
Abstract
Background
Objective
Design
Results
Conclusion
Introduction
Worldwide, children are now more overweight than ever before [1, 2]. Concomitantly, there have been increases in cardiovascular, endocrine, and psychiatric diseases, with studies showing more than a twofold increase in cardiovascular-related mortality in adults who were over-weight as children [2, 3]. Although many factors contribute to obesity, decreased physical activity and increased sedentary activity are important modifiable factors [4, 5].
Although the role of physical activity for overweight children has been studied, its relevance for children with familial hyperlipidemia (FH) is not known. Patients with FH have a 100-fold increase in mortality from coronary artery disease at ages 20-39 years [6], with 50% of men and 30% of women suffering a myocardial infarction by 50 and 60 years of age, respectively [7, 8]. One study [9] showed that the presence of coronary artery disease was more significantly correlated with a higher body mass index (BMI) than the severity of lipid abnormalities in patients with FH. Therefore, preventing obesity by increasing physical activity and decreasing sedentary activities may be particularly important in children with FH.
In this study, we sought to determine the associations between physical activity, adiposity, and fasting lipid profile values in children with FH in two specialized lipid disorder clinics. We hypothesized that decreased physical activity and increased sedentary activity would be associated with greater adiposity and abnormal lipid profiles.
Methods
Study participants
In specialized paediatric lipid disorder clinics at the Hospital for Sick Children, Toronto, Ontario, Canada, and at St Joseph's Hospital, Hamilton, Ontario, Canada, 147 consecutive children were recruited over a 9-month period. As these hospitals were referral centres for the province, patients came from heterogeneous socioeconomic backgrounds. Eligible patients gave written consent or assent as appropriate at the time of their routine visit. All patients had a family history of hyperlipidemia or premature atherosclerotic cardiovascular disease in first or second-degree relatives. Genetic confirmation of the clinical diagnosis of a primary FH, such as familial hypercholesterolemia or familial combined hyperlipidemia, by molecular analysis was unavailable. Patients with secondary causes of hyperlipidemia, such as diabetes and other endocrinopathies, and renal or hepatic abnormalities, were excluded. This study was approved by the Research Ethics Board at both institutions.
Measurements
All measurements were standardized between the centres and made concomitantly at a routine clinic visit. A self-administered questionnaire was used to assess self-reported time spent in various activities descriptively. The questionnaire was created on the basis of questionnaire development guidelines [10, 11], and a review of relevant literature and previous questionnaires on physical activity [12–14]. The questions were chosen to assess self-reported physical activity levels, associated factors, and attitudes regarding physical activities. The questions were worded in an age-appropriate manner. In particular, patients were asked to compare their activity level to their friends and siblings, and estimate the number of hours per week in various activities including gym classes, sports teams, recreational activities, television viewing, computer use, video-game play, and time spent by other family members in physical activity. They were also questioned regarding symptoms during exercise and the availability and use of exercise equipment at home. All patients were urged to complete the questionnaire on their own. However, parents were allowed to provide assistance.
Height was measured to the nearest 0.1 cm with a stadiometer, and weight was measured to the nearest 0.1 kg using a calibrated electronic scale. These anthropometric measurements were performed with patients barefoot and wearing light indoor clothing. BMI was calculated from height and weight measurements and standardized as z scores according to published age and sex standardized normal data [9]. Venous blood was collected from patients after an overnight fast of at least 12 h. Total cholesterol, high-density lipoprotein (HDL)-cholesterol, and triglyceride levels were measured and low-density lipoprotein (LDL)-cholesterol was calculated using the Friedewald equation [15]. All assays were performed in a single institutional laboratory at each of the two study centres meeting current standards and following provincial quality control measures.
Data analysis
Data are described as frequencies, medians with ranges, and means with standard deviations as deemed appropriate. Standardized BMI z scores were tested against a hypothesis of a mean of 0 (normal) with a single sample t-test. Patient-perceived satisfaction with activity level was related to patient characteristics and reported time spent in various activities, using Fisher's exact test, Kruskal-Wallis analysis of variance, and t-tests. Relationships between lipid profile values, time spent in activities, and patient characteristics were correlated using simple linear regression. All analyses were performed with SAS version 6.12 statistical software (SAS Institute, Inc., Cary, North Carolina, USA) using default settings. A P < 0.05 was set as the level of statistical significance.
