
Abstract
Background
Femoral artery intima–media thickness (IMT), an independent predictor of atherosclerotic disease risk, increases with age in sedentary adults. It is not known whether regular aerobic exercise modulates femoral IMT with ageing.
Methods and results
Study 1: Femoral IMT was measured in 173 sedentary, moderately active, and endurance-trained young (20–39 years), middle-aged (40–59 years) and older (60–79 years) men. IMT increased with age in all activity groups (P<0.001). However, IMT was 20–27% smaller in age-matched, endurance-trained compared with sedentary men (P<0.001), and the age-associated increase in IMT was 33% smaller in endurance-trained compared with sedentary men (+0.32 versus +0.45 mm). There was a trend for the IMT to be smaller in moderately active compared with sedentary older men, and the age-associated increase in IMT was 37% smaller in moderately active than sedentary men (+0.28 mm). Study 2: Among 74 premenopausal and postmenopausal sedentary or endurance-trained women, IMT was higher (P<0.001) in postmenopausal compared with premenopausal women regardless of activity status. However, IMT was 15% smaller in endurance-trained compared with sedentary postmenopausal women (P<0.001), and the premenopausal to postmenopausal difference in IMT was approximately 45% smaller in endurance-trained compared with sedentary women (+0.13 versus +0.23 mm).
Conclusions
Femoral IMT increases with age even in habitually exercising adults. However, the age-associated increase and absolute level of IMT are smaller in middle-aged and older adults who perform regular aerobic-endurance exercise, and may contribute to their lower incidence of atherosclerotic disease.
Introduction
Carotid and femoral artery intima–media thickness (IMT) are independent predictors of the future development of atherosclerotic diseases, including coronary artery disease, as well as cardiovascular events [1–3]. The IMT increases two to threefold between the ages of 20 and 90 years even in healthy sedentary adults [1]. This increase in IMT with adult ageing may elevate the baseline risk with which pathophysiological disease mechanisms can interact, eventually leading to clinical occlusive vascular disease [1].
There is marked inter-individual variability in the increase in IMT with advancing age [1]. There is currently little information, however, regarding the factors that influence IMT with ageing [1]. In this context, regular aerobic-endurance exercise is associated with enhanced systemic arterial endothelial function, reduced large elastic artery stiffness, and a reduced risk of arterial atherosclerotic clinical diseases in middle-aged and older adults [4, 5]. It is thus possible that habitual exercise favorably modulates large artery IMT with ageing.
We recently found no relation between habitual exercise status and carotid IMT across age in healthy men [6] and among postmenopausal women [7]. This is probably explained by the lack of an exercise effect on age-associated elevations in local (carotid) distending pressure, the primary determinant of age-associated increases in carotid IMT [6, 8]. However, this may not be the case for femoral IMT. For example, most aerobic-endurance exercise is performed primarily with the legs, and therefore results in regular (e.g. daily) sustained elevations in femoral artery blood flow. This should, in turn, increase femoral artery shear stress and nitric oxide bioactivity, thus possibly suppressing the mechanisms contributing to age-associated increases in IMT [9–11]. Our preliminary observations on the effects of habitual exercise on femoral IMT in healthy men [12] and among postmenopausal women [7] are consistent with this possibility. However, neither of these studies addressed the interactive effects of age and habitual exercise. Rather, results obtained from larger cohorts of men and women varying in age are required to provide a more direct insight regarding this hypothesis.
Accordingly, the primary aims of the present investigation were to determine if: (i) the age-related increase or absolute level of common femoral artery IMT is smaller in endurance exercise-trained compared with sedentary healthy adults; and (ii) similar associations are observed in adults who perform less frequent and intense aerobic exercise. After establishing these associations between age, habitual exercise status, and femoral IMT in men, we then performed a follow-up study to confirm that the age-related increase and absolute level of femoral IMT are also smaller in endurance exercise-trained compared with sedentary women.
Methods
Subjects
Study 1: A total of 173 healthy men aged 20–39 years (young), 40–59 years (middle-aged), and 60–79 years (older) were studied. For at least the previous year, participants were either sedentary (no regular physical activity), moderately aerobically active (light to moderate intensity exercise ≥ 3 times per week), or endurance exercise-trained (vigorous aerobic-endurance exercise ≥ 5 times per week and competing in local road running races). Study 2: A total of 74 premenopausal (20–41 years) and postmenopausal (49–80 years) sedentary or endurance-trained healthy women were studied. All postmenopausal women had an absence of menses for 1 year or more and were not taking any preparation of hormone replacement therapy. In the premenopausal women, four sedentary and six endurance-trained women were taking some form of oral contraceptives.
