
Abstract
Purpose
Our aim was to evaluate whether healthy dietary habits, physical activity and non-smoking are associated with less severe acute coronary syndromes and better short-term prognosis.
Subjects and methods
From October 2003 to September 2004, 2172 patients (1649 males), hospitalized for severe acute coronary syndromes in six major hospitals in Greece were included in the study. The severity of severe acute coronary syndromes was assessed through troponin-I and maximum creatinine kinase MB levels, while 30-day recurrent event rate (death or rehospitalization for cardiovascular disease, angioplasty or coronary artery bypass surgery) was used to evaluate the prognosis of the patients. A ‘healthy index’ that assessed adherence to the Mediterranean diet, moderate alcohol intake, physical activity and abstinence from smoking was developed (range 0–4).
Results
One unit increment in the healthy index was associated with −12.4 ± 2.4 ng/ml decrease in troponin I levels (P = 0.001) and −9.7 ± 2.5 ng/ml decrease in maximum creatinine kinase MB levels (P = 0.001). The in-hospital mortality rate was 3.2% in males and 5.7% in females (i.e. overall 82 deaths, P = 0.009); during the first 30 days following hospitalization the event rate was 15.7% in males and 16.3% in females (P = 0.001). Values of the healthy index above one (i.e. presence of two or more protective factors) seemed to be associated with 44–84% lower risk of having recurrent events (P < 0.001), even after various adjustments were made.
Conclusion
Among patients who had had severe acute coronary syndromes, a healthy lifestyle seemed to be associated with less severe cardiac events and lower risk of death or rehospitalization 30 days after the event.
Introduction
Throughout the twentieth century, many investigators have focused their interest on the prevention of cardiovascular disease. Based on their findings there is now a wide range of evidence to support the concept that several lifestyle-related habits might influence coronary heart disease and stroke risk [1–4]. The beneficial effect of physical activity, abstinence from smoking and healthy diet on human health has been underlined in several studies. Recently the National Cholesterol Education Program Adult Treatment Panel (NCEP ATP III) suggested therapeutic lifestyle changes in order to reduce the prevalence of atherosclerotic disease, which revealed the importance of diet and exercise [5]. From the late 1960s Keys and his colleagues from the Seven Countries study underlined the importance of the dietary habits observed in Mediterranean populations on cardiovascular disease risk [6]. More recently, reports from observational studies and clinical trials have shown an inverse association between the adherence to the Mediterranean diet and all cause, as well as coronary heart disease mortality and morbidity [7–9]. Moreover, although alcohol consumption is considered as a component of diet it is addressed separately in many prevention strategies. This is because moderate alcohol intake has been associated with reduced levels of systolic and diastolic blood pressure, high-density lipoprotein and consequently lower cardiovascular risk [10]. The beneficial effect of physical activity on primary and secondary prevention of coronary heart disease risk has already been underlined in many observational and clinical studies, mainly through the reduction in body mass, arterial blood pressure, as well as inflammation and coagulation marker levels [11–14]. Finally, smoking has now been established as the major preventable risk factor for cardiovascular events, as well as other chronic diseases, especially lung cancer [15–17]. Although smoking has become a target not only of health professionals, but also of legislative and regulatory bodies, its prevalence is still very high in most of the developed countries [18]. Recently, Yusuf et al. [19] from the INTERHEART study reported that, among others, smoking, dietary habits and alcohol intake, as well as regular physical activity account for most of the risk of myocardial infarction worldwide in both sexes and at all ages in all regions.
The incidence of acute coronary syndromes (ACS) has increased substantially during the past years in Greece, while the lifestyle of people has changed unfavourably. Moreover, it has been reported that the risk of recurrent events during the first month after a cardiac event is very high [4]. In this work, we aimed to evaluate the association of individual as well as combined dietary pattern and lifestyle factors (Mediterranean diet, alcohol intake, smoking status and physical activity level) on the severity of patients hospitalized for ACS and the risk of recurrent events within 30 days after hospitalization.
Methods
Study population
Between 1 October 2003 and 30 September 2004 we enrolled almost all consecutive patients that entered the cardiology clinics or the emergency units of six major general hospitals in Greece (Hippokration Hospital in Athens, and the general hospitals in Lamia, Karditsa, Halkida, Kalamata and Zakynthos island). During the study period 2172 patients were admitted for ACS in the selected hospitals (1649 men, 65 ± 13 years old and 523 women, 72 ± 11 years old, P < 0.001). The participation rate varied from center to center from 85 to 99%. At entry a 12-lead electrocardiogram was performed and clinical symptoms were evaluated in all patients. Based on the electrocardiographic findings patients were classified as having ST-segment elevations, non-ST segment elevations or other electrocardiographic findings. Moreover, blood tests were performed to detect evidence of myocardial cell death. We measured troponin I levels and the MB fraction of total creatinine posphokinase (CPK). According to the Joint European Society of Cardiology and American College of Cardiology Committee, blood samples were obtained on hospital admission, at 6–9 h, and again at 12–24 h if earlier samples were negative and the clinical index of suspicion was high [20]. We included only cases with discharge diagnoses of ACS [acute myocardial infarction (MI) or unstable angina]. In particular, acute myocardial infarction was defined by at least two of the following features: electrocardiographic changes (patients with or without ST segment elevations); compatible clinical symptoms; and specific diagnostic sensitive biomarker elevations (troponin I > 0.4 ng/ml and the MB fraction of CPK > 8.8 ng/ml). Unstable angina was defined by the occurrence of one or more angina episodes, at rest, within the preceding 48 h, corresponding to class III of the Braunwald classification [21].