Results
Patient characteristics
The characteristics of the patients are summarized in Table 1. The patient population was 50% male, with a mean age of 12.5 ± 3.2 years (range 5-18). The mean BMI z score of + 0.90 ± 1.30 SD was significantly greater than normal (P < 0.001), with 21% of patients having z scores greater than 2.
Patient characteristicsa
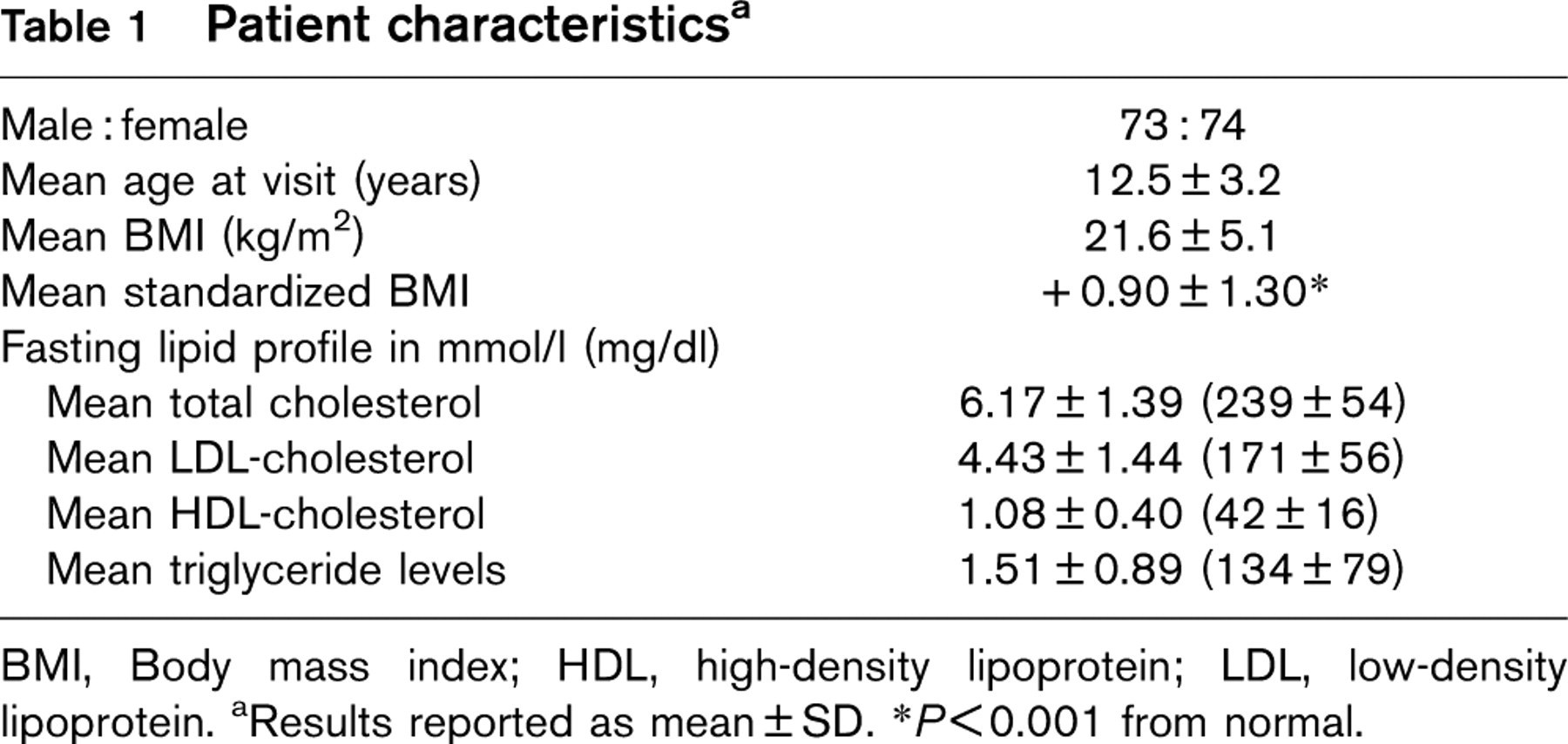
BMI, Body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein. aResults reported as mean ± SD. ∗P < 0.001 from normal.
