
Abstract
Background
Methods
Results
Conclusions
Introduction
There is a large difference in incidence of coronary heart disease (CHD) between Northern Ireland and France that is only partly explained by the classic risk factors [1], indicating that novel risk factors are likely to play a role in CHD cause [2–4]. The Prospective Epidemiological Study of Myocardial Infarction (PRIME) was set up to investigate possible reasons for the difference in CHD incidence between Northern Ireland and France. There are four centres: three in France: Lille (north), Strasbourg (east) and Toulouse (southwest), and one in Belfast, Northern Ireland.
Bilirubin, a bile pigment formed during haem catabolism, scavenges peroxyl radicals [5] and attenuates radical-mediated damage to lipids and proteins [5, 6]. Bilirubin also has antioxidant properties [5, 7, 8], independent of whether it is unconjugated, conjugated, free or albumin bound [7, 9, 10]. It is a better antioxidant at low oxygen tensions [5], such as found within the arterial wall, surpassing α-tocopherol [7]. Physiological concentrations of bilirubin prevent low-density lipoprotein (LDL) oxidation [6] but requires vitamin E as a coantioxidant [6, 9].
Because the LDL oxidation-mediated inflammatory response in the arterial wall is considered crucial to the development of the atherosclerotic lesion [2, 11–13], and because bilirubin inhibits LDL oxidation [6], it was hypothesized that bilirubin may have a beneficial role in atherogenesis and so be negatively associated with CHD incidence. A number of cross-sectional [14–16] and prospective studies [17, 18] have shown this to be the case, an observation strengthened by a recent meta-analysis [19]. One prospective study, however, demonstrated a U-shaped relationship between serum bilirubin and ischaemic heart disease risk [20]. Thus, the aim of this study was to investigate prospectively the relationship between bilirubin concentration and CHD risk.
Methods
Recruitment and examination methods have been described previously [2, 21], but will be summarized briefly.
Population recruitment
Between 1991 and 1993, 10 593 men aged 50-59 years were recruited from industry, various employment groups and general practice. The sample was recruited to match broadly the social class structure of the population.
Personal history
Each participant completed self-administered questionnaires on demographic, socio-economic factors and dietary habits. Additional data on tobacco and alcohol consumption, and physical activity were collected during clinic attendance, and the London School of Hygiene Cardiovascular (Rose) Questionnaire for Chest Pain on Effort and Possible Infarction [22] was also administered.
Clinical examination
Baseline investigations included a standard 12-lead electrocardiogram, and standardized blood pressure measurement. Anthropometric measurements included height, weight and waist and hip circumferences. Body mass index (BMI) and waist-hip ratio (WHR) were then calculated.
Pre-existing coronary heart disease
Participants were considered to have CHD at entry if they reported one of the following: myocardial infarction (MI) or angina pectoris diagnosed by a physician; electrocardiographic evidence of MI; a positive answer to the Rose questionnaire. There were 9758 participants without evidence of CHD at study entry.
Case-control selection and follow-up
Participants completed a clinical event questionnaire annually. Coronary events were defined as the presence of at least one of the following: non-fatal MI, death from CHD or angina pectoris. Events were validated by an independent medical committee [21].
Five-year follow-up has been completed; 335 new CHD cases were identified. Each case was matched to two controls who were study participants of the same age (± 3 years), recruited in the same centre on the same day as the corresponding case (± 2 two days) and were free of CHD on the date of the ischaemic event of the case, giving 670 controls.
Laboratory measurements
Venous blood samples were collected after a 12-h fast. Measurement of total and high-density lipoprotein (HDL) cholesterol, triglycerides, apolipoprotein B (apo B), glutathione peroxidase (GPx), fibrinogen, apolipoprotein A1 (apoA1) and Lp(a) were performed during the recruitment phase on all subjects. Glucose, bilirubin, cystatin C, B12, folate and homocysteine were also measured in samples collected during the recruitment phase, but only in subjects involved in the case-control study, that is, when the 5-year follow-up was complete.
Laboratory measurement of total cholesterol, HDL, triglycerides, apo B, fibrinogen, apoA1, Lp(a) and vitamin E have been described previously [2]. Serum GPx was measured as an index of selenium status using an automated centrifugal analyser [23]. Bilirubin and glucose were measured using automated colorimetric assays (Sigma Diagnostics, UK; Randox, UK). Homocysteine was measured by high-performance liquid chromatography according to the method of Ubbink and colleagues [24]. Serum folate and vitamin B12 were measured simultaneously by radioassay (ICN Pharmaceuticals, USA). Cystatin C was measured by immunonephelometry (Dade Behring, Reuil-Malmaison, France).
