
Abstract
Background
Normal endothelial function depends on nitric oxide (NO) release by endothelial cells. Asymmetric dimethylarginine (ADMA), by competing with
Design
A nested case–control study within the Coronary Artery Risk Development in Young Adults (CARDIA) cohort, an observational study among young adults residing in four US cities.
Methods
Participants were 263 white and black male and female cases with the presence of CAC and 263 sex and race-matched controls without evidence of CAC by computed tomography, 33–47 years old in 2000–2001.
Results
The median level (range) of ADMA was significantly higher in cases (0.55; 0.20–2.22 μmol/l) than in controls (0.53; 0.32–1.30 μmol/l; P=0.03). In conditional logistic regression adjusting for age, field center, educational attainment, smoking status, alcohol consumption, body mass index, waist circumference, hypertension, diabetes, low-density lipoprotein and high-density lipoprotein-cholesterol, triglycerides, renal function and C-reactive protein, the highest tertile of ADMA, compared with the lowest tertile, was associated with 1.80 (95% confidence interval 1.03–3.15) increased odds of the presence of any CAC. By linear regression, a significant independent relationship was also found between ADMA and the degree of CAC.
Conclusion
These results support a role for ADMA as a biochemical marker of CAC.
Introduction
Endothelial dysfunction is a key early feature of atherosclerotic cardiovascular disease affecting both the peripheral and myocardial vessels [1, 2]. Normal vascular function is dependent on nitric oxide (NO) released by healthy endothelial cells [3]. NO is synthesized from
To date, epidemiological studies of ADMA are sparse and have focused on middle-aged or older adults [16–20]. Moreover, no population-based studies of ADMA have been conducted in the United States including ethnic minorities. Given the young age of the participants, the biethnic composition of the cohort, and the availability of coronary artery calcium measures (a surrogate measure of atherosclerotic burden), the Coronary Artery Risk Development in Young Adults (CARDIA) study offers a unique opportunity to obtain a better understanding of the role of ADMA in the early stages of atherosclerosis. The specific aims of this study are to examine, among white and black men and women aged 33–47 years, the demographic, behavioral and biochemical correlates of the ADMA level and the independent association of ADMA with coronary artery calcification (CAC).
Methods
Source population and study design
The CARDIA study is an ongoing longitudinal investigation of heart disease risk factors and subclinical coronary artery disease (CAD) among black and white men and women aged 18–30 years at baseline in 1985–1986. More details of the study design, recruitment and procedures have been published elsewhere [21, 22]. Participants were recruited in four field centers: Birmingham, Alabama; Chicago, Illinois; Minneapolis, Minnesota; and Oakland, California.
For the current study, we used a nested case-control design utilizing data collected at the CARDIA year 15 examination (June 2000–October 2001), in which the participants were 33–47 years old. Cases (n=263) were all study participants who had evidence of CAC (i.e. coronary calcium score >0), and controls were CARDIA cohort members chosen at random with a calcium score of zero and individually matched to cases on sex and race. No matching was performed for any other variables. Of the original 274 cases and 274 controls, 11 case–control pairs were excluded in the final analysis for missing data on covariates of interest.
Age, race/ethnicity, educational attainment, alcohol and tobacco use were ascertained by self-report [23]. Blood samples were drawn after an overnight fast. The protocols for lipid determination can be found elsewhere [24–26]. Anthropometric measures (weight, height, waist/hip ratio) were performed according to the CARDIA study protocol [27], and body mass index (BMI) was calculated as weight/height squared (kg/m2). Fasting plasma glucose was determined using the hexokinase-ultraviolet method [28] and fasting plasma insulin by radioimmunoassay (Linco Research Inc., St Louis, Missouri, USA). The homeostatic model assessment value for insulin resistance (HOMA–IR) was calculated as previously described [29], as follows: HOMA–IR=[(glucose in mg/dl × 0.05551) × insulin in μU/ml]/22.5. C-reactive protein (CRP) was measured using the latex method (BN II nephelometer; Dade Behring, Deerfield, Illinois, USA) [30]. Hypertension was defined as a self-report of hypertension or systolic blood pressure of 140mmHg or greater or diastolic blood pressure of 90 mmHg or greater, or the use of antihypertensive medication. Diabetes was defined as a self-report of diabetes mellitus or fasting blood glucose of 126 mg/dl or greater or the use of antidiabetic medication. Hormone replacement therapy and the use of cholesterol-lowering medication were ascertained by self-report. Renal function was assessed as glomerular filtration rate (GFR) estimated by the Modification of Diet in Renal Disease study formula [31]. The Institutional Review Boards of the field centers approved the study, and all participants gave informed written consent.
