
Abstract
Aim
To evaluate the impact of predictors of adopting a healthy lifestyle in Swedish schoolchildren. Methods A sample of 1409 Swedish schoolchildren (mean age 12.5 years) representative of different socio-economic and geographical living areas participated in a questionnaire-based survey on healthy habits and knowledge of healthy behaviour. A logistic regression analysis was performed to identify intrapersonal, social and environmental predictors of healthy habits.
Results
A normal body mass index (intrapersonal determinant) was connected to refraining from tobacco (P<0.05). For children to perceive family (P<0.001), themselves (P<0.001), or someone else (P<0.01) as a source of inspiration (social determinant) to be physically active was related to a high physical activity level. Paternal (P=0.01) and maternal (P<0.001) attention to the use of tobacco (social determinant) was of importance for children to refrain from such habits. To live in a socio-economically wealthy area (environmental determinant) was of importance for healthy food choices (P<0.01) and physical activity (P<0.05). Children from rural (P<0.01) areas (environmental determinant) were more physically active than children from urban areas.
Conclusion
Social aspects such as parental support for physical activity and refraining from tobacco were found to be important for healthy behaviours. Moreover, environmental factors such as socio-economic and geographical living area favourably influenced food choices and physical activity. Parental attitudes and economy are therefore important for physical activity, healthy food choices and refraining from tobacco in children. Consequently, future interventions need to address the psychological and environmental influences of the home environment through the active involvement of parents, even in school-based interventions.
Introduction
Adverse lifestyle changes accompanying industrialization, urbanization, and increased discretionary income increase the degree of exposure to cardiovascular disease (CVD) risk factors [1]. The early introduction of a healthy lifestyle is essential in the prevention of CVD and several other diseases [2], as health behaviours have been found to track from childhood to adulthood [3]. The initiation of smoking before the teenage years has been associated with regular smoking in young adults [4]. The eating patterns of children and adolescents have changed considerably over time. Not least, increasing exposures to free carbohydrates, contributing to excess calorie intake, have become more common. Diets too rich in fat and too low in fruit and vegetable content are another concern [5, 6]. While evidence for the health benefits of fruit and vegetables grows [7, 8], nutritional surveys reveal that children are not meeting the suggested minimum consumption of 400 g/day [9, 10].
Daily physical activity constitutes the foundation of a healthy lifestyle. At least 50% of children and adolescents are insufficiently physically active [11–13]. Physical activity and inactivity track from adolescence to young adulthood [14]. TV viewing has been associated with obesity in children, adolescents and adults [15], because TV viewing is linked to reduced energy expenditure and the increased intake of snacks [16].
Correlates of physical activity have been identified using an ecological model [17, 18]. This model hypothesizes that physical activity is influenced by three domains: (i) intrapersonal (biological, psychological, and behavioural influences); (ii) social (family or peer support, modelling); and (iii) environmental (facilities, communities, accessibility, etc.) [17].
The aim of the present study was to test this hypothesis further by evaluating the impact of predictors from these three dimensions for adopting a healthy lifestyle in Swedish schoolchildren.
Methods
Sample
In May 2003, a random sample of 2084 schoolchildren from 86 sixth grade classes in 78 schools were invited to the present investigation, originally aimed at an evaluation of an educational programme, ‘An Adventure with Pelle Pump', intended to improve knowledge on cardiopulmonary health and increase healthy behaviours. A detailed description of the study outline has been given elsewhere [19]. Of particular importance for the present report is that the sample was stratified for socioeconomic and geographical areas. Questionnaires were distributed to the respective class teachers with a letter explaining the nature of the project. They were asked to let the children answer the questionnaires during an ordinary lesson, without influencing them with any instructions besides those given in the letter and in the questionnaire.
The study was approved by the Ethics Committee of the Karolinska Institutet, and the children were informed that they could choose not to complete the questionnaire or any of the individual questions at any time.
The questionnaire
The questionnaire, designed to be completed in approximately 30 min, was administered in a classroom setting and included (besides demographic questions on sex, weight and height) 16 questions on health knowledge and 39 on health behaviour, including physical activity, nutrition and refraining from tobacco. Each question on health behaviour contained response alternatives varying from ‘healthy’ (score 4) to ‘unhealthy’ (score 1). Indices were derived for physical activity, nutrition and refraining from tobacco by multiplying the score from each question with a weight factor, relating to time and importance to health, and thus a high index value reflected a healthy behaviour. Details of this process and the validation of the questionnaire have been described in detail previously [19].