Dietary score
Participants completed a dietary questionnaire for four categories of fruit and vegetable intake: citrus fruits, other fruits, raw vegetables, and cooked vegetables. The usual intake of a standard portion of fruit or vegetables for each category during the last week was indicated using the following scale: greater than once per day; daily; three or four times per week; twice per week; once a week; twice a month; once a month; less than once per month/never. The fruit and vegetable intake score was calculated as sum of number of servings per day of fruit and vegetables.
Statistical analysis
Variables with a skewed distribution (bilirubin, glucose, fibrinogen, apo B, folate, B12, Lp(a), homocysteine and triglycerides) were logarithmically transformed and results summarized as geometric means and interquartile ranges. Pearson correlation coefficients were used to investigate the association between bilirubin and other variables separately in cases and controls. Associations between bilirubin and centre, smoking and alcohol intake were examined using one-way analysis of variance (ANOVA) and independent sample t-tests, separately in cases and controls. Comparisons between cases and controls were made using ANOVA, adjusting for case-control triplets by the inclusion of terms representing triplets in the model. For continuous variables, comparisons were summarized as a difference in means between cases and controls, adjusted for triplets. For variables requiring log transformation the data were summarized as a ratio of geometric means in cases and controls, adjusted for triplets. Conditional logistic regression was used to examine the relationships between smoking, alcohol intake and physical activity and case-control status.
To assess the relationship between bilirubin concentration and risk of CHD, the case-control cohort was divided into fifths using quintiles of bilirubin concentration in the control group. Conditional logistic regression was performed to estimate the odds of CHD risk for each fifth relative to the lowest fifth. Linear and quadratic terms were used to model non-linearity in the relationship between risk and the fifths of bilirubin concentration. Two further conditional logistic models were then fitted. In the first model, the odds ratios for bilirubin concentration were adjusted for classic risk factors, namely WHR, diastolic blood pressure (DBP), smoking, total cholesterol, HDL and triglycerides. In the second model, the odds ratios were adjusted for both classic and putative risk factors which have either been linked with CHD risk in the literature or were found to be correlated with bilirubin: namely glucose, alcohol, physical activity, apoB, fibrinogen, GPx and cystatin C.
