
Abstract
Background
Efficient prevention policies need to be informed by knowledge of the cost-effectiveness of preventive treatments. This paper calculates the cost-effectiveness of aspirin, antihypertensive treatments and statins for prevention of cardiovascular disease.
Design
The investigation is a modelling study.
Methods
Ten-year cardiovascular risks and treatment eligibility were determined for each individual in a population of 5603 obtained from the Health Survey of England. Using published costs and evidence of effectiveness the cost-effectiveness of treating each eligible individual was determined over a 10-year time horizon. The marginal cost-effectiveness of additional antihypertensive drugs and increasing doses of statins were determined and a sensitivity analysis was carried out.
Results
Of the 5603 individuals 27.5% (95% confidence interval, 26.3–28.7%) were eligible for at least one treatment: the majority of these were eligible for all three. Cost per cardiovascular disease event prevented is strongly determined by pretreatment cardiovascular disease risk. In three-quarters of patients eligible for all three treatments, the lowest cost per event prevented was with aspirin and in the remainder with two-drug antihypertensive treatment. The marginal costs per event prevented were highest with the addition of a fourth antihypertensive drug and statins. These findings depend on the use of low-cost antihypertensives but are otherwise robust to a wide range of assumptions.
Conclusions
Modelling the cost-effectiveness of treatments to prevent cardiovascular disease is feasible and provides valuable information. Cost-effectiveness analysis argues for more widespread use of aspirin and two-drug antihypertensive treatment and against the use of four-drug antihypertensive treatment or statins.
Introduction
The Framingham risk equation remains the best predictor of cardiovascular risk and is used as the basis for determining treatment eligibility. UK hypertension guidelines recommend antihypertensive treatment for all those whose blood pressures (either systolic or diastolic) exceed 160/100 mmHg or those at over 20% 10-year Framingham cardiovascular disease (CVD) risk whose blood pressures exceed 140/90 mmHg. These guidelines also indicate that statins should be offered to all patients whose 10-year Framingham CVD risk exceeds 20% and aspirin once their blood pressure has been controlled [1]. This means that most patients who are eligible for one drug treatment are eligible for several treatments.
If prevention is to be informed by a consideration of cost-effectiveness it is important to understand which of the several preventive treatments for which each patient is eligible is the most cost effective, which the next most cost effective and so on. There are two reasons for this. Firstly efficient use of resources requires that the most cost-effective interventions are offered first, followed by less cost-effective interventions. If resources are constrained, patients will preferentially be offered only the most cost-effective interventions. Secondly, individual preference may dictate that patients refuse to accept more than a given number of treatments. It is therefore important to ensure that those they have been offered are those that are most cost-effective. Since there are many possible treatments to compare, it is inconceivable that this question can be answered by conducting clinical trials. It may, however, be answered by modelling cost-effectiveness using existing data on costs and effectiveness.
This paper estimates the cost-effectiveness of aspirin, antihypertensive treatments and statins for prevention of CVD. It does so using a model based on a large survey population, published costs and published estimates of effectiveness.
Methods
In this analysis the costs and effects of each treatment are considered over a 10-year horizon in a population of individuals. Costs and benefits are discounted at 3% per annum. Costs are considered from the perspective of the health services and benefits are measured as cardiovascular events prevented.
The model population
The study population was obtained from the Health Survey for England of 1998 [2]. The analysis was restricted to persons aged 35–74 years, who were not identified as having CVD but who had sufficient risk factor information to calculate their Framingham risks. In total 5608 persons fulfilled these criteria and this became the model population.
These data were entered into an Excel spreadsheet and 10-year cardiovascular risk, 10-year coronary risk and 10-year cerebrovascular risk were each calculated for every individual in the model population [3–5]. Coronary risk is the probability of myocardial infarction, new onset angina or sudden cardiac death; cerebrovascular risk is the probability of stroke or transient ischaemic attack; cardiovascular risk is the probability of experiencing any cardiovascular event.
Eligibility for treatment
Each patient's eligibility for treatment was determined from their 10-year cardiovascular risk and their risk factor status. Individuals aged over 50 years whose 10-year cardiovascular risk exceeds 20% are eligible for aspirin. Individuals whose 10-year cardiovascular risk exceeds 20% and diabetic patients are eligible for antihypertensives if either their diastolic or their systolic blood pressure exceeds 140/90 mmHg. All others are eligible if their diastolic or systolic blood pressure exceeds 140/90 mmHg. Individuals whose 10-year cardiovascular risk exceeds 20% and individuals whose total cholesterol or total to HDL cholesterol ratio exceeds 9.0 (a proxy for familial hypercholesterolaemia) are eligible for statins (Table 1).