Participants were included if they were normotensive (< 140/90 mmHg) [13], non-smokers, and were free of overt chronic diseases, as assessed by medical history, physical examination, standard blood chemistries, hematological evaluation (e.g. blood glucose < 7 mmol/l) [14], and treadmill exercise stress test [15]. Participants who demonstrated significant intima–media thickening (> 1.5 mm) or had an ankle–brachial pressure index less than 0.90 [16] were excluded. This study complies with the Declaration of Helsinki. All procedures were reviewed and approved by the University of Colorado at Boulder Human Research Committee, and informed consent was obtained from the participants.
Measurements
Measurements were performed with subjects in the supine position. Premenopausal women were tested 1–6 days after the onset of menstruation (i.e. early follicular phase).
Common femoral artery intima–media thickness
Right common femoral artery IMT was measured from longitudinal two-dimensional (B-mode) images derived from an ultrasound machine (Toshiba SSH-140) equipped with a high-resolution linear array transducer (7.5 MHz) as originally described by Pignoli et al. [17] and more recently by our laboratory [7, 12, 18]. Within a particular study, all scans were analysed by the same experienced investigator who was blinded to the group assignment of the subjects (study 1: F.A.D.; study 2: K.L.M.). In our laboratory, the technique has excellent day-to-day reproducibility for IMT (3 ± 1% coefficient of variation) [18].
Brachial arterial blood pressure
Peripheral arterial blood pressure was measured with a semi-automated device (Dinamap; Johnson & Johnson, Tampa, Florida, USA) over the brachial artery as previously described [18].
Metabolic risk factors
Fasting plasma concentrations of cholesterol, glucose, and insulin were measured in the clinical laboratory affiliated with the University of Colorado Adult General Clinical Research Center as previously described [19].
Body composition
Total fat mass, fat-free mass, and bone density were determined using dual energy X-ray absorptiometry (DPX-IQ; Lunar Corp., Madison, Wisconsin, USA).
Maximal oxygen consumption
A modified Balke incremental treadmill exercise protocol was used to determine maximal oxygen consumption, a measure of maximal aerobic exercise capacity [20].
Statistical analysis
Two-way analysis of variance was used to determine the main effects of age (young versus middle-aged versus older) and habitual exercise status (sedentary versus moderately active versus endurance-trained) and their interaction in men (Study 1). In women (Study 2), the same statistical analysis approach was used with age groups defined as premenopausal versus postmenopausal women, and habitual exercise status defined as sedentary versus endurance-trained. In the premenopausal women, there were no differences in IMT between oral contraceptive users and non-users, so the data were combined within each group. In both studies, Pearson product-moment correlation coefficients were calculated to examine the bivariate relationships between femoral IMT and variables of interest. Significant bivariate correlations with femoral IMT were then used in stepwise multiple linear regression analyses to identify the significant independent determinants of femoral IMT. Statistical significance was set at P < 0.05. All data are reported as mean ± standard error. Data analysis was performed using SPSS software, version 12.0 (SPSS Inc., Chicago, Illinois, USA).
Results
Study 1
Subject characteristics
Selected subject characteristics are presented in Table 1. Age was associated with a higher percentage body fat, low-density lipoprotein (LDL)-cholesterol, fasting glucose and insulin (P < 0.05). At any age, habitual exercise was associated with a lower body mass, adiposity, resting heart rate, LDL-cholesterol, and fasting insulin, with the greatest effect being observed in the endurance-trained men (P < 0.05). Maximal oxygen consumption decreased with advancing age, but was progressively greater with increasing habitual exercise level (P < 0.05).
Femoral artery intima–media thickness
Values for IMT are shown in Fig. 1. IMT was greater (P < 0.0001) with increasing age, but was significantly influenced by habitual exercise status (P < 0.0001). Overall the IMT of endurance-trained men was approximately 20–27% smaller than in sedentary men (P < 0.0001) and tended to be smaller than in moderately active men (P = 0.056). The greatest difference in IMT between endurance-trained and sedentary men was observed in the older men (0.68 ± 0.03 versus 0.85 ± 0.04 mm). Moreover, the age-associated (i.e. young to older group) difference in IMT was 33% smaller in endurance-trained (+ 0.32 mm) compared with sedentary (+ 0.45 mm) men.