Asymmetric dimethylarginine assay
An enzyme-linked immunosorbent assay (ELISA) for ADMA (DLD Diagnostika, Hamburg, Germany) was performed on ethylenediammine tetraacetic acid plasma samples by laboratory staff from the Stanford University Division of Cardiovascular Medicine who were blinded to the case–control status of the participants. ADMA standards and plasma samples were added to the wells of a reaction plate for acylation. The acylation buffer (25 μl), adjustment buffer (25 μl) and acylation reagent (25 μl) were added to the wells, and the mixture was incubated at room temperature on a horizontal shaker. After adding an additional 100 μl adjustment buffer/equalizing reagent to each well, the aliquots from each well were pipetted into the ELISA microtitre plate and the antiserum solution was added to each well, and then incubated for 15–20 h at 4°C. Subsequently, the wells were emptied and rinsed with wash buffer, and a solution of the enzyme conjugate (100 μl) was added to each well and incubated for 1 h at room temperature on a horizontal shaker. Then the wells were rinsed with wash buffer and the substrate solution (100 μl) was added. After 20–30 min, a stop solution was added, and the optical density was then read at 450 nm using a microtitre plate reader (Tecan GENios, Salzburg, Austria). This ELISA assay has been validated against liquid chromatography–mass spectrometry (n=29; r=0.984; P < 0.001) [32].
Coronary computed tomography protocol
Two scans were obtained on each participant, 1–2 min apart. Participants were scanned in the supine position (without getting off the table between scans) over a hydroxy-apatite phantom to adjust for scanner differences across field centers. The Chicago and Oakland field centers used Imatron C-150 scanners, the Birmingham field center used a GE Lightspeed Qxi scanner and the Minneapolis field center used a Siemens VZ scanner. An experienced and trained computed tomography (CT) image analyst (blinded to non-scan data and to the order of images) identified the courses of the coronary arteries using specially developed image-processing software and calculated the Agatston score [33]. Additional quality control procedures, including steps to ensure the comparability of scanners across field centers, have previously been described [34]. In most cases, the CT examination took place less than 30 days after the blood draw during the clinic examination.
Statistical analysis
Univariate case–control differences were ascertained using the t-test for normally distributed continuous variables, the Wilcoxon rank-sum test for continuous variables that were not normally distributed (alcohol intake, triglycerides, HOMA–IR, CT and ADMA), and the chi-squared test for categorical variables. To assess bivariate associations between ADMA and the other study covariates, we estimated the means for continuous variables or proportions of categorical variables according to sex/race-specific tertiles of ADMA adjusting for sex, race, field center and case-control status. A contrast between the lowest and the highest tertiles of ADMA was performed using analysis of covariance (ANCOVA). Conditional logistic regression was then applied to quantify the relative odds of CAC (i.e. calcium score >0 versus calcium score of 0) associated with 1 (sex and race-specific) SD linear increment in ADMA. We assigned a sequential matching number to each case-control pair and employed the SAS PHREG procedure (SAS software, version 8; SAS Institute, Cary, North Carolina, USA) with the matching number specified as the stratification variable. We also considered models with ADMA entered as (sex and race-specific) tertiles 2 and 3 with tertile 1 as the reference group. Both the SD and the tertile cutpoints were estimated among controls. Four sequential models were fitted: model 1 with no adjustment for covariates (sex and race are adjusted for by design); model 2 further adjusting for age, field center, educational attainment, alcohol consumption and cigarette smoking; model 3 further adjusting for BMI, waist circumference, low-density lipoprotein (LDL) and high-density lipoprotein (HDL)-cholesterol, triglycerides, diabetes, hypertension and CRP; and model 4 further adjusting for renal function. We also ascertained whether the association between ADMA and the presence of CAC differed by sex, race, LDL-cholesterol, diabetes, smoking and hypertension. We tested, in unconditional logistic regression models, the significance of the interactions between ADMA as a continuous variable and these other variables as either categorical variables [sex, race, diabetes, smoking (former or current versus never) and hypertension] or as a continuous variable for the case of LDL-cholesterol. None of these interactions were statistically significant at the 0.05 level, and therefore no results stratifying by these variables are presented. Finally, in order to examine whether there was a monotonic relationship between ADMA and degree of CAC (not just the presence or absence of CAC), we estimated ADMA medians according to levels of CAC and then used linear regression of log (calcium score +1) on log (ADMA∗100) as the main continuous predictor, and the same covariate adjustment sequence that we used in the logistic analysis (i.e. models 1–4).