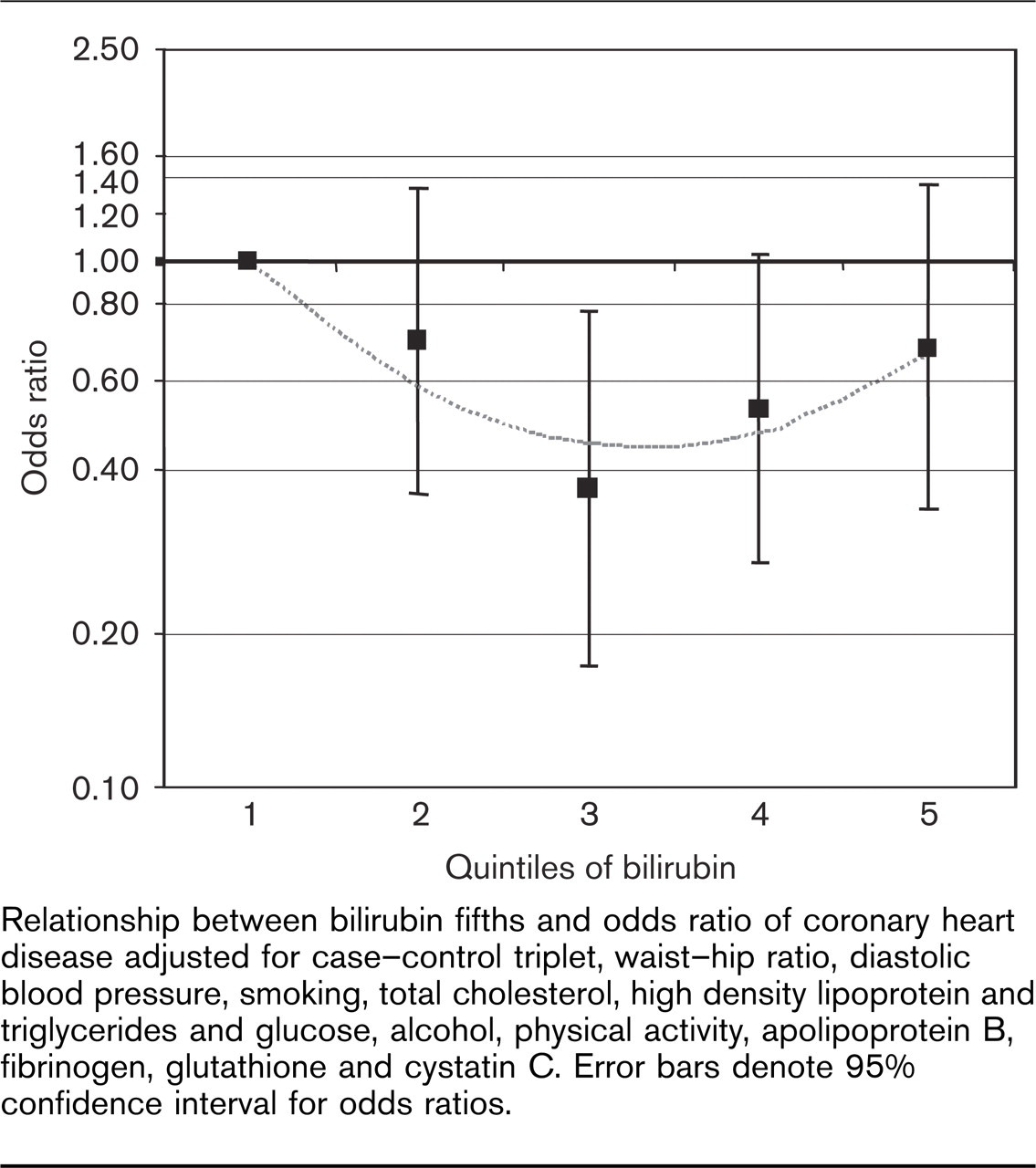
Relationship between bilirubin fifths and odds ratio of coronary heart disease adjusted for case-control triplet, waist-hip ratio, diastolic blood pressure, smoking, total cholesterol, high density lipoprotein and triglycerides and glucose, alcohol, physical activity, apolipoprotein B, fibrinogen, glutathione and cystatin C. Error bars denote 95% confidence interval for odds ratios.
The effect of α-tocopherol on the relationship between bilirubin concentration and CHD risk was investigated by adding it to the conditional logistic model containing bilirubin concentration. To determine if there was effect modification by α-tocopherol, a test for interaction was performed. However, α-tocopherol values were not available for all subjects, and therefore its inclusion into the conditional logistic model decreased the number of observations contributing to the analysis to 216.
The composite effect of dietary antioxidant intake on the relationship between bilirubin concentration and CHD risk was investigated by examining dietary fruit and vegetable intake. To test for interaction between bilirubin and fruit and vegetable intake, dietary score was divided by tertiles into thirds and conditional logistic regression performed. To test for effect modification by fruit and vegetable intake or smoking, namely a different relationship occurring between a risk factor and CHD risk in the presence of different fruit and vegetable intake categories or different smoking status, an interaction term was fitted.
All odds ratios are quoted with 95% confidence intervals. To test for differences between countries in the relationship between bilirubin and CHD, interaction terms were added in the conditional logistic regression model.
Statistical significance was assessed as P < 0.05. Analyses were performed using SPSS 11.0 software (SPSS Inc., Chicago, Illinois, USA) and STATA 8.0 statistical software (Statcorp, College Station, Texas, USA).
Results
Data on bilirubin were available in 216 cases and 434 matched controls. A total of 559 subjects contributed to the matched analysis as only potential triplets for which the case patient and at least one control had data could be included in the analysis.
Bilirubin was significantly positively correlated with HDL cholesterol in cases and controls; and significantly negatively correlated with triglycerides and apoB in cases and controls and with BMI, WHR, systolic blood pressure, DBP, total cholesterol and fibrinogen in controls only.
There was no significant difference in bilirubin concentrations between either the three French centres, or between Belfast and the French centres combined, for cases or controls.
