
Abstract
Background
Methods
Results
Conclusion
Introduction
Myocardial infarction is regarded as a major public health challenge as a result of its high occurrence and its impact on morbidity, mortality, and costs to society [1, 2]. Therefore, numerous potential risk factors for myocardial infarction have been extensively investigated. Among the most established risk factors are smoking, elevated blood pressure levels, unfavourable levels of cholesterol, diabetes mellitus, physical inactivity, and obesity [3, 4]. In addition to their causal relationship with myocardial infarction, these factors are characterized by a lasting high prevalence in most developed countries and by a potential modifiability, and are thus considered to be suitable targets for prevention strategies [5–7].
To our knowledge, in Germany only one population-based cohort study, the MONICA Augsburg study, has as yet evaluated the association between some of the classic risk factors and incident myocardial infarction in men [8]. However, the study is based on the south-western region of Germany only [8], and substantial regional differences in the prevalence of classic risk factors and myocardial infarction mortality within Germany have been observed [9]. Therefore, the aim of this study was to examine thoroughly the prevalence and the impact of individual potentially modifiable classic risk factors and their combinations on incident myocardial infarction within the eastern German European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam cohort.
Methods
Study population
The EPIC-Potsdam cohort comprises 27548 subjects aged 35-65 years recruited between 1994 and 1998 from the general population of the city of Potsdam and its surrounding communities located in eastern Germany [10]. The Ethics Committee of the State of Brandenburg, Germany, gave approval for all study procedures, and informed consent was obtained from participants before enrolment into the study. Baseline examinations included an interview on lifestyle habits and medical history, anthropometric measurements, a food frequency questionnaire, and blood sampling. Follow-up questionnaires are biennially mailed to participants to obtain updated measurements of baseline characteristics and to evaluate newly developed diseases, including myocardial infarction.
Potential cases of incident myocardial infarction were identified based on self-reports of myocardial infarction diagnosis or on death certificates. All potential incident cases who developed myocardial infarction (International Classification of Disease version 10 I21.0-I21.9) up to 30 April 2004 were verified by reviewing the patients’ medical records or death certificates according to World Health Organization MONICA criteria [11]. Participants with a history of myocardial infarction at baseline, a missing follow-up status, or missing values for risk factors or confounder variables were excluded. Consequently, the final study population consisted of 159 incident cases of myocardial infarction (87 non-fatal and 33 fatal in men, 29 non-fatal and 10 fatal in women) and 26 795 participants without this event (10 343 men, 16 452 women).
Risk factor assessment
The six potentially modifiable classic risk factors were defined based on participants’ self-reports given in the standardized interview or on measurements performed by standardized and quality-controlled procedures by trained personnel at baseline examination [12]. Smoking was defined as being a current smoker or having quit smoking less than 5 years ago. This classification was used because the coronary risk of ex-smokers converges to the risk of never-smokers after 3-5 years [13]. Hypertension was defined by measuring a systolic blood pressure of 140 mmHg or greater or a diastolic blood pressure of 90 mmHg or greater, or by self-reporting an intake of antihypertensive medication or a hypertension diagnosis. Diabetes mellitus was defined by a reported intake of antidiabetic medication or a reported diabetes diagnosis. Similarly, hyperlipidemia was defined by self-reporting an intake of antihyperlipidemic medication or hyperlipidemia. Abdominal obesity was defined by a ratio of measured waist circumference to measured hip circumference of 0.8 or greater in women and 0.9 or greater in men [14]. According to recommendations of a regular moderate-intensity activity of at least half an hour on most days of the week [15], participants were judged to be inactive if they reported to be engaged in sports (including all sporting activities except for cycling) less than 2 h per week during summer or winter.