Treatment eligibility criteria derived from the joint British recommendations
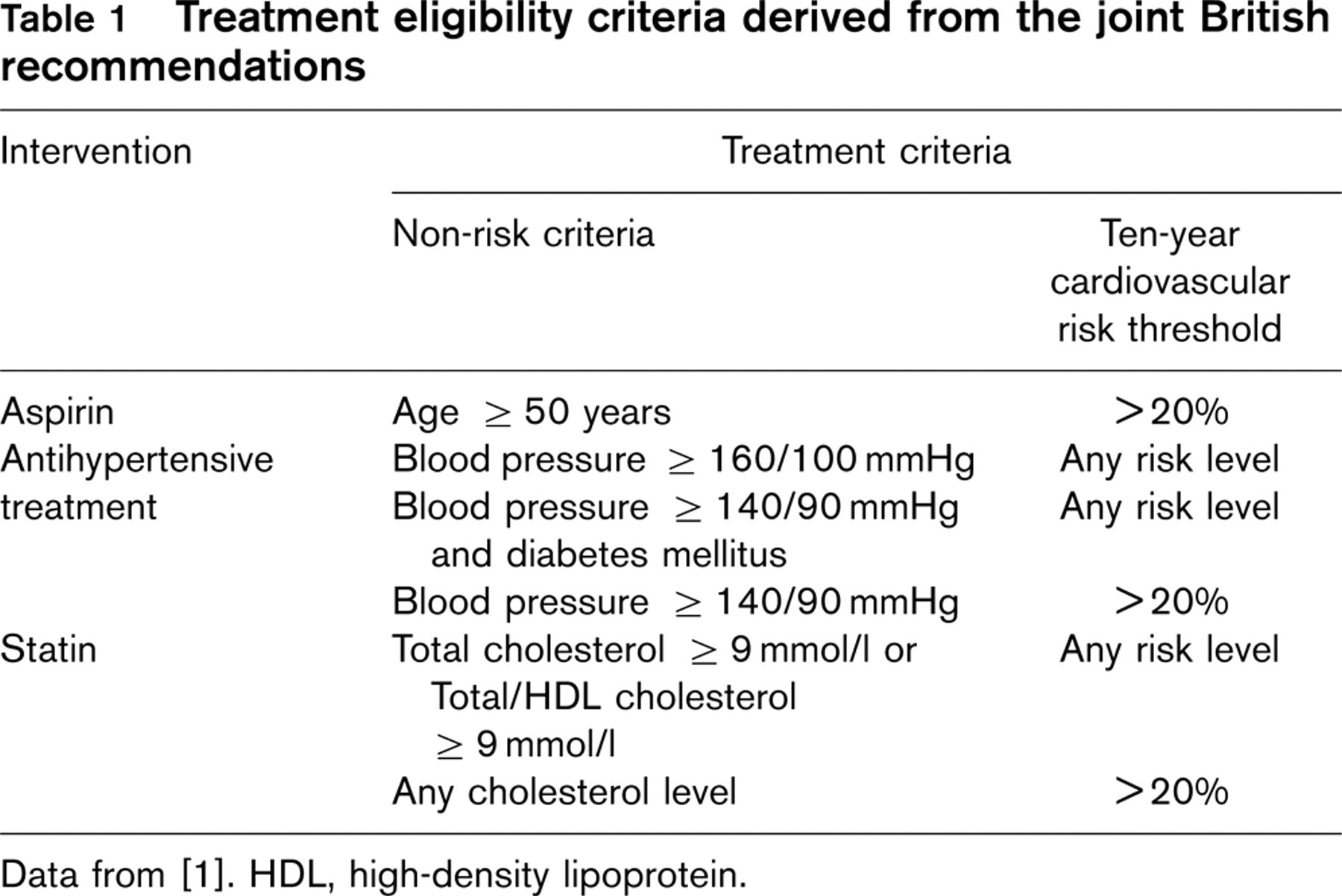
Data from [1]. HDL, high-density lipoprotein.
Patients eligible for antihypertensive treatment who have higher blood pressures require more drugs to achieve a target blood pressure than those with lower blood pressures. To account for this, hypertensives whose systolic or diastolic blood pressures are under 160/100 mmHg are considered to be eligible for two drugs. Those whose systolic or diastolic blood pressures exceed 160/100 mmHg but are under 170/105 mmHg are eligible for three drugs. Those with higher blood pressures are eligible for four drugs.
Effectiveness of treatment
For each treatment, effectiveness is the discounted sum of absolute reduction in coronary heart disease (CHD) risk and absolute reduction in cerebrovascular disease (CVA) risk in the treated patient. The total benefits with each treatment are calculated and entered into a separate column in the Excel spreadsheet. Reductions in CHD risk and CVA risk are determined by calculating the difference between pretreatment and post-treatment risk (pretreatment risk multiplied by relative risk on treatment).
The effectiveness of aspirin in primary prevention is derived from a recent meta-analysis: relative risk of CHD for patients on aspirin is 0.72 [95% confidence interval (CI), 0.60–0.87] and the relative risk of CVA is 1.02 (95% CI, 0.85–1.23) [6]. Aspirin also increases major bleeding events. The same meta-analysis concluded that aspirin increased absolute risk of major bleeding by 0.6% (95% CI, 0.4–0.8%) per 10 years of treatment [6]. For the purposes of this analysis a major bleeding event is considered as equivalent to one CVD event. The absolute reduction in risk with aspirin is therefore reduced by 0.6%.