Overall, IMT was not significantly different (P = 0.13) in moderately active compared with sedentary men. However, in the older men the mean value for IMT was 14% lower in moderately active (0.73 ± 0.05 mm) than in the sedentary. The age-associated difference in IMT was 37% smaller in moderately active (+ 0.28 mm) compared with sedentary men.
Physiological correlates of femoral intima–media thickness
In the pooled Study 1 subject sample, age (r = 0.60) and maximal oxygen consumption (r = −0.50) were the strongest correlates of femoral IMT (both P < 0.0001). IMT was less strongly related to body fat, diastolic blood pressure, and plasma total and LDL-cholesterol (r = 0.27–0.35, all P < 0.05). A multiple stepwise regression model that included age, maximal oxygen consumption, body fat, diastolic blood pressure, and total and LDL-cholesterol revealed that both age (P < 0.001) and maximal oxygen consumption (P < 0.01) independently (r 2 = 0.34) predicted IMT.
Selected subject characteristics for study 1
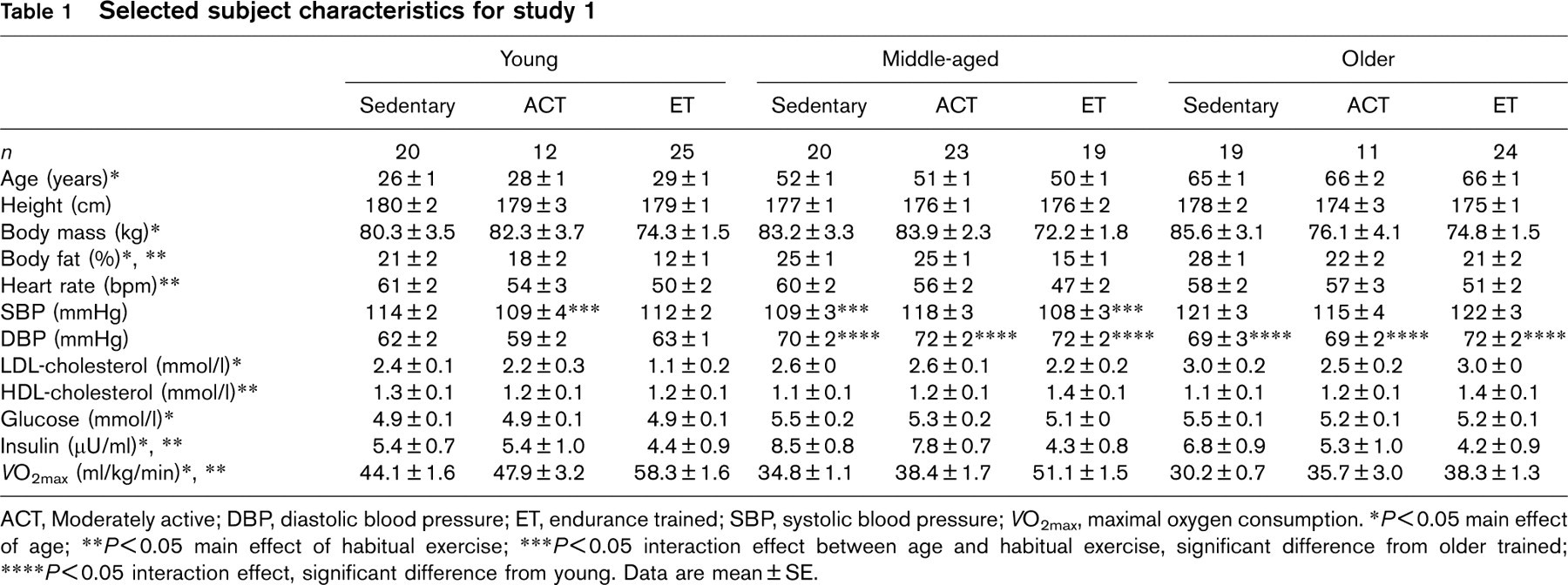
ACT, Moderately active; DBP, diastolic blood pressure; ET, endurance trained; SBP, systolic blood pressure; VO2max, maximal oxygen consumption.