The study was approved by the Medical Research Ethics Committee of our Institution and was carried out in accordance with the Declaration of Helsinki (1989) of the World Medical Association.
Dietary and lifestyle evaluation
The evaluation of the nutritional habits was based on a validated semi-quantitative food frequency questionnaire that included major food groups and beverages usually consumed in Greece [22]. The consumption of certain food items and the portion size as an average per week, during the past year, was recorded. According to a dietary pyramid that has been developed to describe the inherent characteristics of the Mediterranean dietary pattern [23] we have calculated and validated a special diet score for each participant that assessed adherence to the Mediterranean diet (range 0–50). In particular, we evaluated 10 food groups: non-refined cereals and products, fruits and nuts, vegetables, olive oil, non-fat or low fat dairy, fish, poultry, potatoes, pulses, red meat or meat products and eggs, as well as alcohol consumption. The diet score was calculated as follows: for the consumption of items presumed to be close to this pattern (i.e. non-refined cereals and products, fruits and nuts, vegetables, olive oil, low fat dairy, fish, potatoes and pulses) we assigned score 0 when a participant reported no consumption, 1 when she or he reported consumption of one to four times per month, 2 for five to eight times per month, 3 for nine to 12 times per month, 4 for 13 to 18 times per month and 5 for more than 18 times per month. On the other hand, for the consumption of foods presumed to be away from this diet (like meat or meat products, eggs and poultry) we assigned reverse scores (i.e. 0 when a participant reported almost daily consumption to 5 for rare or no consumption). We have assessed separately the consumption of alcoholic beverages in order to independently evaluate their effect on the outcome. In particular, we assigned score 5 for consumption of one to three glasses of wine per day, score 0 for consumption of more than seven glasses of wine per day and scores 4 to 1 for consumption of none, three to four, four to five, five to six and six to seven glasses of wine per day. This score has been validated and associated with surrogate markers of cardiovascular disease, as well as with hard outcomes [24], and higher values of this score indicate greater adherence to the Mediterranean diet.
To evaluate physical activity status of the patients during the past year we used a modified version of a self-reported questionnaire provided by the American College of Sports Medicine [25]. Based on this questionnaire we assessed the frequency (times per week), duration (in minutes per time) and intensity of sports or occupation related physical activity. Participants who did not report any physical activities were defined as sedentary. For the rest of the participants we calculated a combined score by multiplying the weekly frequency, duration and intensity of physical activity. The upper tertile of the score classified participants as highly physically active, the medium tertile as moderately active and the lowest tertile as having low physical activity.
Current smokers were defined as those who smoked at least one cigarette per day or have stopped cigarette smoking during the past 12 months. Former smokers were defined as those who had stopped smoking more than 1 year previously. The rest of them were defined as never smokers or rare smokers.
Then we calculated a ‘healthy lifestyle’ index using the tertiles of diet and physical activity scores, as well as the information about smoking habits and alcohol intake. In particular, we assigned the value of 1 to patients who were in the middle or the upper tertile of the diet score, and the value of 0 to those who were in the lowest tertile. Similarly, we applied the value of 1 to those who were in the middle or upper tertile of the physical activity score and the value of 0 in the rest of them. We decided to combine the second and third tertile of diet and physical activity scores since the values of these tertiles were very close. We have also assigned the value of 1 to those who reported as non-smokers or have stopped smoking for at least 15 years (since this has been reported as the duration that eliminates the risk of smoking on cardiovascular disease [15, 16]) and the value of 0 to those who reported as current or former smokers. Finally, we assigned the value of 1 to those who reported moderate alcohol intake (i.e. 12–30 g ethanol per day) and the value of 0 to the rest. Thus, a 0 to 4 index was developed. Higher values of this index indicate closer proximity to a healthy lifestyle. There is a rationale for using indexes instead of a single factor approach. Many factors are strongly correlated together (like physical activity and smoking habits) and therefore the use of each factor in the same model raises the issue of multi-co-linearity, which is a very frequent problem for the robustness of regression models. Using indexes that combine the information in the form of a score this problem does not exist.
Other investigated characteristics
In all patients a detailed medical history was recorded, including previous hospitalization for cardiovascular disease (i.e. coronary heart disease, stroke or other cardiovascular disease), presence of hypertension, hypercholesterolemia, renal failure and diabetes mellitus. Socio-demographic characteristics included age, sex, years of school and mean annual income of the family (through self reports) during the last 3 years. Height and weight was measured, to the nearest 0.5 cm and 100 g respectively. Body mass index was then calculated as weight (in kilograms) divided by height (in metres) squared.
With the exception of 15 patients who died during the first 24 h of their admission, all participants provided the requested information after the second day of hospitalization when their condition became stable.