Definitions
For the correlates of the domains studied (intrapersonal, social and environmental), an ecological model was used [17]. In the present study, this model was applied to all three studied behaviours.
The intrapersonal domain included sex, age and body mass index (BMI). The BMI was calculated by dividing weight in kilograms by squared height in meters. In youth, BMI values are, according to Cole et al. [20], defined as cut-off points, which pass through 25 and 30 kg/m2 at the age of 18 years.
The social domain included sources of inspiration (multiple answers were possible) for the children to be physically active and the children's perception of their parent's level of attention to their smoking. The following sources of inspiration for physical activity were possible answers: family, coach, physical education teacher, media, the child itself, or someone else (i.e. a dog, idol, or someone other than those previously mentioned). The children graded their perception of the parental level (paternal and maternal attention separately) of attention to smoking on a four graded scale, from ‘pays no attention at all’ to ‘pays great attention'.
The environmental domain included socio-economic living area and living in a rural or urban area. In the present study, socio-economic living area was categorized into the following four categories: S1, very affluent plus affluent; S2, average affluent plus average; S3, average neglected plus neglected; S4, poor plus very poor [21]. A rural living area was defined as a community with less than 30 000 inhabitants. The communities included ranged from 7100 to 29 800 inhabitants, with a mean of 14017.
Statistical analysis
Each index (physical activity, nutrition and refraining from tobacco) was, before statistical analyses, dichotomized as healthy (1) or unhealthy (0) behaviour. Logistic regression analyses were performed with each behaviour index as a dependent variable and the predictors from the three domains as independent variables.
The relationship between the predictors in the social domain and the predictors in the intrapersonal and environmental domains was analysed using two-by-two tables. Significance levels for these tables were calculated using an ordinary chi-squared test.
A two-sided P value less than 0.05 was regarded as statistically significant. No correction for multiple testing was performed. All analyses were performed using SAS version 9.1 (SAS Institute, Cary, North Carolina, USA).
Results
A total of 2084 questionnaires were distributed, of which 1422 (68%) were returned. Thirteen of the returned questionnaires were excluded because of missing replies to more than 20% of the questions analysed. The final number of children included in the present study was 1409, with a mean age of 12.5 years. The characteristics of the children included are presented in Table 1.
As depicted in Figure 1, health behaviours were influenced by all domains. A normal BMI was connected to a beneficial tobacco index (P < 0.04). To perceive your family (P < 0.0001), the child itself (P < 0.0001) or someone else (P < 0.003) as sources of inspiration to be physically active increased the physical activity index. Paternal (P < 0.005) and maternal (P < 0.001) attention to the children's tobacco use were of importance for children to refrain from tobacco. To live in a socio-economically wealthy area was beneficial for the nutrition (P < 0.002) as well as the physical activity indices (P< 0.04). Children from rural areas (P < 0.005) were more physically active than children from urban areas.
The distribution of social predictors, based on the intrapersonal and environmental predictors, in different groups of children, is described in Table 2. Socioeconomic living areas S1-S3 were merged, as differences were considered low between these groups of children, and thereafter compared with S4 in these analyses. As seen in Table 2, perceiving themselves as a source of inspiration for physical activity varied significantly between all groups of children. Perceiving physical activity to be of great importance to themselves was most frequent among girls (75%) and children living in urban settings (75%), and was less frequent among children living in socio-economically poor and very poor areas (62%) and overweight and obese children (60%).