A combination of up to four antihypertensive drugs was considered. These drugs are generally the lowest cost drugs in each of the four main antihypertensive drug classes for which a single daily dosage is possible [7]. The drugs used were bendroflumethazide 2.5 mg, metoprolol 100 mg, enalapril 10 mg and felodipine 5 mg. Evidence suggests that atenolol is less effective than other antihypertensives therefore metoprolol was chosen as the beta-blocker [8] The effect of antihypertensive treatment on systolic blood pressure was calculated using the results of meta-analysis [9]. For example bendroflumethazide 2.5 mg causes an 8.8 mmHg reduction in pretreatment systolic blood pressure of 154 mmHg is an 8.8 mmHg reduction. The reduction is 1.0 mmHg greater for every 10 mmHg higher pretreatment blood pressure. The effects of this reduction in blood pressure on cardiovascular and cerebrovascular risk are calculated as follows. Relative risk of CHD is 0.83 and relative risk of CVA is 0.64 for each 12 mmHg reduction in blood pressure [10]. This is consistent with the epidemiological evidence [11, 12]. The relative risk of CHD following a 24 mmHg reduction in systolic blood pressure is therefore 0.83(24/12) (0.832 = 0.67) (Table 2). The effects of two, three and four antihypertensive drugs can be calculated from their effect on systolic blood pressure (Fig. 1).
Simvastatin and atorvastatin were considered in this analysis, each at doses of 10, 20, 40 and 80 mg. A recent meta-analysis derived equations to estimate the effects of statins on serum low-density lipoprotien (LDL) and derived further equations to estimate the relationship between reduction in serum LDL and relative risk of CHD and CVD [13]. Since patients’ LDL level data were not available, the authors of the meta-analysis were asked to respecify the equations for total cholesterol levels (personal communication, Alicja Rudnicka, 30 November 2004). The equations to estimate reduction in total cholesterol are shown in Table 3 (Fig. 2). Statins were assumed to have one-third of their full effect in year one of treatment, two-thirds in year two and to be fully effective in year three and subsequent years [13].