Follow-up
After the first 4 weeks (30 days) of discharge all patients received a telephone call and answered questions about their vital status (i.e. re-hospitalization due to coronary heart disease, angioplasty, or coronary artery bypass surgery). Moreover, death due to cardiovascular disease was also recorded. During the first 30 days following discharge, 866 (40%) patients were lost to follow-up.
Statistical analysis
Continuous variables are presented as mean values ± standard deviation. The categorical variables are presented as absolute and relative (%) frequencies. Associations between continuous variables and group of patients were evaluated through the analysis of variance (ANOVA), after controlling for equality of variances (homoscedacity). Due to multiple comparisons we applied the Bonferroni correction to correct for the inflation of type I error. Associations between categorical variables were tested by the use of the χ2 test, without the correction of continuity. Correlations between continuous variables were tested by the use of Pearson's correlation coefficient. The evaluation of the healthy index score, as well as individuals' scores, on the severity of ACS was performed through multiple linear regression analysis. Using the Shapiro–Wilk criterion we evaluated the linearity of the residuals, while using the Levene test we evaluated the homogeneity of variances. Multiple logistic regression analysis evaluated the association of the healthy index as well as individual scores on the likelihood of having adverse events, such as in-hospital death or rehospitalization due to cardiovascular causes, surgery or death during the first 30 days following hospitalization.
All statistical calculations were performed on the SPSS version 12.0 software (SPSS Inc, Chicago, Illinois, USA).
Results
According to the discharge diagnosis, 764 (35%) patients were diagnosed as having unstable angina, 699 (32%) patients as having non-Q-wave MI and 709 (33%) patients as having Q-wave MI. Table 1 illustrates various lifestyle and behavioral characteristics of the patients. We observed that patients with MI had on average an 11% lower diet score than patients with unstable angina (P < 0.05). Moreover, diet score was inversely correlated with cardiac troponin I at entry (r = −0.054, P = 0.012), as well as with maximum levels of CPK (r = −0.096, P < 0.0001) and creatinine kinase MB (CKMB) (r = −0.082, P < 0.0001). No differences were observed as regards alcohol consumption between patient groups, in both sexes. Furthermore, we observed that Q-wave MI male patients were more frequently current smokers and physically inactive, as compared with non-Q-wave MI or unstable angina patients. As expected, unstable angina male and female patients had higher score in the ‘healthy index’ as compared to MI patients (Table 1). No differences were observed in the index that assessed lifestyle habits between sexes (P = 0.08).
Table 2 illustrates various clinical characteristics of the patients by discharge diagnosis. Both men and women with unstable angina more frequently had history of hypertension and coronary heart disease, while patients with non-Q-wave MI more frequently had diabetes and renal failure.
Lifestyle characteristics and events by discharge diagnosis
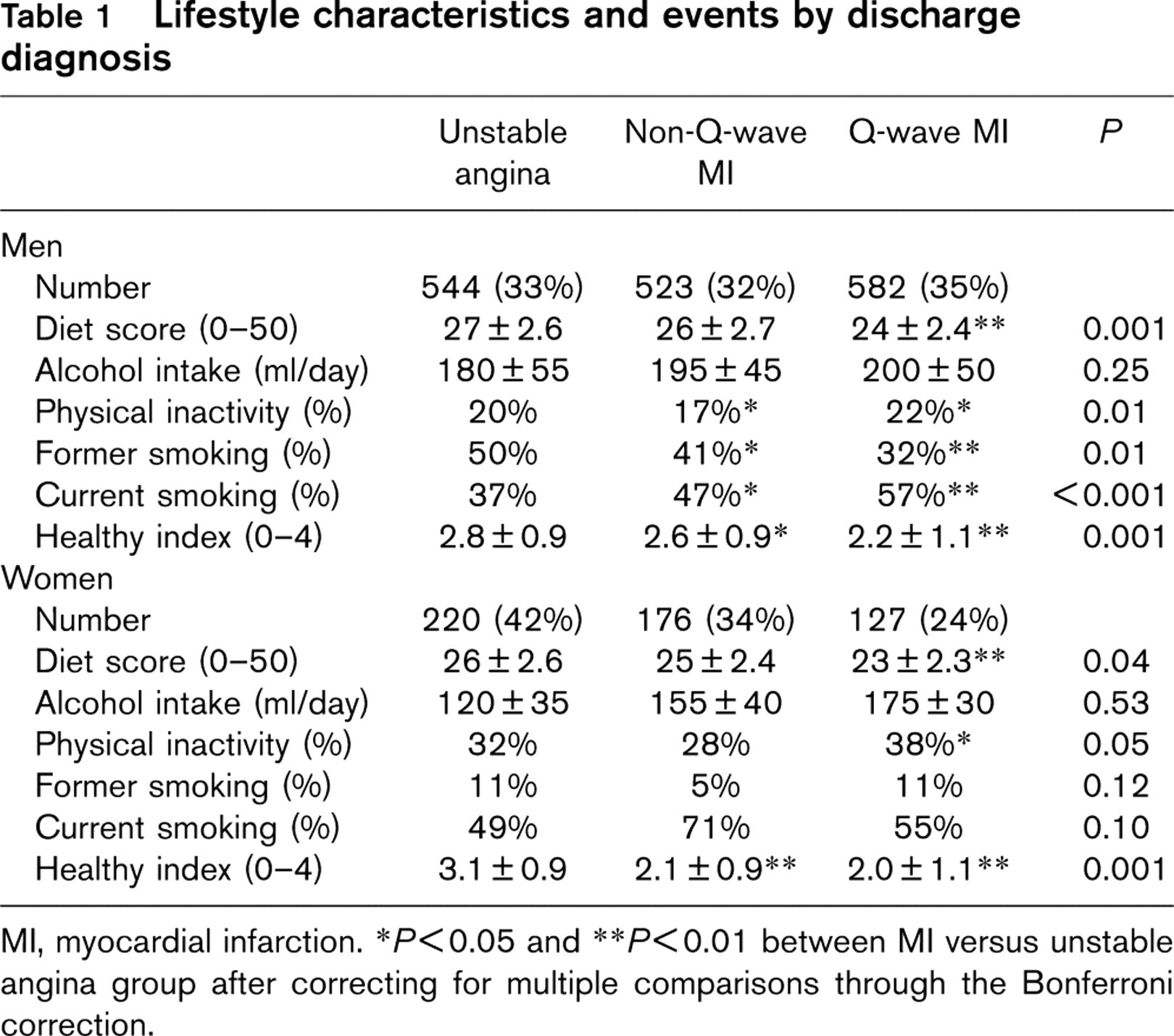
MI, myocardial infarction.