Pertinent characteristics of the children included presented as a percentage, unless otherwise stated
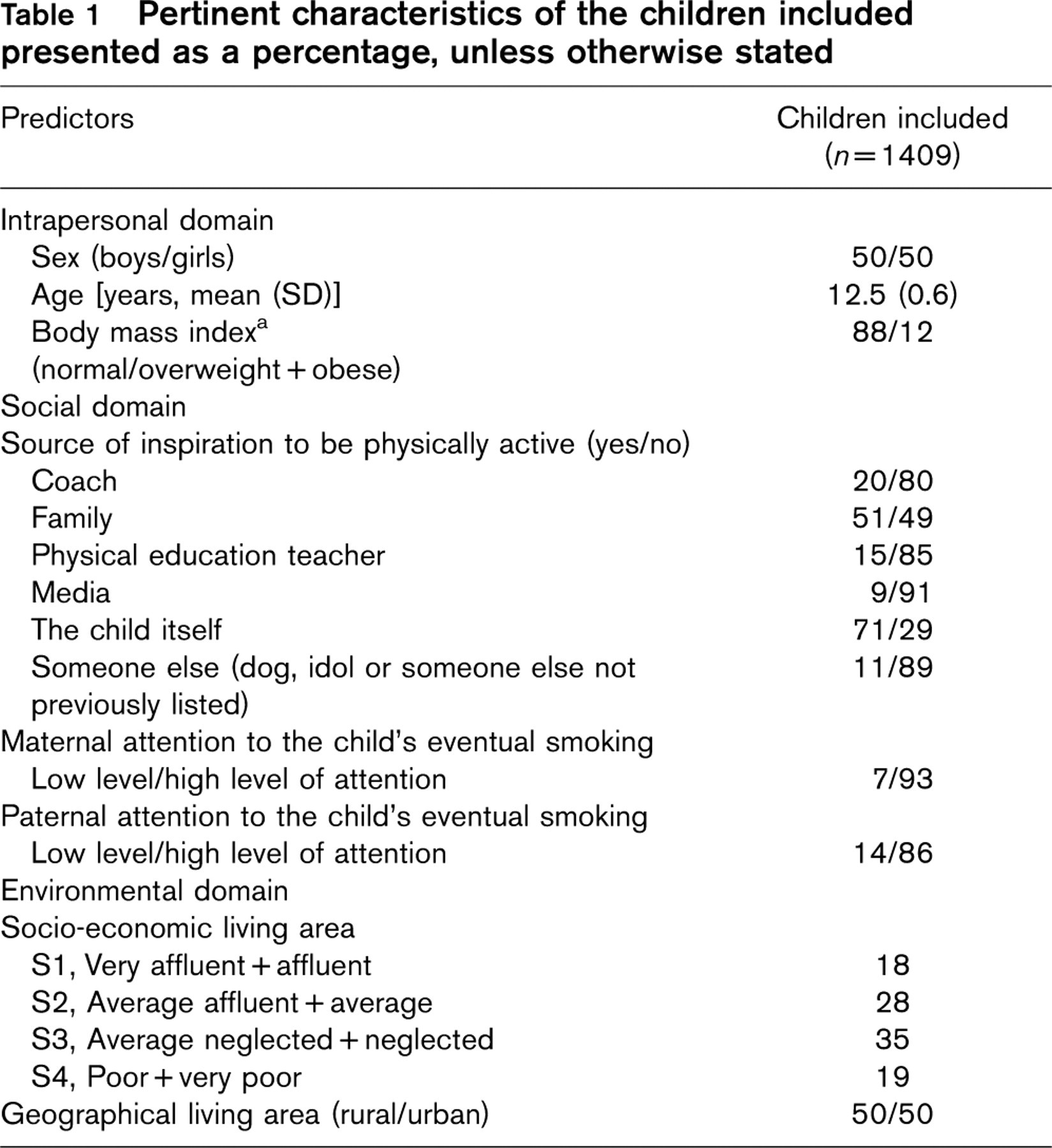
a Body mass index (BMI) levels classified according to international cut-off points for BMI for overweight and obesity by sex, defined to pass through BMI of 25 and 30 kg/m2 at age 18 years [20].
Discussion
Ecological models of health behaviour posit that multiple factors determine individual behaviours. The model applied in the present study, originally developed for physical activity, suggests that one should address the characteristics at many levels and consider the integration and interaction of the factors within each of the three domains intrapersonal, social and environmental [17, 22]. In the present study, this ecological model [17] was applied on three health behaviours, physical activity, diet and refraining from tobacco. All domains were of importance for health behaviours in Swedish school children. The intrapersonal domain, namely age, sex and BMI, is perhaps more likely to influence the type and extent of behaviour, but might not serve as a major reason for a healthy behaviour. In contrast, social and environmental mediators are presumed to have a more direct impact on health behaviours (Fig. 2) [17]. These two domains were of greatest importance in the present population, since the main finding was that parental influence was of great importance for children to be physically active and to refrain from the use of tobacco. Moreover, the health behaviour was significantly influenced by the socio-economic and geographical living area.