Results
Compared with controls, cases tended to be slightly older and were significantly more likely to have hypertension (Table 1). Mean alcohol intake, LDL-cholesterol and triglycerides were also significantly higher in cases than in controls. Waist circumference was marginally larger and HOMA–IR marginally higher in cases than in controls. There were no statistically significant differences in educational attainment, smoking status, diabetes, cholesterol-lowering medication use, hormone replacement therapy in women, BMI, fasting glucose, HDL-cholesterol and CRP in cases compared with controls. Median ADMA was significantly higher in cases (0.55 μmol/l, range 0.20–2.22 μmol/l) than in controls (0.53 μmol/l, 0.32–1.30 μmol/l; P=0.03). Among the cases, the median calcium score was 22 (range 0.8–3923); 47% had a calcium score under 20, and 33% had a calcium score of 50 or above. In descriptive analysis stratifying by sex/race groups (Fig. 1), median ADMA levels were higher in cases than in controls in all four sex/race groups, and the case–control difference tended to be greater in men than in women.
Table 2 shows the means of continuous variables and the proportion of categorical variables according to sex/race-specific tertiles of ADMA, after adjustment for sex, race and case–control status. We found a borderline significant pattern of increased BMI with increasing ADMA levels (P=0.06); the contrast of BMI between the lowest and highest tertiles of ADMA was statistically significant (P=0.02). No significant associations were found between ADMA and HOMA-IR or between ADMA and renal function.
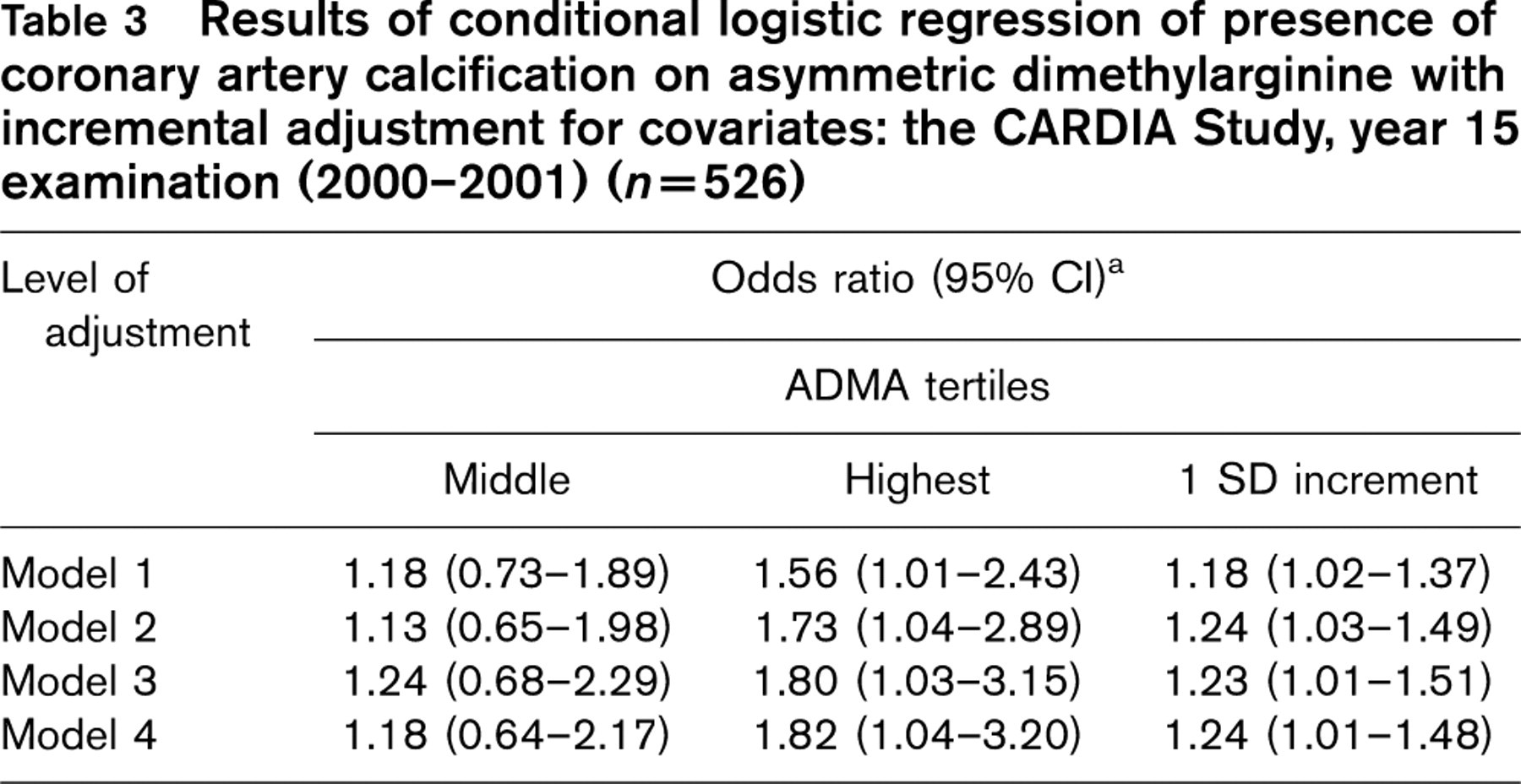