Costs
Costs are calculated as follows. It is assumed that each treated patient must have full CVD risk assessment before starting any treatment. This requires two lipid profiles (£5.67 each, source, Reinhold Grün, LSHTM 1996 and adjusted for inflation) and - to measure blood pressure at two separate visits, elicit other risk factors, determine treatment eligibility and discuss results - one hour of practice nurse time (£32 per hour) [14]. All follow-up appointments are assumed to be with a practice nurse and to take 15 min each. Patients on aspirin are followed up twice a year and have no laboratory tests; patients on antihypertensives are followed up four times a year and have annual urea and electrolytes (£4.72 each, source as above); patients on statins are followed up four times a year and have annual lipid profiles and liver function tests (£5.67 and £4.22, respectively, source as above). Drug costs are obtained from the British National Formulary [7]. Dispensing costs are calculated at £0.874 per prescribed item on the assumption that four prescriptions are issued per year [15]. In this way total costs are calculated for each treatment and entered into a separate column in the Excel spreadsheet (Fig. 3).
Expected reductions in systolic blood pressure with antihypertensive treatment
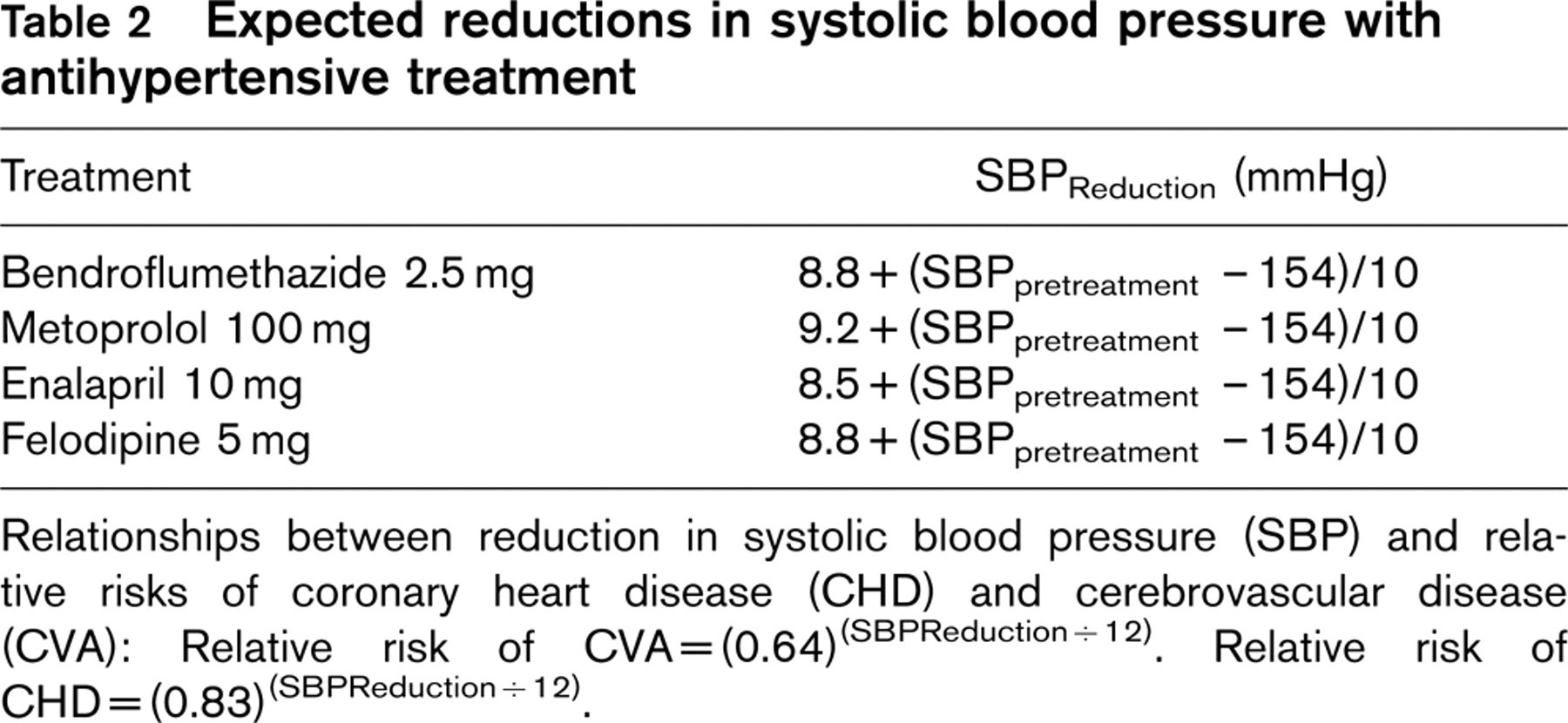
Relationships between reduction in systolic blood pressure (SBP) and relative risks of coronary heart disease (CHD) and cerebrovascular disease (CVA): Relative risk of CVA = (0.64)(SBPReduction / 12). Relative risk of CHD = (0.83)(SBPReduction / 12).
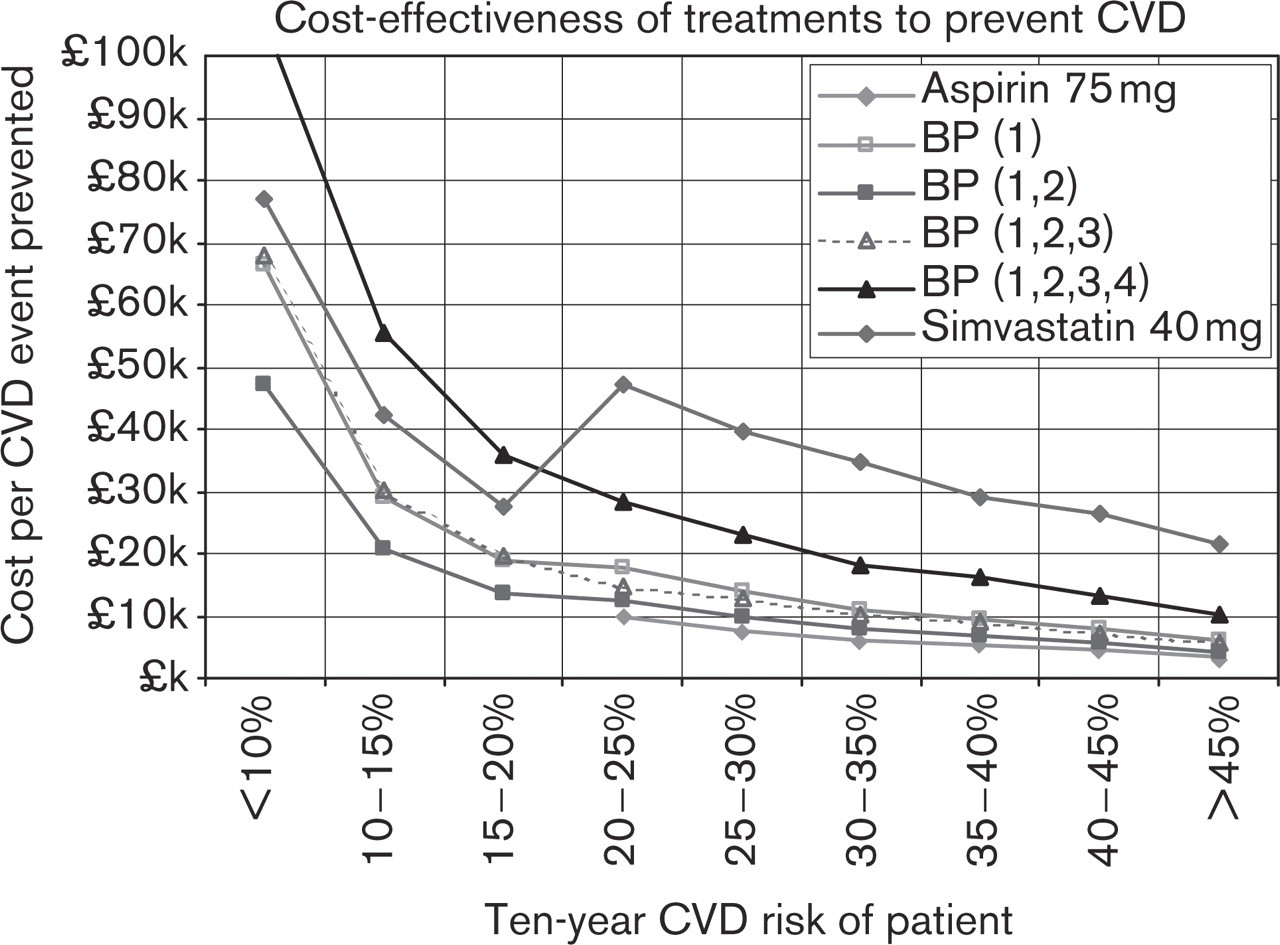
Average cost per cardiovascular event prevented with preventive treatments: patients stratified by cardiovascular disease (CVD) risk. Only one statin (simvastatin 40 mg) has been included on the graph to avoid overcrowding.