∗P<0.05 main effect of age;
∗∗P<0.05 main effect of habitual exercise;
∗∗∗P<0.05 interaction effect between age and habitual exercise, significant difference from older trained;
∗∗∗∗P<0.05 interaction effect, significant difference from young.
Data are mean ± SE.
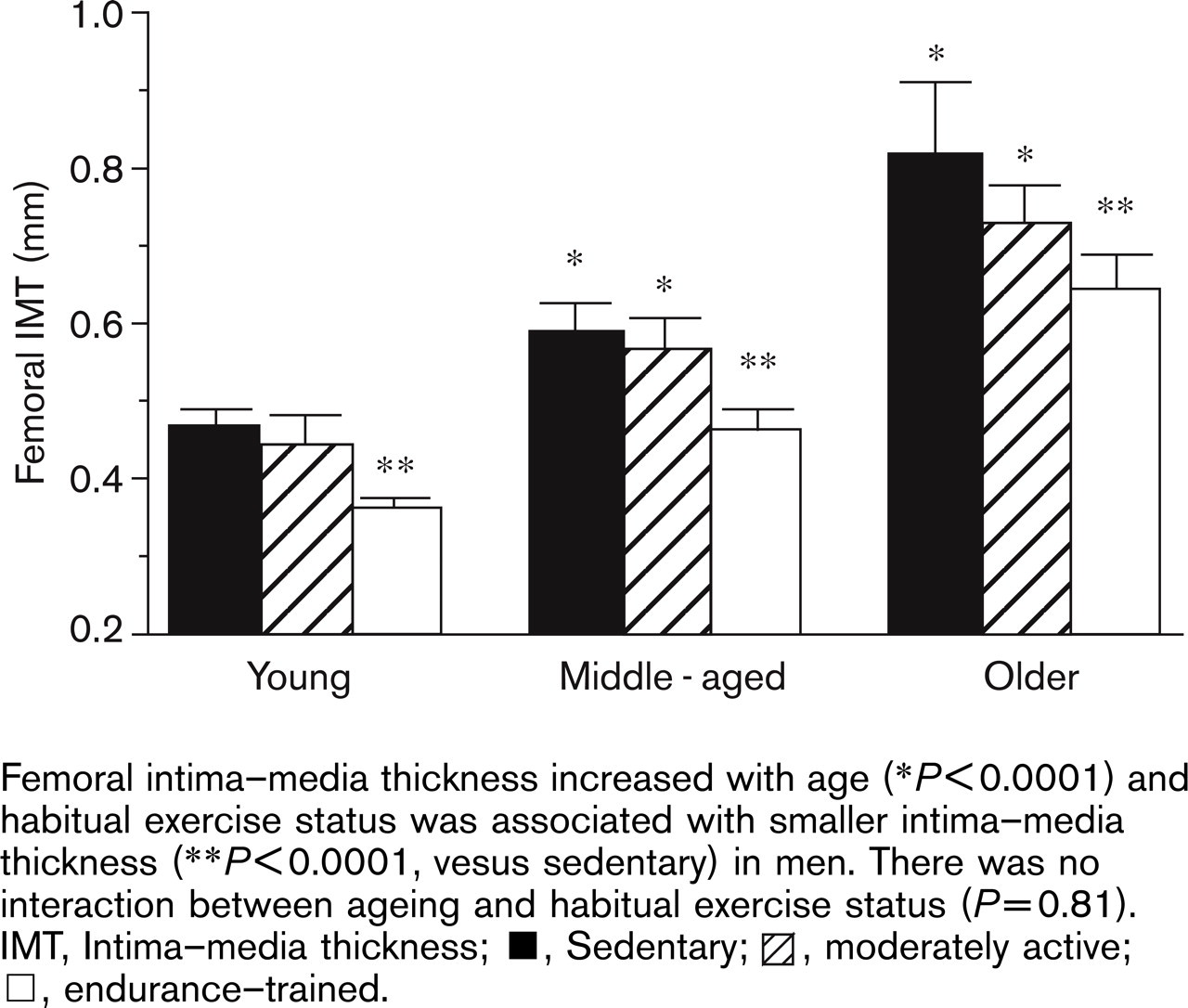
Femoral intima–media thickness increased with age (∗P<0.0001) and habitual exercise status was associated with smaller intima–media thickness (∗∗P<0.0001, vesus sedentary) in men. There was no interaction between ageing and habitual exercise status (P=0.81). IMT, Intima–media thickness; ▪, Sedentary; ○, moderately active; □, endurance–trained.