In unadjusted conditional logistic regression (model 1), there was a significant association between ADMA and the presence of CAC [odds ratio (OR) per 1 SD increment 1.18; 95% confidence interval (CI) 1.02–1.37; Table 3]; the unadjusted OR for the upper ADMA tertile, relative to the lowest tertile, was 1.56 (95% CI 1.01–2.43). After adjusting for age, field center, educational attainment, smoking status and alcohol consumption (model 2), the association became stronger for the upper ADMA tertile (OR 1.73; 95% CI 1.04–2.89). After further adjustment for BMI, waist circumference, hypertension, diabetes, LDL and HDL-cholesterol, triglycerides and CRP in model 3 and for all these factors plus renal function in model 4, the risk relationship did not change appreciably. Median levels of ADMA according to the degree of CAC were as follows (in μmol/l): 0.53 in controls (n=263), 0.56 in cases with a CAC score below 20 (n=123), 0.55 in cases with a CAC score between 20 and 49 (n=54), 0.55 in cases with a CAC score between 50 and 99 (n=42), 0.57 in cases with a CAC score between 100 and 399 (n=36), and 0.59 in cases with a CAC score of 400 and above (n=8). In the linear models with log (calcium score +1) as the dependent variable and log (ADMA∗100) as the independent variable, the estimates of the slopes (± standard error; P value) were 0.69 ± 0.36 (P=0.05) in model 1, 0.78 ± 0.35 (P=0.03) in model 2, 0.79 ± 0.34 (P=0.02) in model 3, and 0.82 ± 0.35 (P=0.02) in model 4.
Characteristics of cases and controls: the CARDIA Study, year 15 examination (2000–2001)

ADMA, Asymmetric dimethylarginine; CRP, C-reactive protein; GFR, glomerular filtration rate; HOMA–IR, homeostatic model assessment value for insulin resistance; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
a P value from t-test for normally distributed continuous variables, Wilcoxon two-sample test for continuous variables not-normally distributed and chi-squared test for categorical variables.
bHOMA–R was available in 262 cases and 262 controls; CRP was available in 255 cases and 258 controls; GFR was available in 262 cases and 263 controls.