Statistical analysis
All relative risks of myocardial infarction and their 95% confidence intervals were estimated by Cox proportional hazards regressions with the attained age (defined by the participants’ age at recruitment and their age at myocardial infarction incidence or censoring) as the dependent time variable. Relative risks for each single risk factor were adjusted for sex, educational attainment (less than university degree versus university degree), alcohol intake (non-drinkers, 0.1-5, 5.1-20, 20.1-40, and > 40 g/day), and the respective other five risk factors. For examining the joint effect of several risk factors only the five risk factors smoking, hypertension, diabetes, abdominal obesity, and sporting inactivity that were significantly associated with myocardial infarction were considered. Relative risks for the number and combinations of risk factors were adjusted for sex, hyperlipidemia, educational attainment, and alcohol consumption. Combinations of risk factors significantly associated with myocardial infarction were identified as suggested by Hoffmann et al. [16] by using a stepwise Cox proportional hazards regression starting with a model including all possible combinations of the absence and presence of the five dichotomous risk factors. Only those combinations with a significant relative risk and a significant population attributable risk (PAR) were considered as most relevant for the risk of myocardial infarction.
PAR for each single risk factor were derived by an equation postulated by Miettinen [17], taking the corresponding relative frequencies and multivariate adjusted relative risks into consideration. Attributable risks for combinations of risk factors were determined based on an equation suggested by Bruzzi et al. [18]. 95% confidence intervals of the PAR were estimated by a variance formula proposed by Whittemore [19]. All analyses were performed using SAS software, version 9.1 (SAS Institute, Cary, North Carolina, USA).
Results
During an average follow-up time of 4.6 years, 159 cases of incident myocardial infarction (120 men, 39 women) occurred among 26954 participants (10463 men, 16491 women). The observed incidence rate of myocardial infarction was increasing with age (1.65, 8.95, 19.88, and 26.31 per 10 000 person-years for 35-44, 45-54, 55-64, and > 65 years at baseline, respectively) and was higher for men than for women (24.50 versus 5.16 per 10 000 person-years).