∗P<0.05 and
∗∗P<0.01 between MI versus unstable angina group after correcting for multiple comparisons through the Bonferroni correction.
After controlling for age, sex, history of coronary heart disease and the other clinical characteristics of the patients (presented in Table 2) we observed that diet score was inversely associated with entry troponin I (b ± SE, −0.89 ± 0.36, P = 0.012) and maximum CKMB levels (b ± SE, −1.35 ± 0.38, P ≤ 0.001). Similarly, physical activity score was inversely associated with entry troponin I (b ± SE, −0.45 ± 0.28, P = 0.03) and maximum CKMB levels (b ± SE, −0.29 ± 0.20, P = 0.03). Finally, current smoking was associated with higher levels of troponin I at entry (b ± SE, 19.06 ± 7.8, P = 0.015) and maximum CKMB levels (b ± SE: 28.4 ± 7.1, P = 0.001). No significant associations were observed regarding alcohol intake, troponin I and CKMB levels. Moreover, one unit increment in the healthy index was associated with −12.4 ± 2.4 ng/ml decrease in troponin I levels (P = 0.001) and a −9.7 ± 2.5 ng/ml decrease in maximum CKMB levels (P = 0.001), after controlling for age, sex and clinical characteristics of the participants.
In-hospital mortality
The in-hospital mortality rate was 3.2% in male patients and 5.7% in female patients (i.e. overall 82 deaths, P for sex differences = 0.009). At this point it should be mentioned that 15 of 82 patients who died during hospitalization did not fulfill the dietary (or any other) records. No significant association of the ‘healthy index’ on in-hospital mortality was observed (Table 3), after adjusting for age, sex, body mass index, education level, income status, discharge diagnosis, history of hypertension, hypercholesterolemia, diabetes mellitus, coronary heart disease, renal failure, and family history of cardiovascular diseases. Moreover, when we evaluated the components of the healthy index (Mediterranean diet, physical activity, moderate alcohol drinking and abstinence from smoking) on mortality during hospitalization no significant associations were observed. Presence of hypercholesterolemia (relative risk = 2.32, P = 0.03), diabetes (relative risk = 2.01, P = 0.07), renal failure (relative risk = 6.42, P = 0.001) were, however, strongly associated with the in-hospital prognosis after the aforementioned adjustments. Moreover, patients with myocardial infarction had 10 times higher risk of dying within hospital as compared with those with unstable angina (relative risk = 10.9, P < 0.001).