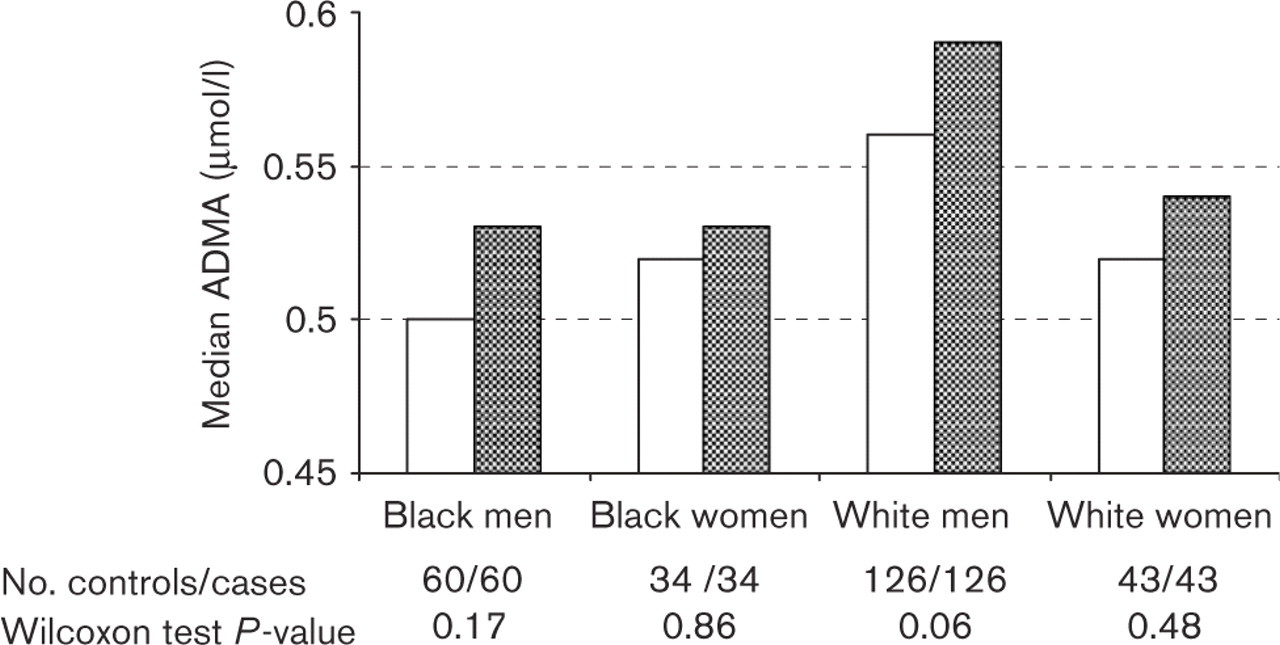
Asymmetric dimethylarginine (ADMA) medians by sex–race groups and case–control status. □, Controls; ▪, coronary artery calcification cases.
Means of continuous variables and proportions of categorical variables, adjusted for age, sex, race, field center and case–control status, by tertiles of asymmetric dimethylarginine (n=526): the CARDIA Study, year 15 examination (2000–2001)
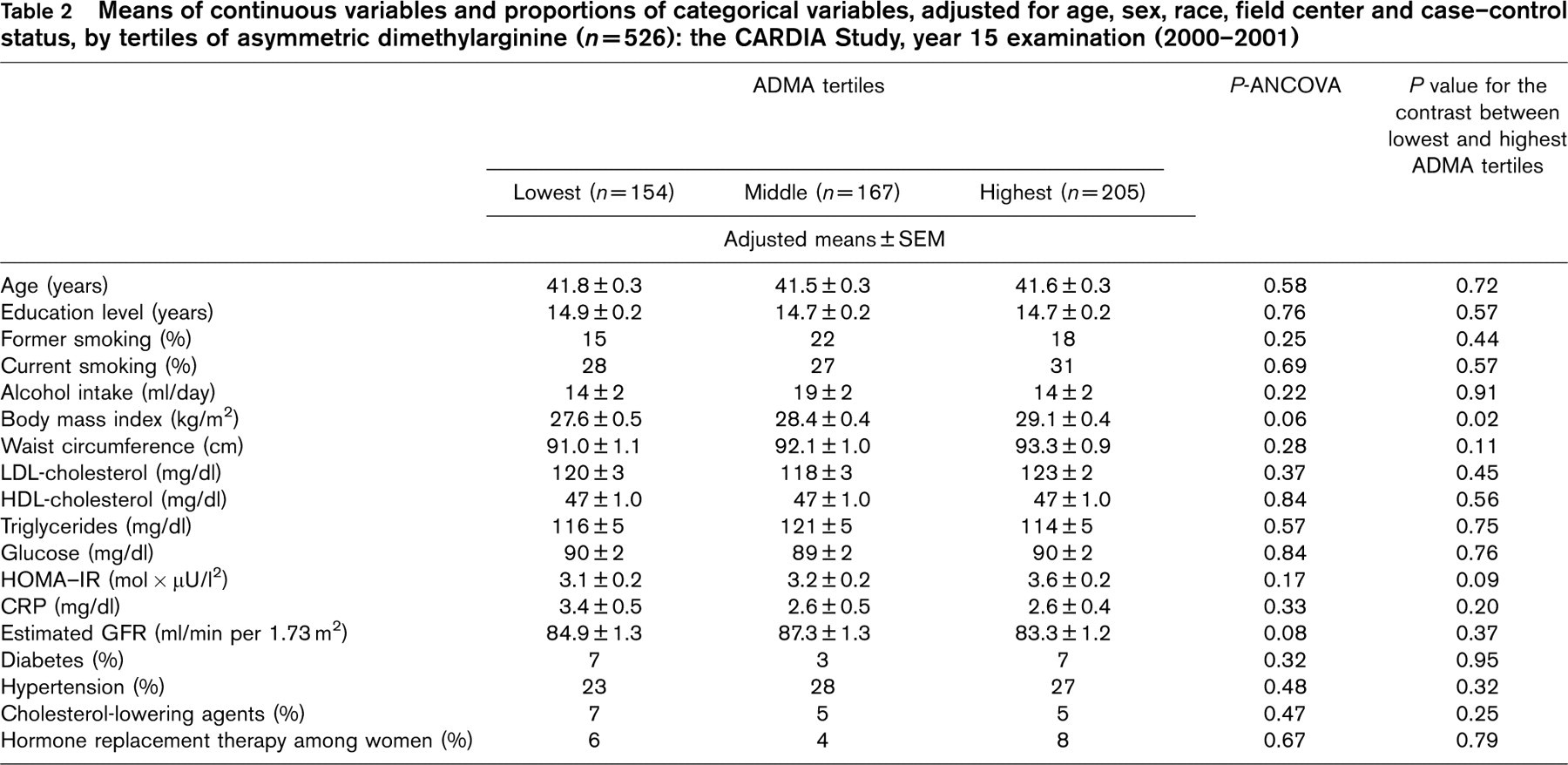
ADMA, Asymmetric dimethylarginine; ANCOVA, analysis of covariance; CRP, C-reactive protein; GFR, glomerular filtration rate; HOMA–IR, homeostatic model assessment value for insulin resistance; HDL, high-density lipoprotein; LDL, low-density lipoprotein. The ADMA tertile cutpoints were as follows (μmol): black men (<0.481, 0.481–0.534, >0.534); black women (<0.483, 0.483–0.566, >0.566); white men (<0.522, 0.522–0.601, >0.601) and white women (<0.495, 0.495–0.570, >0.570).
Results of conditional logistic regression of presence of coronary artery calcification on asymmetric dimethylarginine with incremental adjustment for covariates: the CARDIA Study, year 15 examination (2000–2001) (n=526)
CI, Confidence interval.
aWith the lowest tertile as the reference level. Model 1: no adjustments. Model 2: age, field center, educational attainment, alcohol consumption, cigarette smoking. Model 3: model 2 covariates plus body mass index, waist circumference, hypertension, diabetes, LDL-cholesterol, HDL-cholesterol, triglycerides and C-reactive protein. Model 4: model 3 plus estimated glomerular filtration rate.
Discussion