Perceived activity levels
With respect to perceived activity, 68% of patients felt that they were as ‘active as they should be'. In relation to their peers and siblings, 92 and 72%, respectively, reported that they were either more active or had the same activity level. The majority, 67%, of the patients reported that they were ‘happy with their current weight'.
Participation in physical activity
The median amount of time spent in physical activity and sedentary pursuits per week, and the amount of time spent by their family members in physical activity, is shown in Fig. 1. Regarding structured activities, 86% participated in gym at school and 57% were members of a sports team. In this study, patients spent twice the amount of time in sedentary pursuits than in physical activities per week, with television viewing being the most common sedentary pursuit. No limitations with physical activity were reported by 86% of patients. No difficulties during or after exercise were reported by 60%, with 24% reporting shortness of breath, 7% pain, and 4% fatigue. Exercise equipment was present in the home for 76%, although only 60% actually used the available equipment.
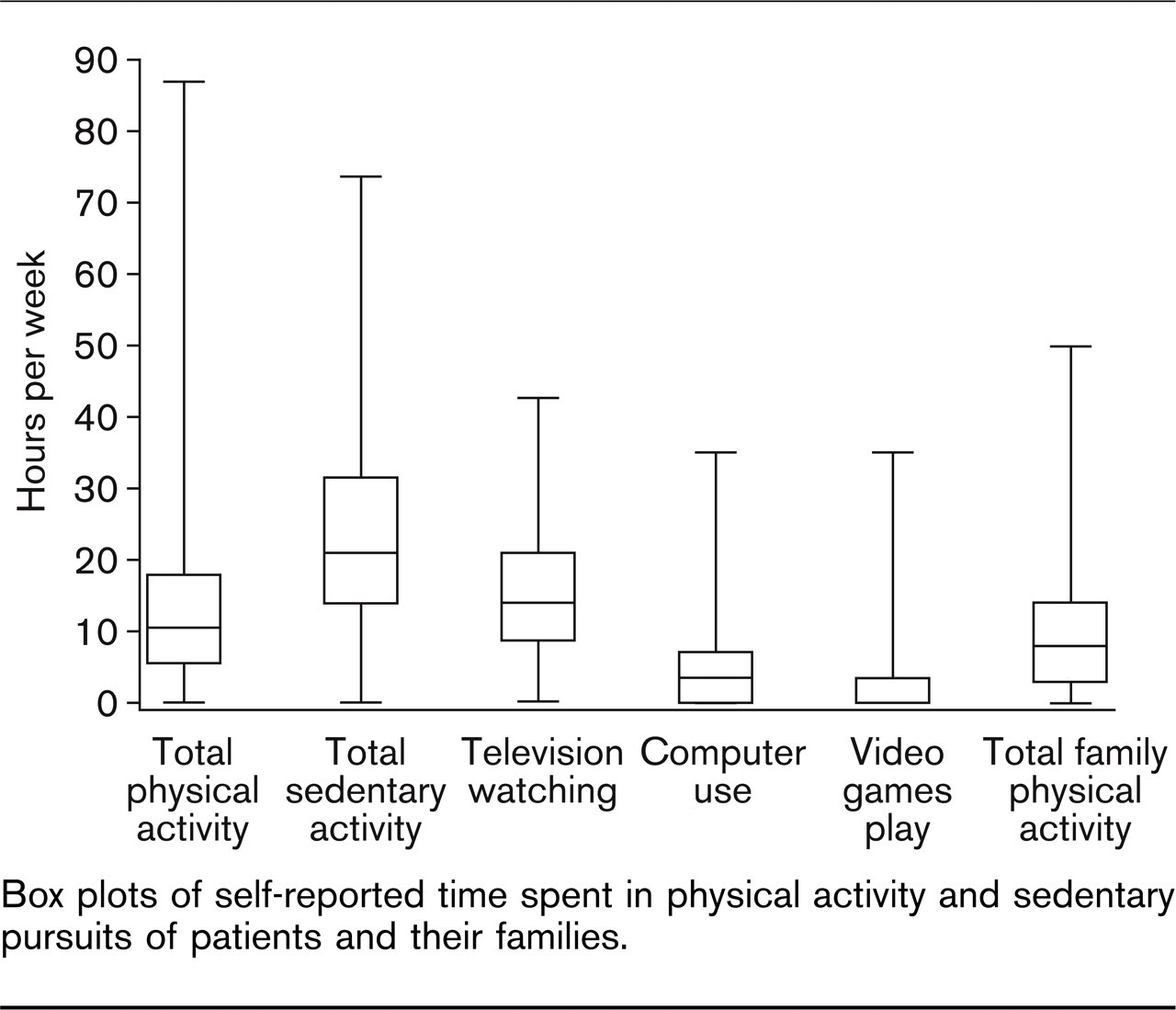
Box plots of self-reported time spent in physical activity and sedentary pursuits of patients and their families.