Expected reductions in total cholesterol with simvastatin and atorvastatin
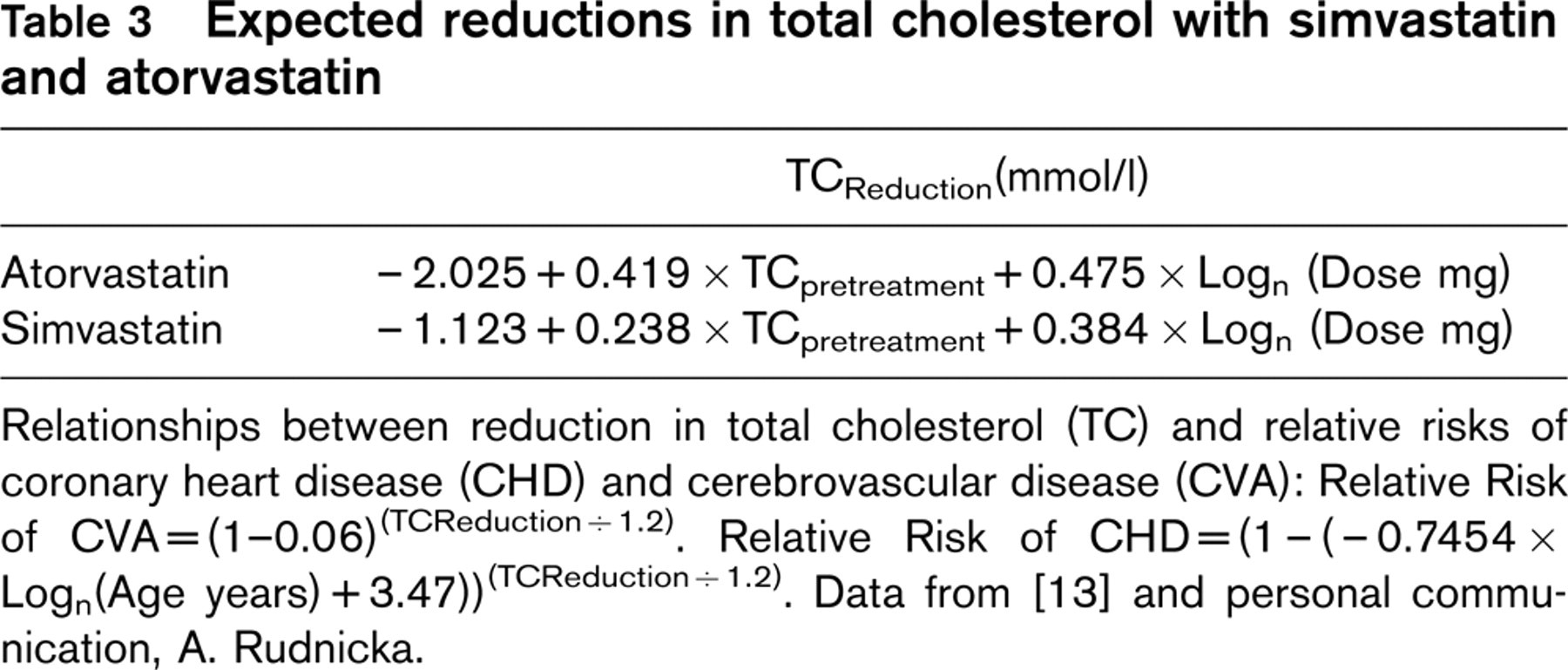
Relationships between reduction in total cholesterol (TC) and relative risks of coronary heart disease (CHD) and cerebrovascular disease (CVA): Relative Risk of CVA = (1-0.06)(TCReduction / 1.2). Relative Risk of CHD = (1 - (−0.7454 × Logn(Age years) + 3.47))(TCReduction / 1.2). Data from [13] and personal communication, A. Rudnicka.
