercise as well as with limited physical efficacy The purpose of the study was to evaluate the effect of a 6-month training program on cardiac autonomic function in patients with diabetes mellitus type II and CAN. Sixteen patients with CAN according to their Ewing scores for CAN (group A:5 male and 11 female, aged 54.8 ± 5.5 yrs) and 16 without CAN (group B:5 male and 11 female, aged 57.2 ± 5.6 yrs) were included in the study. The mean clinic duration of diabetes in the patients of both groups was 8.9 ± 3.4 yrs and 9.6 ± 4.1 yrs, respectively. All patients followed a 6-month aerobic training program and were submitted at the beginning and the end of the study to physical examination and exercise test with spiroergometric study for the evaluation of their VO2peak. Measures of heart rate variability obtained by both time- and frequency domain analysis of a 24-h ECG recording as standard deviation of NN intervals (SDNN), low (LF) and high (HF) frequency components of the NN intervals.
Results It is concluded that a 6-month aerobic training program leads to an improvement of the functional capacity of patients with type II diabetes. Moreover, it has a beneficial modification of cardiac autonomic regulation in diabetic patients with CAN. Therefore, exercise training should become part of the therapeutic approach of these patients.
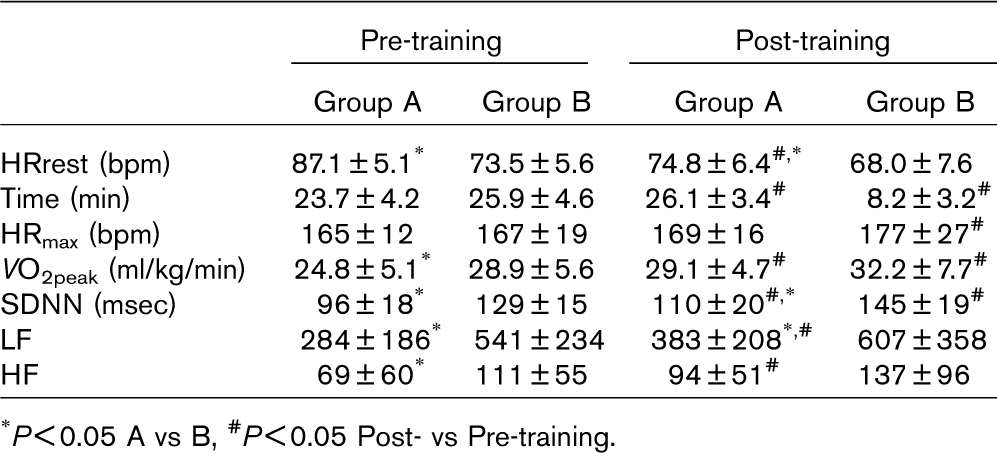
∗P <0.05 A vs B
# P<0.05 Post- vs Pre-training.
369: Predictors of non-adherence to sports in advanced Face III community base cardiac rehabilitation program
DE Iglesias, E Adaniya, A Dalessandro, A Negri, S DePiccoli, N Vainstein, M Khoury, J Thierer
Club de Amigos, Argentina
Background Sports with modified rules can be useful tool in cardiac rehabilitation (CR). Nevertheless, as a difference with callisthenic exercises and aerobic work, adherence has been reported poor.
Objectives The aim of this study was to determinate predictors of non adherence to sports with modified rules (MRS). A cross sectional study was carried out in a group of 140 patients (pts) of a community base CR (Social Club) program. thirty minutes of MRS in each 90 minutes CR session. The program included 3 sessions a week. MRS included were: Swimming, Volley, Football and Tennis.
Results Mean age was 62.82 ± 10, (92.9% males) and mean body mass index (BMI) was 23.69 ± 3.35 kg/m2. 120 patients (85.7%) were on secondary prevention (history of coronary by pass surgery: 25%, myocardial infarction: 47.1%, coronary angioplasty: 31.4% or stable chronic angina: 22.1%); the others were on primary prevention. The prevalence of cardiovascular risk factors (CRF) was: dyslipidaemia 72.1%, hypertension 62.9%, diabetes 10.7% and current smokers 8.6%. Adherence to sports was 71.4%. At the moment of this study, 70.7% of pts were on CR treatment for ≥ year. Univariate analysis showed that age, female sex, wearing glasses, no treatment with beta blockers, stroke, other neurological illness, arthrosis, and low exercise capacity (≤ MET) were predictors of non-adherence to MRS, all with P < 0.001. Left ventricular dysfunction, symptomatic or silent myocardial ischemia, and the BMI failed to predict non-adherence. The only predictor of non-adherence in the multivariate logistic regression analysis was age, OR 1.12 IC 95% 1.04 to 1.20, P < 0.001. Male sex was excluded to the model because it predicts the failure perfectly.
Conclusions Age, that conditioned all the others variables, was the principal predictor of non-adherence to MRS. In the future we should develop modified sports suitable for all ages.
375: Ampelotherapy as a support of postinfarction rehabilitation
Eleonora Vataman, Dorin Lisii, Eugenia Pojoga, Victor Tutuc
Institute of Cardiology, Republic of Moldova
Background We examined whether grape-cure has a positive effect after myocardial infarction (MI).
Materials and methods 150 pts (age 58.1 + 0.7 years, 85% man) with CHF (II-III NYHA class) with previous Q-wave MI were enrolled in cardiac outpatient rehabilitation (COR) program with physical training 4 time per week, 30 min daily, in addition to standard medical treatment. They were randomized into 2 groups:1-grape-cure group (90 pts) and 2-control group (60 pts). At all pts undergoing COR program were evaluated the physical capacity by bicycle ergo meter test, reserve of cardiac function determined by polycardiographic isometric effort test (IET), parameters of remodeling and left ventricular function by echocardiography, lipids, fasting blood glucose, postprandial glucose level, the diagnostic test for glucose tolerance, platelet aggregation study, blood viscosity.
Results It has initially been determined the daily doze of red grapes (700 g) which patients supported without side-effects. Pts in first group showed a significant improvement of exercise capacity after four weeks: duration of exercise increased on 24% (P < 0.05), maximum workload on 20% (P < 0.01). In the I-st group Vcf.cp decreased after initially IET on 18.6% (P <0.05), in the second group—on 19.0% (P <0.01), dp.dt max increased respectively on 20.5% (P < 0.05) and 15.2%, showing essential reduction in reserve function of heart in both groups. After four weeks these parameters were more optimistically in I-st group: after IET Vcf.cp increased on 1.88%, dp.dt max—on 15.6% (P <0.05). In treated group there was a reduction of blood viscosity, a decrease of degree of platelet aggregation and sizes of aggregates. Parameters of glucose tolerance were stable.
Conclusion The four weeks grape-cure on a background of comprehensive cardiac rehabilitation in the second month after myocardial infarction has a positive effect on cardiac performance, blood viscosity, platelet aggregation parameters and glucose tolerance.
381: The training effects of skeletal muscle strength and muscle volume to improve functional capacity in heart failure patients
Kida Keisuke, Akashi Yoshihiro J, Osada Naohiko, Suzuki Kengo, Tamura Masachika, Inoue Koji, Seki Atsushi, Samejima Hisanori, Omiya Kazuto, Miyake Fumihiko
St Marianna University School of Medicine, Japan
Background Nowadays, exercise training is widely accepted as a method to improve functional capacity in cardiac patients. However, the influence of skeletal muscle strength and volume to improve function capacity in heart failure patients is not fully clarified.
Purpose This study was designed to evaluate the strength and volume of the skeletal muscle related to the improve function capacity in heart failure patients.
Methods The subjects were 19 heart failure patients, including 10 with dilated cardiomyopathy and 9 with ischemic cardiomyopathy. Maximum knee extension strength (PT), which is an index of muscle strength, was measured by Biodex. The skeletal muscle volume (MV) was determined according to the electrical impedance analysis. All patients underwent symptom-limited cardiopulmonary exercise testing (CPX) using ergometer according to the ramp protocol. Exercise training was performed for 6 months. Delta values were calculated by the value of the 1st month (1M) deducted from that of the 6th month (6M).
Result The PT revealed no change from the 1M to the 6M. The MV showed a tendency to increase from the 1M to the 6M. The peak VO2 was significantly increased from 20.7 ± 4.7 to 22.5 ± 5.8 Nm/kg (P < 0.01). There was positive correlation between the delta peak VO2 and delta PT (r = 0.51, P < 0.05). However, there was no correlation between the delta peak VO2 and delta MV.
Conclusion In this study, the improvement of functional capacity in heart failure patients who are assumed in the deconditioning status is greatly influenced by the increased lower leg muscle strength, not by the muscle volume.
383: Effect of cardiac rehabilitation on medical resource utilization in patients with coronary heart disease
Choi Jin-Oh, Sung Jidong, Choo Jina, Jang Mija, Park Won-Hah, Hong Kyung Pyo
Department of Medicine, Sungkyunkwan University School of Medicine, Republic of Korea
Background Cardiac rehabilitation (CR) improves functional capacity and cardiovascular outcome in patients with coronary heart disease (CHD). However, there have been few studies on cost-effectiveness of CR. The aim of this study is to evaluate whether CR can reduce the medical resource utilization such as readmission and emergency room (ER) visit in patients with CHD.
Methods Among 3099 patients who were admitted and diagnosed as having CHD between 1994 and 2001, 128 patients were enrolled in CR program in Samsung Medical Center, Seoul, Korea. We defined the other 2971 patients who were not enrolled in CR program as the control group. We obtained data on clinical characteristics, total number of readmission, total duration of hospitalization, and total number of ER visits.
Results Diagnosis of acute myocardial infarction were more frequent in CR group (61.7% vs 28.7%, P < 0.001), mean age was slightly higher in control group (60.8 ± 9.7 vs 56.4 ± 10.4, P < 0.001), and the number of diseased vessels did not differ between groups. Mean duration of follow-up in CR group was longer than that of control group (5.4 ± 2.1 vs 4.7 ± 2.9 years, P < 0.001). In CR group, total number of readmission was smaller (1.0 ± 1.2 vs 1.3 ± 1.8, P=0.001), total duration of hospitalization was shorter (4.7 ± 8.3 vs 10.2 ± 26.2, P < 0.001), and total number of ER visit was smaller (1.1 ± 1.7 vs 1.7 ± 2.5, P < 0.001) than that of control group. In multivariate analysis, numbers of readmission and ER visit were significantly smaller (P < 0.05) in CR group than in control group after adjustment for age, sex, clinical diagnosis, number of diseased vessels, and follow-up duration.
Conclusion Enrollment in CR program was associated with reduced medical resource utilization during the follow-up, which probably can results in favorable cost-effectiveness in CHD management. Full economic analysis of CR is warranted.
390: The training effects of skeletal muscle strength and muscle volume to improve functional capacity in cardiac patients
Kida Keisuke, Akashi Yoshihiro J, Osada Naohiko, Suzuki Kengo, Tamura Masachika, Inoue Koji, Seki Atsushi, Samejima Hisanori, Omiya Kazuto, Miyake Fumihiko
St Marianna University School of Medicine, Japan
Objective This study was designed to evaluate the strength and volume of the skeletal muscle related to the improvement of function capacity in cardiac patients.
Methods The subjects were 83 cardiac patients, 63 with previous myocardial infarction (MI) and 20 with postoperative heart disease (Post OP) including 12 with CABG and 8 with operative valvular disease. Maximum knee extension strength (PT) was measured by Biodex and skeletal muscle volume (MV) was obtained according to the electrical impedance analysis (BIA: ART HAVEN 9 C.O.). Exercise training was performed for 6 months after the onset of MI or the surgery, and all patients underwent symptom-limited cardiopulmonary exercise testing (CPX) using treadmill according to the ramp protocol at the 1st (1M), 3rd (3M) and 6th month (6M) from the begging of exercise training.
Result The PT at the 1M in MI group was 1.75 ± 0.48 Nm/kg and increased to 1.91 ± 0.53 Nm/kg (P < 0.0001) at the 3M. It showed a tendency to increase from the 3M to the 6M. The MV revealed no change from the 1M to the 3M however, it tended to increase from the 3M to the 6M in MI group. The peak VO2 was significantly increased from 26.1 ± 5.2 at the 1M to 28.8 ± 6.2 Nm/kg (P < 0.0001), however, it exhibited no change from the 3M to the 6M in MI group. The PT at the 1M in Post OP group was 1.60 ± 0.28 Nm/kg and increased to 1.78 ± 0.33 Nm/kg (P < 0.005) at the 3M. It showed a tendency to increase from the 3M to the 6M. The MV at the 1M in Post OP group was 18.2 ± 3.7 kg and increased to 18.8 ± 3.6kg (P < 0.0001) at the 3M, 19.4 ± 3.6kg (P < 0.0001) at the 6M, respectively. The peak VO2 was significantly increased from 22.6 ± 4.1 at the 1M to 24.8 ± 3.8 Nm/kg (P < 0.0001), however, it exhibited no change from the 3M to the 6M in Post OP group.