Attitudes towards physical activity
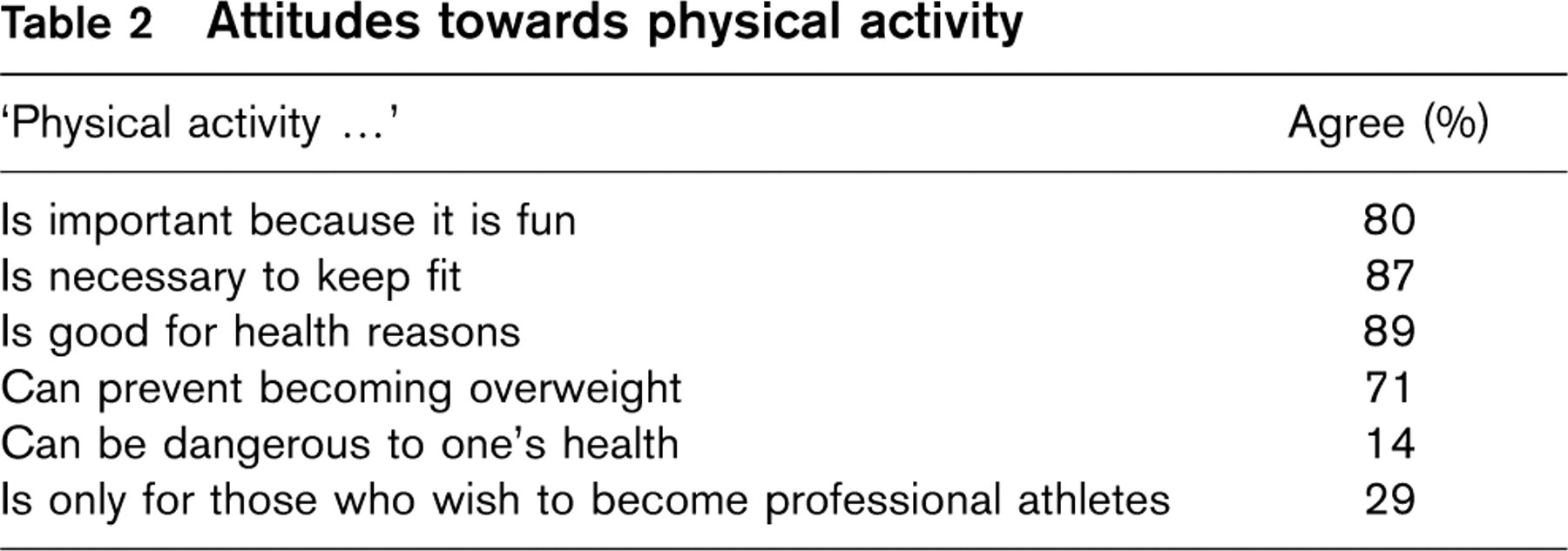
Attitudes regarding physical activity
Patients were presented with six statements about physical activity and asked whether they agreed (Table 2). The majority had positive attitudes towards physical activity, with appropriate perceived benefits. However, 14% did not agree that physical activity was necessary to keep fit, 9% did not agree that it was good for health, and 14% agreed that physical activity can actually be harmful to one's health. Children who believed that they were not as active as they should be were found to be older (P = 0.004) with higher BMI z scores (P =0.01) and higher triglyceride levels (P = 0.007). These children also reported spending fewer hours per week on physical activities (P = 0.009), and more time on sedentary pursuits (P = 0.007).