Study 2
Subject characteristics
Selected subject characteristics are shown in Table 2. There were no group differences in height, arterial blood pressure, or plasma concentrations of LDL- and high density lipoprotein (HDL)-cholesterol, insulin and glucose. Postmenopausal women had a higher percentage body fat and lower maximal oxygen consumption compared with premenopausal women (P < 0.05). Body fat was lower and maximal oxygen consumption was higher in endurance-trained compared with sedentary women (P < 0.05).
Femoral intima–media thickness
Values for IMT are shown in Fig. 2. IMT was higher (P < 0.001) in the postmenopausal compared with the premenopausal women regardless of exercise status. There was no difference in IMT between endurance-trained and sedentary premenopausal women (P = 0.45). However, among postmenopausal women IMT was 15% smaller (P < 0.001) in endurance-trained (0.49 ± 0.03 mm) compared with sedentary (0.58 ± 0.01 mm) women. Moreover, the premenopausal to postmenopausal difference in IMT was approximately 45% smaller in endurance-trained (+ 0.13 mm) compared with sedentary (+ 0.23 mm) women.
Physiological correlates of femoral intima–media thickness
In the pooled Study 2 subject sample, femoral IMT was inversely related to maximal oxygen consumption (r = −0.63, all P < 0.0001). The only other significant correlates of IMT were body mass and percentage body fat (r = 0.33 and 0.46, respectively, both P < 0.05). A multiple stepwise regression model that included maximal oxygen consumption, body fat, and body mass revealed that only maximal oxygen consumption (P < 0.0001) independently (adjusted r 2 = 0.40) predicted IMT.
Discussion
The present findings provide new insight into the modulatory influence of regular aerobic-endurance exercise on IMT with ageing in men and women free of clinical disease. First, femoral artery IMT increases with advancing age in both men and women regardless of habitual aerobic exercise behavior. Second, although femoral IMT increases with age even in physically active adults, compared with the sedentary state daily vigorous aerobic-endurance exercise is associated with a smaller age-related increase and a lower absolute femoral IMT in middle-aged and older men and postmenopausal women. Third, a more moderate frequency and intensity of aerobic exercise also tended to be associated with a smaller age-related increase in femoral IMT compared with the sedentary state, as well as a lower mean femoral IMT in men aged 60 years or older. Fourth, among healthy men and women, femoral IMT is most strongly related to age, maximal aerobic capacity, and whole body fatness. Finally, in young adults the endurance exercise-trained state is associated with a smaller femoral IMT in men, but not women.
Selected subject characteristics for study 2
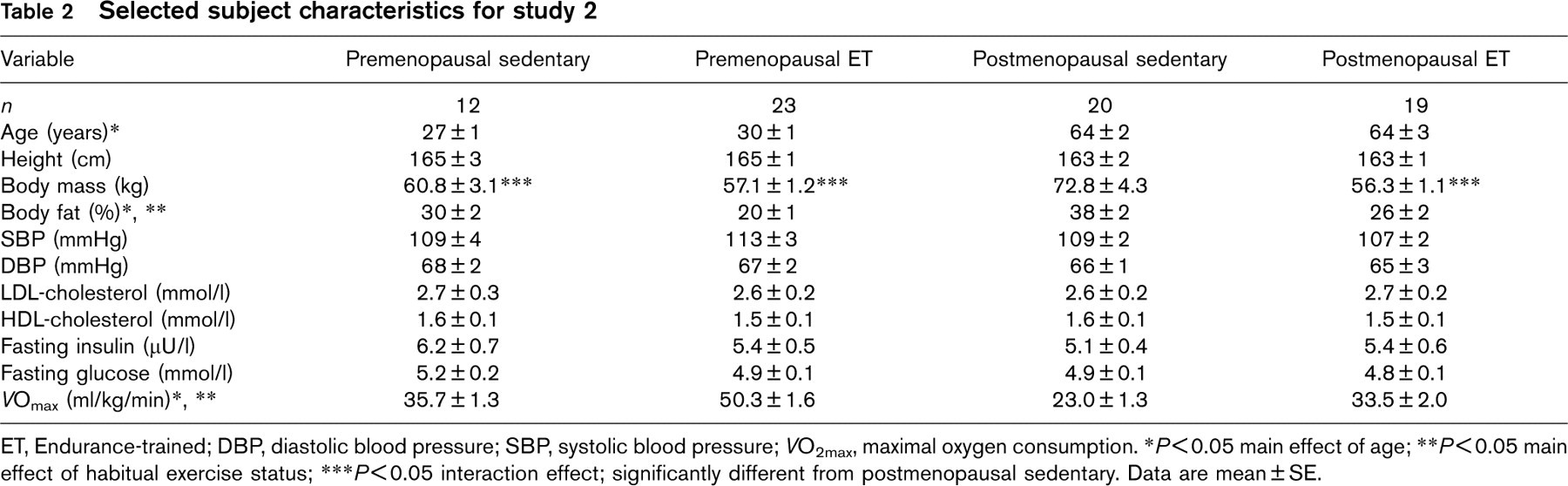
ET, Endurance-trained; DBP, diastolic blood pressure; SBP, systolic blood pressure; VO2max, maximal oxygen consumption.