Conclusion These results suggest that the skeletal muscle strength may be a main determinant of exercise capacity which has been considered to reflect composition changes rather than skeletal muscle volume in cardiac patients.
391: Determinants of patient compliance in an ambulatory cardiac rehabilitation setting
J Berger, V Reenaers, D Hansen, J Vaes, R Geukens, P Dendale
Rehabilitation and Health Centre, Heart Centre, Virga Jesse Hospital, Hasselt, Belgium
Background Effectiveness and benefits of CR programmes are well described. Nevertheless, still an important fraction of eligible cardiac patients do not attend or drop out early after referral by their cardiologist.
Objective We tried to identify predictors contributing to non-attendance and drop out in a multidisciplinary CR setting in patients after hospital discharge.
Methods From a total of 879 eligible patients, 479 were not referred to the multidisciplinary cardiac rehabilitation programme. From the 400 patients referred and enrolled we have sufficient data on 355 (88.75%) concerning their baseline characteristics and risk factors. Effectively, 261 (73.5%) (197 m, 64 w, mean age 62 y) completed the 3 month programme in contrast with 94 patients (68 m, 26 w, mean age 64 y) who were referred did not start up their cardiac rehabilitation program or dropped out within 2 weeks. Various clinical variables were measured: age, gender, medical diagnosis, cardiac history, BMI, systolic and diastolic blood pressure, diabetes, blood lipids and smoking habits.
Results A multiple logistic regression analysis was used to determine the biomedical predictors of non-attendance or early drop out. Predictors of patient compliance:
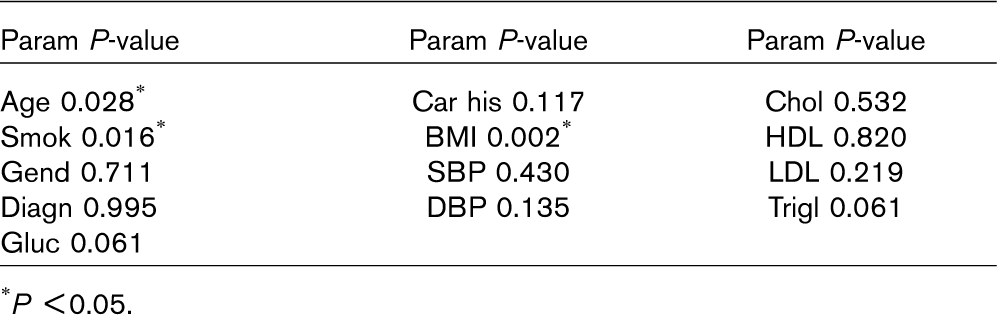
∗P <0.05.
Conclusions Non-attendance and drop out are significantly associated with old age, smoking habits and overweight. Further analysis of psychosocial variables certainly is needed. Strategies to improve referral patterns and adequate approaches for patient retention should be developed.
397: The comparison of in-hospital cardiac rehabilitation course and early exercise testing parameters in patients with acute myocardial infarction treated with primary angioplasty or thrombolytic therapy
I Swiatkiewicz, A Krakowska, J Kubica, M Kozinski, A Sukiennik, W Krupa, L Ludwikowska, R Dobosiewicz, E Zabielska, A Kubica
Dept.of Cardiology and Int. Diseases of Collegium Medicum, Bydgoszcz, Poland
Background Primary angioplasty (PTCA) is now preferred but not widely approachable reperfusion treatment method for ST elevation acute myocardial infarction (STEMI).
Aim To compare the course of early in-hospital cardiac rehabilitation (CR) and early exercise testing (ET) parameters in patients with STEMI treated with PTCA or thrombolytic therapy (TT).
Material and methods In a retrospective manner we analysed outcomes of postinfarction CR in 150 patients: 50 consecutive patients treated with TT and 100 patients undergoing PTCA matched according to demographic and clinical factors. All patients fulfilled a three stage CR programme applied in our centre. The parameters of exercise treadmill test and selected echocardiographic indices at discharge were assessed.
Results In comparison to TT group in the group of patients treated with PTCA CR was initiated earlier, patients faster reached next stages of CR and the hospitalisation stay was significantly reduced. No remarkable differences in heart rate, systolic and diastolic blood pressure during the following stages of rehabilitation and discharge echocardiographic parameters (ejection fraction, left ventricular end-diastolic diameter and degree of mitral insufficiency) were observed between populations. Subjects treated with PTCA earlier underwent an exercise treadmill test, were less likely to have ET positive result and achieved significantly higher workload.
Conclusions In patients after STEMI treated with PTCA CR was implemented earlier and was conducted more intensively what resulted in earlier performance of ET and shorter hospitalisation stay. Despite shorter CR period, patients treated with PTCA presented higher exercise capacity and significantly rarely demonstrated a positive result of ET At discharge there were no significant differences in ejection fraction between STEMI patients treated with PTCA or TT and systolic function of left ventricle assessed with echocardiography was preserved in both groups.
398: The relationship of six-minute walk distance to VO2peak and VT after exercise training in elderly diastolic heart failure patients
S Maldonado-Martin, PH Brubaker, JB Moore, KP Stewart, DW Kitzman
Faculty of Physical Activity and Sport Sciences, University of Basque Country, Spain
Objective To evaluate the change in six-minute walk test (6-MWT) relative to changes in peak oxygen consumption (VO2peak) and ventilatory threshold (VT) after 16-weeks of exercise training (ET) in older diastolic HF (DHF) patients.
Methods Older patients (> 65 years) with isolated DHF (n = 47), performed an exercise test to peak exertion on an upright bicycle ergometer using an incremental protocol. Gas exchange measures were collected along with continuous electrocardiograph monitoring. 6-MWT was performed on an indoor track at a self-selected pace under standardized conditions. During the 16-week intervention period the exercise group (EG) took part in ET program, (50-70% of VO2peak as exercise intensity), while the control group (CG) continued with their regular activities. All tests and measurements were performed in both groups at entry and after the study period.
Results There were not statistical differences between CG and EG at baseline in VO2peak, VT, 6-MWT At follow-up, 6-MWT distance was significantly higher (P < 0.05) than at baseline test in both CG (9%) and EG (11%), but the VO2peak and VT values were only significant increased in the EG after ET (19% and 11%, respectively). In addition, 6-MWT, VO2peak and VT were significantly higher in EG when compared to the CG at the follow-up tests. The mean changes in VO2peak and VT were not significantly correlated with the mean change in 6-MWT after ET in either the CG or EG.
Conclusion 6-MWT is not a useful predictor of VO2peak, questioning the validity of 6-MWT to evaluate the exercise intolerance in elderly DHF patients. In addition, the 6-MWT had a significant practice effect after 16-week of intervention and questions the validity of this test to evaluate in functional capacity in this population. In contrast, VO2peak and VT demonstrated an appropriate training effect and support the use of these variables as outcome measures for older DHF patients.
414: General practitioners referral of cardiac patients to cardiac rehabilitation
M Daly, J Hussey
School of Medicine, Trinity College Dublin, Ireland
Internationally there are many initiatives to increase secondary prevention of coronary heart disease. In Ireland an example of such a programme is the Heartwatch Scheme which was set up to expand rehabilitation at a community level by providing support for general practitioners (GPs) to perform an initial cardiovascular disease risk evaluation on patients with coronary heart disease. Approximately 20% of GPs are part of the scheme.
The objectives of this study included: to determine the percentage of GPs in Dublin that referred patients to cardiac rehabilitation (CR); to determine the type of rehabilitation patients were referred to; and to investigate if GPs are more likely to refer certain patients to CR. In addition reasons for non-referral were examined as were perceived barriers to referral.
Fifty percent of GPs in Dublin were sent a questionnaire after an introductory phone call. The return rate was 68% (161 out of 237) and 24% of the total who replied were Heartwatch GPs. Forty nine percent of GPs (n = 80) referred patients to cardiac rehabilitation and of this group 59% referred to hospital based CR, 55% referred to practice based CR and 3% to community CR. In terms of those who referred patients to CR, 48% were Heartwatch GPs. Referral to practice based CR was found in 46% of Heartwatch GPs compared to 9% of non-Heartwatch GPs.
One of the main reasons for non-referral was that GPs believed hospital staff automatically referred suitable patients. The majority of GPs requested establishment of specific guidelines on the referral procedure and notification on the availability of CR in hospitals and in the community.
The results of this study indicate a need for guidelines for GP referral to CR and a need for improved communication links between GPs and hospital CR teams. The Heartwatch Scheme appears to be successful in terms of encouraging secondary prevention.
416: Exercise training for heart failure patients: etiology makes a big difference
Jannicke Bruvik, Hans-Halvor Bjørnstad, Berith-Laila Hjellestad
Haukeland University Hospital, Division of Cardiology, Bergen, Norway
Method A randomized, clinically controlled trial. The intervention group had resistance-, endurance- and respiratory training 45 minutes 3 times per week for 20 weeks, while the control group did not have any organized training.
Results All patients completed the training period. Three of the patients in the training group improved NYHA class from III to II. (MLHFQ = Minnesota Living With Heart Failure Questionnaire, SF-36 = Short Form 36).
Conclusion The training group had a positive effect in physical and emotional variables. Women improved walking distance, men improved emotional health. Non-ischemic heart failure patients improved both physical and emotional variables, but ischemic patients had no significant improvement in any of the variables and need another approach.
422: Exercise training in patients with chronic heart failure-effects of two different regimes on the maximum strength of the quadriceps femoris
L Karatzanos, A Karaseridis, V Georgiopoulou, D Sakellariou, F Katsaros, E Tsagalou, S Nanas
Cardiopulmonary Rehabilitation Centre, Evgenidion Hospital, University of Athens, Greece
Background This study was designed to examine the effects of a program included strength training on the maximal strength of the quadriceps femoris in chronic heart failure (CHF) patients.
Method 14 stable CHF patients [(M ± S) 56.4 ± 9.6 years, VO2peak:16.2 ± 6.7 ml/kg/min] participated in an exercise training program for 12 weeks, 3 times/week. Participants were randomly assigned to either aerobic (AER, n = 6) or combined regime (COM, n = 8), which included aerobic and strength training. Aerobic exercise was performed in interval type on cycle ergometers. Strength training involved exercises for various muscle groups, including quadriceps femoris. Both regimes were of the same duration.
Maximum strength of each leg quadriceps femoris was evaluated at the beginning and the end of the program with 2-repetition maximum (2-RM) test, which is the maximum resistance to overcome with two repetitions. All participants were familiarised with the procedure before the measurements.
Results In relation to right leg, all participants improved the 2-RM test performance (from 18.5 ± 6.2 kg to 23.9 ± 9.1 kg, P < 0.05). However, the improvement of the COM group (from 20.1 ± 7.5 kg óε 29.3 ± 8.1 kg) was significantly larger than that of the AER group (from 16.3 ± 3.1 kg to 16.8 ± 4.1 kg) (P < 0.05). Concerning left leg, the whole cohort increased performance (from 17.1 ± 4.7 kg óε 22.7 ± 7.5 kg, P < 0.05), but the increase of the COM (from 18.8 ± 4.8 kg óε 27.0 ± 6.3 kg) was much higher than the AER (from 15.0 ± 3.8 kg óε 17.0 ± 4.7 kg) (P <0.05).
Conclusion A combined program of aerobic and strength training seems to improve the maximum strength of quadriceps femoris to a much larger extent than a mostly aerobic regime. This hypothesis needs to be further investigated in larger sample. It is worth noted that, in concern to haemodynamic components and the cardiac rhythm, no derangements were observed during the strength training part of the program.
430: Systematic screening and socially differentiated rehabilitation programme facilitate high participation rate among MI patients
LK Meillier, ML Larsen, FB Larsen, K Lind, DG Andersen, B Gustafson; for the Aarhus Rehab-group
Aarhus University Hospital, County of Aarhus, Denmark
Objectives To prevent social inequalities in prognosis after MI, by offering a socially differentiated comprehensive rehabilitation programme (CRP). The objective of the present study was to facilitate a high participation rate among myocardial infarction (MI) patients by; 1) develop and implement a systematic screening procedure to identify all hospitalised first incidence low SES MI patients and, 2) to allocate high SES MI patients to basic CRP, and low SES MI patients to extended CRP.