Intrapersonal domain
The studied aspects of the intrapersonal domain were only marginally related to health behaviours in the present group of children. We have previously shown [13] that age is of great importance for a healthy behaviour. An increase from 11.5 to 13.5 years was related to a considerable decrease in healthy behaviours. In the present study, the children were all of the same age, which is why age was not analysed as a predictor. Sex did not determine health behaviours, but sex differences as regards all three health behaviours have been reported previously [23–25]. In concordance with these reports we showed in a recent report that boys are more physically active and smoke to a greater extent than girls, whereas girls have a healthier dietary behaviour than boys [13]. A normal BMI was significantly related to a beneficial tobacco index. Our data do not provide an explanation of this finding, which may be worth further exploration.
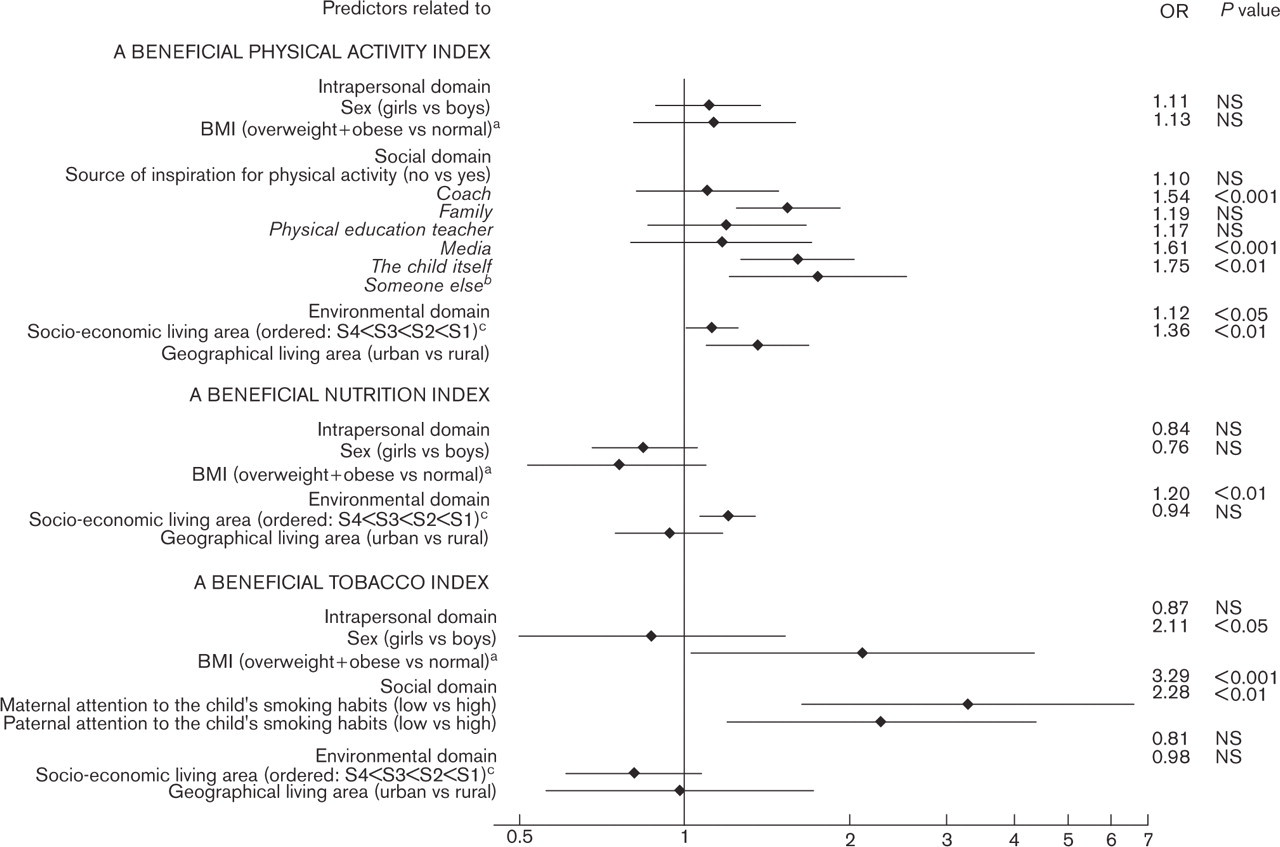
Odds ratio (OR) of impact of predictors on lifestyle habits, i.e. physical activity, nutrition and tobacco. A high index value equals a healthy behaviour. aBody mass index levels classified according to Coleet al. [20]. bSomeone else: dog, idol or someone else not previously mentioned. cSocio-economic living area: S1, very affluent + affluent; S2, average affluent+average; S3, average neglected+neglected; S4, poor+very poor.