∗P<0.05 main effect of age;
∗∗P<0.05 main effect of habitual exercise status;
∗∗∗P<0.05 interaction effect; significantly different from postmenopausal sedentary.
Data are mean ± SE.
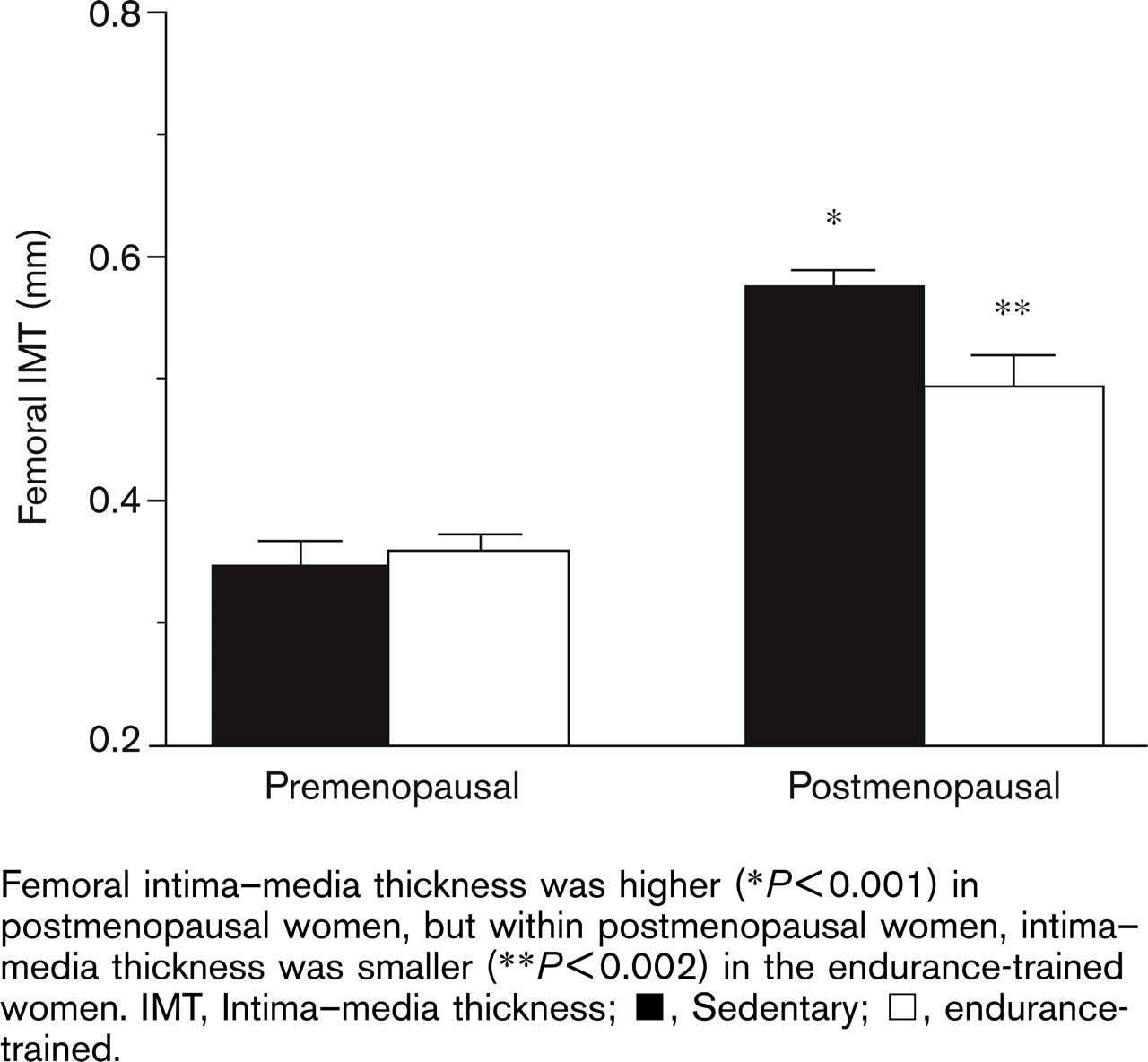
Femoral intima–media thickness was higher (∗P<0.001) in postmenopausal women, but within postmenopausal women, intima–media thickness was smaller (∗∗P<0.002) in the endurance-trained women. IMT, Intima–media thickness; ▪, Sedentary; □, endurance-trained.