Baseline characteristics of incident cases of myocardial infarction (n = 159) and non-cases (n = 26 795) of the EPIC-Potsdam study, 2004
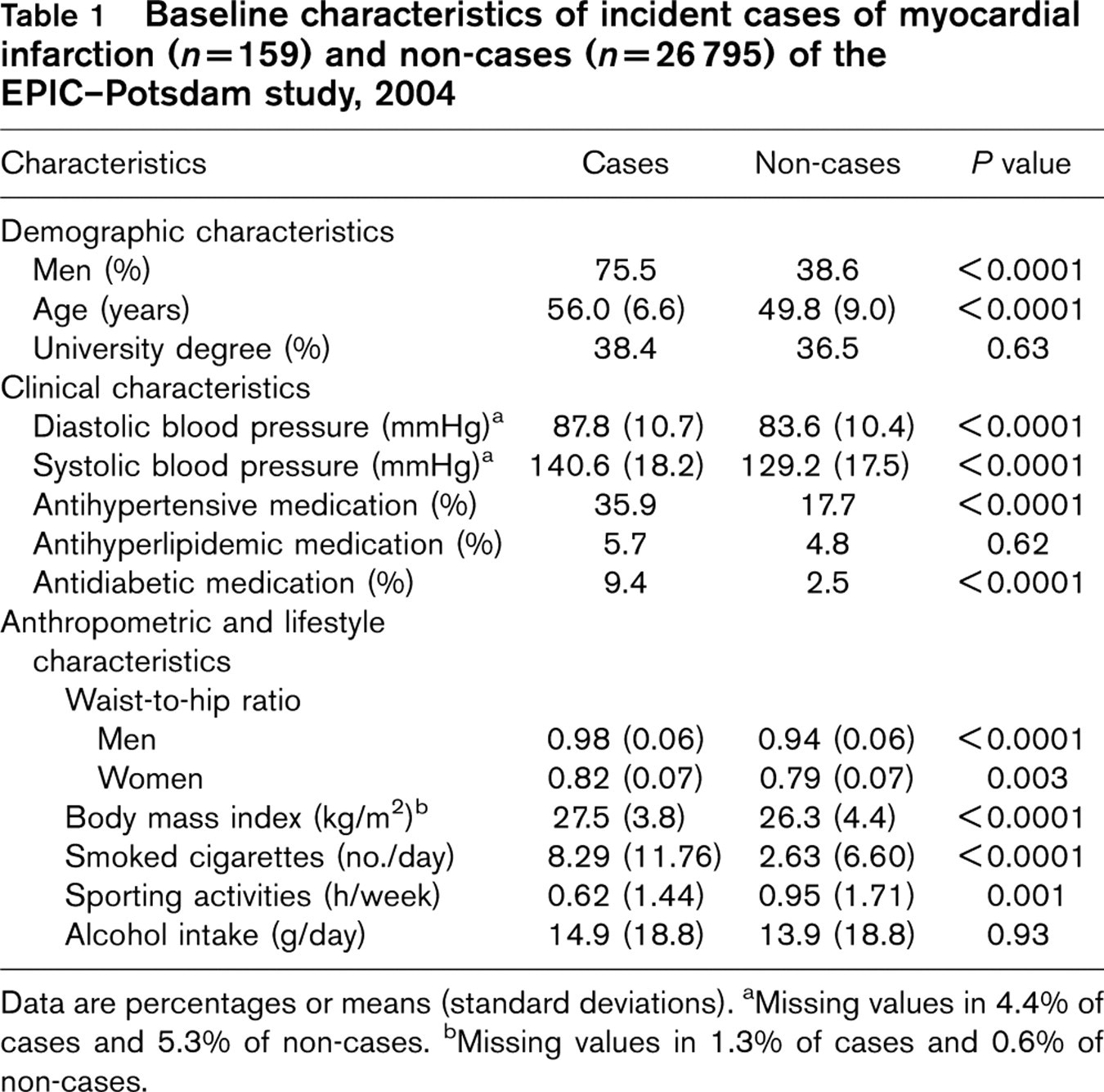
Data are percentages or means (standard deviations). aMissing values in 4.4% of cases and 5.3% of non-cases. bMissing values in 1.3% of cases and 0.6% of non-cases.
Prevalence, relative and population-attributable risk of myocardial infarction for single potentially modifiable classic risk factors in the EPIC-Potsdam study, 2004 (n = 26954)
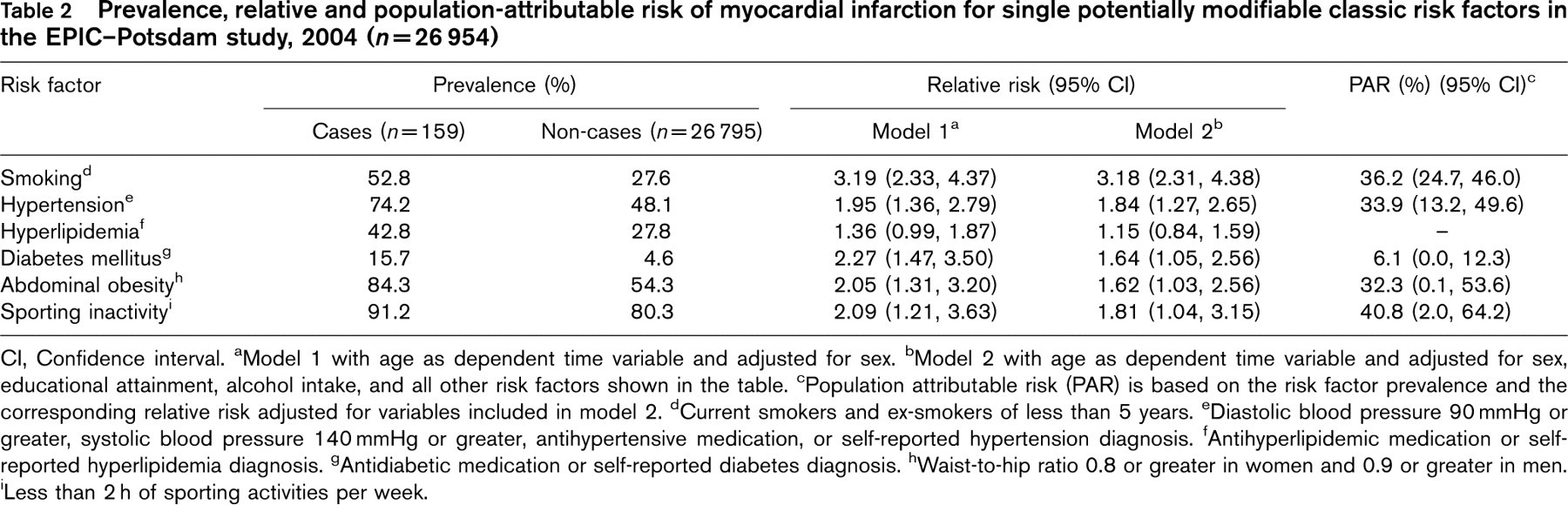
CI, Confidence interval. aModel 1 with age as dependent time variable and adjusted for sex. bModel 2 with age as dependent time variable and adjusted for sex, educational attainment, alcohol intake, and all other risk factors shown in the table. cPopulation attributable risk (PAR) is based on the risk factor prevalence and the corresponding relative risk adjusted for variables included in model 2. dCurrent smokers and ex-smokers of less than 5 years. eDiastolic blood pressure 90 mmHg or greater, systolic blood pressure 140 mmHg or greater, antihypertensive medication, or self-reported hypertension diagnosis. fAntihyperlipidemic medication or self-reported hyperlipidemia diagnosis. gAntidiabetic medication or self-reported diabetes diagnosis. hWaist-to-hip ratio 0.8 or greater in women and 0.9 or greater in men. ‘Less than 2 h of sporting activities per week.
In Table 1 the baseline characteristics of myocardial infarction cases and non-cases are compared. As expected, cases were to a higher percentage men and were older than non-cases. The degree of educational attainment did not differ between the two groups. Mean blood pressure levels were higher and intakes of antihypertensive and antidiabetic medication were more frequent among cases than non-cases, whereas the intake of antihyperlipidemic medication was similar. Except for the daily alcohol consumption, significant differences in means of lifestyle and anthropometric characteristics were observed between the groups.