Clinical characteristics by discharge diagnosis
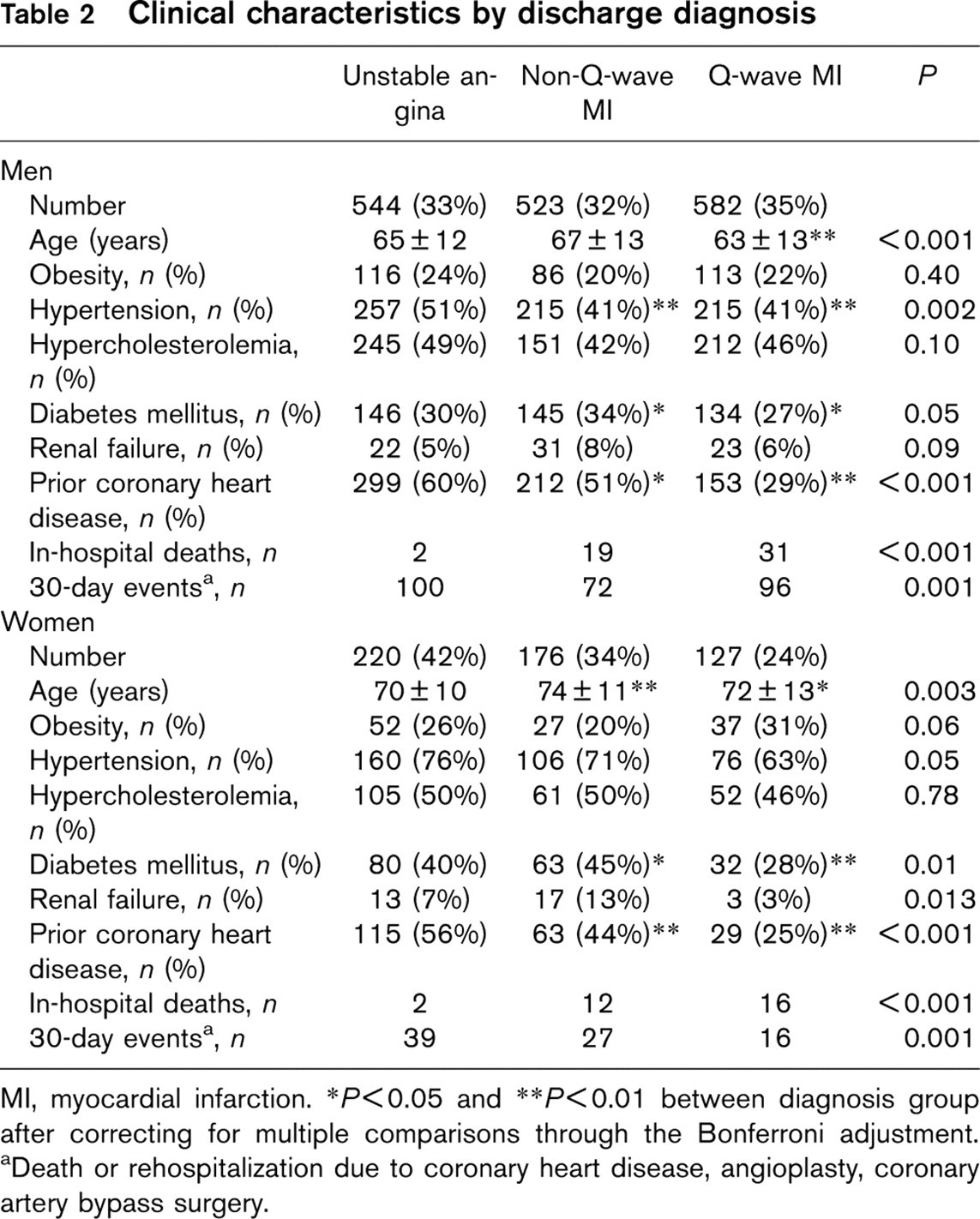
MI, myocardial infarction.
∗P<0.05 and
∗∗P<0.01 between diagnosis group after correcting for multiple comparisons through the Bonferroni adjustment.
aDeath or rehospitalization due to coronary heart disease, angioplasty, coronary artery bypass surgery.
Results from multiple logistic regression analysis that evaluated the healthy index on in-hospital mortality rates
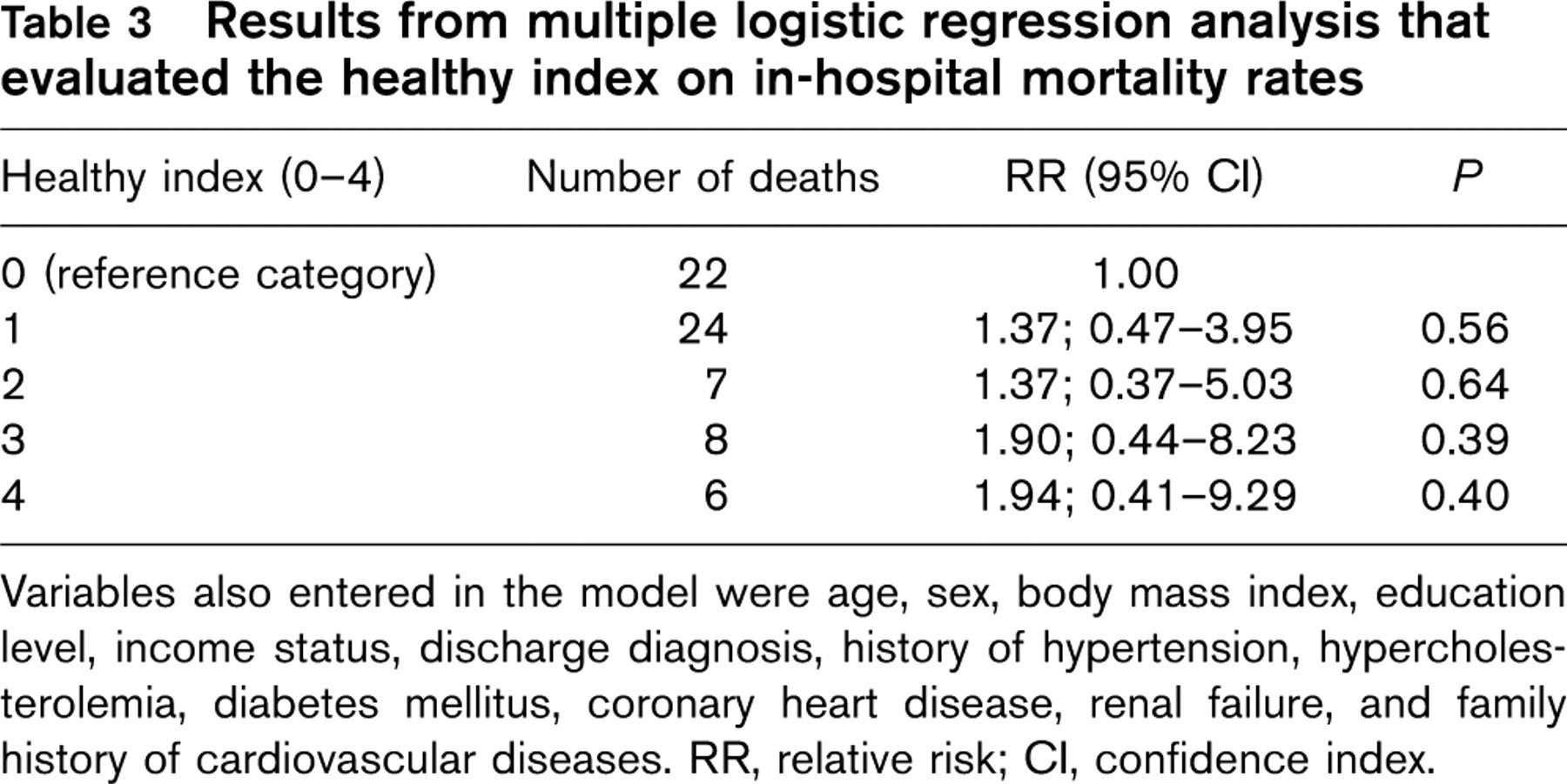
Variables also entered in the model were age, sex, body mass index, education level, income status, discharge diagnosis, history of hypertension, hypercholesterolemia, diabetes mellitus, coronary heart disease, renal failure, and family history of cardiovascular diseases. RR, relative risk; CI, confidence index.
Thirty-day follow-up
During the first 30 days following hospitalization precise information about vital status or rehospitalization due to coronary heart disease, angioplasty and coronary artery bypass surgery was retrieved from 1306 patients (1000 males). The number of events was 268 in males and 82 in females (P for sex differences = 0.001), while 23 of them were fatal (19 in males, P for sex differences = 0.003). The association of the ‘healthy index’ death or rehospitalization during the first 30 days following an ACS is presented in Table 4. As we can see presence of two or more protective factors (i.e. healthy index > 1) seems to be associated with significantly lower risk of having recurrent events, after adjusting for age, sex, body mass index, education level, income status, discharge diagnosis, history of hypertension, hypercholesterolemia, diabetes mellitus, coronary heart disease, renal failure, and family history of cardiovascular diseases. As in the case of in-hospital mortality, when we evaluated the components of the ‘healthy index’ on the event rate following hospitalization no significant associations were observed for individual components of the index on the investigated outcome. Moreover, male sex was the only factor that was positively associated (relative risk = 1.95, P < 0.001) with the 30-day prognosis, while, patients with myocardial infarction had 41% lower risk of having recurrent events than those with unstable angina (relative risk = 0.59, P < 0.001), after the aforementioned adjustments.