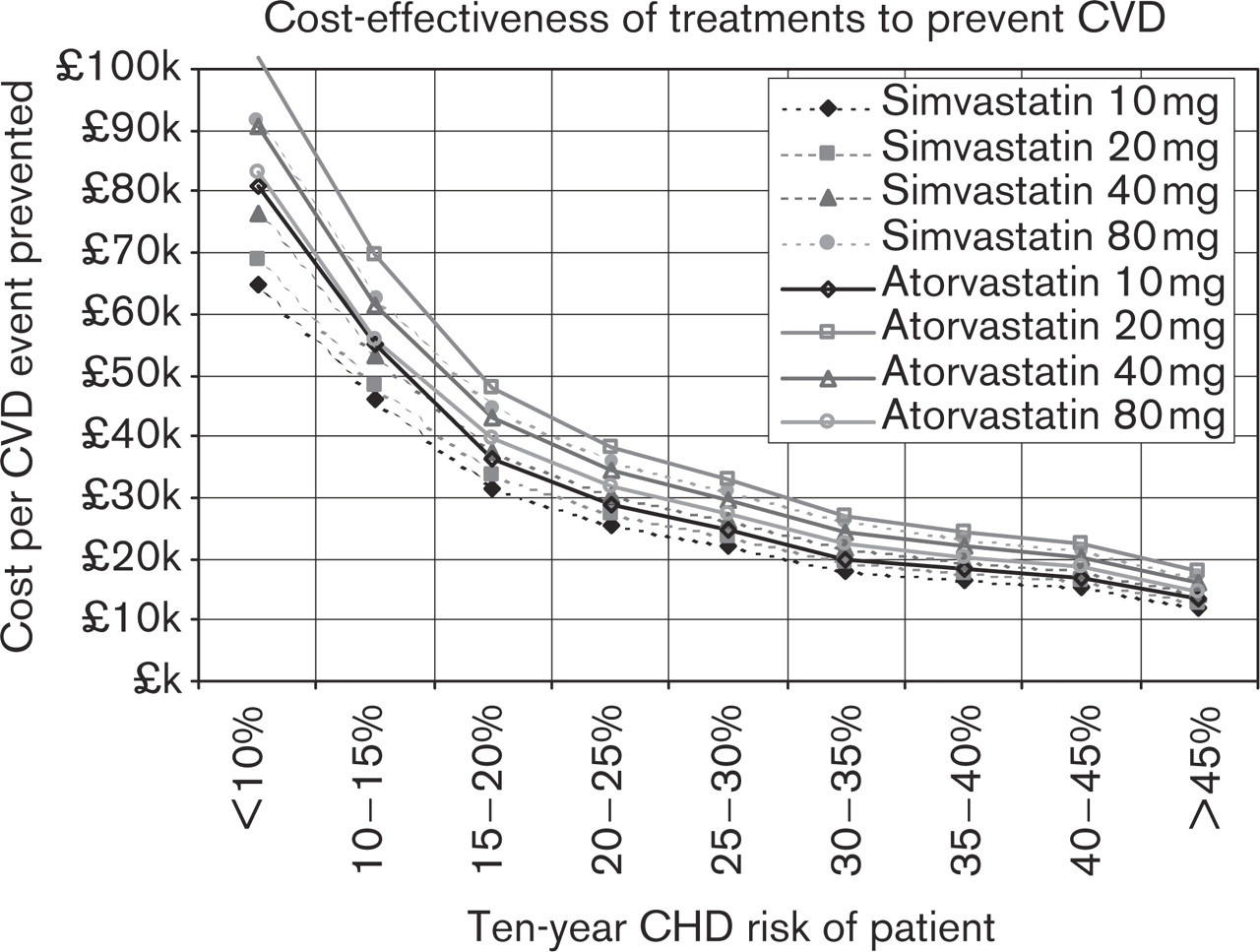
Average cost per cardiovascular event prevented by statins: patients stratified by coronary heart disease (CHD) risk. CVD, cardiovascular disease.
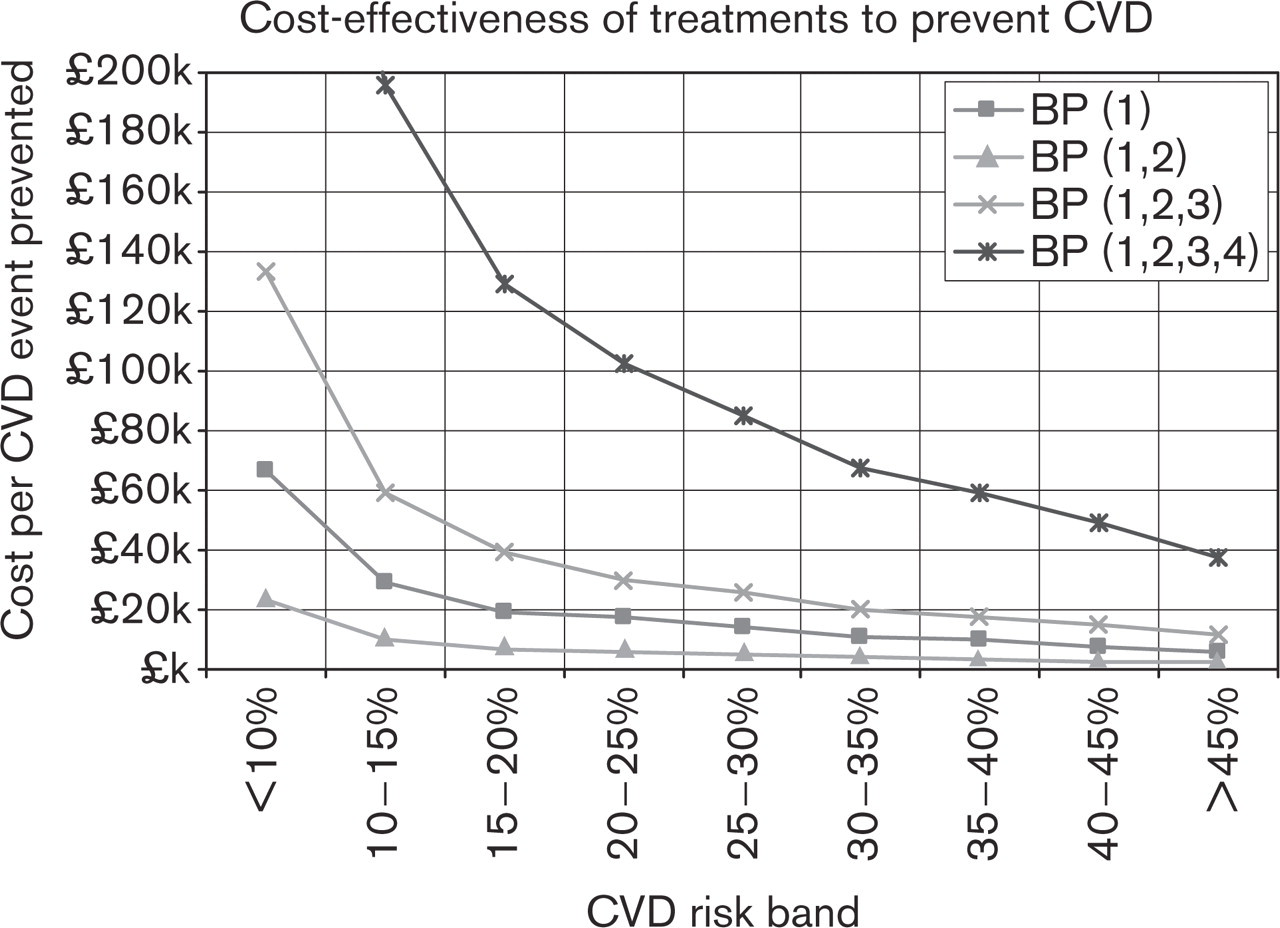
Marginal cost per cardiovascular event prevented with one, two, three and four-drug antihypertensive treatment: patients stratified by cardiovascular risk. CVD, cardiovascular disease.
Cost-effectiveness
For each patient receiving each treatment cost per CVD event prevented is calculated by dividing the discounted cost of the treatment by the discounted reduction in absolute risk of CVD with the treatment. This means that the Excel spreadsheet contains a column of data for each treatment showing the cost per CVD event prevented for each patient receiving that treatment. Summary results are presented for each treatment. These are the sum of the cost of treatments across a number of patients divided by the sum of the benefits of treatment across a number of patients: the average cost per CVD event prevented. Because average cost-per CVD event is dependent on CVD risk these results are stratified by pretreatment risk and presented graphically.
In individuals eligible for all three types of treatment the cost per event prevented with each treatment is compared to determine whether the most cost-effective treatment on average is also the most cost-effective in every individual.
Marginal cost-effectiveness
For antihypertensive treatments and statins the key question is whether additional benefits from using more drugs or higher doses are sufficient to justify additional costs. For these treatments, the marginal cost per CVD event prevented is calculated for each patient. This is the additional cost of adding each further treatment (or the additional cost of increasing the dose of a statin) divided by the additional reduction in absolute risk of CVD.
Sensitivity analysis