There was no significant difference in bilirubin concentration according to weekly alcohol intake (0 g/week; < 225 g/week or ≥ 225 g/week) for cases (P = 0.78), controls (P = 0.26) or cases and controls (P = 0.35).
Bilirubin concentration did not differ significantly according to smoking status (never, current or ex-smoker) for cases (P = 0.13), controls (P = 0.49) or when cases and controls were considered together (P = 0.08).
Table 1 shows comparisons of baseline risk factors between cases and controls, adjusted for the triplet grouping. Bilirubin concentration was found to be significantly lower in cases than in controls.
A U-shaped pattern was evident between bilirubin concentration and CHD risk, with CHD risk significantly lower for bilirubin concentrations in the third, fourth and fifth fifths (see Table 2), compared to concentrations in the first fifth. This U-shaped pattern persisted in the adjusted models, with CHD risk significantly lower for bilirubin concentrations in the third and fourth fifths only. A significant quadratic relationship was found which persisted after adjustment for both classical risk factors and classic plus putative novel CHD risk factors (Fig. 1).
Neither α-tocopherol nor fruit and vegetable intake were found to alter the relationship between bilirubin and CHD risk (α-tocopherol, test for interaction χ2 = 1.58, df = 4; P = 0.81; fruit and vegetable, test for interaction χ2 = 2.16, df = 8, P = 0.98).
There was no difference in the relationship between bilirubin level and CHD risk between France and Northern Ireland (χ2 = 5.95, df = 4, P = 0.20).