In the present study, BMI was not significantly related to diet or physical activity. There is a complex and inconsistent relationship between physical activity and overweight in children [25]. The evidence linking eating patterns with overweight in youth is contradictory and inconclusive. Energy intake is not reliably associated with weight status in epidemiological studies, as a result of an under-reporting of food intake by overweight individuals [26].
Social domain
Physical activity was positively related to perceiving your family, yourself or someone else (i.e. dog or idol) as a source of inspiration to be physically active. A high level of physical activity relates to perceptions of enjoyment, self-efficacy, competence, positive attitudes towards activity, and a perception of few barriers and many benefits [27, 28]. This may explain the high proportion of children who ranked themselves as a major inspiration to be physically active. Sallis et al. [18] found that parental mental support was positively associated with physical activity, whereas other social variables such as peer influence, subjective norms and parental practical support with transportation, seemed to be of less importance.
A somewhat surprising finding was the lack of influence by coaches and physical education teachers on the physical activity index. This might reflect the substantial cut back in time scheduled for physical education in the Swedish school system during the past decade. Contributing factors may also be a lack of understanding of and personal engagement in this important fostering role. Teachers may turn children away from healthy habits by less insightful physical education, or by paying too much attention to competitive rather than health-promoting activities [18, 22]. Engaged and knowledgeable teachers and coaches can, on the contrary, have a strong and favourable influence on the young generation, thereby