Table 2 indicates that the observed prevalences of the dichotomous potentially modifiable risk factors were higher among cases of myocardial infarction than non-cases (P < 0.001). After adjustment for age, sex, educational attainment, alcohol intake, and the other five risk factors, the relative risk of myocardial infarction for smoking was 3.18 [95% confidence interval (CI) 2.31, 4.38]. The corresponding relative risks were 1.84 for hypertension (95% CI 1.27, 2.65), 1.81 for sporting inactivity (95% CI 1.04, 3.15), 1.64 for diabetes mellitus (95% CI 1.05, 2.56), and 1.62 for abdominal obesity (95% CI 1.03, 2.56). Self-reported hyperlipidemia was the only considered risk factor not significantly associated with myocardial infarction in the study population (relative risk 1.15; 95% CI 0.84, 1.59). Therefore, hyperlipidemia was not further considered as a risk factor, but remained as a confounder variable in all models of the following analyses. According to the estimated PAR, 36.2% (95% CI 24.7, 46.0) of myocardial infarctions in the EPIC-Potsdam study were attributable to smoking. Slightly lower attributable risks were obtained for hypertension (PAR 33.9%; 95% CI 13.2, 49.6) and abdominal obesity (PAR 32.3%; 95% CI 0.1, 53.6). Sporting inactivity was the risk factor with the highest PAR (40.8%), but at the same time had a wide confidence interval (95% CI 2.0, 64.2). The lowest percentage of cases was attributable to diabetes mellitus (PAR 6.1; 95% CI 0.0, 12.3). Overall, 84.3% of incident cases of myocardial infarction were explainable by all combinations of the five risk factors (data not shown).
As risk factors often occur simultaneously, we examined the relationship between the number of risk factors present among participants at baseline and the risk of myocardial infarction. Table 3 shows that a markedly higher percentage of non-cases than cases had less than three of the five risk factors, which were significantly associated with myocardial infarction. Consequently, a higher percentage of cases than non-cases was characterized by three or more risk factors. The risk of myocardial infarction increased substantially with the increasing number of risk factors (P for trend < 0.0001). Individuals with four or five risk factors thus had an 11.52-fold increased risk of myocardial infarction compared with individuals with none or one risk factor.