A sensitivity analysis explored the effects of changing the discount rates and costs. It also investigated the effects of using US eligibility criteria for aspirin and New Zealand guidelines for use of antihypertensives. US guidance recommends that aspirin be offered at a 5-year coronary risk of 3% equivalent to a 10-year cardiovascular risk of 10% [6, 16]. New Zealand guidelines recommend anti-hypertensives in high-risk patients whose blood pressures exceed 115/75 mmHg [17].
Results
Of 5603 patients aged 35–74 years and without cardiovascular disease, 1540 (27.5%; 95% CI, 26.3–28.7%) were eligible for at least one treatment: 1259 (22.5%; 95% CI, 21.4–23.6%) were eligible for aspirin, 1161 (20.7%) were eligible for antihypertensive treatment and 1356 (24.2%; 95% CI, 23.1–25.3%) were eligible for a statin. Of the 1540 eligible for at least one treatment, 356 (23.1%; 95% CI, 21.0–25.2%) were eligible for two treatments and 940 (61.0%; 95% CI, 58.6–63.5%) were eligible for all three.
Of the 1161 eligible for antihypertensive treatment, 623 (53.7%; 95% CI, 50.8–56.5%) were eligible for three drugs and 312 (26.9%; 95% CI, 24.3–29.4%) were eligible for four.
Cost-effectiveness and risk
Cost per cardiovascular event prevented is strongly determined by cardiovascular risk. For any treatment it is over £45 000 in an individual at less than 10% 10-year cardiovascular risk and under £30 000 for any treatment in a patient at over 45% 10-year cardiovascular risk. On average the cost per event prevented at any risk level is lowest with aspirin, followed by antihypertensive treatment with two drugs. One and three drug antihypertensive treatments are of similar cost-effectiveness, statins and four-drug antihypertensive treatment are the least cost-effective interventions.
The cost per cardiovascular event prevented with a statin is lower in individuals at just under the cardiovascular risk threshold for treatment than those just above it. Statins mainly prevent coronary events. Individuals with very high cholesterol levels who are just below the cardiovascular risk threshold are at higher coronary risk than individuals just above the cardiovascular risk threshold. Coronary risk is a better predictor of cost per cardiovascular event prevented with a statin.