Methods In-patient register was checked for new hospitalised MI patients, and referral procedures were initiated for patients with significant EKG-changes or with TnT>0.10 u/l or CKMB > 10.0 μ/l. First incidence MI-patients aged ≤ 75 years were referred to basis CRP if they were living with a partner and had a high level of education. Extended CPR was offered to all patients with low level of education, middle education ≤ 55 years or if the patient was living alone, regardless of level of education. Individual basic and extended CRP for 6-8 weeks was initiated preferable within two weeks after discharge. Cohabitant or other near friend was invited to join. Patients were recruited in the period of September 1st 2002, to December 31st 2004.
Results 388 MI patients ≤ 75 years were hospitalised at Aarhus University Hospital in Denmark, having a first incidence MI. 86% (n = 333) of all first incidence MI patients were referred to CRP. 1.5% (n = 6) dismissed, 3.1% (N = 12) did not attend and 1.3% (N = 5) were participating in CRP at another hospital after CBP. 80% (N =310) attended a socially differentiated CRP almost equally distributed among basic (N = 156) and extended CRP (N = 154). Non-attenders were equally distributed among basic and extended CRP. 92% of the attending patients completed the full programme, including a 1-year follow up.
Conclusion It is possible to find and motivate a very high percentage of MI patients to participate in a socially differentiated CRP.
431: Screening for cardiovascular risk factors in relatives of patients with premature heart disease
A McGowan, M O'Reilly, D Murray, A Samad, J Gormley
Cardiac Rehabilitation Department, Sligo General Hospital, Sligo, Ireland
Background Coronary Heart Disease (CHD) remains the leading cause of mortality in Ireland. A positive family history is independent of other coronary risk factors increasing risk, with a further increase for those whose first-degree relatives have an earlier onset of premature CHD. The European Society on Coronary Prevention recommend screening of risk-factors in first-degree relatives of patients with premature CHD for risk factors, but these recommendations are poorly met.
Methods The first-degree relatives of 59 patients with premature CHD were invited for screening of the following CHD risk-factors-fasting lipids and glucose, blood pressure, tobacco smoking, BMI and physical activity levels. Advice was given based on findings and results sent to their Family Doctor. One year later these subjects were retested.
Results A total of 58 off-spring and 30 siblings (males n = 40, females n = 48) were screened. Abnormal lipids were found in 40% of males and in 33% of females. Hypertension was recorded in 2.5% of males and 4.2% of females, and 65% of males and 54% of females had a BMI > 25 kg/m2. Cigarette smoking was reported by 45% of males and 42% of females. Low physical activity levels during sport and leisure were reported by 80% of males and 71% of females. One year later 66 subjects (males n = 30, females n = 36) re-attended (response 75%) for repeat screening. In males abnormal lipid profiles had decreased by 6.7%, cigarette smoking levels decreased by 2% and physical activity levels increased by 32%. However there was an 18% increase in those with a BMI > 25 kg/ m2. In females lipid profiles deteriorated by 2.7%, BMI > 25 kg/m2 increased by 1.6% and cigarette smoking decreased by 3% but physical activity levels increased by 8.3%.
Conclusion High levels of modifiable risk factors were shown in these subjects. The education programme yielded modest improvement in risk factor profiles. An intensive education programme is required for this at-risk population.
438: A positive result for depression with the hads questionnaire is not predictive for an increased cardiovascular risk after coronary angiography in Swiss patients
Cyrille Frei, Jean-Paul Schmid, Stefan Gutknecht, Urs Borner, Hugo Saner
Swiss Cardiovascular Centre Bern, Switzerland
Background Major depression (MD) is a recognized cardiovascular risk factor. The aim of this study was to evaluate the predictive value of two screening instruments for depression including the “Hospital Anxiety and Depression Scale” (HADS) and the “General Depression Scale” (ADS-L) in regard to cardiovascular complications during follow up after coronary angiography.
Methods 305 consecutive patients (pts) referred for coronary angiography to the University Hospital Inselspital Bern completed the HADS and the ADS-L questionnaire. These pts were contacted 12-18 months later and evaluated in regard to recurrent cardiovascular events and mortality.
Results Out of the 305 patients 248 (81.3%) could be contacted and did answer the follow-up questions; 12 patients (3.9%) died during follow-up. 10/39 patients with positive HADS-D had a recurrent cardiovascular event whereas 53/221 pts with a negative HADS-D had a cardiovascular event (P = 0.482). 29/87 pts with positive ADS-L and 37/173 pts with negative ADS-L had a cardiovascular event during follow-up (P = 0.089). The result does not change the predictive value if we consider only those patients with significant coronary atherosclerosis during angiography (HADS-D: P = 0.508; ADS-L: P = 0.062).
Conclusions A positive screening for depression using HADS-D or ADSL using the common “cut off” point of 8 but also a higher “cut off” of 12 score points had no significant predictive value for an increased cardiovascular risk during the period of 12-18 months after coronary angiography. These results are in contrast to the results from earlier studies in other countries. There is a need for further research in regard to the contradictory results.
447: Gender differences in quality of life of cardiac rehabilitation patients
R Goud, N Peek, IM Hellemans
Academic Medical Center, Amsterdam, Netherlands
Background Evaluation of quality of life at the baseline of cardiac rehabilitation (CR) is nowadays recommended, since the psychosocial status of the patient is an important success factor in CR. In the Netherlands about 60-70% of CR centers now use the Quality of Life after Myocardial Infarction (QLMI) questionnaire as a needs assessment instrument at CR baseline.
Objective To examine differences in quality of life between males and females measured at CR baseline.
Methods Demographic, QLMI, and clinical data were prospectively collected for all patients admitted to 8 Dutch CR centers during a period of six months in 2005. All data were collected using an electronic patient record, and randomly validated with independent sources afterwards.
Results Data from 1530 patients were collected; 1388 patients (91%; 1051 males and 337 females) filled in the QLMI questionnaire. The mean total score of the QLMI was 121.6 (± 23.6) out of 168. The mean scores for the physical, social and emotional domain of the QLMI were 47.8 (± 11.2, max 70), 37.5 (± 7.5, max 49) and 55.5 (± 12.6, max 77). Female patients scored significantly lower than male patients (P < 0,001, Mann-Whitney U test) on all domains of the QLMI (total score 114.9 vs. 123.7; physical 44.9 vs. 48.8; social 35.9 vs. 38.0; emotional 51.9 vs. 56.7). These results were corrected for differences in age, smoking status, body mass index, and diagnosis/intervention.
Conclusion Female patients' quality of life at CR baseline is worse than that of male patients, in particular on the emotional domain. We conclude that in women cardiac health problems have a greater impact on quality of life than in men. The difference could be partially explained by a referral bias.
451: The anti-inflammatory effects of long-term systemic exercise on patients with type 2 diabetes mellitus and metabolic syndrome
N Kadoglou, D Perrea, F Iliadis, N Angelopoulou-Sakadami, C Liapis, M Alevizos
“Pythagoras I” project and Propondis Foundation Department of Vascular Surgery University of Athens, Greece
Objective To determine the effects of a long-term exercise training program on novel cardiovascular risk factors in patients with type 2 diabetes mellitus (NIDDM) and metabolic syndrome (MS).
Methods Sixty patients (26 males, 34 females) with NIDDM and MS, but with inadequate glycemic control (HbA1c > 7%) were included in the study. All the participants were overweight (BMI > 27 kg/m2), aged 44-67 (60.64 ± 8.59), without micro-macro-vascular complications. None was receiving lipid lowering medication, but all participants were on anti-diabetic regimen with metformin and/or sulphonylurea. At baseline and at the end of the study all the patients performed a graded incremental exercise test on ergocycle and blood samples were drawn to determine FPG, HbA1c, total cholesterol, HDL, LDL, triglycerides, hsCRP, IL-10 and IL-18. Half of them were randomly assigned to a supervised exercise training program (3 times/week, 45 min/session, 60-85%VO2max) for 14 weeks. The rest of patients served as a control group.
Results At the end of the study exercise training resulted in a significant reduction of FPG (−16.58 ± 3.42; P < 0.001), HbA1c (−0.61 ± 0.44%; P < 0.001), total cholesterol (−19.4 ± 16.35 mg/dl; P = 0.012), LDL (−26.78 ± 2.17; P = 0.011), triglycerides (−14.7 ± 3.56 mg/dl; P = 0.009), and a considerable increment of HDL (3.17 ± 3.21 mg/dl; P = 0.007) and VO2max (3.69 ± 0.26 ml/kg/min; P = 0.001) in comparison to the control group. Moreover exercise training conferred a significant decrease of novel inflammatory factors levels such as IL-18 (from 375.15 ± 212.74 to 223.7 ± 176.76pg/ml; P = 0.018), hsCRP (from 0.52 ± 0.15 to 0.33 ± 0.23 mg/dl; P = 0.028), while IL-10 increased in both groups (P> 0.05). With the exception of IL-10, between-groups comparison showed exercise-induced anti-inflammatory effects (P < 0.05).
Conclusions Exercise training of patients with NIDDM and MS significantly improved glycemic control, lipid profile and cardiorespiratory fitness along with reductions of novel inflammatory markers.
453: Endothelial dysfunction in patients with coronary artery disease and hypertension
LV Yankouskaya
Grodno State Medical University, Grodno, Belarus
Objective The aim of the study was to evaluate endothelial function in patients with coronary artery disease (CAD), and in patients with CAD in combination with arterial hypertension (AH) second degree.
Design and methods The study population included 57 patients with stable CAD and 20 healthy volunteers. The patients with CAD were divided into four groups: group A included 16 patients with CAD I class, B-19 patients with CAD I class in combination with AH II degree, C-8 patients with CAD II class, D-14 patients with CAD II class in combination with AH II degree. The forearm blood flow (FBF) was measured using strain-gauge plethysmography during reactive hyperemia and after sublingual nitroglycerin administration. Plasma nitrite plus nitrate level was determined using the Griess method. The patients were treated with the atenolol, enalapril, aspirin, molsidomin. Two weeks after the treatment the same examinations were performed.
Results FBF during reactive hyperemia reduced in groups with disease progress (group A −15.58 ± 1.64%, B-12.87 ± 1.56%, C-8.55 ± 0.66%, D-8.22 ± 1.71%). Endothelial-dependent vasodilatation was significantly lower in groups C (72.4%; P < 0.001)and D (73.4%; P < 0.001) to compare to that both in healthy subjects and in patients of group A (C-45.1%; P < 0.05 and D-47.2%; P < 0.05). FBF in all groups after treatment increased, however, kept lower to compare with healthy subjects (P < 0.05).
FBF after sublingual nitroglycerin administration was similar in A, B, C groups. However, in most severe group D, it was lower (28.18 ± 1.78%, P < 0.05) compare to that in healthy subjects (35.04 ± 2.03%). The plasma nitrite and nitrate level in patients of all groups was significantly lower than that in control subjects (P < 0.01).
Conclusions Our studies show that patients with stable CAD have disturbed endothelial function and usual pathogenic treatment is not effective for it recovery. It is very impotent to diagnose atherosclerosis in its asymptomic stage.
459: Additional benefit of exercise training in patients with cardiac resynchronization therapy
M Courregelongue, P Bordachar, S Brette, S Lafitte, R Roudaut, J Clementy, H Douard
Haut Leveque hospital, Pessac, France
Background Both biventricular pacing (BVP) and exercise training have been demonstrated to improve exercise tolerance in patients with severe heart failure. Little is known about the potential additional benefit of exercise training in heart failure patients with cardiac resynchronization therapy.
Methods Thirty-four patients with severe heart failure and ventricular conduction delay were implanted with a multisite device. Fifteen patients were randomly assigned to the exercise group (BVP +, exercise +) and underwent a 4 to 8 weeks training program including cycle ergometer and callistenics exercises 1 month after implantation. The other 19 patients were assigned to the control group (BVP +, exercise -). A quality of life questionnaire, a cardiopulmonary exercise testing and a 6-minutes-walking-test were performed before implantation and after 1, 3 and 6 months.
Results Twelve patients in the training group and 14 patients in the control group completed the 6-months follow-up. No significant cardiovascular event occurred during the training sessions. After 6 months of BVP, the improvement in peak VO2 was higher in the training group compared to he control group (+ 4.2 ± 2.1 versus + 1.9 ± 1.6 ml/kg/mn; P = 0.05). Similarly, the improvement in the distance walked during 6 minutes was significantly higher in the training group (+ 103 ± 31 versus + 47 ± 27 m; P = 0.003). No significant difference was observed between the 2 groups in terms of quality of life (P = 0.57).