Aging, habitual exercise and femoral intima–media thickness
In the present studies we were able to demonstrate for the first time that femoral IMT becomes greater with age even in endurance exercise-trained men and women. Even the performance of essentially daily vigorous aerobic-endurance exercise in adults with a low cardiovascular disease risk factor burden does not prevent the age-associated increase in femoral IMT. Rather, this observation suggests that influences directly linked to ageing in adult humans such as biological processes fundamental to cellular ageing and prolonged exposure of the vascular wall to modest adverse changes in cardiovascular disease risk factors (e.g. subclinical increases in LDL-cholesterol and arterial blood pressure) are sufficient to increase femoral artery wall thickness.
Our results do, however, provide the first evidence that some lifestyle behaviors may modulate the age-associated increase in femoral IMT in healthy adults. In particular, our findings support an important influence of habitual aerobic-endurance exercise in both attenuating the increase in femoral IMT with ageing and establishing a lower absolute femoral IMT in middle-aged or older men and postmenopausal women. The strongest, most consistent exercise-related difference in femoral IMT was observed in endurance-trained men and women compared with sedentary individuals. However, the age-associated difference in femoral IMT was also smaller in men who performed a more moderate frequency and intensity of aerobic exercise compared with sedentary men, although over all ages absolute levels of femoral IMT did not differ significantly between these two activity groups. The greatest differences in femoral IMT between the exercising and sedentary men were observed in the older groups. It thus appears that the modulatory influence of regular aerobic-endurance exercise is most evident in adults with the highest baseline femoral IMT; that is, it has a greater impact with advancing age. Importantly, the results of study 2 establish that the association between habitual vigorous exercise and femoral IMT with ageing in men also is observed in postmenopausal women, an understudied population at elevated risk of coronary artery disease [21].
Physiological correlates and mechanisms
Maximal oxygen consumption (i.e. maximal aerobic exercise capacity) was the strongest correlate of IMT in both men and women in the present studies. Adiposity was the only other significant correlate of IMT in both sexes. Other risk factors that were related to IMT included plasma total and LDL-cholesterol and diastolic blood pressure in the men and body mass in the women. Any or all of these influences may have contributed to the increases in femoral IMT with age in our overall subject samples. However, maximal aerobic capacity and body fatness were the only consistent correlates of femoral IMT that differed between men and women who participated in vigorous exercise and their sedentary peers. As such, higher aerobic fitness and lower body fatness are the phenotypical factors associated with the lower femoral IMT observed in the exercising middle-aged and older men and postmenopausal women in the present studies.
We can only speculate on the mechanisms underlying these fitness and adiposity relationships with femoral IMT. Increases in IMT in healthy adults are thought to be mediated primarily by smooth muscle cell hypertrophy within the intimal layer [22], although some contribution of subclinical atherosclerosis cannot be ruled out. The vascular endothelium is responsible for maintaining vascular homeostasis, and does so by balancing the production and release of factors that are known to modulate vascular smooth muscle tone, hypertrophy or migration to the intimal layer. The endothelium releases factors with vasodilator, antihypertrophic and antiproliferative effects (e.g. nitric oxide), as well as factors that are vasoconstrictors, proliferative and hypertrophic (e.g. endothelin-1 and angiotensin II). Habitual exercise can influence several of these local factors, including the growth-promoting factors angiotensin II and endothelin-1 [23, 24]. In addition, the short-term elevations in leg blood flow during frequently performed exercise and the resulting increase in shear stress are known to increase vascular nitric oxide release [9], which may also act to suppress femoral artery wall thickening [11]. Increased adiposity or the obese state appear to have the opposite (adverse) effects on these putative modulators of arterial wall thickness [25, 26].