This study documents, for the first time, an independent association of ADMA with the presence versus the absence of CAC among young adults entering middle life who were free of clinically evident cardiovascular disease. Moreover, there was a significant graded association between ADMA and the degree of CAC. These findings support the notion that elevated plasma ADMA (a surrogate measure of endothelial dysfunction) may be a useful biomarker of coronary atherosclerotic disease burden. This finding is consistent with recent evidence that enhanced coronary calcification is strongly related to flow-mediated vasodilation in patients with suspected CAD [35]. It should be noted, however, that, in our study, the difference in median ADMA levels between those with and without CAC was rather small (0.02 μmol/l). In addition, the increase in ADMA that is clinically meaningful and the degree to which ADMA may add prognostic information for clinical CAD above and beyond other well-established risk factors is presently unknown.
How might chronically elevated levels of plasma ADMA promote the initiation or the progression of atherosclerosis? The acute systemic administration of ADMA to healthy individuals has been shown significantly to reduce NO generation, and to cause an increase in systemic vascular resistance and blood pressure [36]. Endothelium-derived NO is vital for the maintenance of normal vascular tone, and has a multitude of anti-atherogenic properties including the inhibition of endothelial adhesiveness, a reduction of platelet activation, the prevention of smooth muscle cell proliferation, and a reduction of oxidative stress [37, 38].