Comparison of baseline risk factors between cases and controls by analysis of variance with inclusion of terms for triplet in the model
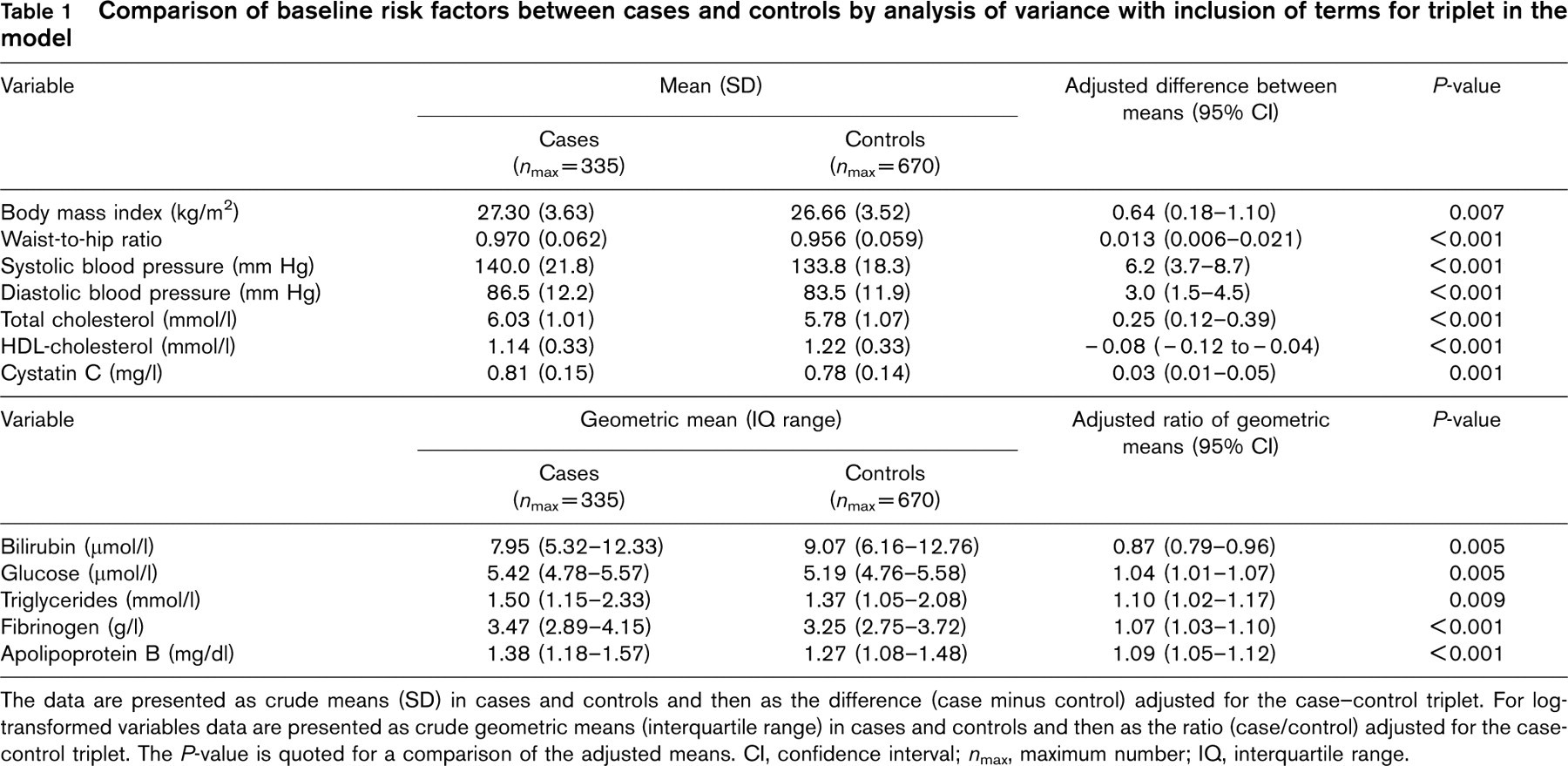
The data are presented as crude means (SD) in cases and controls and then as the difference (case minus control) adjusted for the case-control triplet. For log-transformed variables data are presented as crude geometric means (interquartile range) in cases and controls and then as the ratio (case/control) adjusted for the case-control triplet. The P-value is quoted for a comparison of the adjusted means. CI, confidence interval; n max, maximum number; IQ, interquartile range.
Conditional logistic regression analysis showing the unadjusted and adjusted odds ratio of coronary heart disease risk for fifths of bilirubin based on control values
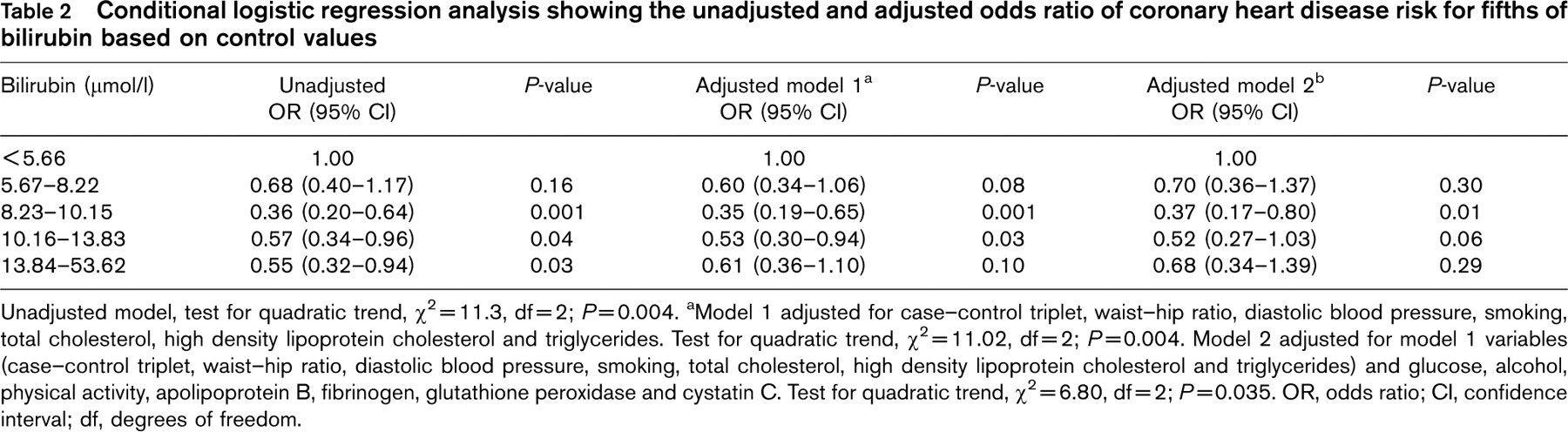
Unadjusted model, test for quadratic trend, χ2 =11.3, df = 2; P =0.004. aModel 1 adjusted for case-control triplet, waist-hip ratio, diastolic blood pressure, smoking, total cholesterol, high density lipoprotein cholesterol and triglycerides. Test for quadratic trend, χ2 = 11.02, df = 2; P = 0.004. Model 2 adjusted for model 1 variables (case-control triplet, waist-hip ratio, diastolic blood pressure, smoking, total cholesterol, high density lipoprotein cholesterol and triglycerides) and glucose, alcohol, physical activity, apolipoprotein B, fibrinogen, glutathione peroxidase and cystatin C. Test for quadratic trend, χ2 =6.80, df = 2; P = 0.035. OR, odds ratio; CI, confidence interval; df, degrees of freedom.