Results from multiple logistic regression analysis that evaluated the healthy index on 30-day outcome (death or re-hospitalization due to cardiovascular disease)
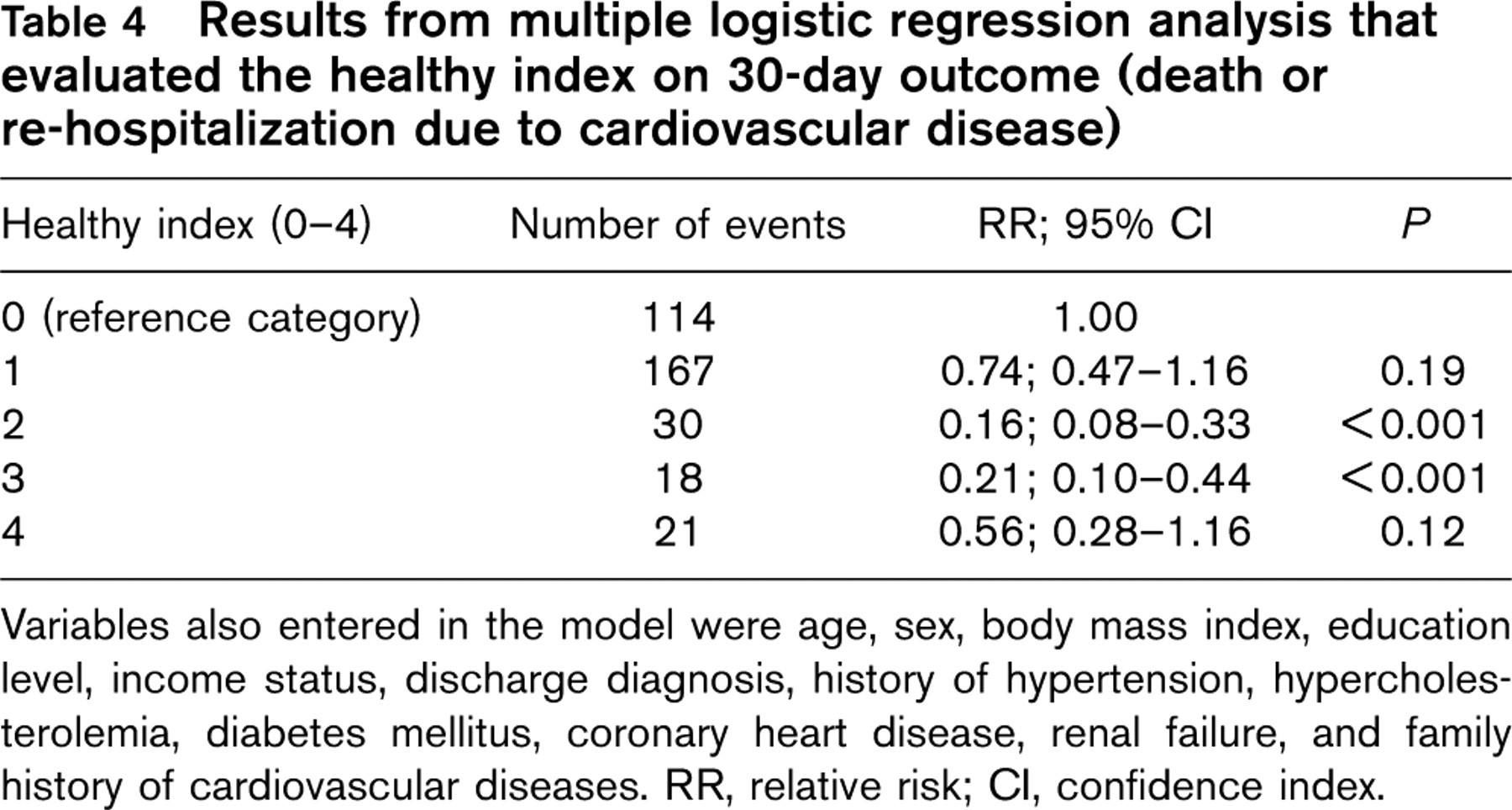
Variables also entered in the model were age, sex, body mass index, education level, income status, discharge diagnosis, history of hypertension, hypercholesterolemia, diabetes mellitus, coronary heart disease, renal failure, and family history of cardiovascular diseases. RR, relative risk; CI, confidence index.
Even after adjusting for obesity, hypertension, diabetes and history of coronary heart disease, however, residual confounding may still exist. Thus, we stratified the previous analyses by the presence of hypertension, diabetes, obesity and history of coronary heart disease. These analyses showed similar results (not presented in the text or tables) to those observed in the multiple regression models.
Discussion
In this work we evaluated the effect of a healthy lifestyle on the severity and the prognosis of patients who had had an acute coronary syndrome. In particular, we observed that adherence to the Mediterranean diet, physical activity, moderate alcohol consumption and abstinence from smoking for at least 15 years or non-smoking, were associated with less severe cardiac events and a better short-term prognosis of these patients, after controlling for various confounding factors.
Diet has long been associated with the development and progression of atherosclerosis. Dietary factors exert their influence largely through their effects on blood lipids and lipoproteins, as well as on the other established modifiable cardiovascular risk factors, with the exception of cigarette smoking. Several investigators during the past decades have associated diets rich in fruits, vegetables, non-refined cereals and low-fat dairy