Conclusion Exercise training can safely be performed in patients with heart failure and cardiac resynchronization therapy and allows a substantial additional improvement in functional capacity.
468: Effects of a comprehensive cardiac rehabilitation program in myocardial infarction elderly patients
E Rivas-Estany, J Barrera Sarduy, J Alvarez Gómez, S Sixto Fernández, S Hernández García, M Martínez Ramos, M Díaz Vazquez
Institute of Cardiology and Cardiovascular Surgery, Havana, Cuba
In the last decades there have been remarkable increases in the growth of the old population throughout the world. Elderly patients are at high risk of disability following a coronary event or heart failure. Multifactorial cardiac rehabilitation (CR) in these circumstances has gained increasing acceptance.
To assess the effects of a comprehensive CR program in elderly patients with myocardial infarction (MI), we included 61 cases of both sexes aged more than 65 years. They had a mean age of 69.3 years and 41% were more than 70. Patients were tested through exercise stress test and rest/exercise isotopic ventriculography at 2, 3 and 12 months of evolution after MI; serum cholesterol was also determined at these intervals. PWC showed a significant increasing from 64 ± 23 to 86 ± 24 W (26%) (P < 0.001); other functional ergometric variables had similar behaviour. Mean rest left ventricular ejection fraction was 49 ± 11% without significant change with exercise or in the subsequent tests. Serum cholesterol and triglycerides showed a tendency to decrease till the end of follow-up. There were not complications during exercise training sessions. Patients had a morbidity of 29% and a cardiac mortality of 3.3% during the mean time of 32 ± 23 months of following-up.
It was confirmed an increasing of quality of life without further risk in this group of elderly MI patients adhered to a comprehensive CR program. They also showed similar behaviour and beneficial physiologic response than younger patients.
470: Long-lasting physical exercise and ventricular remodeling after anterior wall myocardial infarction
E Rivas-Estany, S Sixto Fernández, R Stusser Beltranena, J Alvarez Gómez, J Barrera Sarduy, S Hernández García, M Martínez Ramos, M Díaz Vázquez
Institute of Cardiology and Cardiovascular Surgery, Havana, Cuba
The beneficial effects of comprehensive cardiac rehabilitation and secondary prevention in patients with coronary artery disease are well documented. Physical exercise is currently recommended for patients after myocardial infarction (MI), however its effects on ventricular size and remodeling have to be precised. The aim of our study was to assess the effects of a long-lasting physical training program on left ventricular function and remodeling after MI.
In an observational study we included 90 patients with anterior transmural MI (mean age: 55 ± 10 years), 41% of them with severe left ventricular dysfunction (LVEF <40%); they were assigned to a supervised physical training program lasting one year at least (exercise intensity: 60-80% of heart rate reserve).
Functional capacity increased from 73.4 ± 20% to 85.3 ± 19% and maximal oxygen consumption from 18 ± 4 to 21.7 ± 4 ml/kg/min in the ergospirometry bycicle test, similar significant increases showed other ergometric parameters evaluating physical fitness. 54% of patients had exercise-induced ST segment depression in the two-month ergometry evaluation, only 29% had it in the six-month test. Neither cardiothoracic X-ray index, end-diastolic and end-systolic diameters nor LVEF, assessed by rest/stress echocardiogram or radioisotopic ventriculography showed significant change in the follow-up.
Patients had a mean total mortality of 11.1%, with a cardiovascular mortality of 8.9%, and a morbidity of 16.7% during a mean following-up time of 36.3 ± 17 months.
It was concluded that long-term exercise training did not show adverse effects on left ventricular remodeling and function. Post-MI patients obtained an increasing of work capacity and other parameters reflecting quality of life.
474: Angiotensin II type 1 receptor gene a1166c polymorphism affects aerobic power response to training in coronary artery disease
J Defoor, B Raman, K Martens, G Matthijs, R Fagard, L Vanhees; CAREGENE Study
K.U. Leuven, Leuven, Belgium
Background Aerobic phenotypes show wide variability to similar aerobic training stimuli, which is partly attributed to heritability. The Angiotensin II type 1 receptor (AGTR1) gene is the major mediator of the effects of Angiotensin II, which has been shown to be involved in the determination of aerobic power. The aim was to evaluate whether the AGTR1 gene A1166C single nucleotide polymorphism (SNP) is associated with aerobic power or with its response to training in patients with coronary artery disease (CAD).
Methods All biologically unrelated Caucasian patients with CAD who had achieved maximal exhaustion during incremental bicycle testing at baseline and after completion of three months of cardiac rehabilitation from 1990 through 2001 (n = 1095) were eligible for inclusion in the CAREGENE Study. 935 blood samples were obtained for DNA-analysis. In 927 patients the AGTR1 gene A1166C SNP was identified by sequenom MassARRAY RT technology (Lark technologies, Essex, UK).
Results Frequencies of the AGTR1 gene A and C alleles were 0.71 and 0.29, respectively. Covariate-adjusted aerobic power (ml/min/kg) at baseline was comparable (F = 2.43, P = 0.08) for patients homozygous for the wild-type A allele (22.5 ± 0.2), heterozygous (22.1 ± 0.1), and homozygous for the mutative (rare) C allele (21.3 ± 0.6) (mean ± SE). Aerobic power increased significantly (P < 0.001) for each genotype with physical training. The adjusted response of aerobic power to training tended to be larger (F = 2.64, P = 0.07) in patients homozygous for the mutation (28.0 ± 2.2%) as compared with the AA (23.1 ± 0.8%) and AC (25.0 ± 0.9%) genotype of A1166C.
Conclusions In CAD the AGTR1 gene A1166C SNP may be associated with the aerobic power response to physical training.
479: Genetic NCIL G13368A polymorphism of the NADH-dehydrogenase mitochondrial subunit 5 and aerobic power in coronary artery disease
J Defoor, M Antritsou, K Martens, G Matthijs, R Fagard, L Vanhees; CAREGENE Study
K.U. Leuven, Leuven, Belgium
Background Aerobic power and the response to physical training are highly dependent of genetic variation. The genetic contribution has been shown to occur largely through maternal transmission. This is considered an argument for involvement of the mitochondrial genome, which is exclusively maternally transmitted. The purpose of this study was to investigate whether the NciL G13368A polymorphism of mitochondrial subunit 5 of the NADH-dehydrogenase (MTND5) gene is associated with aerobic power or its response to physical training in patients with coronary artery disease (CAD).
Methods All biologically unrelated Caucasian patients with CAD who had exercised until exhaustion during incremental bicycle testing at baseline and after completion of three months of cardiac rehabilitation from 1990 through 2001 (n = 1095) were eligible for inclusion in the CAREGENE Study. 935 blood samples were obtained for DNA-analysis. In 922 patients the MTND5 NciL G13368A polymorphism was determined using sequenom MassARRAY RT technology (Lark technologies, Essex, UK).
Results Frequencies of the MTND5 gene common (wild-type) G and rare (mutation) A alleles were 0.89 and 0.11, respectively. Covariate-adjusted aerobic power (ml/min) was similar (F = 0.03, P = 0.87) at baseline for carriers of the G and A allele (1721 ± 13 vs. 1715 ± 38, respectively) (mean ± SE) and increased significantly (P < 0.001) for both groups with physical training. An association with the aerobic power response to training was not observed (G allele: 24.2 ± 0.6% vs. A allele: 22.1 ± 1.6%) (F=1.47, P = 0.23).
Conclusions The NciL G13368A polymorphism of the MTND5 gene is not associated with aerobic power or with the response to physical training in CAD.
480: NAD(P)H oxidase P22phox gene A640g and C242T polymorphisms and aerobic power in coronary artery disease
J Defoor, E Logghe, K Martens, G Matthijs, R Fagard, L Vanhees; CAREGENE Study
K.U. Leuven, Leuven, Belgium
Background Aerobic power (AP) and its response to physical training depend on the genetic make-up of individuals. NAD(P)H-oxidase is a source of superoxide production, associated with endothelial dysfunction. The purpose was to evaluate whether the A640G and C242T single nucleotide polymorphisms (SNPs) of the p22phox subunit of the NAD(P)H oxidase gene are associated with AP or with its response to physical training in patients with coronary artery disease (CAD).
Methods All biologically unrelated Caucasian patients with CAD who had exercised until exhaustion during graded bicycle testing at baseline and after completion of three months of cardiac rehabilitation from 1990 through 2001 (n = 1095) were eligible for inclusion in the CAREGENE Study. 935 blood samples were obtained for DNA-analysis. A640G and C242 T SNPs of p22phox were identified by sequenom MassARRAY RT technology in 892 and 930 patients, respectively.
Results Frequencies of the p22phox A640G SNP AA, AG, and GG genotype were 0.26, 0.48 and 0.27, respectively; of the C242 T SNP CC, CT and TT genotype 0.44, 0.45 and 0.10, respectively. The A640G SNP was overall modestly associated (F = 2.54, P = 0.079) with covariate-adjusted AP at baseline as well as after training. AP at baseline (ml/min) and after training was lower in patients homozygous for the rare G allele (1680 ± 23.0 and 2064 ± 26.0, respectively) (mean ± SE) as compared with heterozygotes (1739 ± 17.2 and 2132 ± 19.4, respectively) and homozygotes for the common A allele (1731 ± 23.6 and 2115 ± 27.0, respectively). C242 T was not associated with AP at baseline or after training. Physical training significantly (P < 0.001) increased AP, but associations between either p22phox polymorphism and the response to training were not observed.
Conclusions The A640G SNP, but not C242 T, was modestly associated with aerobic power before and after physical training in CAD. Neither polymorphism was associated with the aerobic power response to training.
481: Is stress testing really necessary for safe cardiac rehabilitation?
António Rui Leal, Orquídea Silva, Vasconcelos Teixeira, Lopes Gomes; Cardiovascular Prevention and Rehabilitation Unit
UPRCV, Hospital de Sto António, Porto, Portugal
Background Stress testing (ST) seems indispensable to perform cardiac rehabilitation programs (CRP). We intended to analyse till what point is ST really necessary in the context of a CRP, performed with safety, in patients with Ischemic Heart Disease (IHD).
Method Retrospective study involving data collection from the clinical story, CRP sessions/complications and results of ST, in a period of about 2 months, before or during PRC; sample data was randomized and chose from about 30% of sessions from the CRP, using a observation grid. Comparison was performed between two groups: those who performed ST (STG; n = 51) and those who did not performe (NST; n = 69).
Sample 120 patients (7.5% women), aged 57 + 10.5 years (30-82) diagnosed MI (53.3%), Angina (23.4%) and ACS (23.3%). LVEF was normal in 55% of the cases or with light depression in 20.8%, moderate in 16.7% and severe in 7.5%. No significant differences were found concerning sex, age, diagnose, LVEF or resting HR (67.7 vs 67.1 bpm) between the two groups.
Intervention Supervised group exercise, using modified Borg Scale, HR and ECG, along with educational and psychotherapy, when needed.
Statistics Descriptive and ANOVA to compare between groups, in SPSS 12.5.
Results ST analysis: 41.3% were normal, 25.5% suggesting isquemia while 33.2% were abnormal or non conclusive. Max HR was 145.67 bpm + 20.42 bpm. Comparing both groups, max. HR C during CRP was slightly superior in STG (98 vs 94bpm; P < 0.01), but the number of complications were similar (1.80 vs 1.83; P < 0.01). In 2.391 sessions/hours performed in the CRP, we found 31 complications minor, like chest pain (61.9%) and dizziness (19.0%), among others (19.1%). The most serious was a ventricular taquicardia post-exercise. No major complications were found. Percentage of minor complications was 1.2%.
Conclusions This suggestes that Stress Testing is dispensable in CRP for patients with IHD, if certain rules of security are followed.
483: ARG213GLY polymorphism of the extracellular superoxide dismutase gene and aerobic power in coronary artery disease
J Defoor, W Mysak, K Martens, G Matthijs, R Fagard, L Vanhees;Study, K.U. Leuven, Leuven, Belgium
Background The heritability of aerobic power (AP) and its response to physical training is frequently demonstrated. Endothelial nitric oxide (NO) is released during exercise and increases coronary and peripheral arterial vasodilation. The EC-SOD gene Arg213Gly single nucleotide polymorphism (SNP) is associated with extracellular superoxide dismutase (EC-SOD) plasma levels. EC-SOD quickly dismutates superoxide production, thus preventing the loss of NO-bioactivity. The association of the EC-SOD gene Arg213Gly SNP with AP and its response to physical training was evaluated in coronary artery disease (CAD).