The magnitude of the association between the number of present risk factors per individual and the risk of myocardial infarction may vary according to the underlying combination of risk factors. Therefore, we identified those risk profiles that had a significant relative and attributable risk of myocardial infarction and were thus most important in contributing to the coronary event in the study population. Three of the five identified combinations included sporting inactivity in addition to two of the risk factors abdominal obesity, hypertension, and smoking (Table 4). The relative risks of myocardial infarction for these combinations of risk factors varied between 2.48 and 6.62 and their PAR ranged from 3.2 to 12.8%. The further two combinations comprised sporting inactivity, abdominal obesity, hypertension, and either diabetes or smoking as components. The risk profile with smoking as the fourth factor had the highest relative risk (9.08, 95% CI 5.38, 15.34) as well as the highest attributable risk (PAR 23.5; 95% CI 15.9, 30.4) of the five combinations. Altogether, 55.8% of myocardial infarction cases in the EPIC-Potsdam cohort were attributable only to the five specified combinations of risk factors.
Prevalence and relative risk of myocardial infarction for the number of present potentially modifiable classic risk factors in the EPIC-Potsdam study, 2004 (n = 26 954)
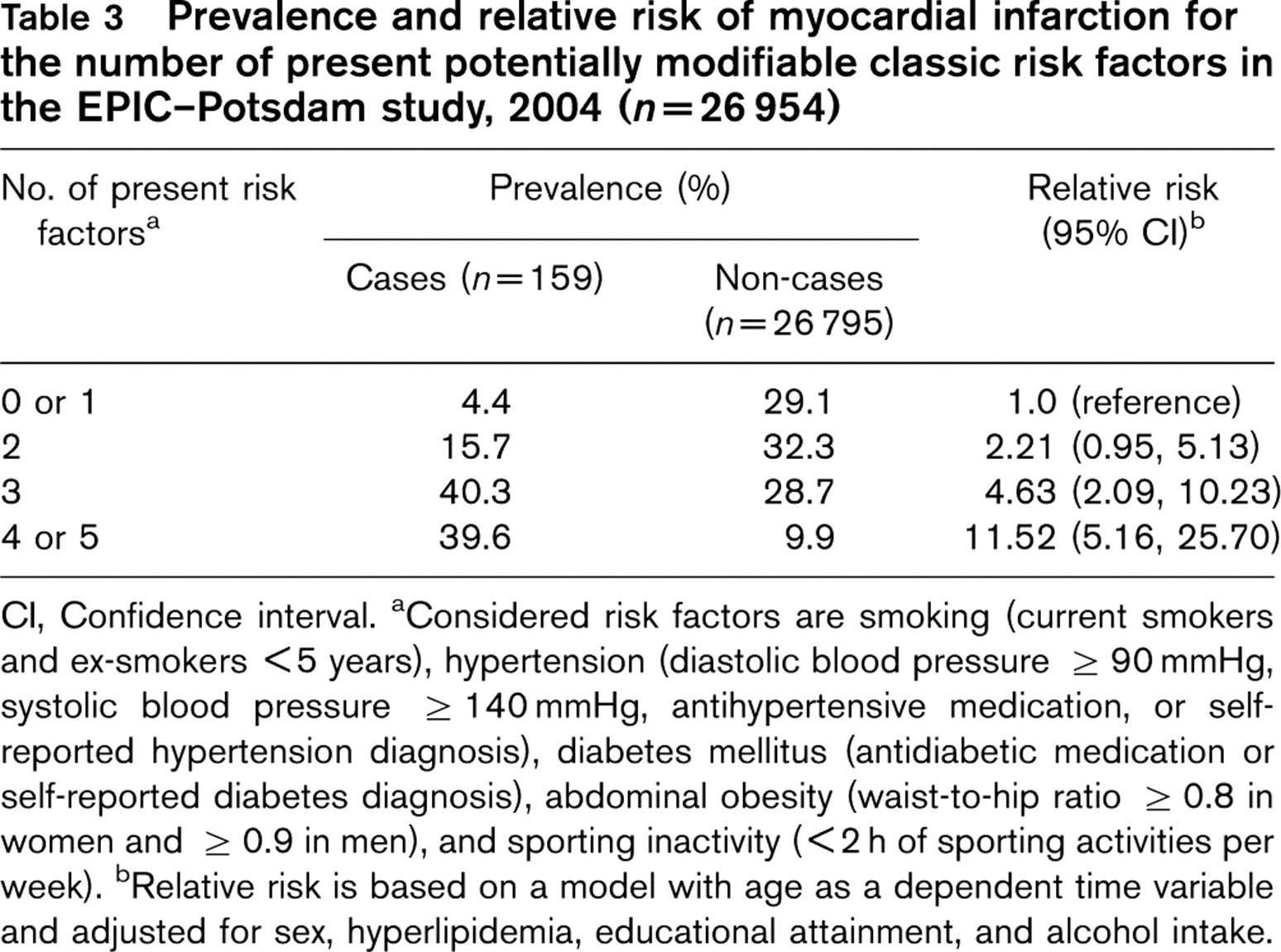
CI, Confidence interval. aConsidered risk factors are smoking (current smokers and ex-smokers <5 years), hypertension (diastolic blood pressure ≥ 90 mmHg, systolic blood pressure ≥ 140 mmHg, antihypertensive medication, or self-reported hypertension diagnosis), diabetes mellitus (antidiabetic medication or self-reported diabetes diagnosis), abdominal obesity (waist-to-hip ratio ≥ 0.8 in women and ≥ 0.9 in men), and sporting inactivity (< 2 h of sporting activities per week). bRelative risk is based on a model with age as a dependent time variable and adjusted for sex, hyperlipidemia, educational attainment, and alcohol intake.