Sex differences
The mean BMI z score was significantly greater for boys (1.27 ± 1.37) than girls (0.52 ± 1.11; P < 0.001). A comparison of boys and girls regarding time spent in physical activity and sedentary pursuits is shown in Fig. 2. Although the reported levels of physical activity were similar (P = 0.85), boys spent more time in sedentary pursuits (P = 0.004), which included watching television (P = 0.04) and using the computer (P = 0.03). There was no significant difference in the activity levels of family members (P = 0.37) when comparing boys and girls.
Factors associated with adiposity
Higher BMI z scores correlated with lower LDL-cholesterol (r = −0.21, P = 0.02) and higher triglyceride levels (r = +0.33, P < 0.001), but not with total or HDL-cholesterol. Higher BMI z scores did not correlate with total reported time spent in physical activity; however, they did correlate with a greater reported time spent in sedentary pursuits (r= + 0.24, P = 0.004), particularly TV watching (r = +0.26, P = 0.003). Furthermore, less reported time spent by other family members in physical activity correlated with increased BMI z scores for the patient (r = −0.21, P = 0.01).
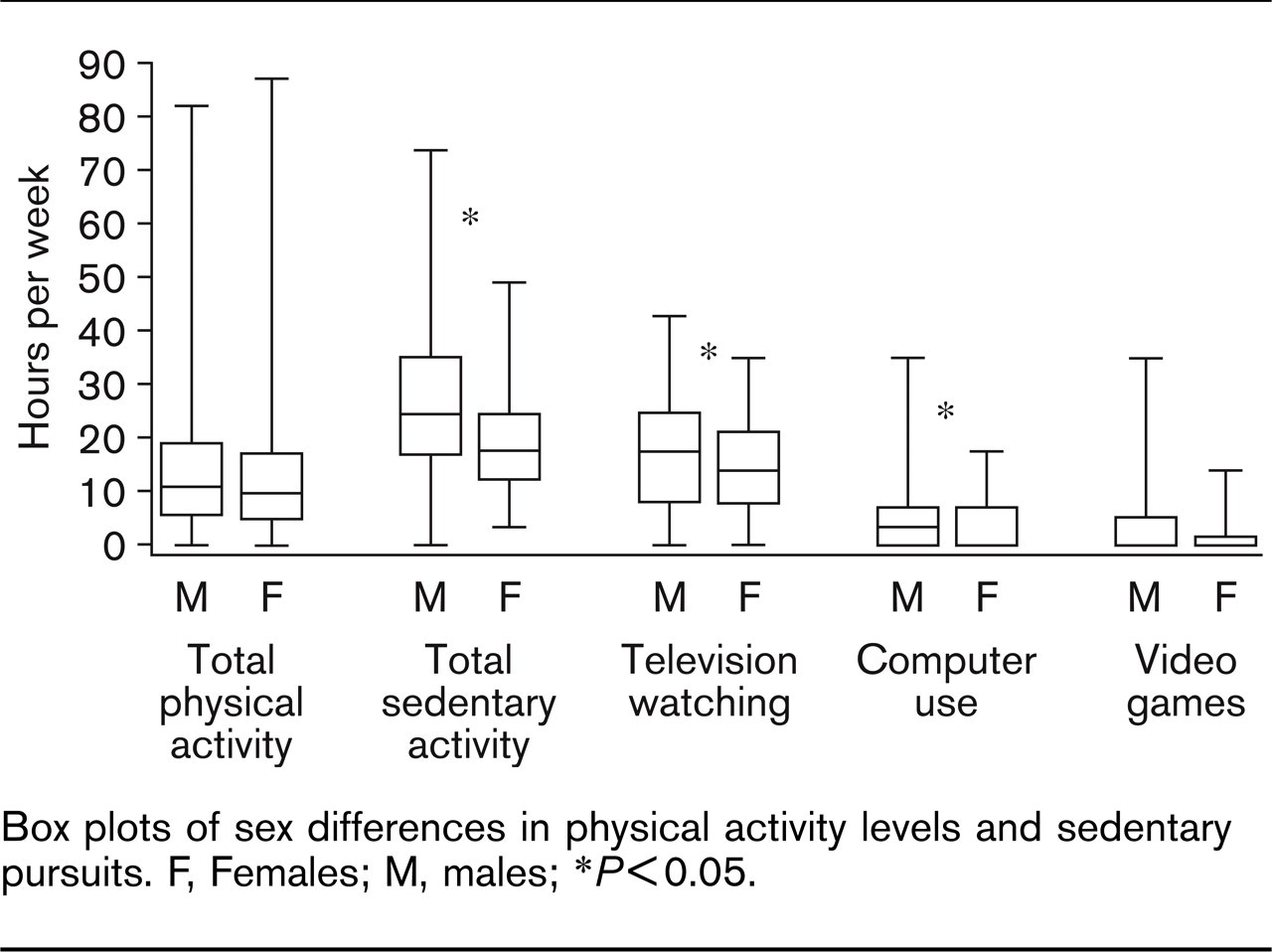
Box plots of sex differences in physical activity levels and sedentary pursuits. F, Females; M, males; ∗P < 0.05.
Factors associated with physical activity
Increased reported time spent in physical activity significantly correlated with age (r = + 0.20, P = 0.02) and time spent by other family members in physical activity (r = + 0.24, P = 0.003). There was no significant correlation between physical activity and lipid profile values, BMI or time spent in sedentary pursuits.
Factors associated with lipid profile values
Higher triglyceride levels correlated with higher BMI z scores (r = + 0.33, P < 0.001), greater reported time spent in sedentary pursuits (r = + 0.26, P = 0.002), greater reported time spent watching television (r = + 0.26, P = 0.002), and fewer hours spent by other family members in physical activity (r = −0.18, P = 0.04). Lower LDL-cholesterol levels were significantly associated with higher BMI z score (r = −0.21, P = 0.02). HDL and total cholesterol levels were not significantly associated with adiposity or activity variables.