Earlier studies characterized ADMA as a uremic toxin that accumulates in renal disease and causes endothelial dysfunction [7]. Subsequent studies have suggested that the major cause of ADMA elevation in patients with cardiovascular disease or associated risk factors is an impairment of ADMA metabolism. Metabolic factors that inhibit ADMA degradation include LDL-cholesterol, glucose, and homocysteine [39, 40].
Our results are consistent with earlier studies showing associations between ADMA and different manifestations of cardiovascular disease. One study among non-smoking middle-aged Finnish men found that the highest quartile of ADMA (>0.62 μmol/l, compared with the other three quartiles combined) was associated with a fourfold increased risk of acute coronary events after adjustment for LDL, diabetes, hypertension and a family history of CHD [16]. A Japanese study demonstrated a relationship of ADMA with carotid intima–media thickness [17]. In a Korean study [18], elderly subjects with elevated ADMA concentrations were found to be at increased risk of ischemic stroke. ADMA was shown to be significantly correlated with coronary flow reserve measured by transthoracic Doppler echocardiography and with flow-mediated vasodilation among hypertensive patients [19]. In the AtheroGene Study [20], a prospective cohort of 1908 patients with CAD, the risk of a future cardiovascular event was associated with increasing thirds of baseline ADMA, such that individuals in the highest third at entry had a hazard ratio 2.5 times higher than those in the lowest third, and this relationship remained nearly unchanged after adjustment for potential con-founders.
There is evidence that NO deficiency and elevated ADMA levels occur with chronic kidney disease; this phenomenon may lead to hypertension and to further cardiovascular complications [41]. The increased oxidative stress of chronic kidney disease is likely to be a primary cause of the increased plasma ADMA because its catabolic enzyme, DDAH, is extremely sensitive to inhibition by oxidants. We, however, did not find an association between ADMA and estimated GFR in our sample of young adults; we speculate that this null finding may be due to the fact that renal function was generally preserved in our sample.
Recent evidence indicates that plasma ADMA levels may be reduced by either pharmacological or non-pharmacological interventions. For example, ADMA levels are increased in patients with insulin resistance, and reduced after treatment with rosiglitazone [15]. After weight loss following gastroplastic surgery in morbidly obese patients, ADMA concentrations decreased in parallel with an improvement of parameters associated with the metabolic syndrome [42].
The calcification of atheroma occurs early in plaque development as part of the inflammatory pathophysiological cascade of CAD, and is actively regulated like bone mineralization [43]. Although its value in cardiovascular risk stratification is not definitely established, the presence of higher thresholds of coronary calcium have been shown to predict angiographic CAD [44] and coronary events [45–47] independently. A new line of evidence suggests that the pattern of calcification (spotty versus intermediate versus extensive, reflecting the morphology of the plaque and the extent of arterial remodeling) may allow the identification of vulnerable plaques in coronary arteries [48].
We recognize several significant limitations in our study. First, the observational and cross-sectional nature of the data (ADMA was measured only at the year 15 examination) precludes any causal inference. Second, the low prevalence and low CAC scores among CARDIA participants that may have resulted in an underestimation of the differences in ADMA between those with and without CAC. Third, the study was underpowered for stratified analysis by sex/race groups. However, as demonstrated in Fig. 1, the association between ADMA and the presence of CAC was consistent across sex/race groups, albeit more pronounced in white men and black men. Fourth, our cases and controls were selected from four different sites and we did not require that each case and his/her matched control came from the same geographical location. We addressed this limitation by adjusting for field center in the analysis. Finally, we used an ELISA (DLD Diagnostika) method for the determination of ADMA, which has been shown to correlate weakly with the reversed phase high-performance liquid chromatography method [49]. Therefore, our ADMA levels may not be comparable with earlier studies that relied on high-performance liquid chromatography. On the other hand, our study has the unique characteristic of being based on a population-based, biethnic sample with minimal interference from clinically evident cardiovascular disease or pharmacological agents (only 5% of participants were using cholesterol agents and 6% of women were on hormone replacement therapy).
Conclusion
ADMA was independently associated with CAC among young adults entering middle life, suggesting that ADMA may be a useful marker of the initial stages of atherosclerosis. Additional studies are warranted to establish more definitively the value of ADMA as a prospective marker of clinical cardiovascular risk in populations with adequate representation of both sexes and race/ethnic groups. In addition, more research is needed to elucidate the usefulness of lowering ADMA using medication or non-pharmacological approaches, so as to prevent atherosclerosis progression and its consequences.