Prevalence, relative and population attributable risk of myocardial infarction for important combinations of potentially modifiable classic risk factors in the EPIC-Potsdam study, 2004 (n = 26 954)
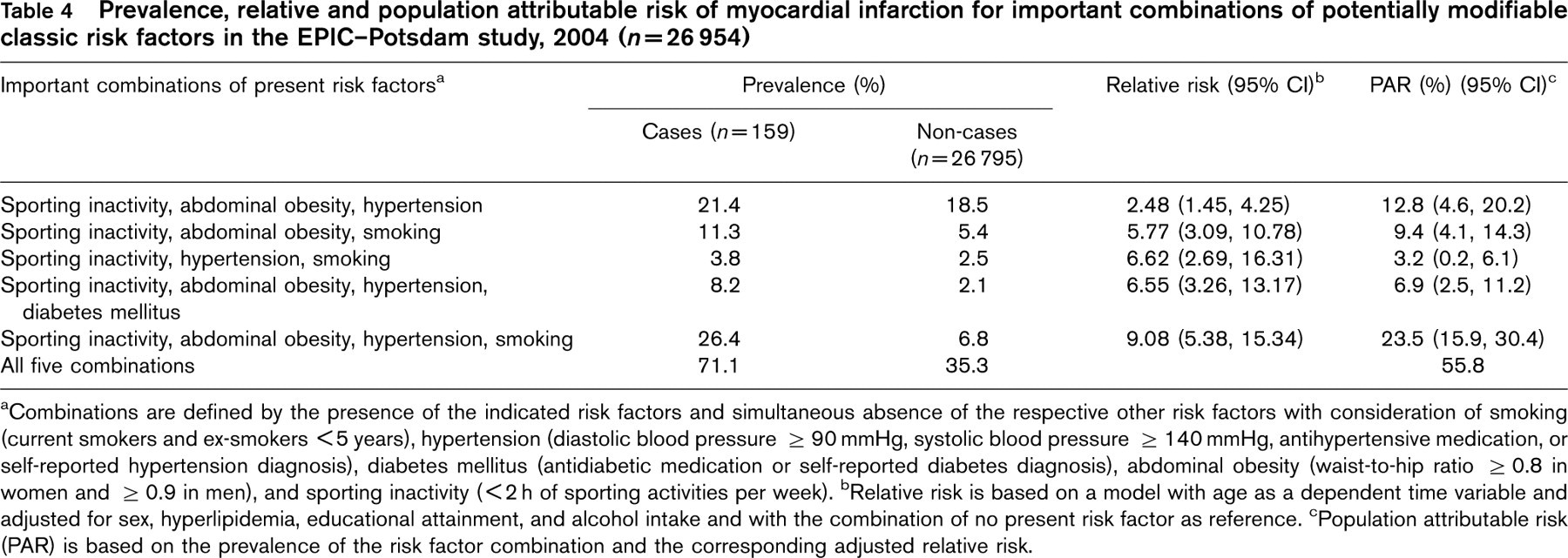
aCombinations are defined by the presence of the indicated risk factors and simultaneous absence of the respective other risk factors with consideration of smoking (currentsmokers and ex-smokers <5 years), hypertension (diastolic blood pressure ≥ 90 mmHg, systolic blood pressure ≥ 140 mmHg, antihypertensive medication, or self-reported hypertension diagnosis), diabetes mellitus (antidiabetic medication or self-reported diabetes diagnosis), abdominal obesity (waist-to-hip ratio ≥ 0.8 in women and ≥ 0.9 in men), and sporting inactivity (< 2 h of sporting activities per week). bRelative risk is based on a model with age as a dependent time variable and adjusted for sex, hyperlipidemia, educational attainment, and alcohol intake and with the combination of no present risk factor as reference. cPopulation attributable risk (PAR) is based on the prevalence of the risk factor combination and the corresponding adjusted relative risk.
Discussion
The results of this study confirm the high prevalence of classic coronary risk factors and emphasize their vast contribution to the risk of myocardial infarction in the EPIC-Potsdam cohort, especially at the simultaneous presence of several risk factors and for certain risk factor combinations.