products with lower incidence of coronary heart disease and cancer [6–9, 26–28]. Mediterranean diet encompasses these dietary characteristics and has been associated with reduced incidence of coronary heart disease and cancer, since the 1960s. In particular, Ancel Keys and his colleagues from the Seven Countries Study attribute the lower incidence of coronary heart disease observed in southern European population compared to northern European and US participants, to their special dietary habits, the so-called Mediterranean diet [6]. Recently, Trichopoulos and Lagiou [28] reported that the gradual loss of the survival advantage of Mediterranean European citizens, compared with other European citizens, might be linked to the continuing abandonment by the former of their dietary traditions. Our results support these reports. In particular, we observed that greater adherence to the Mediterranean diet is associated with a significant reduction in markers of myocardial damage, as well as with a reduced rate of in-hospital mortality and recurrent events 1 month following hospitalization. Moreover, our findings were independent from the common cardiovascular risk factors, as well as family history of coronary heart disease. The investigated type of diet is low in saturated fat, high in monounsaturated fat, mainly from olive oil, high in complex carbohydrates, from legumes and high in fibre, mostly from vegetables and fruits [9]. Based on the results from the Seven Countries Study [6], the protective role of the Mediterranean diet against atherosclerosis was explained, mainly, due to the reduction of cholesterol and blood pressure levels. A few years ago, the findings from the Lyon Diet Heart study illustrated the potential importance of the Mediterranean dietary pattern, especially when compared with other recommended diets, like the Step-I diet [8]. It still remains a matter of debate, however, if the protective influence is primarily caused by single nutrients, such as dietary fatty acids, potassium or dietary fibre or if it can be attributed to the Mediterranean diet as a whole.