reinforcing parental efforts. Today's parents have longer work hours, and many families consist of only one parent. Parents increasingly rely on schools and teachers to take on great responsibilities when it comes to teaching their children on health variables such as diet and physical activity. This view gains support from the finding that children in socio-economically poor areas considered their coaches as an inspirational resource to a greater extent than children in wealthier areas. Increased attention to extra curricular activities and physical education time and content thus seems to be particularly important in such living areas. Teachers need to be given the potential to direct the children towards a lifetime of involvement with sports and physical activities. However, parents need to recognize that they are the greatest inspiration for their children's health choices, and this responsibility should not be transferred to teachers or coaches.
Proportions (%) of the connection between intrapersonal and environmental predictors with social predictors
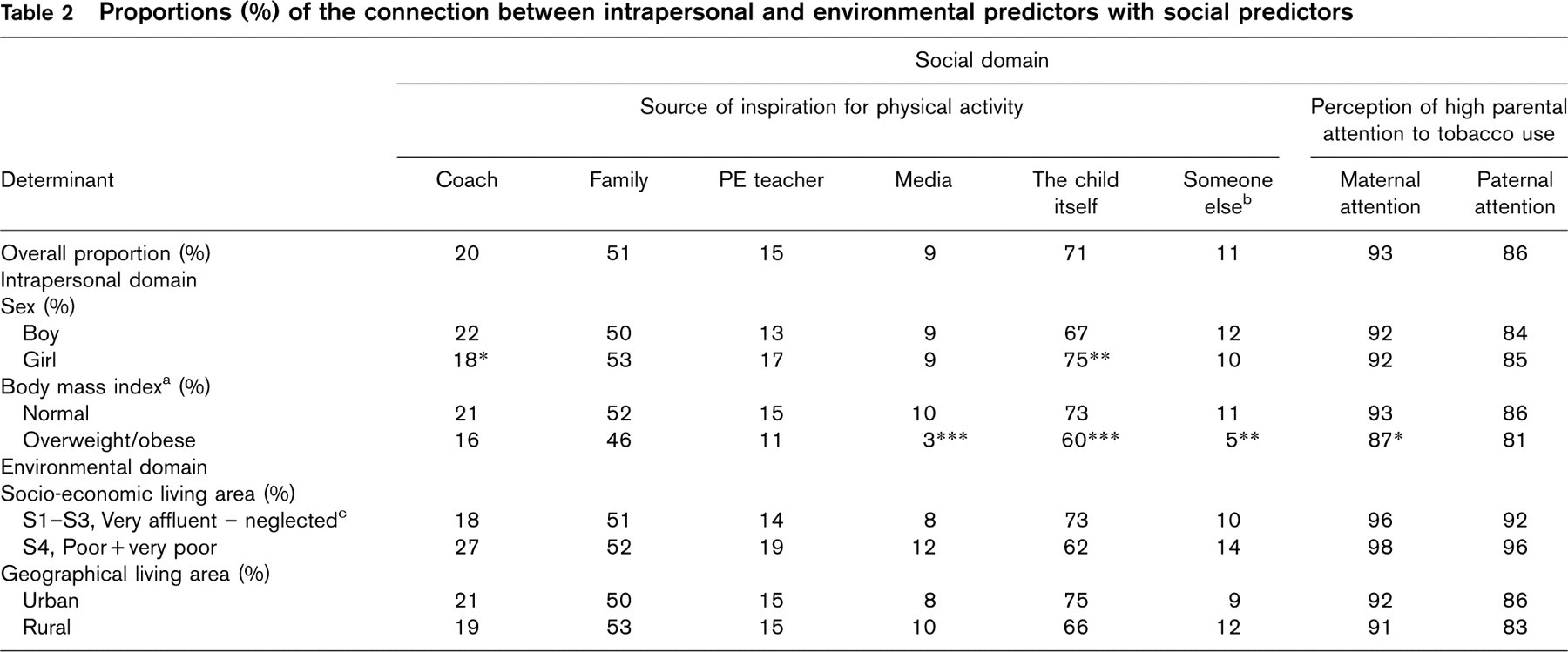
aBody mass index (BMI) levels classified according to international cut-off points for BMI for overweight and obesity by sex, defined to pass through BMI of 25 and 30 kg/m2 at age 18 years [20]. bSomeone else: dog, idol or someone else not previously mentioned. cThe distribution of social variables in socio-economic living areas S1-S3 was low and therefore these three groups were merged and thereafter compared with S4 in the chi-squared analysis. Differences between groups of children are described as: ∗P < 0.05, ∗∗P ≤ 0 .01, ∗∗∗P ≤ 0.001; unmarked proportions, differences not significant.
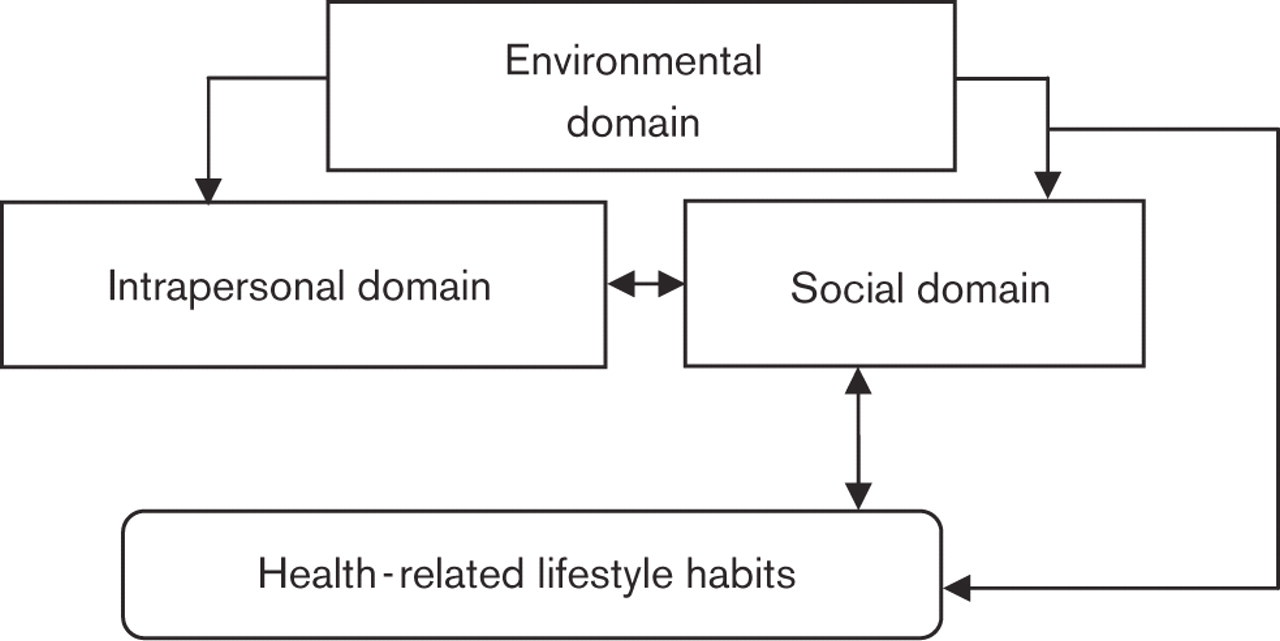
Modified version of the ecological model of physical activity after Spence and Lee [17], when applied on all three health behaviours studied (physical activity, nutrition and tobacco use).