Cost-effectiveness
Of the 940 persons eligible for all three types of treatment, cost per event prevented was lowest with aspirin in 75.2% (95% CI, 72.5–78.0%). The next lowest cost per event prevented is invariably with two-drug antihypertensive treatment. Cost per event prevented was lowest with two-drug antihypertensive treatment in 24.8% (95% CI, 22.0–27.5%), usually followed by aspirin. In 6.2% (95% CI, 4.6–7.7%) of patients aspirin was less cost-effective than three-drug or four-drug antihypertensive treatment. These individuals were characterized by high cerebrovascular risks in relation to their coronary risks. Cost per event prevented with aspirin, two-drug, one-drug and three-drug antihypertensive treatment was always lower than with a statin.
In 1262 (93.1%; 95% CI, 91.7–94.4%) patients eligible for statins, simvastatin 10 mg was the most cost-effective intervention. In the remainder of cases higher doses of simvastatin were the most cost-effective interventions.
Marginal cost-effectiveness
With antihypertensive treatments the marginal cost per event prevented falls when a second drug is added and then rises exponentially with each additional treatment. This is because the marginal cost of a second drug is low - follow-up costs have already been incurred - whereas the benefits are similar in magnitude to the first drug. Subsequent drugs offer diminishing returns at increasing costs. The marginal cost per event prevented with the fourth drug is usually very high.
With statin treatments the marginal cost per event prevented rises when simvastatin 10 mg is increased to 20 mg or substituted by atorvastatin 10 mg. Cost per event prevented rises with each subsequent increase in simvastatin dose. Since atorvastatin 20 mg costs the same as 40 or 80 mg, however, the marginal cost per event prevented at higher doses is zero.
Sensitivity analysis
The effects of changing the eligibility criteria were explored as follows. Eligibility criteria were changed to 10% 10-year cardiovascular risk alone for aspirin and 10% 10-year cardiovascular risk along with a blood pressure of 115/75 mmHg for two-drug antihypertensive treatment.
The cost per event prevented with either intervention in patients at 10–15% risk was lower than the marginal cost per event prevented with the addition of a fourth antihypertensive drug in any patient.
Because most costs and benefits accrue at the same time, the findings are not sensitive to the discount rate. Changes in the cost of follow-up also make little difference because they affect all treatments equally. The findings are sensitive, however, to the cost of treatments. For example cost per event prevented is four times higher with losartan than with low-cost antihypertensives: higher than with a statin. Similarly, if the price of simvastatin 10 mg falls by 75% it is of similar cost-effectiveness to aspirin and two-drug antihypertensive treatment.
Discussion
The principal strength of this analysis is that it is explicit about the method of calculating costs and benefits. It uses the best estimates of the effectiveness of treatment and the combinations of risk factors found in real patients from a population survey. Any analysis is as good as its underlying assumptions. The analysis can also be adapted to any set of assumptions about costs, effects of treatment on risk factors or benefits of treatment. The analysis does not estimate the number of quality-adjusted life years (QALY) gained with treatment, but it is unlikely that events prevented by aspirin or two-drug antihypertensive treatment result in different QALY gains than those prevented with statins or four-drug antihypertensive treatment.
For simplicity it has been assumed that all patients accept and comply with treatment. This means that cost per event prevented in clinical practice may differ from the figures calculated here. Assuming full compliance does not greatly affect comparisons between treatments unless we have reason to believe that compliance is likely to be much better with statins or multidrug antihypertensive treatment than with aspirin one-drug or two-drug antihypertensive treatment. Evidence suggests that compliance with aspirin (83% at 3.6 years) [18] and antihypertensive treatment (78% reported at 1 year in Canada and over 80% in the USA) [19] may be higher than with statins (25% at 2 years in Canada and 39% at 1 year in the USA) [20, 21].
This analysis has a number of striking implications. Firstly, if it is worth treating a patient with one low-cost antihypertensive it is even more cost-effective to give them two. Secondly, since statins (and aspirin) in primary prevention have more effect on coronary disease than stroke, eligibility criteria should be based on coronary risk for these interventions. Thirdly cost-effectiveness can be used to inform eligibility criteria. Since costs per event prevented are low with aspirin and two-drug antihypertensive treatment it is worth extending their use to lower risk patients.
The corollary of this is that some treatments are not cost-effective. If we use a cut-off of (for example) £40 000 per event prevented the addition of a fourth antihypertensive is rarely justified. It is therefore not often worthwhile attempting to achieve a target blood pressure. Similarly increasing the dose of a simvastatin 10 mg to achieve a target cholesterol level is rarely cost-effective. In both cases the desire to optimize a single risk factor runs contrary to cost-effective use of resources.
Modelling cost-effectiveness of treatments to prevent cardiovascular disease is feasible and provides valuable information. Cost-effectiveness analysis supports more widespread use of aspirin and two-drug antihypertensive treatment with low-cost drugs. It places the burden of proof on new antihypertensives to demonstrate additional benefits to justify their high cost. Analysis also supports ‘fire and forget’ over ‘treat to target’ strategies for both statins and antihypertensives.