Methods All biologically unrelated Caucasian patients with CAD who had exercised until exhaustion during graded bicycle testing at baseline and after 3 months of cardiac rehabilitation from 1990 through 2001 (n = 1095) were eligible for inclusion in the CAREGENE Study. 935 blood samples were obtained for DNA-analysis. In 902 patients the EC-SOD gene Arg213Gly SNP was identified by sequenom MassARRAY RT technology.
Results 97.1% of the patients were homozygous for Arg213, 2.9% were heterozygous, none were homozygous for Gly213. Overall, the Arg213-Gly SNP was modestly associated (F = 3.33, P = 0.068) with covariate-adjusted AP at baseline and after training in favour of the mutation. At baseline AP (ml/min) was higher, although not significantly (F= 1.75, P = 0.19), in heterozygous patients as compared with Arg213Arg homozygotes (1815 ± 72 vs 1718 ± 13, respectively) (mean ± SE). AP increased significantly (P < 0.001) for both genotypes with physical training and remained higher (F = 4.72, P = 0.03) in Gly213-carriers after training (2281 ± 81 vs 2101 ± 14, respectively). In the latter patients the response to training (ml/min) tended (F = 2.57, P = 0.11) to be higher (460 ± 49 vs 380 ± 8, respectively).
Conclusions In CAD the EC-SOD Arg213Gly SNP was associated with aerobic power, particularly after physical training. An impact on training response should not be dismissed.
485: Effects of creatine supplementation with exercise training on physical fitness in coronary artery disease and chronic heart failure
J Defoor, A Stevens, D Schepers, P Hespel, M Decramer, L Mortelmans, F Dobbels, J Vanhaecke, R Fagard, L Vanhees
K.U. Leuven, Leuven, Belgium
Background Creatine monohydrate is an established ergogenic aid in sports and is claimed to have therapeutical applications in a variety of diseases. The effect of oral creatine supplementation (CR; 5g/day) in conjunction with exercise training on physical fitness was investigated in patients with coronary artery disease (CAD) with varying left ventricular function and with chronic heart failure.
Methods 80 cardiac patients (m/F: 74/6), were included in a doubleblind randomized placebo-controlled (PL) trial over 3 months. Cardiorespiratory endurance training as well as moderate resistance training was followed (3 sessions/wk). At baseline and after training left ventricular ejection fraction (LVEF) was measured by ECG-gated SPECT, aerobic power was determined during graded bicycle testing, peak isometric and isokinetic knee extensor strength, endurance and recovery were assessed by an isokinetic dynamometer, and health-related quality of life (HRQL) was evaluated with the SF-36 and MacNew Heart Disease questionnaires. Furthermore, in a subgroup (PL: n =8; CR: n = 8) biopsies were taken from m. vastus lateralis to determine total creatine (TCr) content.
Results At baseline LVEF, physical fitness, HRQL and TCr were similar in both groups (P > 0.05). With training aerobic power, muscular strength, endurance and recovery, and HRQL improved significantly (P < 0.001). Similar training effects, however, were found in CR and PL (P > 0.05), irrespective of LVEF at baseline. TCr after training was similar to baseline values in both groups. After 3 months of training only exercise duration (min) differed significantly (P < 0.05) between CR (10.3 ± 3.7) (mean ± SD) and PL (8.6 ± 2.0). No detrimental effect on renal or liver function was observed, nor were there any reports of adverse effects in CR.
Conclusions The training programme was effective in improving physical fitness and HRQL. An additional benefit of oral creatine in CAD was observed for posttraining exercise duration.
487: Optimizing rehabilitation treatment for central european patients after cardiovascular events implementing a special heart-lifestyle-training course on crete
U Hildebrandt, D Antoni, G Muche, G Wüchner, GF Diakakis, PE Vardas
Klinik St. Irmingard, Prien, Germany
In Germany, the possibility exists for patients after a myocardial infarction (MI) or coronary artery bypass (CAB) to take part in a 3-week rehabilitation programme. Due to an insufficient integration concept regarding the follow-up, the long-term results are not satisfying. Thus the Euroaspire-Study reveals that 1 year after the treatment 60% of patients blood pressure is insufficiently controlled, they are physically inactive. Taking into account the results of the Lyon-Heart-Study and the PET-Study (Percutaneous Angioplasty Compared with Exercise Training) a 2-week heart-lifestyle training (HLT) was developed to improve the long-term effects. Several hospitals co-operated in establishing this programme with the following remarkable features: Individual physical and theoretical training with physical exercises, sports, hiking in the mountains; relaxation exercises. Background to the Mediterranean nutrition: Special attention to the patient's spouse; Improving compliance by a motivating environment; Private financing (motivation); Further medical-scientific training. More than 300 patients have participated in this special HLT course over the last 3 years. The training course is carried out in co-operation with the Cardiology Department of the Heraklion University Hospital during spring and autumn season in the beautiful and stimulating Cretan landscape.
The aim of the 2-week programme is a permanent change of individual habits, an improvement of social support and social competence, a strengthening of self-confidence, a minimization of fears and depression by psychological support. Optimal motivation is the most important pre-requisite for the permanent lifestyle changes.
This project may serve as an example that rehabilitation and prevention can be improved by offering the patient such additional training, even if this calls for more self-financing and self-responsibility without raising the costs for the public heath-care-system.
491: Ventilatory threshold exchange between walking and cycling is not accurate for training intensity determination in untrained cardiac patients
D Hansen, P Dendale, J Berger, V Reenaers, R Meeusen
Vrije Universiteit Brussel, Brussels, and Virga Jesse Hospital, Hasselt, Belgium
Background Because one exercise test (bike or treadmill) is executed at the start of cardiac rehabilitation, the training intensity from this test has to be exchanged to other training modes (walking, cycling) for proper training intensity determination. It is unknown whether the ventilatory threshold (VT) can be used for this purpose.
Materials and methods 46 cardiac patients (43 AMI patients, mean age 59.5 ± 8.4 years) performed a maximal cycling and walking exercise test, in which data on oxygen uptake (VO2) and heart rate (HR) are collected. With application of the V-slope method, VT is determined. Next, the correlations between walking and cycling for VO2 and HR at VT and peak work level are calculated.
Results Correlation coefficients between walking and cycling for VO2 and HR at peak work level and VT.
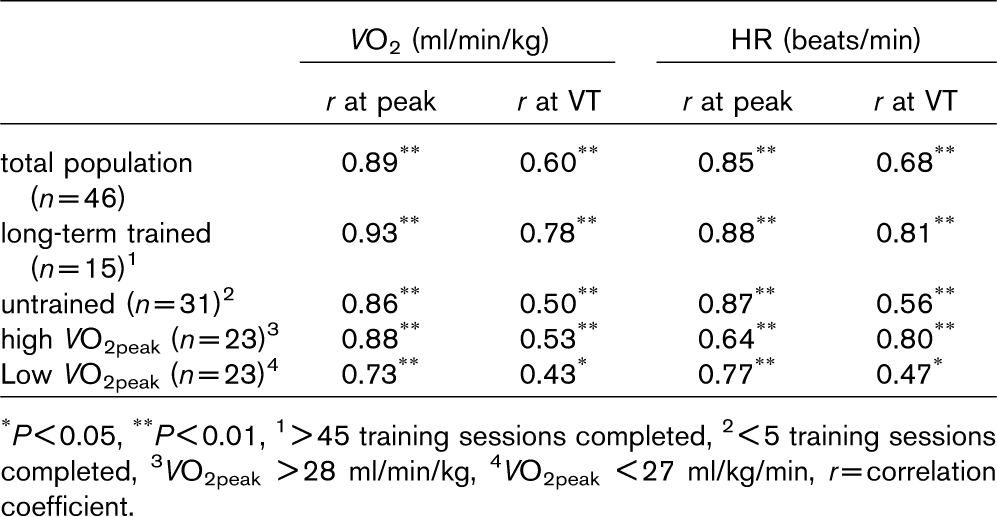
∗P<0.05
∗∗P<0.01
1>45 training sessions completed
2<5 training sessions completed
3 VO2peak >28 ml/min/kg
4 VO2peak <27 ml/kg/min, r=correlation coefficient.
Conclusions Peak exercise capacity can be exchanged well between modes in cardiac patients. However, VT exchange between modes is not accurate in untrained or deconditioned patients, while it is justified in long-term trained patients.
493: Does the model of cardiac rehabilitation influence on changes of health-related quality of life in patients with coronary heart disease
A Jegier, K Szmigielska, S Bakula, M Bilinska, L Brodowski, M Galaszek P Mrozek, B Olszewska, W Piotrowski, I Przywarska, J Rybicki; POLKARD
Sports Medicine Department Medical University of Lodz, Poland
In Poland cardiac rehabilitation is mainly performed in hospitalsinpatient cardiac rehabilitation (ICR). Although outpatient cardiac rehabilitation (OCR) is less expensive it is less popular in Poland due to lack of specialized centers. The beneficial influence of CR on quality of life is known.
The aim of the study was to evaluate an impact of ICR and OCR on health-related quality of life of patients with coronary heart disease (CHD).
We studied 562 patients with CHD from 9 centers of CR in Poland. First group-313 patients aged 56.1 ± 8.8 years who participated in ICR the second group-249 patients aged 57.4 ± 9.1 years who participated in OCR. OCR lasted 8 weeks. ICR lasted 3 weeks and then physical training was continued at home for 5 weeks. The examination was performed at the beginning of CR and after 8 weeks. Quality of life was assessed using EuroQuol 5D (EQ-5D) and SF36 questionnaires.
In the first examination patients from both groups did not differ significantly in terms of: mobility, self-care, usual activities, pain/discomfort and anxiety/depression (EQ-5D). Also the health status measured on visual analogue scale (VAS) was similar 65.7 ± 16.4 points in ICR group and 65.2 ± 16.2 points in OCR group P > 0.05. Physical, psychological and social functioning according to SF36 did not differ too.
After 8 weeks an improvement of quality of life in majority of parameters was observed in both models of CR. Health status (VAS) was improved by 11.1% from 65.7 ± 16.4 points to 69.5 ± 14.8 points in ICR group and by 10.4% from 65.2 ± 16.2 points to 69.6 ± 16.5 points in OCR group (P> 0.05). Improvement in almost all of aspects of physical, psychological and social functioning was observed in both groups of patients. Vitality increased significantly by 13.2% in ICR group and by 15.5% in OCR group, bodily pain decreased by 29.0% in ICR group and by 38.2% in OCR.
Comprehensive cardiac rehabilitation improves quality of life without differences between inpatient and outpatient models.
495: Does the model of cardiac rehabilitation influence on changes of exercise capacity in patients with coronary heart disease-multicenter study in poland
A Jegier, K Szmigielska, S Bakula, M Bilinska, L Brodowski, M Galaszek P Mrozek, B Olszewska, W Piotrowski, I Przywarska, J Rybicki; POLKARD
Sports Medicine Department, Medical University of Lodz, Poland
Although outpatient cardiac rehabilitation program (OCR) is less expensive most of the patients in Poland are rehabilitated in hospitalsinpatient cardiac rehabilitation (ICR).
The aim of the study was to evaluate the impact of ICR and OCR on exercise capacity in patients with coronary heart disease (CHD).
We studied 562 patients with CHD from 9 centers of CR in Poland. First group-313 patients aged 56.1 ± 8.8 years who participated in ICR and the second group-249 patients aged 57.4 ± 9.1 years who participated in OCR. OCR lasted for 8 weeks. ICR lasted for 3 weeks and then physical training was continued at home for 5 weeks. The examination was performed in all patients at the beginning of CR and then after 8 weeks. Submaximal modified Bruce multistage protocol exercise test was performed with evaluation of workload during the last stage of the test (in METs) and rate of perceived exertion on Borg scale.
In first examination the workload during the last stage of the exercise test was similar in both groups of patients, in ICR group was 7.0 ± 2.4METs, in OCR group was 6.6 ± 2.8METs (P>0.05). The rate of perceived exertion on Borg scale was also similar in both groups 13.7 + 1.4 points in ICR group and 13.4 + 1.6 points in OCR group (P> 0.05).
Last workloads intensity increased significantly by 32.1% from 7.0 ± 2.4 METs before CR to 8.6 ± 2.5 METs after 8 weeks in ICR group and by 38.1% from 6.6 ± 2.8 METs before CR to 7.9 ± 2.5 METs after 8 weeks in OCR group. Differences between groups were statistically insignificant. The rate of perceived exertion on Borg scale was not changed after 8 weeks in both groups of patients in spite of bigger workloads.