The prevalences of the risk factors hypertension, diabetes mellitus, and sporting inactivity as well as the mean waist-to-hip ratio at baseline (1994-1998) of the EPIC-Potsdam study were similar to those observed within a representative sample of the adult east German population of the German National Health Interview and Examination Survey 1998 [20–23]. In contrast, the prevalences of smoking and hyperlipidemia were lower in our study population than in the survey sample [24, 25]. The observed differences may be partly due to varying risk factor definitions and the different age ranges of the study populations, but may also be related to the higher socio-economic status of the EPIC-Potsdam participants. However, in our cohort as well as in the national survey the most frequent risk factor was sporting inactivity, whereas diabetes showed the lowest frequency.
The risk factors showed a markedly higher prevalence among participants who developed myocardial infarction than among participants without this event, and were independently and significantly associated with the risk of myocardial infarction. An exception was hyperlipidemia, which in contrast to evidence from the literature [8, 26, 27] was only in tendency, but not significantly, related to the risk of myocardial infarction. One possible reason for this observation may be that in our study the definition of hyperlipidemia was based on self-reports, which had a low reproducibility kappa coefficient [28]. The further considered risk factors smoking, hypertension, diabetes mellitus, and abdominal obesity each showed a significant direct association with the risk of myocardial infarction that was independent of the respective other risk factors, age, sex, educational attainment, and alcohol intake and of similar strength as in other cohort studies [27, 29–32]. The varying definition of physical activity across studies, including the different assessment of the type, frequency, duration, and intensity complicates the comparison of the relative risk estimates with our study; however, an increasing coronary risk with lower physical activity was evident in most prospective studies [33].