Parents often perceive that there is nothing they can do to prevent their child from becoming a smoker [29]. However, in the present study we found that parental attention to smoking habits was of the utmost importance for the children to refrain from tobacco. This is in line with findings that negative parental attitudes on smoking are protective against adolescent tobacco use [30–32]. Castrucci et al. [33] even found parental opinions to have a mediating effect on the influence of children observing their parents smoking. Therefore, preventing the initiation and continuation of smoking among adolescents will require interventions that address both individual and parental attitudes with respect to tobacco.
Environmental domain
Children from wealthy or rural areas have a higher reported physical activity than those from less affluent or urban areas. Accumulating evidence underlines the significant role of socio-economic status on physical activity and inactivity [18, 34]. One explanation may be a better link between knowledge on the importance of an active lifestyle and the actual access to sports facilities, including both arenas and the economic capability to buy needed equipment and to provide transportation to various activities. It has been reported that children from more deprived areas often do not have the same physical activity and recreation opportunities, including fewer convenient facilities for physical activity, compared with children from higher income families [18, 35]. Furthermore, industrialization increases transportation involving less energy expenditure, which contrasts with the means of transportation for children in rural areas and may explain the higher levels of physical activity within their daily life.
The only predictor significantly related to healthy dietary variables among the children included was to live in a socio-economically wealthy area. This might be explained by the fact that family income often presents a barrier to healthy eating. Children in lower socio-economic groups consume less fruit and vegetables and have a higher intake of fat compared with children from more affluent areas [36]. One study reported that as many as 40% of adolescents with a lower income background did not meet the recommended daily consumption of fruit and vegetables [37]. We have previously shown that, in this population of children, only approximately 10%, regardless of socio-economic living area, consumed fruit and vegetables more than once per day [13]. Sandvik et al. [38] reported that European children have a positive attitude towards fruit and vegetable consumption in general. However, the actual consumption remains below the recommended levels in all European Union countries. Consequently, promoting healthier diets among children requires a multifaceted approach targeting children, parents, families and schools and also including societal and political approaches, not the least as regards pricing.
Study limitations
As has been pointed out previously [13, 19], there are limitations in studies based on self-reported information, such as the potential for self-report bias and errors in recall, which need to be recognized. Information on dietary patterns, physical activity variables and smoking habits were available only in a frequency domain, but not as the total volume of these variables. When studying predictors of healthy behaviour it was also a limitation that no aspects from the social domain were considered when designing the questions on dietary habits. Therefore, the social domain could not be analysed as regards such habits. Future questionnaires should preferably cover all aspects and domains of the ecological model. Furthermore, when analysing some of the predictors in the social domain, groups were rather small, and a weakness in power might be the reason why there were no significant impacts on health behaviours.
Conclusion
Ecological models of health behaviours posit that multiple factors determine individual behaviours. In the present study it was found that the three studied domains: intrapersonal, social and environmental, were of importance for health behaviours in Swedish school children, and in particular social and environmental. Social aspects such as parental support for physical activity and refraining from tobacco were found to be of direct importance for these behaviours. Furthermore, environmental factors such as socio-economic living area and geographical living area were of impact for dietary habits and physical activity. Therefore, not only do parents influence the health behaviours of their children through where they choose to live and their income level, but parental support and attention to health behaviours are also of major importance.
Consequently, future interventions need to address the psychological and environmental influences of the home environment through the active involvement of parents, even in school-based interventions.
Footnotes
Acknowledgements
The authors would like to extend their sincere gratitude to all the children who participated in this study and to their teachers for helping with the distribution of the questionnaires. They would also like to thank Associate Professor John Öhrvik, for expert statistical advice. This study was supported by non-committed grants from the Swedish Heart and Lung Foundation.