Discussion
This study adds weight to the hypothesis that bilirubin concentration affects CHD risk [25].
In PRIME, bilirubin concentrations were significantly lower in cases than in controls, in agreement with the Framingham Offspring Study [17]. Our results differ, however, in that a U-shaped pattern was observed between bilirubin and CHD risk, which persisted even after adjustment for other cardiovascular risk factors.
A similar U-shaped relationship was found in the British Regional Heart Study (BRHS) [20], which again persisted after adjustment for lifestyle factors, biological factors and pre-existing disease. Given that bilirubin requires vitamin E as a co-antioxidant it was hypothesized that if participants with high bilirubin were vitamin E deficient, bilirubin would be less atheroprotective, weakening the inverse association between bilirubin concentration and CHD, thus producing the observed quadratic association between bilirubin and CHD risk. The relationship between bilirubin concentration and CHD risk in PRIME, however, was not modulated by α-tocopherol concentrations. It is likely that PRIME lacked power to detect a relationship between bilirubin and α-tocopherol. Alternatively, the relationship between α-tocopherol and bilirubin may be more complex, involving modulation by other micronutrient factors, such as ascorbic acid. The composite effect of dietary antioxidant intake, however, neither confounded nor modified the relationship between bilirubin and CHD risk. This negative finding does not rule out an effect of α-tocopherol and other micronutrient factors, as a correlation between dietary fruit and vegetable intake and serum levels of antioxidants and micronutrients was not established.
In the BRHS [20] participants with bilirubin in the highest fifth, with a concentration greater than or equal to 17 μmol/l, had liver enzymes measured. Participants with high bilirubin and elevated alanine transaminase and aspartate amino transferase had an even greater risk of CHD than those with high bilirubin only, suggesting an interaction between bilirubin, elevated liver enzymes and CHD risk. This could contribute to the increased CHD risk associated with the highest fifth of bilirubin concentration in PRIME, in which liver enzymes were not measured. Alternatively, if increased bilirubin reflects liver damage, the adverse effects would outweigh any beneficial effects of elevated bilirubin on CHD risk.
In PRIME, the relationship between serum bilirubin and smoking status just failed to reach statistical significance. Several studies have demonstrated that cigarette smoking decreases serum bilirubin concentrations [26, 27], and a number have suggested that smoking is associated with reduced bilirubin concentrations. Cigarette smoking increases oxidative stress [28] and therefore it was hypothesized [15] that the reduced bilirubin concentration in smokers may be due to oxidation of bilirubin by reactive species generated in cigarette smoke.
In this study bilirubin concentration was not associated with weekly alcohol intake, in keeping with many [16, 20, 25, 29, 30], though not all [31], previous studies. Thus, the relationship between alcohol intake and bilirubin concentration appears to be weak.
Conclusion
In the PRIME cohort, bilirubin concentration has a U-shaped association with CHD risk. This relationship has been observed in a previous prospective study [20] and was suggested as being due to reduced endogenous antioxidants when dietary intake is insufficient. We found no evidence that one such dietary antioxidant, α-tocopherol, was important in this respect. This study supports the hypothesis that bilirubin is a novel CHD risk factor in middle-aged men.
Footnotes
Acknowledgements
We thank the following organizations which allowed the recruitment of the PRIME subjects: the Health screening centers organized by the Social Security of Lille (Institut Pasteur), Strasbourg, Toulouse and Tourcoing; Occupational Medicine Services of Haute-Garonne, of the Urban Community of Strasbourg; the Association Inter-entreprises des Services Médicaux du Travail de Lille et environs; the Comité pour le Développement de la Médecine du Travail; the Mutuelle Géneérale des PTT du Bas-Rhin; the Laboratoire d'Analyses de l'Institut de Chimie Biologique de la Faculteé de Médecine de Strasbourg; the Department of Health (NI) and the Northern Ireland Chest Heart and Stroke Association.