Comprehensive cardiac rehabilitation improves exercise capacity without differences between inpatient and outpatient model. It may be an argument to increase number of OCR centers in correct healthcare politic.
496: The influence of AMPD1 gene mutation on cardiac rehabilitation in patients with myocardial infarction treated by PTCA
J Potocka, M Biliñska, B Dobraszkiewicz-Wasilewska, I Korzeniowska-Kubacka, R Piotrowicz
Clinic and Dept. of Cardiac Rehab., National Inst.of Cardiology, Warsaw, Poland
Background The presence of the mutation in gene encoded an enzyme AMP deaminase (AMPD1) is responsible for its diminished activation in the skeletal muscle cells. It leads to: 1) increased production of adenosine, which could be responsible for a better prognosis in patients with cardiac diseases; 2) impairment of energetic metabolism in skeletal muscles. The aim of our study was to assess the influence of AMPD1 mutation on the effects of rehabilitation in patients (pts) after MI treated with PCI.
Materials 180 pts after acute MI treated with PCI were included into the study and were divided in two groups: M (+) 80 pts with AMPD1 gene mutation and M(−)100 pts without mutation. In group M (+) 65 pts and in group M (−) 70 pts were reffered for cardiac rehabilitation including ergometric exercise training, 3 times per week, for 8 weeks. At the beginning and at the end of rehabilitation we performed spiroergometric test (SET) and analysed the following variables, characterising exercise capacity: METS, VO2/kg,% VO2max, VE.
Results There are no intergroup differences in baseline SET values. In group M (+) the following variables increased significantly after rehabilitation: METS (6.34 vs 7.16, P < 0.001); VO2/kg (22.3 vs 25.1, P < 0.002); %VO2max (75.8 vs 85.4, P <0.01) and VE (57.6 vs 66, P < 0.004). The analysed variables did not change significantly in group M(−) after 8 week rehabilitation: METS (6.72 vs 7.18, NS); VO2/kg (23.5 vs 25.1, NS); % VO2max (81.5 vs 84.3, NS) and VE (59.7 vs 63.6, NS)
Result Exercise training has a beneficial effect on exercise capacity only in pts with AMPD1 mutation.
497: EURO 2004 football games increases risk of acute coronary syndromes two or threefolds?
António Rui Leal, Jezabel Azevedo, João Amado, Vasconcelos Teixeira, Lopes Gomes; Cardiovascular Prevention and Rehabilitation Unit
UPRCV-Hospital de Sto Antonio, Portugal
Background Few studies have been conducted to quantify how much football games can trigger cardiac events. The aim of this preliminary prospective study is to investigate the association between Euro 2004 football games and hospital admissions for acute coronary syndromes (ACS, excluding possible environmental effects.
Methodology Analyse hospital admissions with CID 9 diagnosis (410-414 during Euro 2004 World Cup. Analyse of clinical data base from Cardiology and individual interview and questionnaires with a stress scale (0-10).
Initial sample Selection of 203 patients (> 39y), admitted in Emergency Room (ER) and interned by ACS between May and July 2003 (n = 104) and 2004 (n = 99).
Final sample 10 patients admitted in a day after 2 important football games, 25th June and 5th July 2004 in ER by ACS. Seven patients were interviewed, two were dead and one missed the follow-up.
Statistics descriptive statistic with principal components analyse and Pearson. coefficient to correlate atmospheric variables and ER admissions.
Results In studied months the hospital admissions showed 1 to 1.3 ACS cases/day. In the first 15 days of June 2003 were admitted 75% of the total for this month, associated by increase in temp. (max. 37.2). After Portugal vs England were admitted 6 ACS cases and after Portugal vs Greece final other 4 cases, representing an increase by 4 folds. Six in 7 patients recognised they watched the football games and 5 attributed their disease to this. One patient didn't remember. They were 8 men and 2 women (48-77y), admitted with Unstable Angina (2), ACS without ST supra (4) and AMI (4). They all presented 2-5 relevant risks factors, 60% with serious cardiac/atherosclerotic disease and 30% Diabetes Mellitus Type II.
Conclusion As a preliminary study, this paper suggests that hospital admissions for ACS can be doubled or tripled by emotional/competition upsets, such as special football games, manly in men with relevant cardiovascular risks factors and diabetes.
500: High prevalence of “external” locus of control in male heart failure patients attending a cardiac rehabilitation programme
R Walker Schmid, JP Schmid, H Saner
Swiss Cardiovascular Centre Bern, Switzerland
Background The locus of control (LOC) construct refers to the degree to which an individual believes that he can influence the course of the disease. The recovery from of a cardiac event can be perceived as being influenced mainly by one's own actions (internal health LOC, I), powerful others LOC (external control, P) or by chance (fatalistic orientation, C). Since patient's (pts) compliance is strongly influenced by the LOC, we were interested to assess the LOC pattern in a cardiac rehabilitation (CR) programme.
Methods LOC was determined in 213 patients (pts) with coronary artery disease and preserved left ventricular function (mean age 58.6 ± 11.9yrs, 71% male, group A) and 39 pts with heart failure (CHF, mean age 58.3 ± 13.5yrs, 82% male, group B) by a specific questionnaire (“Fragebogen zur Erhebung von Kontrolluberzeugung zu Krankheit und Gesundheit”, KKG).
Results Pts of group A showed no difference in I (P = 0.451), P (P = 0.409) and C (P = 0.121) when compared with a standard population. Pts of group B showed no difference in I (P = 0.800) either, but differed highly significantly in P (P < 0.001) and C (P = 0.001). The comparison of group A and B showed a significantly higher P score in group B (22.2 ± 5.1 vs 24.4 ± 6.0, P = 0.044). There was no gender related difference in group A, whereas in group B, only men showed high P (P < 0.001) and C (P = 0.001) LOC. These men also showed a significantly higher depression score of the Hospital Anxiety and Depression Scale (5.0 ± 4.9 vs 3.2 ± 3.4, P = 0.018), which on his part correlated with I (r = −0.45, P = 0.040) and C (r = 0.34, P = 0.037).
Conclusions Male CHF pts in a CR programme are characterised by a lower confidence in their own potential to positively influence the disease progression. This LOC pattern correlates with symptoms of depression. To optimise the compliance and long term outcome in these pts, special emphasis has to be placed on the reinforcement of their faith in their own possibilities.
506: Comparision of early and late effects of interval training and swimming pool training in post MI patients
B Dobraszkiewicz-Wasilewska, R Baranowski, J Potocka, I Korzeniowska-Kubacka, J Osak, R Piotrowicz
Clinic & Dept. of Cardiac Rehab., National Inst. of Cardiology, Warsaw, Poland
Background Different types of training are implemented in cardiac rehabilitation. We compared the short term and late effects of cycloergometric interval training [CT] and swimming pool training [SPT] in past MI patients.
Patients and methods The group of 73 men post MI (mean age 52 ± 11 yrs, NYHA class 1-2) were included into the study. After first cycle of 16 CT the patients were randomised into next 16 CT or SPT. Before the first cycle (1), before second cycle (2) after second cycle (3) and 6 moths later (4) all pts had symptoms limited exercise and ergospirometric test. Walking distance [WD] and peak VO2 [VO2] were assessed.
Results The two cycles was finished by 50 men; 10 pts returned to work during rehabilitation, 8 had health problems not related with cardiovascular system, 4 were hospitalised due to recurrence of the coronary symptoms. No adverse events were observed during CT and SPT.
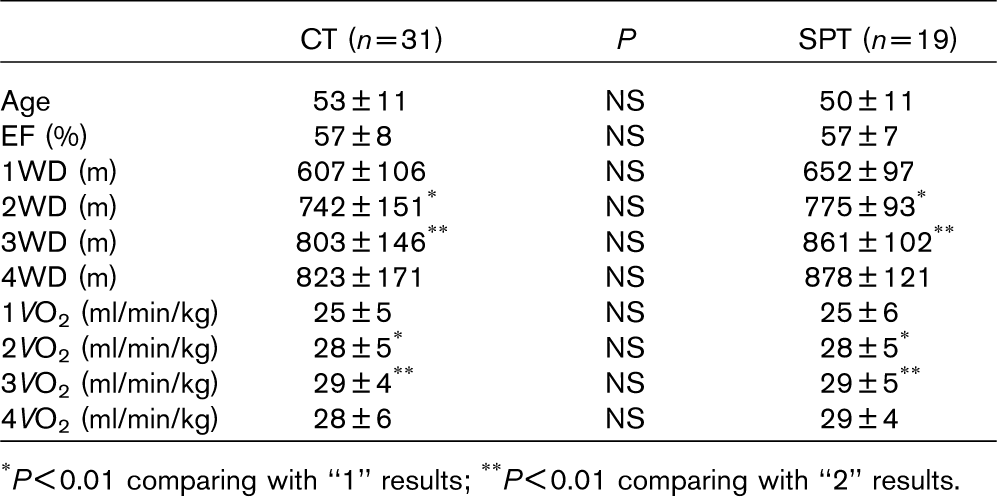
∗P<0.01 comparing with “1” results;
∗∗P<0.01 comparing with “2” results.
Conclusions Short term and late effects of swimming pool training are comparable with the effects of CT training. Swimming pool training is a safe and efficient alternative for cardiac rehabilitation in post MI patients.
510: Predictive factors for different types of cardiac rehabilitation after cardiac and thoracic aortic surgery
V Goeber, H Saner, J Kainth, FF Immer, JP Schmid, T Carrel
Swiss Cardiovascular Center Bern, University Hospital, Bern, Switzerland
Background Patients profile in cardiac surgery is changing. The number of older patients (pts) and pts with significant comorbidities is increasing whereas improved surgical methods and postoperative medical care allow for earlier discharge. The aim of this study was to assess pts characteristics leading to different types of care after cardiac surgery and to find criteria for planning cardiac rehabilitation (cr).
Methods In this prospective cohort study pts data were assessed before, during and after cardiac surgery until discharge.
Results Complete data from 166/203 consecutive pts with cardiac or thoracic aortic surgery (113 males, 53 females; mean age 65.1 years) has been collected (5 pts died within 7 days after surgery, 32 pts were lost for follow-up). 117 pts (70.5%) attended inpatients cr and 36 pts (21.7%) ambulatory cr whereas 13 pts (7.8%) did not attend any cr programme. Regarding preoperative characteristics there was a significant correlation between the euroSCORE (P = 0.013), particular in chronic obstructive lunge disease (P = 0.018) and peripheral artery disease (P = 0.026) and a higher rate of inpatient cr following surgery. No significant correlation was found among cardiovascular risk factors, kind of cardiac surgery, postoperative complications and type of rehabilitation. Concerning postoperative data there was a significant correlation among ICU-stay more than 1 night and a higher rate of inpatient rehabilitation (P = 0.048).
Conclusions Our results indicate that several factors can be used to plan the rehabilitation after cardiac and thoracic aortic surgery: first of all the euroSCORE and the length of ICU stay whereas no significant predictive value was found for cardiovascular risk factors, kind of cardiac surgery and postoperative complications. Further investigations are recommended to evaluate practicability of this criteria for optimal planning of the cr following cardiac and thoracic aortic surgery.
519: Do low-frequency electrical myostimulation and conventional aerobic training induce similar effects on exercise capacity in patients with chronic heart failure?
G Deley, B Vergès, JC Eicher, S Salmi-Belmihoub, JM Casillas
Laboratoire INSERM/ERITm 0207, Motricité et Plasticité, UFR STAPS Dijon, France
Specific physical trainings are nowadays presented as important components of the therapy of patients with chronic heart failure (CHF). Although aerobic and/or strength training programs (CONV) are classically proposed, low-frequency electrical myostimulation (EMS) has recently been demonstrated to induce similar beneficial results in these patients. However, in this study, authors concluded that results were very interesting but have to be considered with caution due to the small number of patients included. The aim of the present study was therefore to complete these results by including more patients.
Forty-eight CHF patients (NYHA II and III) underwent 5 weeks of exercise training, 5 days a week-1 for one hour, in EMS (n = 24) or CONV training (n = 24). At baseline and after the training period, they performed a symptom-limited cardiopulmonary exercise test and a 6-min walk test.
Before training, no difference was observed between the two groups. Peak VO2 was improved by 15% after EMS and 17% after CONV Moreover, VO2 at ventilatory threshold was 11% higher after both training programs, and the distance covered in 6 minutes was increased by 11% after EMS and 16% after CONV. There was no significant difference between improvements after EMS and CONV training programs.