Discussion
In our patients with FH, despite regular dietary and exercise counseling, cardiovascular risk education, and close follow-up in specialized paediatric lipid disorder clinics, patients had on average significantly greater weight for height measures than the normal population, with 21% of patients having BMI z scores 2 SD above normal. This is significantly greater than that reported in the Canadian Fitness Survey [1], in which 11.8% of girls and 13.5% of boys between the ages of 7 and 13 years were classified as obese. The increased adiposity exacerbates lipid abnormalities and would probably contribute additional metabolic risk to a situation that is already high risk.
Our study showed a correlation between a higher BMI z score and increased triglyceride levels. This is consistent with previous studies [16, 17] in children without FH in which obesity has been associated with elevated triglyceride levels. The association between BMI and LDL-cholesterol levels is less clear [18, 19]. Our finding that increased BMI is associated with decreased LDL-cholesterol is in agreement with a study by Nakamura and colleagues [20]. Interestingly, in our study, total cholesterol and HDL-cholesterol levels were not associated with BMI. This is in contrast to the positive correlation with total cholesterol levels and a negative correlation with HDL-cholesterol levels reported previously [16, 21] in children without FH. This discrepancy may be explained by the fact that our patients had FH and were on a low fat and cholesterol-restricted diet. Furthermore, the differences in the impact of obesity on lipid abnormalities associated with specific hyperlipidemias have not been well studied. It is possible that our observation of a relationship of increased BMI and decreased LDL-cholesterol may be spurious. In general, lipid abnormalities associated with obesity and the metabolic syndrome include higher triglyceride levels and lower HDL-cholesterol levels, with no real change in LDL-cholesterol levels, but instead, a shift towards smaller and denser LDL-cholesterol particles. We did not measure the LDL-cholesterol particle size in our study.