Habitual exercise and femoral intima–media thickness in young men versus women
We found that a smaller femoral IMT in endurance-trained compared with sedentary individuals was observed in young adult men, but not in premenopausal women (Figs 1 and 2). This difference may be explained by the high circulating levels of estrogen in the women. We recently demonstrated that sedentary postmenopausal women using chronic estrogen supplementation since the onset of menopause have a smaller femoral IMT compared with their estrogen-deficient sedentary peers, and similar to that of postmenopausal endurance-trained women [7]. The endogenously high plasma estrogen concentrations in sedentary premenopausal women in the present study may act to reduce the IMT of the femoral artery wall, thus negating any corresponding effects of habitual exercise observed in the endurance-trained premenopausal women.
Habitual exercise effects on femoral versus carotid intima–media thickness
The present findings on femoral IMT differ from our previous observations on habitual aerobic exercise and the age-associated increase in carotid IMT [6, 7]. The physiological basis for this difference is unknown. It may be related to the fact that acute leg exercise produces local changes in arterial shear stress or other hemodynamic influences in the femoral artery to which the carotid arteries are not subjected. Repeated on a regular basis, this stimulus could produce unique adaptations not observed systemically in large conduit arteries. Moreover, local (carotid) distending pressure [8], the primary determinant of age-associated increases in carotid IMT, is not affected by habitual exercise status [6]. Finally, the influence of habitual exercise may be different among vascular beds as a result of differences in arterial wall composition, signaling cascades, or responses to signals that modulate the arterial wall [27].
Clinical significance
Our findings may have important clinical implications. Arterial IMT equals or exceeds that of most other traditional risk factors for cardiovascular disease [27]. IMT is an independent predictor of coronary atherosclerosis, cardiovascular events, and occlusive peripheral artery disease [2, 28–30]. Moreover, wall thickening is believed to contribute to increases in arterial stiffness and systemic vascular resistance, which would, in turn, increase arterial blood pressure and the pulsatile afterload on the left ventricle, thereby increasing the risk of hypertrophic heart disease [1, 31]. Recent findings indicate that femoral IMT may be a stronger predictor of coronary atherosclerosis than carotid IMT [2, 3]. The smaller age-associated increases and lower absolute femoral IMT in habitually exercising adults may act to reduce baseline femoral IMT and delay or even prevent the attainment of pathological levels, thus preventing the development of clinical atherosclerotic diseases, particularly peripheral artery disease. Importantly, the strongest association between regular exercise and femoral IMT is observed in middle-aged and older men and in post-menopausal women, namely the groups at the greatest risk of vascular disease.
Limitations
It is important to emphasize that we only studied healthy non-smoking adults without evidence of overt chronic diseases. As such, our results can only be generalized to this population. It is possible that habitual exercise could have even greater beneficial effects on IMT in smokers, adults with other risk factors, or patients with chronic disease (i.e. atherosclerosis, type 2 diabetes, hypertension). Relatedly, given our rigorous inclusion criteria, it is possible that even our sedentary healthy older men and postmenopausal women may be genetically protected from developing atherosclerosis; if so, we may be underestimating the impact of both recreational activity and vigorous exercise on IMT. Moreover, we did not study recreationally active women, and thus cannot rule out a possible influence of this level of habitual exercise on age-associated increases in femoral IMT in women. Finally, we only studied pre and postmenopausal women; therefore, we cannot generalize our findings to perimenopausal women.
Conclusion
The results of the present complementary studies on healthy men and women demonstrate that femoral IMT increases less with age and that absolute femoral IMT is lower in middle-aged and older adults who regularly perform aerobic-endurance exercise compared with their sedentary peers. This may be an important factor contributing to the lower prevalence of peripheral occlusive arterial diseases in habitually active middle-aged and older adults.