These results confirm those of the study of Deley and coworkers: five weeks of low-frequency electrical myostimulation (EMS) and conventional (CONV) exercise training produce similar beneficial changes in exercise capacity and muscle performances in patients with CHF. Electrical myostimulation may therefore be considered as a good alternative for rehabilitation particularly in patients with severe CHF. Indeed, it is safe and well-tolerated and it could be easily realized at home.
532: Heart manual: translation, adaptation to the Italian culture and its implementation in clinical setting
Roberto F.E. Pedretti, Simona Sarzi-Braga, Alessandra Ianni, Mariani Paola, Elena Genoni, Mario Pribetich, Giorgio Bertolotti
Salvatore Maugeri Foundation, IRCCS, Tradate (Va), Italy
Background The Heart Manual (HM) is a facilitated self-help and educational tool effectively used in rehabilitation programs for patients with coronary artery disease (CAD) in the United Kingdom. Great attention is raising around the inter-cultural applicability of such tools in order to facilitate their spreading and to compare interventional programs results. In this setting the HM has firstly to show equivalent contents in the original UK and Italian version, than an effort is required to make HM appropriate for the Italian culture. Finally this educational tool needs to be employed in the clinical setting in order to evaluate patient's approval and its real effectiveness.
Aim To standardize HM for Italian clinical use in a multidisciplinary phase II—III rehabilitation program of patients with CAD.
Method;: 1) Translation of the text from English into Italian by a team of experts confident with the HM topics; 2) check for the appropriateness of the first Italian version by a native English people; 3) second review by an expert committee board (cardiologist, psychologist, physiotherapist, dietician) aimed to make the version appropriate for Italian cultural profile; 4) delivering of HM in clinical setting (phase II—III rehabilitation program in CAD patients) by health care professionals; 5) patients approval evaluation by means of a 4 items questionnaire (looking for comprehensibility, caring and effectiveness of the device).
Results 38 CAD patients (male 87%, mean age 65 ± 10 years) received the Italian version of the HM during the rehabilitation period; 76% of them read all HM sections and found them effortless and comprehensible (57% very much; 43% fair). Majority of patients (65%) found HM very helpful in the knowledge of their disease. None of the sections appeared more helpfulness than other.
Conclusion The Italian version of the HM may be an useful toll that can improve educational support and quality of care of cardiac patients and their relatives.
538: Analysis of functional status by different evaluation scales in cardiac rehabilitation
M Pribetich, E Milani, E Genoni, RFE Pedretti
IRCCS Salvatore Maugeri Foundation, Division of Cardiology, Tradate, Italy
Background It is unclear which tool may be the more appropriate to evaluate effectiveness of cardiac rehabilitation programs.
Aim of the study To asses the role of 3 validated scales in the functional evaluation of patients with heart disease during a cardiac rehabilitation program.
Methods 124 patients referred to our centre for a cardiac rehabilitation program were included in the present analysis: 79 (64%) men, mean age 66 ± 11, LVEF (%) 52 ± 11, 60% after cardiac surgery, mean Hb (g/dl) 12 ± 2. At the beginning and at the end of the program all patients were evaluated with the Barthel Index (BI [score 0-95]), Katz Index of Activity of Daily Living (ADL) (KI [score 0-6]) and Rivermead Mobility Index (RMI [score 0-15]). The time between the initial and the final evaluation was in average 14 ± 5 days.
Results In general population all scales showed statistically significant changes: BI (88 ± 14 vs 93 ± 6, P = 0.000), KI (5.5 ± 1.1 vs 5.8 ± 0.5, P = 0.000), RMI (12 ± 3 vs 14 ± 2, P = 0.000). Patients were divided in 3 subgroups according to some relevant clinical characteristics: age, LVEF, cardiac surgery as index event. In older patients (> 80 years) and in those with LVEF < 30% a lower score at the initial evaluation was observed in all scales, therefore between the 2 tests were higher than in other subgroups.
Conclusion All the analyzed scales showed significant changes between the beginning and the end of the rehabilitation program. However in our population the initial score seems to indicate only a modest impairment of the functional status with the exception of older patients and those with severe left ventricular dysfunction. Therefore the use of such scales should be probably limited to specific subgroups of patients and integrated with other clinical and instrumental variables.
540: Physical training and age: effects of a cardiovascular training program on quality of life and functional capacity after coronary artery by-pass grafting
E Milani, M Pribetich, E Genoni, RFE Pedretti
IRCCS Salvatore Maugeri Foundation, Division of Cardiology, Tradate, Italy
Aim of the study Effects of a short cardiovascular training on work capacity and quality of life were analyzed in different subgroups of patients, with different age, after coronary artery bypass graft (CABG).
Methods 58 patients, all men, referred to our centre for a rehabilitation program after a recent CABG were included in the present analysis: age 61 ± 7 years, LVEF (%) 50 ± 8, Hb (g/dl) 12 ± 1. Two groups of patients were identified according to age: group 1 (n = 39, age 50-64 years) and group 2 (n = 19, age 65-76 years). At the beginning and the end of the training program a cardiopulmonary test (CPX) and a Quality of Life evaluation, using the visual analogic scale of the EuroQol (EQ) group were performed. The program had a 4 week duration and included supervised aerobic training sessions at cycle/treadmill and large muscle activity sessions. Intensity of cycle/treadmill exercise sessions was based on the first CPX data, both groups of patients performed in average 10 training sessions.
Results A significant improvement of maximal oxygen consumption (VO2max), maximal work capacity and quality of life was observed in the general population and in both groups of patients. Conserning functional parameters, VO2max and maximal work capacity showed an increase of 18.6% (P = 0.0001) and 24.4% (P = 0.0001) in group 1 vs 12.1% (P = 0.002) and 9.8% (P = 0.009) in group 2. Concerning EQ score, the opposite trend was found: a 13.3% increase (78 ± 14 vs 88.4 ± 9.6, P = 0.0001) was observed in group 1 vs a 24.3% increase (66.3 ± 12.7 vs 82.4 ± 12.4, P = 0.0001) in group 2.
Conclusion After a training program in patients with a recent CABG, EQ score improves in older patients more than functional parameters such as VO2max and work capacity. Therefore, in advanced age, quality of life evalutation represents a more sensitive index in the assesment of a training program and should be recommended in the outcome analysis of cardiovascular rehabilitation programs after CABG.
541: Long-term adherence to a home-based physical training program in patients with heart disease: one-year follow-up
E Genoni, E Milani, M Pribetich, S Sarzi Braga, RFE Pedretti
IRCCS Salvatore Maugeri Foundation, Division of Cardiology, Tradate, Italy
Aim of the study To evaluate the adherence of cardiac patients to a home-based physical training program one year after cardiac rehabilitation.
Methods 82 patients referred to our centre for a rehabilitation program were enrolled: n = 64 men (78%), mean age 64 ± 11 years, LVEF (%) 50 ± 12, 73% after cardiac surgery At the end of the rehabilitation period (23 ± 9 days) an individualized program of exercise training at home was prescribed. At one year after discharge an interview was obtained by phone and 17 items regarding health condition and adherence to home exercise training were collected.
Results 4 groups of patients were identified according to interview results:1) “NO TRAINING” (n = 6,7%): patients who didn't perform exercise because of subsequent clinical problems; 2) “NO ADHERENCE” (n.38,46%): patients who didn't perform or withdrawn the program in absence of significant clinical problems; 3) “PARTIAL ADHERENCE” (n =18, 22%): patients who performed exercise training respecting partially the program; 4) “FULL ADHERENCE” (n = 20, 25%): patients who were fully compliant to the training program. At univariate analysis the number of training sessions (P = 0.005), the number of educational sessions (P = 0.027), a subsequent outpatient rehabilitation program (0.029) and the civil state (P = 0.001) were all significantly associated with a good adherence. There was also a trend toward significance for age and ischemic heart disease. Multivariate analysis identified only the number of training sessions during the in-hospital period as a significant predictor of adherence to a home-based exercise program.
Conclusions These findings showed that at one year after discharge the adherence to a home-based training program is low (not higher than 47%). Patients who showed low interest to the rehabilitation during the in-hospital period are those at high risk of no adherence. It is necessary to early identify them in order to optimize training counseling and educational programs.
563: The indicators of adaptation persons in rehab and no-rehab groups during 15 years follow-up
K Mazurek, M Kowalska, J Tylka, M Stepnowska, R Piotrowicz
Department of Cardiac Rehabilitation, National Institute of Cardiology, Warsaw, Poland
The main effect of complex rehabilitation in cardiac patients should be the change of life style especially in elements related with cardiac risk. It seems to be interesting to compare patients who are underwent (R +) and not underwent (R-) rehabilitation, during the same time.
The aim of the study was an assessment of dependence between intensity of symptoms which characterized Type A behavior pattern and indicators of state and trait anxiety hostility and curiosity formulated by Spielberger in R + and R - groups. R + 40 male patients (age: 31-61, mean age = 52); R-31 male patients (age: 31-60, mean age = 50. Both groups were examined twice: in the beginning of the rehabilitation and after 15 years the period of rehabilitation. Medium duration of rehabilitation process was 9.3 years.
Psychological state was estimated by: JAS (Jenkins Activity Survey for Health Prediction)-this method evaluates aspects of Type A behavior pattern and STPI-method to evaluate the level of: anxiety, hostility, curiosity as a personality trait and as a state.
In the beginning of the observation of both groups there was only one significant difference between R + and R - of Jenkins Activity Survey for Health Prediction J-job involvement (202 ± 46.43 vs 180 ± 36) There are not differences in the beginning of results of STPI After 15 years The same dependency was observed in the aspect of Jenkins Activity Survey for Health Prediction J(187.6 ± 49.88 vs 163.8 ± 45.1; also appears one significant difference of STPI-hostility as a trait (28.7 ± 8.5 vs 30 ± 4.9). The intensity of all aspects of Type A behavior are changed-patients present lower level of life under time pressure, competition aggression and enmity in both groups. Although the stronger changes were observed in the rehabilitated group.
In the rehabilitated group we observed less tendency to show hostility in personal relations. The cardiac rehabilitation has a positive impact on the reduction of psychical tension and social contacts.
571: Pulse pressure and rate-pressure product during rehabilitation at low altitude in hypertensive patients
R Zivkovic, Lj Suric-Lambic, M Vasiljevic, M Zdravkovic
Medical Center Stari Grad Belgrade, Serbia and Montenegro
Background The circulatory changes caused by exposure to lower altitude (< 1.800 M) have not been well studied even though increasing number of people are spending holidays on the mountain. However, regular exercise training, supervised and controled, is recomended as a useful therapy for reducing blood pressure in hypertensive patients.
Objective The aim of our study was to evaluate the effect of rehabilitation on pulse pressure (PP) and rate-pressure product (RPP) during exercise testing at 1230. M altitude in hypertensive patients.
Methods Fifty treated hypertensive patients, 50.5 ± 6 years old with average blood pressure 154 ± 11/93 ± 7 mmHg who lived at 80-420 M. altitude enroled in the study. Submaximal cycle exercise testing performed before (I-ET) and after (II-ET) a three week rehabilitation programme (walking, bicycle training and aerobic exercise). PP and RPP obtained on I and II ET at rest and at the end of exercise testing. Exercise testing time (ETT) obtained before and after rehabilitation.
Results At rest PP on I ET was 60.90 ± 9.88 mm Hg and on II ET was 51.50 ± 8.7 mm Hg (P =0.0001); At the end of exercise testing PP on I ET was 92.50 ± 20 and on II ET was 86.20 ± 20 mm Hg (P = 0.13). At rest RPP on I ET was 13.2 ± 2 and on II ET 11.61 ± 2 (P = 0. 001); At the end of exercise testing RPP on I ET was 30.5 ± 2 and on II ET 27.3 ± 5 (ns). ETT before rehabilitation was 8.04 ± 3min., and after 9.56 ± 3 min (P = 0.01). After rehabilitation 33 (66%) patients achieved higher exercise level and 17 achived same or lower exercise level on II-ET.
Conclusion Rehabilitation in hypertensive patients at low altitude caused decrease in PP and RPP at rest and after submaximal exercise testing and improvement of exercise capacity expressed by prolonged exercise time.
574: The effect of smoking on quality of life of cardiac rehabilitation patients
R Goud, N Peek, IM Hellemans
Academic Medical Center, Amsterdam, Netherlands
Background Evaluation of quality of life (QoL) at cardiac rehabilitation (CR) baseline is nowadays recommended, since the psychosocial status of the patient is an important success factor in CR. Currently about 60-70% of CR centers in the Netherlands use the Quality of Life after Myocardial Infarction (QLMI) questionnaire at CR baseline.