Alcoholic beverages are widely consumed throughout the world, while alcohol intake plays an important role in the Mediterranean dietary pattern since it is consumed regularly, in moderation (15–30 g of ethanol daily) and almost always during meals. It has long been reported that heavy alcohol consumption is hazardous to various body organs, and in several countries it is considered as one of the leading causes of preventable deaths, after smoking [29]. There is now, however, also a substantial body of evidence that the intake of light to moderate amounts of alcohol is associated with reduced morbidity and mortality from several cardiovascular conditions, particularly coronary heart disease [30]. The interpretation of these beneficial effects has been extensively discussed and it has been suggested that the effects on cardiovascular disorders might not be due to alcohol per se but to other confounding factors [31]. In our work, no significant association was observed between alcohol intake and the severity and short-term prognosis of ACS, when we controlled for various potential confounders. This may be attributable to the lack of any biological mechanism or to unknown confounding that may exist.
Based on several observational studies mortality or morbidity caused by coronary heart disease has been inversely associated with individuals' physical activity status [1, 2, 13]. In particular, some investigators report that even a single session of moderate to long duration exercise can reduce blood pressure, glucose and triglyceride levels and can increase high-density lipoprotein cholesterol levels. After controlling for various factors, our study showed that physical activity status is inversely associated with markers of myocardial damage, like troponin I and CKMB. On the other hand, physical activity status does not seem to be associated with in-hospital mortality, as well as with the short-term prognosis of patients with ACS. When physical activity was considered in the healthy index score, however, it seemed to significantly confer a reduction of in-hospital death rates and the number of recurrent events.
Finally, cigarette smoking is considered as one of the most significant modifiable risk factors for various chronic diseases, including cardiovascular, while stopping smoking has been associated with a substantial reduction in the risk of coronary heart disease. The benefits from stopping smoking, however, seem to be associated with the years since cessation [1, 3, 32, 33]. We confirmed the harm caused by cigarette smoking on the cardiovascular system, because we observed that cigarette smoking is positively associated with the severity of ACS, irrespective of various potential confounders.
Nowadays it is widely accepted from public health strategies that inappropriate diet and physical inactivity together with tobacco use have been recognized as the major risk factors for cardiovascular diseases. Recently, the INTERHEART study demonstrated a high prevalence of modifiable risk factors, including smoking and physical inactivity, in coronary heart disease patients [34]. Moreover, the investigators suggested that among others, smoking, consumption of fruits, vegetables and alcohol, as well as regular physical activity account for most of the risk of myocardial infarction worldwide in both sexes and at all ages in all 52 regions of the study. The NCEP ATP III suggested particular lifestyle changes, including diet and exercise, in order to reduce the prevalence of atherosclerotic disease [5]. In this study we revealed the association of lifestyle on the reduction of the severity of ACS. Adherence to the Mediterranean diet, moderate alcohol consumption, abstinence from smoking and physical activity were found to be associated with lower levels of markers of myocardial damage, as well as with better prognosis of these patients. Although the small number of in-hospital deaths or 30-day events observed in high healthy index categories (see Tables 3 and 4) may restrict our findings, we revealed that presence of two or more of the aforementioned protective factors (i.e. healthy index > 1) was significantly associated with about 70% lower risk of dying at hospital and with 80% lower risk of having recurrent events, irrespective of various potential confounders. Moreover, we observed that about 40% of the recurrent events are attributed to unfavorable lifestyle habits. Thus, it could be speculated that a substantial number of coronary patients could be prevented from having a second cardiac event if they have followed a healthier lifestyle. It is also of interest that the attributable risk, which indicates what percentage of in-hospital deaths are caused by unhealthy lifestyle habits, was about 10%. Although the number of deaths that could be prevented is relatively small, the observed reduction is of considerable importance from a public health point of view.
Limitations
Although this study has managed to evaluate the influence of lifestyle on ACS severity and prognosis, it relied on hypotheses concerning the possible mechanisms through which these effects are exerted, such as the favourable modification of the inherent thrombotic-lytic mechanisms, of the no or slow reflow phenomenon (peripheral embolism attenuation). No objective biochemical markers concerning coagulation, oxidative stress or inflammation status were available. Angiographic evidence was also lacking. Further studies might take upon them the task of providing such evidence.
Conclusion
Although dietary habits and lifestyle may change over time, generally they are characteristics that describe a person's way of living and reflect lifelong health behaviours. In this work we observed that among patients who had had an acute coronary syndrome, a healthy lifestyle was associated with less severe cardiac events and a significant reduction in the risk of death or re-hospitalization.
Footnotes
Acknowledgements
The authors would like to thank the field investigators of the GREECS study: Yannis Kogias, Yannis Mantas, Spyros Zombolos, Peter Stravopodis, Antonis Antonoulas, George Giannopoulos, Sophia Arapi, Theodoros Gialernios, Constandina Massoura, George Papanagnou, Antonis Karanasios, Lambros Rizos, Michalis Mparmparoussis, George Kassimatis, Skevos Sideris, Nick Daskalopoulos for their support in the clinical evaluation and Alexander Chalamandaris for the database management.