Regarding physical activity, the majority of our patients had positive attitudes towards physical activity, understood its benefits, and felt that they were at least as active as their peers and siblings. However, we found that these children were spending twice as much time in sedentary pursuits, particularly television viewing, compared with physical activities. When boys and girls were compared, boys were more overweight, and reported spending more time in sedentary pursuits than girls. These findings are consistent with a recent Canadian physical activity survey [22].
With regards to self-reported activity levels, patients who reported that they were less active than they thought they should be had higher BMI z scores, increased triglyceride levels, and reported spending less time in physical activities and more time in sedentary pursuits. We also noted that increased BMI z scores were significantly associated with greater reported time spent in sedentary pursuits, but not with less time spent in physical activity. This apparent discrepancy may be due to several reasons. First, although a self-report measure of physical activity has moderate correlation with objective measures, patients generally overestimate the time spent in physical activity [23]. Second, higher amounts of physical activity than reported in our study may be required in children to have any impact on BMI, as a low or moderate amount of activity may be easily compensated by increasing energy intake. Third, this finding may suggest a ‘reverse causation’ in which obese children are less likely to be physically active than non-obese children as has been suggested previously [24]. On the contrary, knowing that this population is much more overweight than the reported normative data, our finding may suggest that the amount of time spent in sedentary pursuits may be a more important determinant of BMI than physical activity. This theory is supported by a recent study [25], which illustrated that the determinants of activity and inactivity are different. Furthermore, a recent randomized controlled trial [26] showed that decreasing sedentary pursuits, especially television watching, was better than promoting active behaviours in reducing BMI over a 1-year period.
Interestingly, we did not find an association between physical activity levels and lipid profiles either. This lack of association may be due to the first two reasons
described above for the lack of correlation between physical activity and BMI. Furthermore, the association may also be confounded by potential differences in the types of FH and the degree of compliance with dietary therapy in our patients. As our study was cross-sectional we were unable to control for these confounders.
Another important predictor of physical activity levels and BMI in children was the reported time spent by other family members in physical activity. This is consistent with previous studies [27, 28], which have shown that the parents’ level of physical activity and their BMI positively correlated with that of their children. Moore and colleagues [28] reported that children were two times more likely to be active if their mother was active, 3.5 times if their father was active, and 5.8 times if both parents were active when compared with the children of inactive parents. This emphasizes the fact that parents not only provide a genetic predisposition for physical activity and fitness, but are also critical in acting as role models and providing encouragement and access to fitness [29, 30].
The results of our study must be viewed in the light of its limitations. The use of BMI as a measure of adiposity may be imperfect, although it is currently used clinically and in the majority of studies to define the terms ‘overweight’ and ‘obesity'. The use of z scores of BMI rather than percentiles allows the identification of dose-response relationships with other factors while accounting for age and sex differences. Our activity questionnaire was not formally assessed for its validity or reliability. However, the cross-sectional associations observed are plausible, interesting and relevant. The questionnaire was designed to assess both attitudes and practices regarding activity and was not designed for longitudinal assessment. There is also a possibility that some children may not have understood the questions in the questionnaire. However, in developing the questionnaire we ensured that the questions were worded in an age-appropriate manner. Furthermore, parents were allowed to help their children complete the questionnaire.
Treatment goals for children with FH currently include dietary and pharmacological interventions aimed at improving dyslipidemia and the prevention and treatment of additional cardiovascular risk factors. Regarding the latter, it is important to address lifestyle modifications such as decreasing sedentary activities and increasing physical activity. Physical activity has several benefits in children that are particularly important in those at high risk of coronary artery disease, such as children with FH and obesity. For example, in overweight children, physical activity contributes to increased cardiovascular fitness, better lipid profiles, and improved fasting insulin levels [31, 32]. Furthermore, physical activity has a direct beneficial impact on the vasculature through decreased vascular tone and improved endothelial function [33]. Promoting physical activity in these children therefore sets the stage for preventing cardiovascular disease as an adult.
Current guidelines from Health Canada [34, 35], for example, state that children and youth should decrease their total time spent in sedentary pursuits by 90 min per day and increase their time spent in physical activity to 90 min per day. However, to be optimally effective, family members must also be encouraged to play an active role in promoting physical activity. The physical activity prescription should therefore be directed towards both children and their family members in order to achieve maximal success.