Objective To examine differences in QoL between non-smokers, patients who quit smoking directly after their cardiac incident (quitters) and patients who continued smoking after their cardiac incident (smokers) measured at CR baseline.
Methods Demographic, QLMI, and clinical data were prospectively collected for all patients admitted to 8 Dutch CR centers during a period of six months in 2005. All data were collected using an electronic patient record, and randomly validated with independent sources afterwards.
Results A total of 1316 patients (317 quitters, 124 smokers and 875 non-smokers) filled in the QLMI questionnaire. Smokers scored lower than non-smokers (P < 0.001) on all QLMI domains, meaning the physical, social and emotional domain while quitters only scored lower on the emotional domain (P < 0.001). Smokers also reported lower scores on the emotional and physical domain (P < 0.01) compared to the quitters. (scores for non-smokers/quitters/smokers: total 123.6/120.2/113.2 out of 168; physical 48.5/47.6/44.6 out of 70; social 37.9/37.4/35.8 out of 49; emotional 56.9/54.3/50.5 out of 77). Results were corrected for differences in age, gender, BMI and diagnosis/intervention.
Conclusion QoL at CR baseline is lower for smokers than for non-smokers. However smokers feel emotionally and physically worse than quitters. This suggests that: 1) By stop smoking quitters increase their emotional and physical condition, or 2) by continue smoking smokers worsen their emotional and physical condition or, 3) patients that continue smoking do so because they feel emotionally and physically unable to quit.
579: Six minute walking test in patients with mild to moderate heart failure as a determinant of cardiac rehabilitation modality
M Dudziak, D Rawicz-Zegrzda, J Rogowski
Cardiac Rehabilitation Center, Wiezyca, Poland
Background The six minutes walk test (6MWT) is commonly used in clinical trials as an useful instrument to assess exercise capacity of elderly patients.
Aim The aim of this study was to invastigate the utility of 6MWT as a measure of the effectiveness of cardiac rehabilitation for refered patients with mild to moderate heart failure after coronary artery by-pass graft (CABG) and valve replacement (VR).
Methods One hundred and twenty two patients, (10% from all participants refered for cardiac rehabilitation during last two years), mean age 64 years (SD 12), were assessed for health status, and after clinical evaluation, electrocardiography, echocardiography 6MWT were performed. All participants were categorized into a four level classification according to their NYHA class. Second 6MWT test were performed after four weeks of cardiac rehabilitation.
Results The mean of I 6MWT distance was 254 m (SD-167) at the moment of first examination. After four weeks of rehabilitation significant improvement in II 6MWT-distance are observed in 65% of patients (mean 112m (SD-81)). In 22% of participants II 6MWT did not differ from the first result. 13% of patients were not able to walk whole the time. The results of the 6MWT were concordant with the change s in symptoms. The 6MWT-distance decreased significantly with increasing age (ANOVA P = 0.01) and with worsening in left ventricular ejection fraction (ANOVA P = 0.001).
Conclusion The 6MWT is safer, easier to administer, better tolerated, and better reflects activities modality in group of patients refered for cardiac rehabilation, after CABG or MV, than other exercise tests. It may be used as supportive evidence for symptom benefit.
581: Follow-up of patients with heart coronary disease and cardiac failure included in a cardiac rehabilitation program
M Abeytua, T Martínez, E Vaquerizo, P Avanzas, Fr Colino, L Pérez, M Martínez, E Jiménez, Fr Ramos-Becerril
Gregorio Marañón Hospital, Madrid, Spain
Background Cardiac rehabilitation (CR) is admitted as a complementary treatment to conventional treatment of cardiac failure (CF).
Objective To judge the outcome of patients with heart coronary disease (HCD) and CF included in a CR program.
Materials and methods We studied 58 consecutive patients with CHD and CF (ejection fraction (EF) ≤ 40%). All patients received conventional treatment and were included in a CR program. The CR program consisted of physical training, cardiological lectures, psychological group therapy and relaxation techniques learning during 2-3 months. Median follow up: 37.5 months.
Results The average age was 55.81 years (from 29 to 74). There were 7 (12%) woman. The EF pre CR was 32.17 ± 6.5 and post CR was 34.55 ± 9 (P = 0.6) and in the follow-up during a 1 year, EF = 34.46 ± 8. Quality of life improved at the end of CR program: EuroQoL-5D analogyc visual scale pre CR 60.72 and post CR 68.72 (P = 0.005), SF-36 physical component pre CR 43.48 and post CR 45.18 (P = 0.05) and SF-36 mental component pre CR 48.32 and post CR 52.94 (P =0.015). The Kaplan Meier survival was = 93%.
Conclusion Patients with HCD and CF included in a CR program improved quality of life and have high survival rates.
588: Impact of a short cardiac rehabilitation program on the various components of the metabolic syndrome
K Schoovaerts, V Reenaers, R Guilliams, F Vandereyt, J Berger, P Dendale
Rehabilitation and Health Centre, Heart Centre, Virga Jesse Hospital, Belgium
Background The metabolic syndrome is a growing world-wide problem. A new definition was presented by the International Diabetes Federation (IDF) in April 2005. The aim of this study is to evaluate the impact of a short (6 weeks) rehabilitation program on the various components of the metabolic syndrome, especially in heart patients.
Methods Retrospectively, the different parameters of the metabolic syndrome were analyzed in heart patients who followed our multi-disciplinary rehabilitation program (physical training, medical and dietary advise, psychological counselling). Following data were collected at the beginning and after 6 weeks of rehabilitation: waist circumference, level of triglycerides, HDL level, systolic and diastolic blood pressure and fasting plasma glucose.
Results We included 83 cardiac patients (64 men, 19 women) with a mean age of 62.5 years. At the start of their program, 41 men (64%) and 14 women (73.7%) fitted the definition of the metabolic syndrome. After 6 weeks of rehabilitation, there was an overall reduction of 19.3% in the presence of the metabolic syndrome. Our data show a significant improvement of waist circumference, systolic blood pressure, fasting plasma glucose and level of triglycerides.
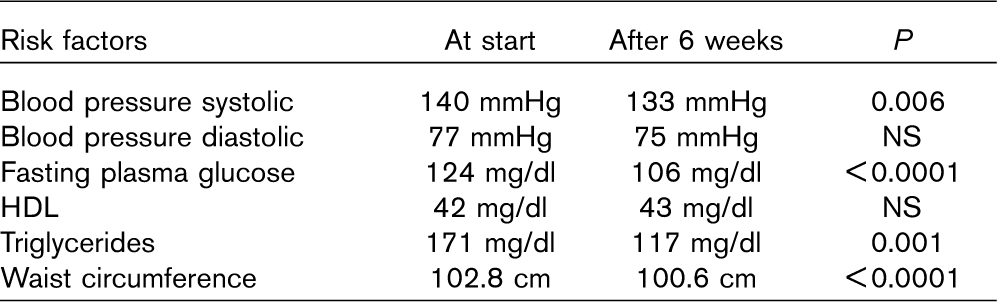
Conclusions This short-term study demonstrates that the multi-disciplinary approach during 6 weeks of rehabilitation provides a reduction of the metabolic syndrome in cardiac patients. Further investigation on the long-term effects is warranted.
601: Functional electrical stimulation improves endothelial function and reduces peripheral immune responses in patients with chronic heart failure
AI Karavidas, KG Raisakis, JT Parissis, DK Tsekoura, S Adamopoulos, DA Korres, A Zacharoulis, I Fotiadis, E Matsakas, A Zacharoulis
Heart Failure Clinic, Attikon University Hospital Athens, Greece
Background Previous studies have shown beneficial effects of functional electrical stimulation (FES) on muscle performance and exercise capacity of patients with chronic heart failure. This study evaluates the impact of FES on endothelial function and peripheral markers of immune activation in patients with moderate to severe heart failure.
Methods Twenty-four patients with a LVEF < 40% and NYHA II-III symptoms, undergoing optimized drug therapy, were randomized (2:1) in a 6-week training program of FES (n = 16) or served as a control group (n = 8). Endothelial function were assessed by Doppler Flow Mediated Dilatation (FMD) of the brachial artery, as well as peripheral pro-inflammatory/anti-inflammatory markers such as tumor necrosis factor (TNF)-α, interleukin (IL-6), soluble intercellular adhesion molecule (sICAM)-1, soluble vascular cell adhesion molecule (sVCAM)-1 and interleukin (IL)-10 were measured before and after the training program.
Results A significant improvement of 6-min walk test (< 0.05), Minessota Living score (P < 0.01) and FMD (P < 0.05) was observed only in the FES treated group. FES also causes a significant reduction of TNF-α (P <0.01), sICAM-1 (P<0.05), and sVCAM-1 (P <0.05), as well as a respective increase in ratio IL-10/TNF-α. In FES group, percentage improvement of Minnesota Living score was significantly correlated with respective changes in circulating TNF-α (r = 0.624, P <0.01), sVCAM-1 (r = 0.665, P < 0.001) and ratio IL-10/TNF-α (r = −0.641, P < 0.01).
Conclusion FES is an alternative exercise training program that improves endothelial function in patients with CHF, having also anti-inflammatory effects.
605: Correlation of the cardiovascular risk factors interaction with the revascularization procedures prognosis in symptomatic coronary patients
CA Sarãu, DM Duda-Seiman, M Iurciuc, S Iurciuc, L Barbu, A Avram, L David, I Sarãu, D Gaita, S Manca°
Institute of Cardiovascular Diseases, Cardiac Rehabilitation Clinic, Timisoara, Romania
Objective It has been analyzed the incidence of cardiovascular risk factors and of the metabolic syndrome (MS) in revascularized symptomatic coronary patients included in cardiac rehabilitation programme. It has been appreciated the efficiency of post procedural rehabilitation by cardiovascular risk.
Method In 61 revascularized coronary patients it has been assessed the aggregation of traditional risk factors, it has been evaluated the cardiovascular lipidic risk and the cardiovascular risk related to the presence of MS. Statistic processing: mean value ± SD%, multiliniar regression (p, R2). Lot characteristics: male patients (75.4%), female patients (24.6%), revascularized by coronary artery by-pass grafting (CABG) −64% and by PTCA −36%. 57.37% of the patients presented metabolic syndrome, 93.8% presented LDL> 100 mg/dl. 41% of the patients were smokers. All patients were monitorised 4 month since the inclusion in the rehabilitation programme.
Results The incidence of BMI < 25 kg/mp has significantly increased/ revascularised lot (P = 0.0001), but without any significant difference by revascularisation procedure. Patients with CABG with or without MS have reached LDL ≤ 100 mg/dl (P = 0.003, respectively 0.004) in percent of 12%, respectively 27%. No significant difference in patients revascularised by PTCA with or without MS. Patient with CABG and MS (P = 0.00001) and patient with PTCA without MS (P = 0.009) have obtained the control of SBP ≤ 135 mmHg (54%, respectively 18%). The rate of ex-smokers/revascularised lot has significantly increased (P = 0.0004).
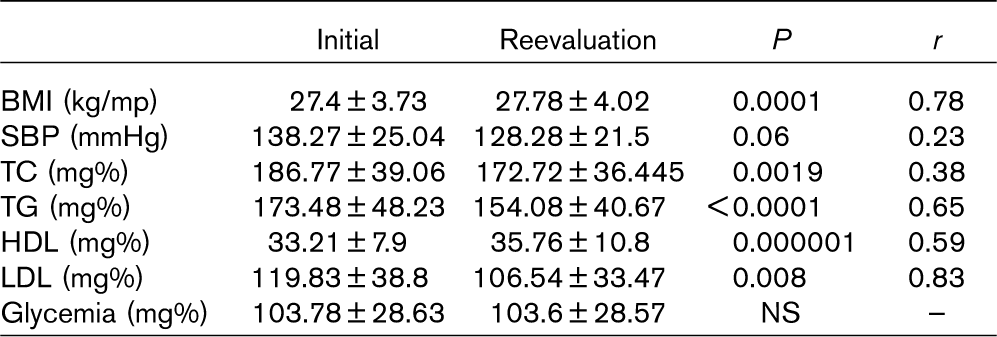
Conclusions 1. Patients with CABG were more motivated and they had a better compliance to the rehabilitation programme comparing with PTCA patients. 2. Presence of MS must be individualized in rehabilitation programmes, regardless the revascularization method. 3. The positive response obtained on LDL must be correlated with the other determinants of global revascularization risk for the evidence of an efficient prophylaxis.