As the impact of a risk factor depends on both its frequency in the population and the strength of its association with a disease, we examined the PAR of the five risk factors that were significantly related to myocardial infarction. As a result, 6% of cases of myocardial infarction in the study population were attributable to diabetes mellitus, whereas one-third or more were each explainable by smoking, hypertension, abdominal obesity, and sporting inactivity. Although sporting inactivity was associated with only a moderate increase in coronary risk, it showed the highest PAR (40.8%) among the examined risk factors. This observation is explainable by the enormously high percentage of sporting inactive individuals among the cases of myocardial infarction in the study population. However, the wide confidence intervals of the relative risks for sporting inactivity and abdominal obesity resulted in a relatively low precision of their PAR. Because for estimation of PAR the varying prevalence of a risk factor across populations has to be considered, it is difficult to compare PAR of this study with those of other studies. However, it is worth mentioning that in the western European countries of the large-scale case-control study INTERHEART the PAR of smoking, hypertension, diabetes, abdominal obesity, and exercise were of similar magnitude for myocardial infarction as in our study population [5]. Furthermore, 84.3% of incident cases of myocardial infarctions in the EPIC-Potsdam cohort were attributable to the presence of the five risk factors together. In the INTERHEART study, 93.9% and therefore ‘only’ 9.6% more cases of myocardial infarction in western Europe were explained by the additional consideration of four further risk factors [5].
Several risk factors are usually present at the same time [6] promoting a clearly higher coronary risk than observed for single risk factors [8, 34]. Actually, the majority of participants in the EPIC-Potsdam study showed more than one classic risk factor, and coronary risk increased substantially with an increasing number of present risk factors. Not only a varying number of risk factors, but also varying combinations of risk factors might contribute differently to the incidence of myocardial infarction. Therefore, we were also interested in those combinations of potentially modifiable risk factors with the highest impact on myocardial infarction. Five important combinations each including three or four risk factors were identified. Together they explained 55.8% of cases of myocardial infarction in our study population. Corresponding to a similar analysis within the same study population [16], the risk profile with the highest impact was characterized by the simultaneous presence of sporting inactivity, abdominal obesity, hypertension, and smoking, and was attributable to 23.5% of myocardial infarctions. A prominent role was again observed for sporting inactivity as it was the only risk factor included in each of the five combinations.
From a public health point of view, one strength of this study is the determination of risk profiles, which might be efficient targets for prevention strategies to reduce the incidence of myocardial infarction [35]. Compared with the common approach of considering the joint effect of several risk factors [5], risk profiles are more specific. An advantage of the prospective study design is that risk factors were assessed before myocardial infarction occurred, resulting in a minimized possibility of recall bias. In addition, all potential cases of myocardial infarction were medically verified and therefore should not be biased by misclassification. The limitations of this study include the fact that definitions of the risk factors smoking, diabetes, hyperlipidemia, and sporting inactivity were based purely on self-reports of participants and thus self-reporting-associated misclassifications have to be taken into account. Furthermore, the estimation of stratum-specific PAR generally requires a categorization of continuous variables. Consequently, different threshold values for the definition of risk factors may result in different risk estimates. However, for most risk factors we used established definitions. Participants in the EPIC-Potsdam study were recruited from the general population; but, as usual in cohort studies, were of slightly higher socio-economic status [10], which may limit the generalizability of the results. However, as mentioned above, the prevalence of most risk factors was similar between our study cohort and the adult east German population. Finally, because of the moderate number of cases of myocardial infarction the results of the present study are limited to analyses including men and women together. However, all relative risks were adjusted for sex and an additionally performed analysis revealed no significant interactions between sex and the examined risk factors (P for interaction equals 0.79 for smoking, 0.77 for hypertension, 0.65 for hyperlipidemia, 0.70 for diabetes, 0.07 for abdominal obesity, and 0.14 for sporting inactivity). However, in further studies separate analyses for men and women should be preferred as a result of indications of sex-specific differences in the impact of some risk factors on coronary heart disease [36].
Conclusion
Up to 84.3% of cases of myocardial infarction could have been prevented in the EPIC-Potsdam cohort if smoking, hypertension, diabetes mellitus, abdominal obesity, and sporting inactivity would have been avoided. The findings emphasize that prevention strategies to decrease the prevalence of established risk factors are of the utmost relevance to reduce the burden of heart disease.
Footnotes
Acknowledgements
The authors would like to thank Ellen Kohlsdorf and Wolfgang Bernigau for data management, and Wolfgang Fleischhauer for ascertainment of cases of myocardial infarction. The recruitment phase of the EPIC-Potsdam study was supported by the Federal Ministry of Science, Germany (01EA9401) and the European Union (SOC 95201408 05F02).